Biological Indicators of Cardiovascular Health by Foster Care History in Adults
Darlynn M. Rojo-Wissar, Sean R. Womack, Tomas Baka, Adam P. Spira, Ryan D. Davidson, Eric S. Zhou, Candice A. Alfano, Chandra L. Jackson, Michael A. Grandner, Stephanie H. Parade

TL;DR
Adults who were in foster care as children have worse cardiovascular health, especially higher blood pressure, compared to those without foster care history.
Contribution
This study identifies cardiovascular health disparities in U.S. adults with a foster care history using nationally representative data.
Findings
Foster care alumni had lower overall cardiovascular health scores compared to non-alumni.
Foster care alumni had notably lower blood pressure health scores, indicating hypertension.
Protective factors like higher income did not reduce cardiovascular risks in foster care alumni.
Abstract
Childhood adversity contributes to adult cardiovascular health disparities, but the cardiovascular health of foster care alumni, who experience unique compounded stressors such as attachment disruption and environmental upheaval, is understudied. In this study, biological cardiovascular health indicators were described among U.S. adults with and without a foster care placement history. Cross-sectional data from 4,625 adults (representing 17,226,361 U.S. adults) approaching and in early midlife (2016–2018) from The National Longitudinal Study of Adolescent to Adult Health were used. Biological indicators of cardiovascular health included BMI, blood lipids, blood glucose, and blood pressure, which were each scored on a standardized scale of 0–100, with higher scores indicating better cardiovascular health. An unweighted average of these standardized scores was also computed.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
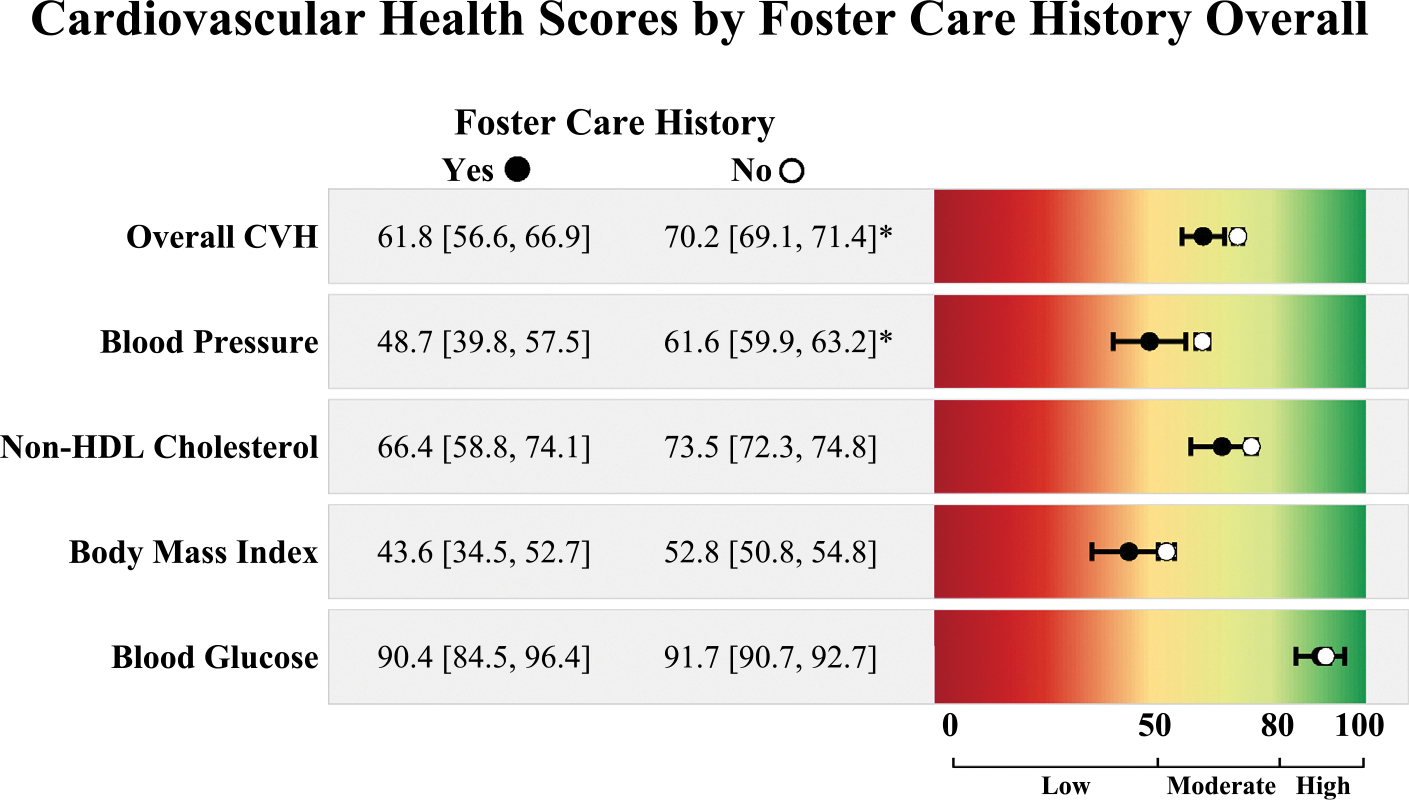 Figure 1
Figure 1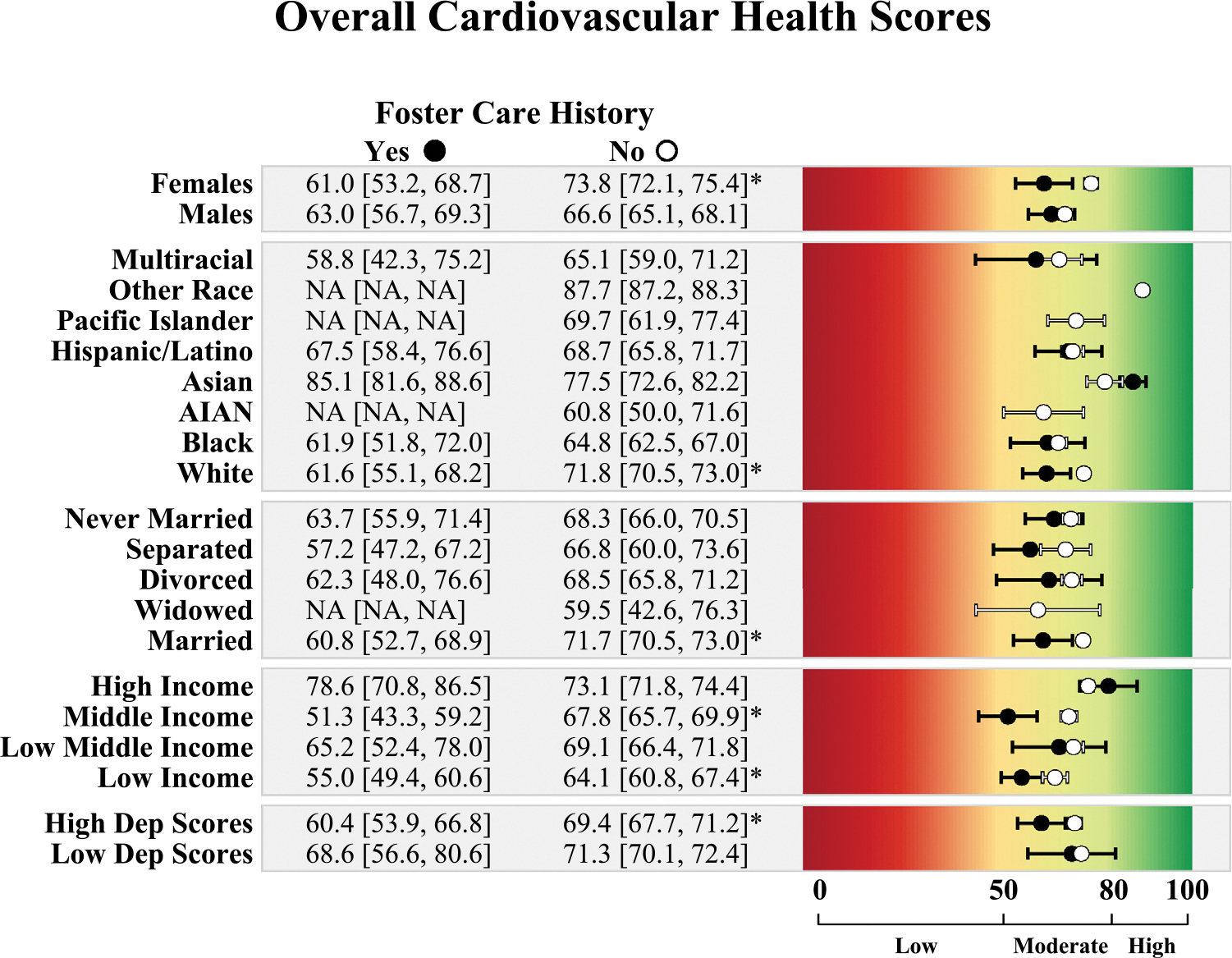 Figure 2
Figure 2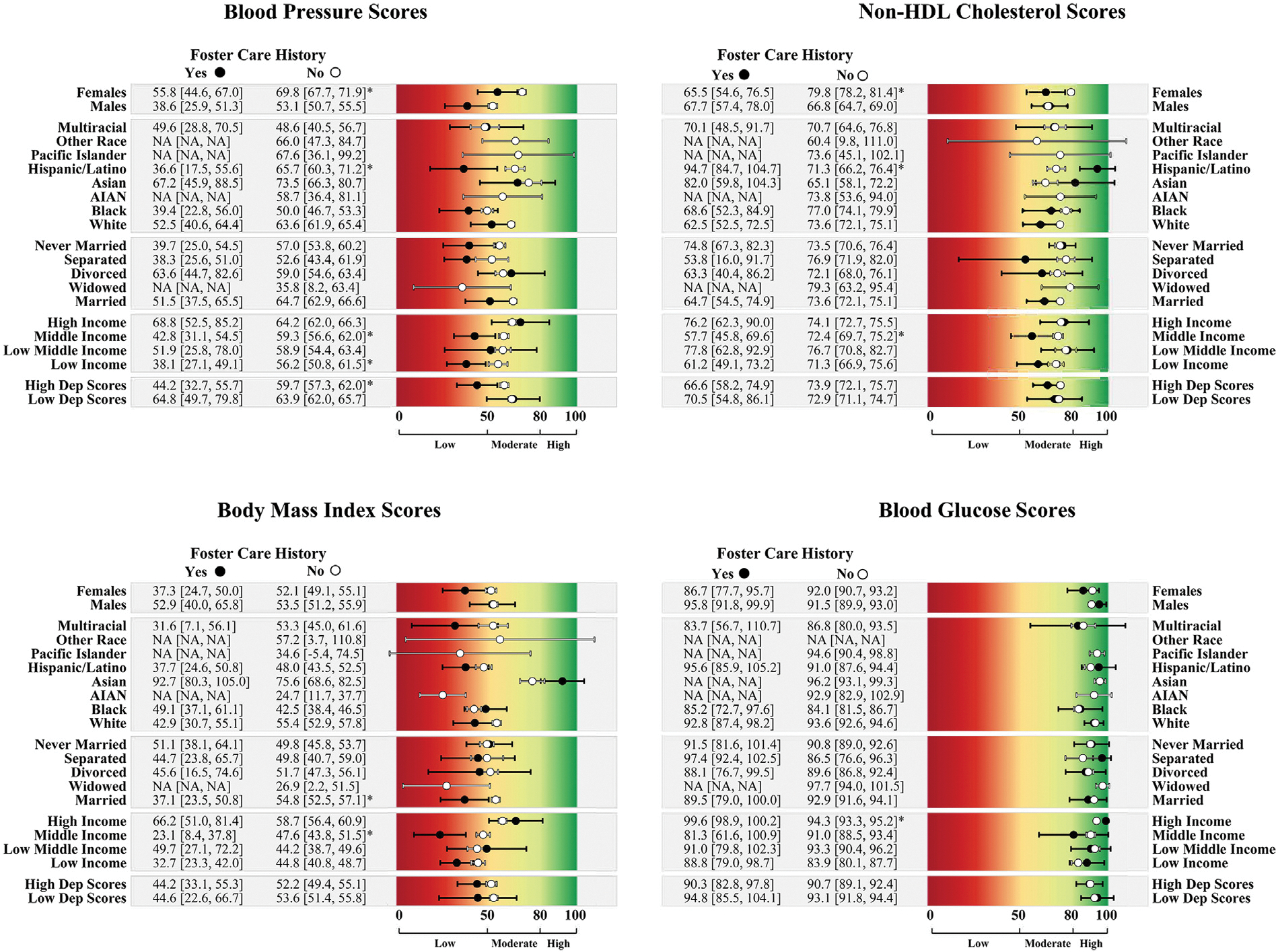 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health
INTRODUCTION
A recent American Heart Association (AHA) paper identifies a lack of attention to adversity in cardiovascular medicine research and practice as a major source of health disparities and emphasizes the need to invest in adversity-related science to improve cardiovascular health (CVH) nationally.^1^ The importance of childhood adversity, in particular, has been highlighted, defined as “subjectively perceived threats to the safety or security of the child’s bodily integrity, family, or social structures.”^2^ Although foster care (FC) is not directly mentioned in this scientific statement, it represents a population of over 400,000 children in the U.S.