Governance and policy in global neurosurgery: a scoping review of national and international efforts
Ellianne dos Santos Rubio, Khalil St. Brice, Felix Toussaint, Jimena Colado-Martinez, Garrett W. Thrash, Ali Azan Ahmed, James Kelbert, Walt Johnson

TL;DR
This paper reviews how governments and organizations shape global neurosurgery policies to improve access and reduce disparities.
Contribution
The study maps governmental stakeholders and their roles in advancing global neurosurgery through policy and funding.
Findings
WHO is the most cited organization guiding global neurosurgical policy.
National Ministries of Health are key in developing country-specific neurosurgery policies.
International partnerships improve access in low-resource settings.
Abstract
Governmental organizations play a key role in making Global Neurosurgery timely, safe, and accessible. They are essential in decreasing disparity and improving outcomes through informing policy, funding, and resource allocation. The Boston Declaration aims to promote collaboration between high-income and low- and middle-income countries in addressing these challenges and realizing more equitable access to neurosurgical care worldwide. To identify and map key governmental stakeholders in Global Neurosurgery, emphasizing their roles in policy development, funding, resource allocation, research support, capacity building, advocacy, and international cooperation in addressing unmet neurosurgical needs. We employed a mixed-methods approach, analyzing the roles of governmental organizations in neurosurgery. A comprehensive literature review was conducted using PubMed, Embase, and Global Index…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
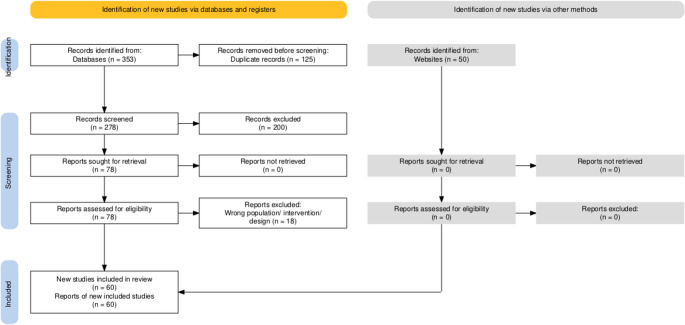 Figure 1
Figure 1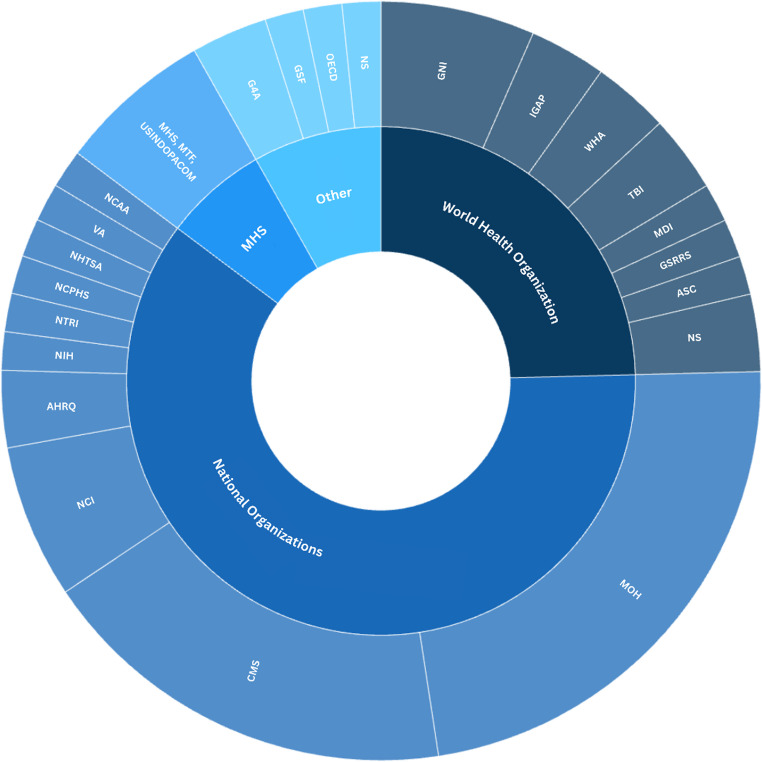 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health and Surgery · History of Medical Practice · Biotechnology and Related Fields
Introduction
The Bogotá Declaration marked a watershed moment in the global advocacy for neurosurgical services with the launch of the Global Action Plan in 2016 [1]. This initiative fundamentally redefined neurosurgery, not only as a specialized medical field, but as an essential component of global health. This is further evidenced by the increasing literature devoted to the challenges centered around neurosurgical care [2–5], the establishment of Global Neurosurgery-oriented organizations [6], and the addition of Global Neurosurgery sessions to various international meetings [7]. This momentum culminated in the Boston Declaration (April 24, 2025), where over one hundred governmental and non-governmental entities collectively affirmed neurosurgery as a global public good, calling for coordinated investment, workforce expansion, and policy integration. Actionable commitments such as an increase in educational efforts to enhance the neurosurgical workforce, more funding for resources, publication and research opportunities etc.
