Angioleiomyoma: How to Suggest the Diagnosis on Imaging?
Elena Enriquez, Filip M. Vanhoenacker

TL;DR
This paper explains how to diagnose angioleiomyoma, a benign tumor, using imaging techniques like ultrasound and MRI.
Contribution
The paper highlights the characteristic imaging features of angioleiomyoma to aid in its diagnosis.
Findings
Angioleiomyoma has distinctive features visible on ultrasound.
MRI also shows characteristic signs of this benign tumor.
These imaging traits help distinguish it from other superficial tumors.
Abstract
Teaching point: An angioleiomyoma is a benign superficial tumor that presents with relatively characteristic features on US and MRI.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
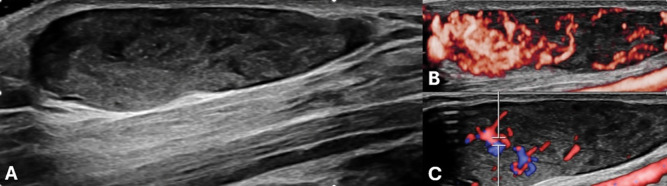 Figure 1 A–C
Figure 1 A–C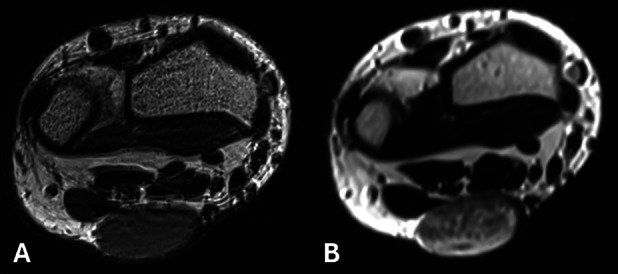 Figure 2 A–B
Figure 2 A–B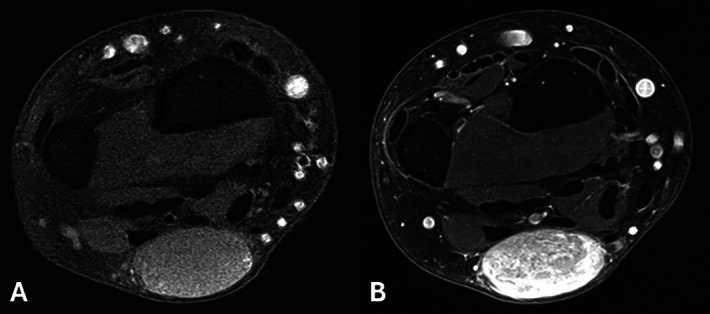 Figure 3 A–B
Figure 3 A–BPeer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumors and treatment · Vascular Tumors and Angiosarcomas · Soft tissue tumor case studies
Case
A 40-year-old man presented with a slow-growing soft tissue lump on the palmar side of the left wrist accompanied by cold-induced pain for over 6 years.
Grey-scale ultrasound (US) demonstrated an oval hypoechogenic lesion with tiny intralesional anechoic foci superficial to the flexor fascia (Figure 1A). Subsequent power Doppler and color Doppler showed extensive vascularization (Figure 1B) with arterial and venous signals (Figure 1C).
Doppler-Ultrasound: hypoechogenic lesion with tiny intralesional anechoic foci and extensive vascularization.
Magnetic resonance imaging (MRI) revealed a well-defined lesion, appearing slightly hyperintense compared to muscle on T1-weighted images (WI) (Figure 2A) and slightly heterogeneous hyperintense on T2-WI with multiple hypointense foci (Figure 2B) and a subtle incomplete peripheral rim of low signal. After intravenous administration of gadolinium contrast, marked enhancement of the lesion was seen (Figure 3A-B).
MRI. The lesion is slightly hyperintense compared to muscle on T1-WI and heterogeneous on T2-WI.
MRI. T1-WI before and after gadolinium contrast shows marked enhancement.
Since malignancy could not be definitively ruled out, a biopsy was performed. The diagnosis of angioleiomyoma was made.
Comment
An angioleiomyoma is a benign tumor arising in the subcutis or dermis almost always located at the extremities [1]. It originates from the smooth muscles of blood vessels and can be categorized into three subtypes (solid, venous and cavernous), depending on the predominant type of vessel involved. The lesion mostly presents in the fourth to sixth decades of life. An angioleiomyoma grows slowly and may be painful [1].
The etiology of an angioleiomyoma is unknown. The differential diagnosis includes neural sheath tumors, hemangiomas, inclusion epidermoid cysts, tenosynovial giant cell tumors, among others [1].
Conventional radiographic and computed tomographic (CT) scans are nonspecific. Intralesional calcifications are rare [1].
Ultrasound shows a superficial, well-defined, predominantly hypoechogenic lesion with tiny anechoic foci, which correspond to vessels [1]. The lesion is hypervascular on Doppler with mixed arterial and venous signals. Sometimes a feeding vessel can be visualized [1].
MRI likewise demonstrates a superficial and well-defined lesion, which is typically isointense or mildly hyperintense compared to skeletal muscle on T1-WI. On T2-WI, an angioleiomyoma is of intermediate to high signal with intralesional hypointense foci, which may result in a dark reticular appearance [1]. These foci are related to thrombosed small vascular structures or fibrous tissue. A peripheral dark rim may be seen on both pulse sequences. Vivid homogeneous or heterogeneous enhancement is seen [1].
The combination of a slow-growing superficially located and well-defined mass at the extremities, the presence of a dark reticular sign and peripheral dark rim on T2-WI and the hypervascular nature may be useful to suggest an angioleiomyoma in the differential diagnosis [1].
However, as imaging features are not pathognomonic, histological examination is recommended. Surgical excision is the treatment of choice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.