^3^ who face significant adversity. Compounded experiences of abuse, neglect, caregiver loss, environmental upheaval, and placement instability make this group a critical target for CVH research and intervention work. Indeed, adults with a FC placement history are 50%–100% more likely to develop cardiovascular disease (CVD).^4,5^ They are also more likely to experience CVD-related hospitalization and death than those who did not experience FC.^6^
Increased risk for CVD among those with a history of FC may occur through biological embedding of stress, which can result in substantial allostatic load, leading to dysregulation of metabolism, lipids, glucose, adipose tissue, and an increased risk of hypertension.^1^ Indeed, BMI, blood lipids, blood glucose, and blood pressure are key biological indicators of CVH^7^ and are not only associated with the development of CVD but also with a variety of other poor health outcomes,^8,9^ including mortality.^10^ Unfortunately, there is little research evaluating these key biological indicators of both the biological embedding of stress and of CVH risk in the FC population. The sparse work that does exist has largely neglected to examine these biological indicators objectively or as a reflection of health on a continuum and has instead often relied on self-reported diagnoses.^11–13^ Previous work is also limited by the grouping of people from several racial minority groups into a single other category, potentially obscuring important group differences.^11–13^ Addressing these knowledge gaps, especially in adults approaching and in early midlife, a developmental period directly prior to the average CVD onset,^14^ is vital for improving CVH and preventing CVD in individuals with a history of FC.
Data from the nationally representative National Longitudinal Study of Adolescent to Adult Health (Add Health) was used to describe multidimensional CVH in adults with and without a FC history. This included scores for objectively measured BMI, blood lipids (non–high-density lipoprotein [HDL] cholesterol), blood glucose, blood pressure, and an overall score across these domains. In the context of the limited available literature, it was hypothesized that these continuous biological indicators of CVH would generally be poorer among those with a history of FC placement than among those without a FC placement history. The prevalence of these biological indicators of CVH by relevant psychosocial factors^7,15,16^ was also explored to identify patterns and generate hypotheses for future research.
