Physiotherapy interventions in post- and long-COVID-19: a scoping review of the literature up to February 2023
Judith Gartmann, Christian Sturm, Andrea Bökel

TL;DR
This review summarizes physiotherapy interventions for post- and long-COVID-19, identifying key areas like respiratory therapy and strength training.
Contribution
The study provides a scoping review of physiotherapy interventions for post- and long-COVID-19 up to February 2023.
Findings
Six studies were included, focusing on physiotherapy management for post- and long-COVID-19.
Respiratory therapy, aerobic training, and strength training are highlighted as key intervention areas.
The review emphasizes the need for further research on physiotherapy treatments for this condition.
Abstract
Physiotherapy is an accepted and recommended treatment for post- and long-COVID-19 condition. It is assumed that physiotherapists reported a lack of information on physiotherapy interventions and treatment parameters. This scoping review provides an overview of the evidence on physiotherapy interventions published in the scientific literature. The scoping review includes studies analysing physiotherapy treatment parameters and interventions in post- and long-COVID patients. Studies focusing on telemedicine or exclusively home-based workouts are excluded. A systematic literature search was conducted by two independent researchers in the databases PubMed, EBSCO, SCOPUS, Web of Science, EMBASE, PEDro, Cochrane, and WISO. Following the abstract screening process, data extraction and critical assessment were performed. In this scoping review, 6 studies were included, providing information…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
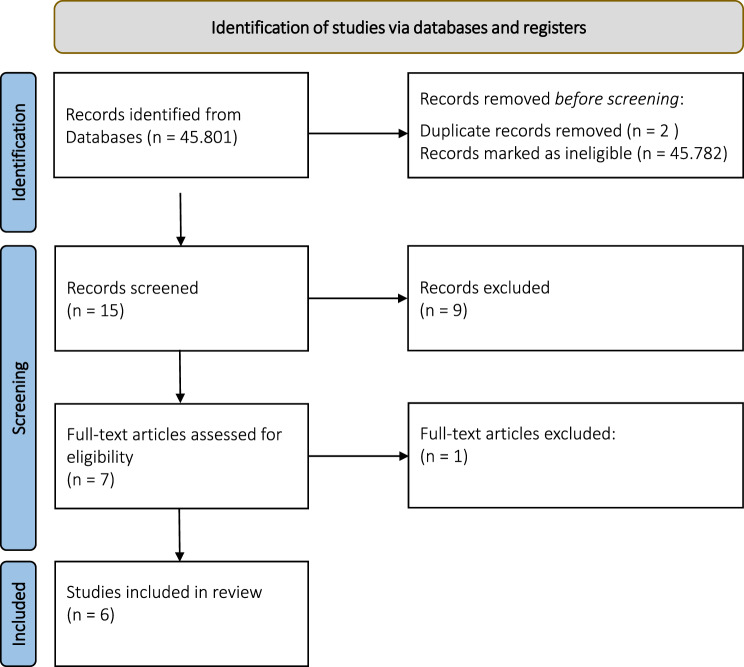 Figure 1
Figure 1- —Medizinische Hochschule Hannover (MHH) (3118)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · Chronic Obstructive Pulmonary Disease (COPD) Research · COVID-19 Clinical Research Studies
Background
The prevalence of long-COVID varies across different studies, ranging from 12.7 and 43% depending on the source [1–3]. Various systematic reviews and meta-analyses have concluded that long-COVID is more prevalent in hospitalised adults with severe cases of COVID-19 than in those with milder cases that do not require hospitalisation [3, 4]. Patients with long-COVID can exhibit a wide range of symptoms. The most common symptoms are fatigue (47%), dyspnoea (32%), myalgia (25%), joint pain (20%), headache (18%), cough (18%), and chest pain (15%) [5]. Due to this wide variety of symptoms and the numerous potential comorbidities, many authors recommend a multimodal, multidisciplinary and individually tailored rehabilitation approach [6, 7] which also includes physiotherapy and symptom self-management. Treatment is symptom-oriented [8, 9]. As physiotherapy interventions show positive effects in the treatment of symptoms of chronic obstructive pulmonary disease [10–12], fibromyalgia [13] or HIV [14, 15] it is a worldwide accepted and recommended treatment in rehabilitation.
Physiotherapists working in outpatient practices are uncertain about how to treat the long-term effects of the COVID-19 virus [16].