This manuscript maps the evolution of government agencies and their influence on the governance of neurosurgical services and organizations. To achieve this, we identify the key roles in these agencies, review agency policy, and examine the resources devoted to the programs. These factors will be examined in terms of their relevance to the evolution of Global Neurosurgery. In this way, the paper attempts to demonstrate how policymaking in these governments has been an important factor in the expansion of neurosurgery as an essential health sector beyond the confines of individual countries.
Materials & methods
A mixed-methods approach was employed to examine the role of governmental organizations in shaping Global Neurosurgery policies and governance frameworks over time. This approach provides a comprehensive understanding of both qualitative insights and quantitative data relevant to the field of Global Neurosurgery.
Search strategy and sources
A systematic literature search was conducted across three primary databases: PubMed, Embase, and Global Index Medicus, from database inception (PubMed 1872) to October 2024, following the PRISMA-ScR (Preferred Reporting Items for Scoping Reviews) guidelines and the Joanna Briggs Institute (JBI) methodology framework.. The search strategy was designed to capture a wide range of studies related to both neurosurgery and governance. For example, in PubMed, the search terms included “neurosurgery” and “governance,” combined with “policy,” “governmental agencies,” and related MeSH terms. Similar search strategies were applied in the other databases to ensure comprehensive coverage. The complete PubMed search string and database-specific adaptations are provided in Supplementary Table 1.
To supplement the peer-reviewed literature, we also searched the WHO’s IRIS database to gather policy documents and organizational reports relevant to global health governance, explicitly focusing on neurosurgery. In total, 283 articles were identified across the four primary databases.
Grey literature search
Grey literature records retrieved from Global Index Medicus and institutional websites were screened in parallel with peer-reviewed sources and are included in the PRISMA flow diagram totals. This search used official websites, reports, and bulletins from global health ministries, international organizations, and governmental health agencies. We employed targeted search terms such as “Ministry of Health,” “neurosurgery,” “government,” and the names of specific countries to identify relevant documents and ongoing governmental initiatives. This allowed us to incorporate up-to-date information on the role of governments in developing Global Neurosurgery.
Study selection and inclusion criteria
Studies and documents were selected based on predefined inclusion and exclusion criteria. The inclusion criteria encompassed governmental organizations at local, national, continental, and global levels, institutions that fund neurosurgical capacity-building initiatives, and public health organizations contributing to policy development related to Global Neurosurgery. Additionally, we included reports and communications from international collaborations that directly impacted neurosurgical services in low- and middle-income countries (LMICs).
We excluded non-governmental organizations (NGOs), private sector entities, and academic institutions unless they were directly involved in governmental policymaking or had documented participation in public health initiatives related to neurosurgery. A complete list of the stakeholders and organizations included is provided in the supplementary materials.
Data extraction and analysis
Once relevant studies and grey literature were selected, we used Rayyan AI [8] to facilitate the blind screening and data extraction. Authors F.T. and K.S. independently conducted the initial screening. Any discrepancies between the two reviewers were resolved through discussion, reaching a consensus on the final selection of documents.
For each relevant document, we extracted key data related to the role of governmental organizations in developing and implementing neurosurgery policies. This data included information on policy frameworks, partnerships, and specific programs to address gaps in neurosurgical services in LMICs.
The extracted data was systematically entered into a spreadsheet for further analysis. We categorized the organizations based on their role in Global Neurosurgery, level of influence in policymaking, and the extent of their financial investment in neurosurgical programs. This categorization allowed us to identify trends in governmental involvement across different regions and assess the impact of various initiatives on global neurosurgical development (Fig. 1).
Fig. 1PRISMA diagram illustrating article screening and exclusion criteria
Synthesis of results
The synthesized data was analyzed qualitatively to identify recurring themes related to governmental involvement in Global Neurosurgery. Key areas of focus included:
- Policy development: How governments have integrated neurosurgery into national health policies.
- Collaborations: The role of intergovernmental and international partnerships in advancing neurosurgical services in LMICs.
- Impact: What has been the impact of governmental involvement on Global Neurosurgery.
Additionally, we used a framework to assess the evolution of Global Neurosurgery governance over time, evaluating shifts in policy priorities and the effectiveness of funding mechanisms. The results were presented in a structured table, categorizing the organizations by their roles and contributions to the field.
Results
Here, we summarize the 60 articles after PRISMA screening and investigate the major stakeholders of governmental organizations in Global Neurosurgery (Fig. 2). Across the 60 included articles, WHO was referenced in 25%, national Ministries of Health in 23%, CMS in 18%, military health services in 7%, and international coalitions such as G4 Alliance and International Global Action Plan on Epilepsy (IGAP) in 5%. A detailed breakdown of all included studies, including study type, region, organization type, and scope of contribution, is provided in Table 1.