METHODS
Study Sample
The Add Health, which began recruitment of participants in Grades 7–12 during the 1994–1995 school year, is one of the largest and most comprehensive nationally representative longitudinal studies of American adolescents to date (N=20,745).^17^ Sampling for Add Health consisted of a school-based sampling design where high schools were selected through stratified sampling on the basis of factors such as school size, type, and census region.^18^
For the current analysis, data were used from Wave V (2016–2018), in which participants were aged 33–43 years (mean=37.13 [SE=0.12]), and relevant data on the biological indicators of CVH were collected to track the emergence of chronic disease as participants advanced in age. Anthropometric, cardiovascular, metabolic, and inflammatory measures were obtained through examinations and blood draws/tests. Other data were collected using a mixed-mode survey, with questionnaires administered through interviewer during home visits, by telephone, through the web, or by mail.^17^ There were 5,381 participants who completed the Wave V home examination and had a biomarker sample weight. The analytic sample consisted of 4,625 of these participants (Table 1) who also had a cluster variable to identify groups of students within the same schools, a poststratification variable to identify census region from when they were first recruited, and who had data on FC history (assessed in Wave III). This secondary analysis of deidentified data was deemed exempt from oversight by Brown University’s IRB.
Measures
Regarding the biological indicators of CVH, Add Health field examiners measured participant height and weight and blood pressure, collected health history and medication information, and collected venous blood samples from participants, which were assayed for lipid and glucose concentrations. These data were used to create standardized scores for each biological indicator (BMI, blood pressure, blood glucose, blood lipids [non-HDL cholesterol]) on a scale of 0 to 100 using AHA criteria. Scores on the 4 indicators were also averaged to create an overall CVH score, with higher scores indicating better CVH across all biological indicators. AHA scoring criteria were applied to these stress-related biological indicators of CVH (the 4 health factors in Life’s Essential 8)^7^ owing to its widespread adoption as a standardized way to measure individual components of CVH and CVH overall. Its large-scale use for monitoring population CVH and intervention effectiveness facilitates greater comparability of findings across studies, particularly in population-based research. The AHA scoring criteria also allow for comparability across the individual biomarkers by harmonizing the continuous measures into a standardized scale and incorporating key clinical considerations—such as disease status and medication use—into its scoring algorithm. The standardized scores are easy to interpret, and the scoring indexes have been widely validated in prior studies. For example, the 4 health factors are associated with the development of CVD and a variety of other outcomes, including dementia,^19^ advanced biological aging,^8^ depression,^9^ and both CVD-specific mortality and all-cause mortality.^10^ Although there is some evidence that overall CVH scores can be accurately estimated in situations where not all 8 metrics are available,^20^ the overall CVH score in this paper may be most representative of biological indicators of CVH. Additional measurement and scoring information are available in Appendix Tables 1 and 2 (available online).^7^
FC history status was retrospectively assessed with the question, Did you ever live in a foster home? Maltreatment in foster or adoptive care and the number of placements were also reported. Age was computed by subtracting participants’ birthdates from the date of their Wave V visit. Participants reported their biological sex assigned at birth (male, female), their race and ethnicity (categorized as non-Hispanic/Latino White, Black, American Indian or Alaskan Native, Asian, Pacific Islander, other race, multiracial, or Hispanic/Latino), and marital status (married, widowed, divorced, separated, never married). Poverty index scores (low income ≤1.30, low middle income of 1.31–1.85, middle income of 1.86–3.50, and high income >3.50) were computed using household annual income and size using federal poverty guidelines.^15^ The 5 items from the negative affect subscale of the Center for Epidemiologic Studies-Depression scale^21^ were used to assess total depressive symptoms. A dichotomous variable indicating those in the bottom and top 50% of scores (0/1) was used in analyses to approximate relative symptom burden in lieu of an established clinical cutoff.
