A novel adaption to suction-assisted seroma aspiration
MA Langford, W Chow, P Kalu, J Birch

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1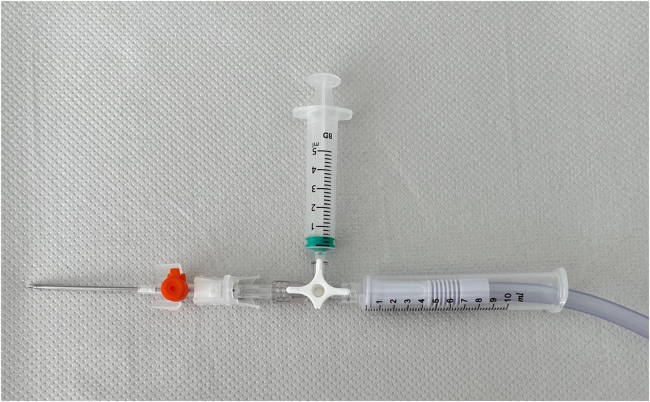 Figure 2
Figure 2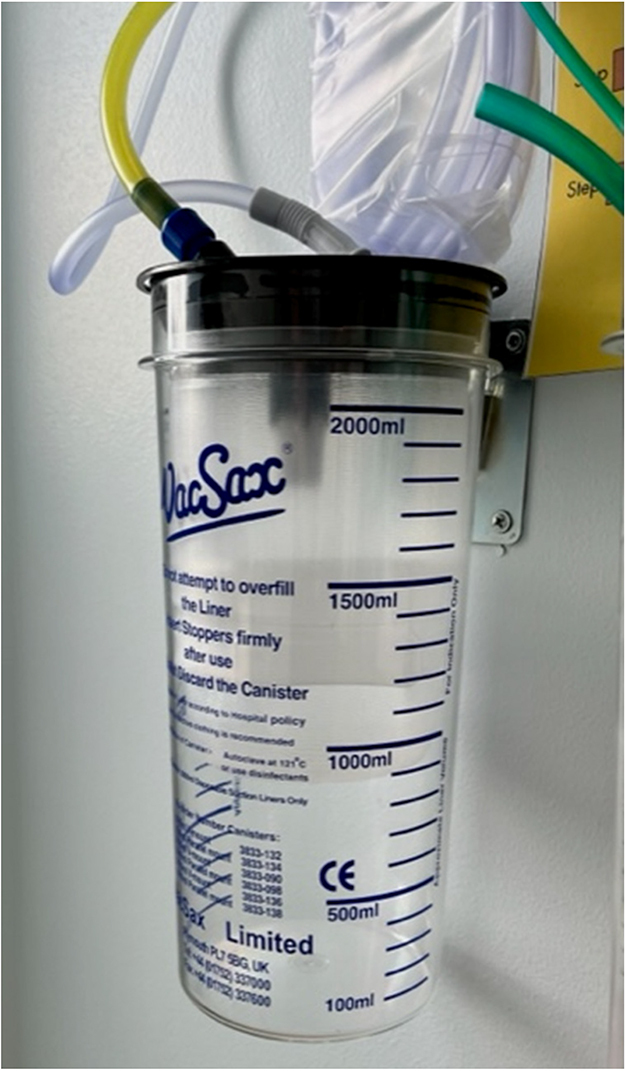 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Implant and Reconstruction · Body Contouring and Surgery · Lymphatic System and Diseases
Background
Seroma formation is a common sequela of lymph node dissection and autologous breast reconstruction.^1^ Simple syringe aspiration of a seroma can be cumbersome and physically tiring, and has led to the description of augmented techniques.^2,3^ Here, we document our modification of a previously described technique to aid in the location, drainage and, if required, sampling of seroma fluid.^3^
Technique
The seroma is assessed clinically and an ideal site for puncture is identified, with or without an ultrasound scan. The equipment used for this is shown in Figure 1. Using an aseptic technique, a 14G cannula is placed on one end of a three-way-tap. The second port is connected to a 5ml syringe, and the third port is connected to a 10ml syringe, with the plunger removed to allow the end of simple suction tubing to be placed snugly in the lumen.
The skin is punctured with the canula and then attached to a three-way tap opened to the 5ml syringe. Using gentle manual vacuum suction via the 5ml syringe, the seroma cavity is entered, as confirmed by a flashback of seroma fluid, and appropriate samples for laboratory examination are prepared. The three-way tap is then turned to the 10ml syringe with one end of the simple suction tubing placed inside the syringe (Figure 2), while the other end is connected to wall suction (Figure 3). The needle is left in the cannula to allow telescoping into deeper aspects of the cavity using a softer tip. Suction strength can be altered depending on the success of aspiration, the viscosity of the aspirate and patient comfort.
Constituent pieces required for the technique. Clockwise from top: 14G cannula, 5ml syringe, three-way tap, 10ml syringe with plunger removed and suction tubing.
Constituent parts assembled for use
Attachment to wall suction, with visible markings to allow measurement of aspirated fluid
Discussion
Compared with the previously described vacuum wound drainage system, wall suction improves efficiency and reduces the physical strain on the operator's hands. We use a cannula instead of an angiocatheter to allow telescoping, with a softer end reaching the deeper aspects of any cavity. This method is easy to replicate and is more efficient than manual aspirations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Merchant A, Speck NE, Michalek M et al. Comparing seroma formation at the deep inferior epigastric perforator, transverse musculocutaneous gracilis, and superior gluteal artery perforator flap donor sites after microsurgical breast reconstruction. Arch Plast Surg 2022; 49: 494–500.35919555 10.1055/s-0042-1751103 PMC 9340184 · doi ↗ · pubmed ↗
- 2Fitzgerald JEF, Hayes AJ, Strauss DC. Vacuum-assisted sterile drainage of large post-operative seromas: the Royal Marsden technique. Ann R Coll Surg Engl 2011; 93: 646.
- 3Park JE, Nigam M, Shenag DS, Song DH. A simple, safe technique for thorough seroma evacuation in the outpatient setting. Plast Reconstr Surg Glob Open 2014; 2: e 212.25426395 10.1097/GOX.0000000000000179 PMC 4229271 · doi ↗ · pubmed ↗