Fig. 2. Stakeholder mapping of world and national health organizations. This is a qualitative visual representation of stakeholder frequency, with sector sizes reflecting proportional citation frequency. GNI = Global Neurosurgery Initiative, IGAP = International Global Action Plan on Epilepsy, WHA = World Health Assembly, TBI = Collaborating Centre Task Force on Mild Traumatic Brain Injury, MDI = Minimum Dataset for Injury, GSRRS = Global Status Report on Road Safety, ASC = African Subcommittee, WHO = World Health Organization, MOH = Ministries of health, CMS = Centers for Medicare & Medicaid Services, NCI = National Cancer Institute, AHRQ = Agency for Healthcare Research and Quality, NIH = National Institutes of Health, NTRI = National Trauma Research Institute, NCPHS= National Commission for the Protection of Human Subjects, NHTSA = National Highway Traffic Safety Administration, VA = Department of Veteran Affairs, NCAA = National Collegiate Athletic Association, MHS = Military Health Systems, MHT = Military Treatment Facilities, USINDOPACOM = US Indo-Pacific Command, G4A = G4 Alliance, GSF = Global Surgery Foundation, OECD = Organization for Economic Cooperation and Development, NS = Not Specified
Table 1. Summary of included studiesAuthorRegionOrganisation TypeContributionAsija et al. 2024South Asia (India, Nepal - LMIC survey)Academic or Hospital-Led Policy Effort (Neurosurgical Departments/Respondents)Functional Neurosurgery - Training Gap/Affordability/Access BarriersZaidi et al. 2024South Asia (Pakistan)National Ministries & Public Health Agencies (MOH Pakistan + Academic Partner)Stroke Systems - Lack of Units/Delayed Referral/No National Strategy Shakir et al. 2024Global South (LMICs)National Ministries & Public Health Agencies (MOH/National Insurance Bodies)Brain Tumor Care - Underfunding/Policy Instability/No ReimbursementTini et al. 2024Global South (LMICs; examples include Ukraine, Philippines)National Ministries & Public Health Agencies (governments; UHC packages); Multilateral Coalitions/Advocacy Platforms (WHO initiatives referenced in citations)Neuro-oncology (GBM) - Policy levers across NSOAP domains: insurance/UHC inclusion, regulate RT/drugs; build registries, labs, workforce; enable trials/telemedicine Gupta et al. 2024Global (LMIC emphasis)Global Health Agencies (WHO - IGAP/WHA)Epilepsy/neurology policy - positions neurosurgery within WHO’s IGAP; outlines monitoring/implementation needs and opportunities for neurosurgical engagement.Kim et al. 2023Southeast Asia (Cambodia - Phnom Penh)National Ministries & Public Health Agencies (major government hospital; residency program)Neurosurgical Burden - Trauma-dominant caseload; workforce shortage; capacity buildingWoodle et al. 2023Asia-Pacific (U.S. Military facility in Okinawa, Japan)Military Health Systems (U.S. Department of Defense/Military Treatment Facilities)Pediatric Neurosurgery Delivery - Demonstrates feasibility of high-level neurosurgical care within overseas military hospitals; supports military readiness policyPattisapu et al. 2023Global South (LMIC focus - Africa & Asia)Multilateral Coalitions/Advocacy Platforms (G4 Alliance, WFNS, Global Surgery Networks)Neurosurgical Advocacy - Global policy voice; NSOAP inclusion; representation in WHO processesSalisu-Kabara et al. 2022*West Africa (Nigeria)Academic or Hospital-Led Policy Effort (Tertiary Hospital Surgical Unit)Traumatic Brain Injury (TBI) - Limited neurosurgical workforce; Delayed referrals; Lack of critical care infrastructureAruah et al. 2023West Africa (Nigeria)National Ministries & Public Health Agencies (Federal Ministry of Health Nigeria)Spinal Trauma - Inadequate rehabilitation services; Poor policy implementation; Limited funding for post-surgical careJaved et al. 2023South Asia (Pakistan)Global Health Agencies (WHO/WHA; PGSSC); National Ministries & Public Health Agencies (MOH Pakistan; NVSC2025)System strengthening (neurotrauma) - Pakistan WHA68.15 signatory; NVSC2025 developed with WHO/PGSSC; calls for equitable public-sector neurosurgical access and policy follow-through.Tebha et al. 2023LMICs (Africa, Asia, Americas)National Ministries & Public Health Agencies (MOH-Oriented Review Framework)Glioblastoma - Radiotherapy & Workforce Shortage/High Cost Burden Garcia et al. 2023Global (WHA75)Global Health Agencies (WHO/WHA; IGAP); Multilateral Coalitions/Advocacy Platforms (G4 Alliance; GSF; GAPSBi-F)Global advocacy - neurosurgical delegation at WHA75; push for folic-acid fortification resolution; highlight IGAP (epilepsy/neurologic disorders) and financing via GSF.Shlobin et al. 2023Multi-Regional (Latin America, Africa, Asia)Global Health Agencies (WHO/GAPSBiF)Spina Bifida Prevention - Folic acid fortification advocacy; neurosurgeons in prevention policyBarthélemy et al. 2022Global South (LMICs)National Ministries & Public Health Agencies (LMIC health ministries; WHO benchmarking)Neurotrauma Surveillance - National registry data dictionaries; WHO alignment; infrastructure gapsVeerappan et al. 2022Global (Case Studies Across LMICs)Multilateral Coalitions/Advocacy Platforms (UN SDG3, Harvard PGSSC, WFNS)Public Health Integration - Food fortification; RTA legislation; neurosurgeon-led advocacy modelsJamjoom et al. 2022Middle East (Saudi Arabia)National Ministries & Public Health Agencies (MOH + Military & Private Hospitals)Workforce Distribution - Regional neurosurgeon disparity; recommends redistribution strategiesGoyal et al. 2022North America (USA)National Registry/Regulatory Bodies (CoC/NCDB)Glioblastoma Surgery - Access disparities at high-volume CoC centers; race/socioeconomic inequityMasiliūnas et al. 2022Europe (Lithuania)National