A preliminary search on physiotherapy interventions was conducted in 2021 using the following databases: PubMed, Pedro, Embase and Cochrane Database. The search revealed no current or ongoing systematic or scoping reviews on the topic of physiotherapy treatment parameters. Nevertheless, the preliminary search demonstrated that multidisciplinary rehabilitation in infectious diseases and physiotherapy is a recommended treatment for post- and long-COVID symptoms, including pulmonary symptoms and pain [17–24].
Systematic reviews conclude that rehabilitation using an exercise programme could improve both physical and psychological outcomes [25, 26] as well as quality of life [27]. However, the relevant training guidelines regarding the frequency, intensity, timing and type of exercise for long-term rehabilitation are not yet fully clear [25, 26]. Therefore, high-quality clinical studies need to be developed and implemented [18, 22, 28–31]. Due to the lack of studies to date, rehabilitation is partly based on expert opinion [32] and on research into rehabilitation methods proven to be effective in treating similar symptoms in different contexts [16, 33].
This scoping review aimed to summarise the available evidence on physiotherapy interventions and treatment parameters for managing patients with post- and long-COVID conditions.
Methods
This scoping review was registered in on Open Science Framework (Registry number http://osf.io/5k3tA). As no patients and public were involved a positive vote of an ethical committee was not necessary.
The proposed scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews [34, 35]. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist extension for scoping reviews was used for reporting [36].
The methodological framework provided by the JBI was used. This methodological framework includes several steps from defining the research question and the eligibility criteria, conducting the literature research, study selection and data extraction. Additionally, a critical appraisal was conducted using the JBI critical appraisal tools. The quality of the methodology of the selected studies was evaluated with regard to the extracted data.
Review question
The primary question guiding this scoping review is ‘What kind of physiotherapeutic interventions are used in both outpatient and inpatient settings for post- and long-COVID-19 patients?’ This question is divided into subquestions, as illustrated in Table 1. Table 1. Sub-questions of the scoping reviewPerspectiveResearch questions(1) Descriptivea) How many studies were published between January 2020 and February 2023 on physiotherapy interventions in patients with post- or long-COVID-Syndrome?(2) Methodsa) Which research methods were used in the published literature?b) What population characteristics were described in the published literature?c) What definitions of post- and long-COVID-19 were used in the published literature?(3) Physiotherapy interventionsa) What types of physiotherapy interventions were reported in the published literature?b) What was the reported frequency of the physiotherapeutic interventions?c) What was the reported intensity of the physiotherapeutic interventions?(4) Physiotherapy and Post-/Long-COVIDa) What was the impact of physiotherapy on post- or long-COVID-19 symptoms?b) Were adverse events reported for physiotherapeutic interventions in patients with post- or long- COVID syndrome?c) Were negative influences reported for parallel, applied physiotherapeutic interventions in patients with post- or long-COVID syndrome?d) Were differences reported in- and outpatient interventions?
Eligibility criteria
The decision to include only German and English language studies in this study was based on the authors’ proficiency in both, thus allowing for a more accurate analysis and interpretation of the data. Studies addressing post-COVID, post-acute COVID and long- COVID were included. Studies that also examined acute COVID-19 or COVID-19 in general were only considered eligible if the results pertaining to post- COVID, post-acute COVID or long- COVID were reported separately and in a comprehensible format. Randomised controlled trials, observational studies, case reports, umbrella reviews, rapid reviews focusing on post- and long-COVID-19 in adults were considered for inclusion in this scoping review, when published between January 2020 and February 2023. Qualitative studies were excluded due to the quantitative nature of the analysis in this study, which focuses on treatment details. Grey literature, text and opinion papers were not considered for inclusion in this scoping review.
Studies analysing telemedicine and solely home-based workouts were not included in this study because the telemedicine approach has not yet been widely established in German physiotherapy care.
Eligibility criteria are shown in Table 2. Table 2. Eligibility criteriaInclusion criteriaExclusion criteriaLong-COVID-19Post-COVID-19Post-acute COVIDAdult patients aged above 18 yearsPhysiotherapy interventionsPhysiotherapy interventions with additional home exercise workoutRandomised controlled trials, observational studies, case reports, umbrella reviews, rapid reviewsGerman or English languagePublication date between January 2020 and February 2023Acute COVID-19Non-COVID-19Other infectious diseasesOther respiratory disordersNon-systematic reviewsStudy protocolsEditorials, lettersNarrative reviewsQualitative studiesGrey literatureChildren and adolescent patients aged under 18 yearsTelemedicineSolely home-based workouts
Sources
Databases PubMed, EBSCO, Scopus, Web of Science, Embase, PEDRO, Cochrane and WISO were searched by two independent researchers. A professional librarian was not involved.