Statistical Analysis
To generate unbiased estimates and retain national representativeness, design-based analyses incorporating sampling weights, school-level clustering, and regional poststratification were applied in STATA, Version 16.0 (StataCorp, College Station, TX). First, the sample was described; then, mean CVH indicators by FC history across contextual characteristics were estimated. Differences were considered meaningful if 95% CIs did not overlap. Finally, to further contextualize these findings, supplemental analyses were conducted among those with a FC history, examining mean CVH scores by maltreatment in foster or adoptive care and multiple placements. All available data were used; thus, sample sizes vary slightly owing to mostly minor missingness (Appendix Table 3, available online).
RESULTS
There were 113 participants (weighted n=313,604) with a FC placement history and 4,512 participants (weighted n=16,912,757) without a FC placement history (Table 1). Those with a FC history had a lower proportion of participants who were White or Hispanic/Latino of all races and a larger proportion who were Black and multiracial than those without a FC history. Those with a FC history also had a lower proportion of married participants; a higher proportion of divorced, separated, or never-married participants; and a greater proportion of participants in the lower ends of the poverty index and in the top 50% of depressive symptom scores.
Scores for the CVH outcomes are reported as mean (95% CI). Participants with a FC history had lower overall CVH scores (61.8 [56.6, 66.9]) than those without a FC history (70.2 [69.1, 71.4]) (Figure 1). For the individual biological indicators, blood pressure scores were significantly lower in adults with a FC placement history (48.7 [39.8, 57.5]; scores <50 indicative of hypertension) than in those without (61.6 [59.9, 63.2]). There were no meaningful differences in non-HDL cholesterol, BMI, or blood glucose scores by FC placement history, although non-HDL cholesterol and BMI were trending toward poorer health in those with a FC history. Finally, only 14.7% of those with a FC history had ideal CVH (i.e., no biological indicators of CVH in the low range [≤50]), compared with 27.4% without (p=0.049).
Stratified CVH scores by FC history and contextual factors are reported in Figures 2 and 3. Overall, CVH scores were lower among adults who were female, White, married, from low- and middle-income brackets, and in the top 50^th^ percentile of depressive symptom scores for those with a FC history than for those without.
Among individuals who were female, Hispanic/Latino, low-income, middle-income, and in the top 50^th^ percentile of depressive symptom scores, those who had a FC history had lower blood pressure health scores than those without a FC history. For blood lipids health, those with a FC history had a lower score than those without a FC history if they were female or in the middle-income bracket. Among Hispanic or Latino individuals, the opposite pattern emerged, where those with a FC history had better blood lipid health scores than those without a FC history.
BMI health scores were significantly lower in married adults with a FC history than in married adults without. Among middle-income adults, those with a FC history had significantly lower BMI health scores than those without. Counterintuitively, among those in the high-income range, those with a FC history had higher blood glucose health, although mean scores for both groups were in the high blood glucose health range.
CVH scores were generally similar regardless of maltreatment history in foster or adoptive care or number of FC placements. However, most individuals with a maltreatment history had notably lower blood pressure scores, all of which were within the low health range (Appendix Figures 1 and 2, available online).
DISCUSSION
Using data from a nationally representative sample of American adults approaching and in early midlife, reporting childhood FC involvement was associated with a greater risk for poorer CVH in this study. Findings also suggest that CVH disparities may be exacerbated when intersected with other relevant contextual factors (e.g., sex, race and ethnicity, SES). Current AHA guidelines recommend integrating psychosocial stressors and other social determinants of health in cardiovascular risk assessment and in the implementation of treatment recommendations for the prevention of CVD.^22^ Findings from this study support the consideration of FC history as a social determinant of CVD,^23^ which could improve cardiovascular risk assessment and open avenues for early interventions focused on alleviating the effects of exposure to adversity on long-term CVH. Investment in CVH promotion efforts in this population is critical for increasing health equity in this group at a disparately higher risk for CVD.