Ministries & Public Health Agencies (MOH/national stroke program)Acute Ischemic Stroke - Comprehensive national policy; expanded reperfusion access; door-to-needle improvementRolle et al. 2022Caribbean (CARICOM member states)National Ministries & Public Health Agencies (helmet legislation; enforcement systems)Traumatic Brain Injury - Helmet safety governance; laws & enforcement; infrastructure/regulationsSinger et al. 2022GlobalGlobal Health Agencies (WHA/WHO); Multilateral Coalitions/Advocacy Platforms (GAPSBi-F; FFI; IFSBH)NTD prevention (folic acid fortification) - urges WHA resolution; 58 countries mandate fortification; advocates pediatric-led policy action and monitoring.Jella et al. 2021North America (USA)Health Financing & Reimbursement Bodies (CMS/MACRA)Low-Back Pain Imaging - OP-8 metric; MACRA-linked reimbursement; utilization trends by hospital type Lepard et al. 2021Global (HIC vs. LMIC)National Ministries & Public Health Agencies (helmet legislation)Road-Traffic Injury Prevention - Mandatory helmet laws; improved outcomes; policy effectiveness by income levelMorii et al. 2021East Asia (Japan - Hokkaido)Academic or Hospital-Led Policy Effort (endovascular stroke network evaluation)Acute Ischemic Stroke - Drive-and-Retrieve thrombectomy model; access expansion; cost-effectivenessLefever et al. 2021North America (USA)Professional Society/Coalition (AANS/CNS Washington Office; advocacy to government)US Neurosurgery Advocacy - Legislative process; lobbying/PACs; federal & state policy engagement Tate et al. 2021 Global (multisite; militaryrelevant)Military & Defense Health Systems (DoD/VA collaboration; ENIGMA Military WG)Traumatic Brain Injury - Multi-site harmonization; data sharing; research coordinationKim et al. 2020North America (USA)National Ministries & Public Health Agencies (NCI/NIH)Brain Metastasis - Federal Research Strategy/Coordination GapsAntony et al. 2020Oceania (Australia)National Ministries & Public Health Agencies (State/Territory Health Departments; public hospitals)COVID-19 service delivery - Elective case reductions; urgent care maintained; triage & preparedness lessonsRichter et al. 2020North America (USA)Health Financing & Reimbursemen t Bodies (CMS/Medicare; ACOs; bundledpayment programs)Reimbursement policy - Inflation-adjusted neurosurgery payments declined; bundled-payment context; service viabilityDallas et al. 2019North America (USA)National Ministries & Public Health Agencies (AHRQ/HCUP–NIS; payer mix incl. Medicare/Medicaid/private)Pediatric NMS fusion - High median cost; regional/hospital variation; payer differencesMcClelland III et al. 2019North America (USA)Health Financing & Reimbursement Bodies (CMS/Medicare; ATRA policy)SRS payment policy -ATRA altered Gamma Knife vs. LINAC parity; utilization shiftsChilders et al. 2019North America (USA)Health Financing & Reimbursemen t Bodies (CMS/RVU system); Academic or Hospital-Led Policy Efforts (ACS-NSQIP registry)Payment policy (RVUs) - shows variation in work RVUs explained by objective measures (OR time, LOS, readmission/reoperation); recommends using registry data to improve RVU updates and reduce specialty differences.Rumalla et al. 2018 North America (USA)Health Financing & Reimbursement Bodies (CMS/Medicare; insurance schemes)Epilepsy readmissions - national database analysis of drivers of 30-day readmission; payer/insurance and clinical factors inform reimbursement and quality policy.Khan et al. 2019South America & South Asia (Chile; Pakistan)National Ministries & Public Health Agencies (National disaster/health ministries; WHO Emergency Medical Teams standards; UN/NGO partners)Disaster/trauma systems - Mass Casualty Centres model; civilian–military integration; 24/7 surgical capacityYousefzadeh-Chabok et al. 2018Middle East (Iran)National Ministries & Public Health Agencies (MOHME; national trauma registries)Cerebrovascular/trauma systems - national registry initiatives (INTRD; NSCIR) and hospital data processes; highlights standardized data capture for policy/surveillance.Cancedda et al. 2018Sub-Saharan Africa (Rwanda)National Ministries & Public Health Agencies (Rwanda MOH; CDC/PEPFAR); Multilateral Coalitions/Advocacy/Donors (Global Fund); Academic or Hospital-Led Policy Efforts (U.S. universities/teaching hospitals)Health workforce & systems - government-led HRH scale-up with external partners; documents policy/financing model and outcomes for training, retention, and service delivery.Foster et al. 2018Global (HIC emphasis)Academic or Hospital-Led Policy Efforts (without formal mandate) (universities/clinical guideline groups)Low back pain policy; align practice to evidence; prioritize self-management/exercise; curb routine imaging/opioids/surgery; redesign pathways & payment/public-health strategies.Yoon et al. 2018North America (USA)Health Financing & Reimbursement Bodies (Insurers; state price tools)Price transparency/value - large cost variation in neurosurgery; promote “expected payment” episode data; pair with scorecards, reference pricing.Ostrom et al. 2017North America (USA)National Ministries & Public Health Agencies (NCI/NIH); Academic or Hospital-Led Policy Efforts (institutional biobanks/consortia)Neuro-oncology biobanking - governance, consent, linkage to registries; recommends standardized policies and national coordination to advance glioma/GBM research.Villelli et al. 2017North America (USA-Massachusetts vs. New York control)Health Financing & Reimbursement Bodies (Medicare/Medicaid/private insurers)Spine surgery & reform; MA reform shifted payer mix-fewer uninsured/private, more Medicare; treated cohort older.Menger et al. 2017North America (USA)Health Financing & Reimbursement Bodies (private insurers; Medicare/Medicaid; TRICARE; workers’ comp)Preauthorization & access; insurer preauth causes delays/denials; Medicare protective vs. other payers.Broglio et al. 2017North America (USA-national)Military & Defense Health Systems (DoD); Multilateral Coalitions/Advocacy Platforms (NCAA)Concussion research network; NCAA-DoD CARE Consortium design & governance; >25k athletes enrolled across sites.Kuo et al. 2016East Asia (Taiwan)National Ministries & Public Health Agencies (traffic/health authorities; trauma registries)Helmet policy & outcomes; helmet use linked to lower mortality/ICU need/complications (adjusted ORs); supports enforcement & prevention. Sharma et al. 2017North America (Canada-Ontario)National Ministries & Public Health Agencies (MOHLTC; provincial program)System redesign/PNO; centralized neurosurgery services with teleradiology/outreach; bundled funding & transfer coordination.Russell et al. 2017Africa (continental overview)Multilateral Coalitions/Advocacy Platforms (IBRO, WFNS, WFN, ILAE)Neuroscience history/capacity; charts growth of African neuroscience; highlights roles of IBRO/WFNS/WFN/ILAE and need for sustained training/funding links.Menger et al. 2015North America (USA-national)Health Financing & Reimbursement Bodies (CMS); National Ministries & Public Health Agencies (policy context)ACA & value agenda; argues for specialty registries (N2QOD) to define quality/value; urges unified, data-driven advocacy.Middleton et al. 2015Oceania (Australia & New Zealand)Multilateral Coalitions/Advocacy Platforms (ANZ networks; research consortia); National Ministries & Public Health Agencies (government funders/policy)*SCI research strategy; proposes networks/partnerships, priority-setting & consumer engagement; national registries/infrastructure roadmap.Kondo et al. 2015East Asia (Japan)National Ministries & Public Health Agencies *(MHLW/public health programs)*Folic acid & NTDs; FA awareness increased supplement use; recommends mandatory food fortification to lower spina bifida riskStrom et al. 2013North America *(USA — Louisiana)*National Ministries & Public Health Agencies *(State helmet law; NHTSA; Louisiana Highway Safety Commission)*Motorcycle TBI prevention - repeal raised fatalities; reinstatement increase helmet use but fatalities stayed high; recommends added policy/enforcement.Groman et al. 2013North America *(USA)*Health Financing & Reimbursement Bodies *(CMS; CMMI; IPAB; PCORI)*Payment reform/quality - ACA shifts reimbursement toward value; VBP, readmission/HAC penalties, physician value-modifier; need better specialty-relevant metrics and data infrastructure.Cheng et al. 2011East Asia (Taiwan)Health Financing & Reimbursement Bodies (National Insurance Schemes — Taiwan NHI)Data governance/claims registries - describes standardized NHI datasets and linkage for research & policy; notes application/review processes and privacy controls.Khalessi et al. 2010North America (USA)National Ministries & Public Health Agencies (AHRQ/DHHS; CMS)Stroke (mechanical thrombectomy)/reimbursement - formal response to AHRQ Draft Technical Brief; advocates evidence-based Medicare coverage; coordinates multispecialty inputEmejulu 2008West Africa (NigeriaNational Ministries & Public Health Agencies (MOH; public tertiary hospitals)Workforce/capacity - ~15 practicing neurosurgeons/150 M; services rated inadequate; calls for training expansion, facilities, enabling policyBean 2005North America & East Asia (USA, Japan - OECD compari son)National Ministries & Public Health Agencies (national health systems; OECD context)Health-system comparison - Japan’s universal insurance + price controls vs. U.S. market pricing; argues neurosurgery must show cost-effectiveness to inform coverageHolst et Cassidy 2004GlobalGlobal Health Agencies *(WHO Collaborating Centre Task Force on MTBI)*MTBI policy framework - establishes task force; best-evidence synthesis on epidemiology/diagnosis/prognosis/treatment/costs; guidance to reduce burden.Borg et al. 2004GlobalGlobal Health Agencies (WHO Collaborating Centre Task Force)MTBI care & costs - early educational info and activation help; intensive routine follow-up not supported; indirect costs exceed direct.Bean 2002North America (USA)Health Financing & Reimbursement Bodies (CMS/HCFA; AMA CPT; RUC)Valuation mechanics - Explains CPT-RUC-CMS linkage; Medicare fee schedule becomes de-facto national schedule shaping neurosurgery paymentsKhamlichi 2001Africa (continental overview; North, West, East, Southern Africa)Global Health Agencies (WHO African Subcommittee/WFNS link)Workforce & training − 565 neurosurgeons across Africa; major equipment gaps; priorities: local training, instruments, CT access, shunts.Antioch 2000Oceania (Australia - Victoria)Health Financing & Reimbursement Bodies (State health funding authorities)Hospital financing/casemix - evaluates DRG/casemix purchasing and performance frameworks; recommends design goals and bundled/episode-based approaches for surgical services.National Commission on the Protection of Human Subjects, 1977North America *(USA - federal)*National Ministries & Public Health Agencies *(DHEW; National Commission)*Psychosurgery policy - proposed 2-yr moratorium debated; federal review instead; IRB oversight; informed consent; safeguards for vulnerable groups; national reporting
To contextualize policy evolution over time, Table 2 presents a timeline of major global milestones in neurosurgery governance, from the 2004 World Report on Road Traffic Injury Prevention to the 2025 Boston Declaration, highlighting the progressive formalization of neurosurgery within international health agendas.