Identifying CVH risk factors prior to midlife is crucial. Although the prevalence of CVD is relatively low during this period,^14^ health factors that pose a risk for CVD (e.g., elevated blood pressure, obesity) are often present decades before disease onset.^24,25^ Adults with a FC placement history had meaningfully lower blood pressure health scores and CVH scores overall, implicating FC history as a potential risk factor for poorer CVH in early midlife. In the study sample, which is representative of over 17 million American adults aged 33–43 years, the mean blood pressure score for adults with a FC placement history fell in the hypertensive range. This finding is particularly concerning given that several studies have demonstrated that elevated blood pressure in young adulthood and early midlife increases the risk for CVD and related mortality in later life above and beyond traditional cardiovascular risk factors.^26–28^ This suggests that FC placement history represents an important social factor in the developmental course of hypertension and CVD.
Although scores on other biological indicators of CVH (i.e., lipids, glucose, BMI) were not significantly different for individuals who experienced FC relative to those who did not, blood lipid (non-HDL cholesterol) and BMI health scores were trending toward being significantly poorer among those with a FC history. Blood pressure may be more reactive and responsive to stressors experienced by children who are removed from their homes than to other biological indicators of CVH through its connection with the hypothalamic–pituitary–adrenal axis and sympathetic nervous system.^29,30^ FC-related stressors may affect other biological indicators of CVH more slowly over time and less directly. Future research will elucidate the part of the life course when trends toward non-HDL cholesterol and BMI differences by FC history become significant. Contrary to non-HDL cholesterol and BMI, blood glucose health scores were very similar by FC history. This could be explained by the homeostatic counterregulation that glucose levels are subject to, particularly with regard to insulin.^31^ The authors posit that among people in this age range, the body may still be compensating for stress-induced dysregulation through insulin’s modulatory effects, maintaining normal levels of blood glucose despite underlying physiological strain. Differences in blood glucose levels may be observable at much older ages than the other biological indicators of CVH.
Subgroup analyses by sex, race/ethnicity, income, marital status, and depressive symptoms revealed nuanced patterns in CVH differences by FC history. In brief, among those without a FC history, males had poorer CVH than females across most biological indicators of CVH, but this sex difference was not seen among those with a FC history—suggesting that FC may negate the protective effect of being female. Disparities in overall CVH by FC history were only evident among White adults, possibly owing to the cumulative stress experienced by racially minoritized groups. Among Hispanic adults, those with a FC history had poorer blood pressure health but better non-HDL cholesterol health than those without, which should be examined further in future research. Differences by income and marital status suggest that FC may undermine the protective effects of higher income and marriage. Among adults with high depressive symptoms, those with a FC history had poorer blood pressure health. When examining differences in CVH by traumatic FC experiences, it appeared that blood pressure health may be further negatively affected among people with a FC history if they also experienced maltreatment in foster or adoptive care. These hypothesis-generating findings are discussed further in the Appendix (available online) but should be interpreted with caution owing to small sample sizes in some subgroups. Future studies should examine whether findings across subgroups replicate in larger, more diverse samples of people with a history of FC placement. However, findings highlight a likely need for comprehensive support across multiple domains (e.g., relationship counseling, financial resources) for people who experience FC to ensure their well-being and successful development into adulthood.