Table 2. Timeline of major milestones in global neurosurgery policyYearMilestoneDescription2015WHA 68.15First global surgery resolution recognizing emergency and essential surgical care and anesthesia as part of universal health coverage.2016Bogotá DeclarationLaunch of the Global Neurosurgery Action Plan and formal recognition of neurosurgery in global health dialogs.2019WHA 72 Follow-UpMember states reviewed progress on implementation of WHA 68.15, with references to surgical workforce and governance.2022WHO IGAPIntersectoral Global Action Plan on Epilepsy and Neurological Disorders (2022–2031), indirectly reinforcing neurosurgical priorities.2025Boston DeclarationGlobal pledges from over 100 GOs, NGOs, and academic institutions to expand neurosurgery collaboration and capacity.
Global and regional governments
This group includes key health-related governmental organizations, such as the World Health Organization (WHO), its regional divisions, and the World Bank Group (WB). These organizations are fundamental in designing policy and supervising the delivery of neurosurgical care worldwide. The WHO is mentioned in about 25% of the reviewed literature, which implies its critical role in formulating policy direction on health that has vast effects on neurosurgery. The World Health Assembly (WHA), the governing body of WHO, sets its priorities, agenda, and budget. The WHO then engages with Member States’ Ministries of Health through WHO HQ, regional and national offices to facilitate better policies, health systems, and programs through an integrative approach to planning at the country level.
National ministries of health
These agencies were mentioned in 23% of the articles as having an essential role in developing healthcare strategies appropriate for different countries concerning the needs for neurosurgery. They are instrumental in establishing the national system and setting healthcare trends that directly affect the provision of neurosurgical services. While East Africa and countries like India have started national neurosurgery programs to improve the quality of education and training of neurosurgeons, there are still many challenges in providing these services [9, 10].
Insurance coverage and military service
Even though insurance services such as the Centers for Medicare and Medicaid Services (CMS) do not fund projects that deliver neurosurgical services, they influence how neurosurgical procedures are regulated and reimbursed, which has a significant effect on patient access and healthcare delivery in the US. They have been mentioned in 18% of our review search. 7% of our manuscripts mentioned U.S. military services and the importance of maintaining their implementation of neurosurgical procedures during warfare.
International collaborative initiatives
This group encompasses transnational collaborations, including G4 Alliance, WHO Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders (IGAP), and Global Neurosurgery Initiative (GNI) of the Program in Global Surgery and Social Change (PGSSC) at Harvard Medical School, with direct neurosurgical involvement, and is mentioned in 5% of articles. In collaboration with GNI and G4 Alliance, Ecuador has been the first country in Latin America to launch a National Surgical Strengthening Plan, including UHC [11], paving the way for an equitable surgical care for the nation, but also putting pressure on the region to do the same [12].
Discussion
Global policy influence and governance mechanisms
The role of governmental organizations is key, not only in the development of policies, but also in their implementation across varying geographic regions. The expansion of the field in the past few decades point to the increased involvement of these organizations in advocating for the availability of neurosurgical services to all. This attitude is changing as Global Neurosurgery has become a more prominent discussion area [13]. Policy development and governance have played an essential role in the development of Global Neurosurgery. One of the most significant achievements was the WHA Resolution on Surgery and Anesthesia (2015) as UHC components [14]. Incorporating surgery into UHC is an important milestone in appreciating the need for surgical services within health systems and strengthening their capacity. In LMICs, insufficient health care coverage leads to staggering out-of-pocket expenses and reduces access to care. Therefore, the Lancet commission on Global Surgery 2015 underlined the importance of Universal Healthcare Coverage (UHC) for surgical professions such as Global Neurosurgery, thus making neurosurgery essential surgical care. They have estimated that a decrease in life-long disabilities and preventable deaths by introducing UHC is not only a sign of improved healthcare access, but is also cost-effective [15].
Indirect public health pathways elevating neurosurgery
Beyond direct policy inclusion, neurosurgery has also gained legitimacy through indirect public health frameworks. Governmental influence on neurosurgical recognition has also occurred indirectly through broader public health agendas. In 2004, the WHO and WB, launched the “World Report on Road Traffic Injury Prevention,” which highlighted road traffic injuries as a worldwide public health priority, emphasizing that they were largely preventable. Traumatic brain injury treatment during warfare resembles LMICs’ resource limitations. It therefore ties directly into the global neurosurgical efforts to design global guidelines, data sharing, and equitable partnerships as the ENIGMA Brain Injury Workgroup suggests [16].
In that same year a United Nations General assembly passed resolution 58/289 (UN Road Safety Collaboration) to improve road safety [17]. In 2020, resolution A/RES/74/299 was made with the goal to decrease road traffic accidents by 50% by 2030, focusing on prevention and post-traumatic care [18]. The Global Status Report on Road Safety by the WHO in 2023 has shown that road traffic injuries are a leading cause of Traumatic brain injury and neurotrauma worldwide, particularly in LMICs, thus proving that Neurosurgery is essential surgical care and trauma systems need to be enhanced [19]. Over the years the road safety initiatives of the WHO have shown improvement in various nations such as 79% reduction of road traffic fatality in Tanzania and implementation of stricter helmet and seatbelt laws with reduction of fatalities in Brazil, Ethiopia, Vietnam etc [20]. For example, WHO and UN road safety frameworks between 2004 and 2023 increasingly framed traumatic brain injury as a preventable burden, indirectly positioning neurosurgical care as an essential component of emergency response systems.
Capacity-building and NGO collaboration
While intergovernmental policies provide global direction, their implementation has relied heavily on hybrid NGO–government collaborations. Integrating neurosurgeons’ efforts for advocacy through research on existing global neurosurgical inequities has driven global politics in the healthcare domain. The WHO has launched several projects over the years to address some of these issues at a global scale, such as the WHO Global Initiative for Emergency and Essential Surgical Care in 2005 (GIEESC) [21] aims to reduce preventable death and disability from surgical conditions by improving emergency and essential surgical care in resource-limited settings. Although less frequently highlighted, these groups are doing critical work by advocating for neurosurgical access in LMICs and are steadily strengthening their position due to their advocacy and policy engagements. They focus on mobilizing resources and building capacity to close the gap in essential neurosurgical services [10, 22–24].
An example of this is found in Colombia’s development of a resource-stratified traumatic brain injury (TBI) management protocol (Beyond One Option for Treatment of Traumatic Brain Injury: A Stratified Protocol- The BOOTStraP) [25]. This protocol provides practical, resource-stratified algorithms for TBI care at all stages: prehospital, emergency department, surgery, and intensive care. The IGAP [26] in 2022, which focuses on transforming global care for epilepsy and neurological disorders by setting clear objectives and targets for countries to achieve over the next decade, with a strong focus on equity, multisectoral action, and measurable progress. The 76th WHA resolution on food micronutrient fortification [27] in 2023, which solidified a global commitment to accelerate and expand food micronutrient fortification aims to prevent congenital disabilities, such as spina bifida, and other health consequences of vitamin and mineral deficiencies through evidence-based, large-scale interventions The resolution also supports the development of National Surgical,* Obstetric*,* and Anesthesia Plans (NSOAPs)* [28] for countries by developing national blueprints for expanding and improving surgical, obstetric, and anesthesia care, aiming to reduce preventable death and disability by integrating these services into national health systems and policies.
The developments would not have been possible without such collaboration, which has bettered the clinical setup in regions where the burden of disease for neurosurgical services is high but the provision of care is poor [29]. On the NGO side, organizations like the Global Neurosurgery Committee (GNC) of the World Federation of Neurosurgical Societies (WFNS), The Lancet Commission on Global Surgery, GNI of the PGSSC at Harvard Medical School, Global Alliance for Prevention of Spina Bifida (GAPSBiF), G4Alliance etc. have been of importance in launching these efforts. Still, significant challenges remain in improving data collection systems [2, 6, 15, 30].
Persistent barriers to implementation
Despite the encouraging developments, there are still considerable challenges to advancing Global Neurosurgery. The diverse barriers to implementing these policies are particularly apparent in Sub-Saharan Africa, where there is a lack concrete national policies or strategies for neurosurgery-oriented services, due to lack of governmental funding for healthcare, training, infrastructure and resource resulting in high out-of-pocket expenditure for patients, lack of neurosurgical but also affiliated specialty workforce such as nurses, anesthesiologists, neurologists, intensive care units, bioengineering etc [31]. One of the most persistent barriers is the limitation of funding. Although the WHO’s Emergency and Essential Surgical Care Program has successfully advocated for neurosurgery, most countries still lack the resources to build neurosurgical units or train enough specialists [13, 32]. Sub-Saharan Africa remains a critical region where neurosurgery is severely under-resourced, with fewer than one neurosurgeon per 1.8 million people, far below the WHO’s recommended threshold of one per 100,000 [15, 33].