Limitations
This study has limitations. First, FC placement history was assessed using a single self-report question, which may lead to measurement error related to recall bias, underreporting, or misclassification. For example, some people might not consider kinship placements to be FC, and some might not remember short-term placements. Second, important contextual information on placement history was absent, such as age of placement, re-entry into FC, duration of placement(s), and kinship versus nonrelative FC. These contextual factors should be examined in future studies and may be important in differentiating levels of risk and identifying potential protective factors associated with specific FC experiences. Third, CVH outcomes were limited to 1 time point, prohibiting the testing of developmental patterns of CVH, which should be examined in future studies to identify periods of risk and inform intervention timing. Despite the limitations, this study has several noteworthy strengths. First, the use of a large, diverse cohort study representative of over 17 million American adults is a strength. The study sample’s age range allowed to provide novel descriptions of biological indicators of CVH among adults approaching and in early midlife, prior to the typical age of CVD onset. Finally, measures of CVH were collected by trained phlebotomists during in-home assessments, which represents a methodologic advantage over studies that rely on self-reports of disease status.
CONCLUSIONS
In summary, experiencing FC placement in childhood may be a substantial social risk factor for poorer CVH in adults approaching and in early midlife, particularly with regard to blood pressure. Furthermore, this study provides evidence that FC history contributes to CVH disparities among adults within sociodemographic groups that are generally considered to be protected against developing CVH problems, such as females, people who have moderate to high income, and those who are married. AHA guidelines recommend incorporating childhood adversity and lifetime social stressors into CVD risk assessments.^22^ In light of these findings, the authors suggest the inclusion of FC placement. Targeted CVH interventions may be necessary to address the unique needs of the FC population. Because FC placement occurs during childhood and often coincides with an increased level of service involvement, there is potential for early intervention. Future longitudinal research among children and adults with a FC placement history is needed to confirm these findings, determine the mechanisms linking placement to poorer CVH outcomes, and identify key points of intervention. These efforts are crucial for mitigating CVH disparities and promoting health equity and wellness in this group.
Supplementary Material
Supplementary Materials
Supplemental materials associated with this article can be found in the online version at https://doi.org/10.1016/j.amepre.2025.108097.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Westcott SK, Lewis TT, Albert MA. Tackling adversity and cardiovascular health: it is about time. Circulation. 2023;147(1):e 1–e 3. 10.1161/CIRCULATIONAHA.122.061763.36576955 · doi ↗ · pubmed ↗
- 2Suglia SF, Koenen KC, Boynton-Jarrett R, Childhood and adolescent adversity and cardiometabolic outcomes: a scientific statement from the American Heart Association. Circulation. 2018;137(5):e 15–e 28. 10.1161/CIR.0000000000000536.29254928 PMC 7792566 · doi ↗ · pubmed ↗
- 3In foster care on the last day of FY. Children’s Bureau. https://cwoutcomes.acf.hhs.gov/cwodatasite/in Care September Thirty/index. Updated 2022. Accessed July 25, 2022.
- 4Batty GD, Kivimäki M, Almquist YB, Cardiovascular disease events in adults with a history of state care in childhood: pooling of unpublished results from 9 cohort studies. med Rxiv. Preprint. Online January 27, 2024. 10.1101/2024.01.26.24301814. · doi ↗
- 5Hjern A, Vinnerljung B, Brännström L. Cardiovascular disease and risk factors in individuals with a history of out-of-home care. Pediatrics. 2024;153(2):e 2023063174. 10.1542/peds.2023-063174.38263888 · doi ↗ · pubmed ↗
- 6Jackisch J, Almquist YB. Childhood adversity is associated with hospitalisations and survival following external causes and non-communicable diseases: a 46-year follow-up of a Stockholm birth cohort. J Epidemiol Community Health. 2023;77(4):209–215. 10.1136/JECH-2022-219851.36737239 PMC 10086507 · doi ↗ · pubmed ↗
- 7Lloyd-Jones DM, Allen NB, Anderson CAM, Life’s essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146(5):e 18–e 43. 10.1161/CIR.0000000000001078.35766027 PMC 10503546 · doi ↗ · pubmed ↗
- 8Zhang R, Wu M, Zhang W, Association between life’s essential 8 and biological ageing among U.S. adults. J Transl Med. 2023;21(1):622. 10.1186/s 12967-023-04495-8.37710295 PMC 10503107 · doi ↗ · pubmed ↗