Another significant issue is the unavailability of dependable data, essential for effective policymaking and resource allocation. Many LMICs still lack the infrastructure to capture epidemiological data on TBI, cerebrovascular accidents, and other neurosurgical conditions. Without reliable data, governments and international organizations face difficulties formulating evidence-based policies, becoming aware of the economic impact of lacking specific policies, such as TBI, etc., and allocating resources where they are most needed [34–36]. The NGO, Mission: Brain and their Global Neurosurgery Research Group (GNRG) have fostered collaboration with the Sierra Leone Ministry of Health to bridge the gap with these services. Significant challenges remain in improving data collection systems, including technological and economic challenges [2, 6, 15, 30]. Infrastructure difficulties, such as lack of reliable water and electricity, transportation, weak healthcare systems, political instability, and allocation of resources, also limit timely access to neurosurgical care [13].
Future directions and evolving global leadership
Despite these constraints, several developments indicate emerging resilience and renewed global momentum. Looking ahead, the Boston Declaration (April 2025) marks a significant step forward in fostering global leadership in neurosurgery and integrating it fully into the health sector. Governments will continue to play a central role in advancing the field of Global Neurosurgery and prioritization of collaboration of NGOs and academic institutions with national health systems.
There is still a need for increased training opportunities, improved healthcare infrastructure in LMICs, and innovative capacity building strategies to ensure that neurosurgical services remain sustainable in these regions. The role of international partnerships will remain crucial. The success of partnerships and the collaboration between government agencies provides a strong model for future cooperation between governments and global agencies. Moreover, strategic investments in data systems will allow governments and international agencies to track and assess the impact of neurosurgical interventions more effectively. Sadly, the recent development of US withdrawal from the WHO in January 2026 will affect funds to support WHO projects, as the US contributes 14% to the WHO’s budget [37]. The US has cut USAID funding, research funding, and support of institutions such as the National Institute of Health (NIH) and the Centers for Disease Control and Prevention (CDC). These cuts have significant effect on the reduction of other UN agencies budgets such as the United Nations Children’s Fund (UNICEF), United Nations High Commissioner for Refugees (UNHCR), United Nations Population Fund (UNFPA), World Food Program (WFP), etc., resulting in a budget reduction between 20 and 60% [38–41]. The US also withdrew from supporting Sustainable Development Goals (SDGs), including SDG3 on health. The US withdrawal from the WHO will most likely lead to an increase in nations’ healthcare system disruptions, reduction in training of specialists, resource development, and research in already marginalized regions, further increasing healthcare disparities. This hurdle emphasizes the necessity of collaboration with NGOs and academic institutions in LMICs to maintain the growth of Global Neurosurgery.
Conclusion
In conclusion, the role of governments and international organizations in Global Neurosurgery cannot be overstated. These stakeholders are instrumental in developing policies, securing funding, and promoting partnerships that make neurosurgical care available to underserved populations. However, significant challenges remain, particularly regarding funding, data collection, and the persistent shortage of neurosurgical services in LMICs. The Boston Declaration (2025) provides a significant opportunity to highlight and advance the Global Neurosurgery agenda by strengthening policies and forging new international partnerships. In the coming years, governments and international organizations will need to pursue advancement of neurosurgical education, increased neurosurgical capacity and infrastructure, and creation of data management systems. Only through these concerted efforts will Global Neurosurgery be able to raise the needs of underserved populations in LMICs and ensure more equitable access to neurosurgical care.
Supplementary information
Below is the link to the electronic supplementary material.ESM 1(DOCX 14.8 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organization WH (2015) Strengthening emergency and essential surgical care and anaesthesia as a component of universal health coverage (Resolution WHA 68.15). [Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA 68-REC 1/A 68_R 1_REC 1-en.pdf
- 2Organization WH, World report on road traffic injury prevention (2004) : Road Safety Timeline; 2004 [Available from: https://www.who.int/teams/social-determinants-of-health/safety-and-mobility/road-safety-timeline#year-2004
- 3Organization WH, WHO Global Initiative for Emergency and Essential Surgical Care (2021) [Available from: https://www.who.int/initiatives/who-global-initiative-for-emergency-and-essential-surgical-care
- 4Chaubey S World Health Organization’s funding and the United States withdrawal 2025 2025/01/24/. Available from: https://ddnews.gov.in/en/world-health-organizations-funding-and-the-united-states-withdrawal/
- 5USA U. GLOBAL FUNDING CRISIS: AID CUTS ANYWHERE THREATEN SECURITY AND PROSPERITY EVERYWHERE (2025) [Available from: https://www.unicefusa.org/stories/global-funding-crisis-aid-cuts-anywhere-threaten-security-and-prosperity-everywhere
- 6UNFPA United States Government cuts future funding for UNFPA 2025 [Available from: https://www.unfpa.org/united-states-government-cuts-future-funding-unfpa
- 7UNHCR Faces Sharp US-Driven Budget Cut as Global Displacement Peaks. (2025) [Available from: https://www.indiatracker.in/story/unhcr-faces-sharp-us-driven-budget-cut-as-global-displacement-peaks
- 8Nichols M UNICEF projects 20% drop in 2026 funding after US cuts 2025 21 June 2025 Available from: https://www.reuters.com/world/unicef-projects-20-drop-2026-funding-after-us-cuts-2025-04-15/