Search strategy
The search strategy is focused on published studies. The primary search strategy is based on the 4 domains of population, physiotherapy intervention, outcome, study design shown in Table 3. The secondary search strategy involves the combination of these domains: ‘population AND physiotherapy intervention’, ‘population AND physiotherapy intervention AND outcome’, and ‘population AND physiotherapy intervention AND outcome AND study design’. Table 3. Search terms and MeSHDomainSearch termsMeSH termsPopulationLong-COVID, post-COVID-19,Post-acute COVID”Post-acute COVID-19 syndrome”Physiotherapy interventionPhysiotherapy, aerobic exercise, physical activity, resistance training, passive mobilisation, active mobilization, manual therapy, massage therapy, lymphatic drainage, electrotherapy, ultrasound, respiratory therapy, proprioceptive neuromuscular facilitation (PNF), Vojta, Bobath, pressure ulcer management, prevention“Physical therapy modalities“OR “Physical therapy specialty“OR”Exercise therapy” OR “Exercise movement techniques” OR “Physical fitness“OR “Musculoskeletal manipulation” OR “Relaxation” OR “Stress, physiological” OR “Immobilisation” OR “Prevention & control” OR “Manual lymphatic drainage“OR “Electric stimulation therapy“OR “Ultrasonic therapy“OR “Respiratory therapy“OR “Breathing exercises“OutcomePhysical fitness, fatigue, general health, pain, return to work, physical health, mental health, mobility, vital capacity, dyspnoea, myalgia, arthralgia, functional capacity, health-related quality of life, stress, range of movement, patient-reported outcome measures“Physical fitness“OR “Fatigue“OR “Mental health” OR “Return to work“OR “Pain management” OR “Vital capacity“OR “Myalgia“OR “Arthralgia” OR “Quality of life“OR “Patient-reported outcome measures“OR “Health” OR “Health status”Study designRandomised control trialObservational studiesCase reports“Randomised controlled trial” OR “Observational study” OR “Case reports”
The search terms and relevant keywords were identified and deposited with medical subject headings (MeSH) (Table 3). The strategies for the literature search are listed in the Appendix I.
Screening process
Two independent researchers collected the identified literature in separate Excel sheets and removed duplicates. Titles and abstracts were then screened by two independent reviewers to ascertain whether they met the inclusion criteria for the scoping review. Thereafter, the full-text articles that met the inclusion criteria in the title and abstract screening process were screened independently by the two researchers with the aim of identifying the inclusion criteria. The reasons for the exclusion of sources of evidence at full-text that do not meet the inclusion criteria were recorded and reported in the scoping review. In the next step both independent researchers compared their search results. Any disagreement was resolved through discussion or consulting with a third independent researcher.
Critical appraisal
Additionally, a critical appraisal of each included article was conducted by the two independent researchers using the JBI critical appraisal tools [37]. The quality assessment evaluated the methodological quality with regard to the extracted data on physiotherapy interventions and treatment parameters. Thereafter, both researchers compared the results of the critical appraisal. In the event of differences in the quality report the results were discussed or a third independent researcher was involved for reaching a consensus.
Data extraction
Data was extracted from the included papers by two reviewers independently using a data extraction tool that has been developed by the reviewers. The data extraction tool was created in MS Word providing specific details on the study design, research method, population characteristics, definition of post- and long- COVID-19, intervention and key findings relevant to the review question/s, e. g. these included frequency and intensity of the intervention, the outcome of the study and adverse events.
Results
The literature search was conducted in March 2023.
Descriptive
How many studies were published between January 2020 and February 2023 on physiotherapy interventions in patients with post- or long-COVID syndrome?
45.801 articles were screened on the inclusion criteria. 19 papers remained. After reduction of duplets 15 articles remained for the title and abstract screening process after which 9 studies were excluded. Finally, 6 studies were included in the scoping review (Table 4). A flow diagram can be found in Fig. 1 [38].Fig. 1. Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram [36]Table 4. Illustration of the included studiesNo.AuthorYearCountryStudy designObjectivePost-COVID-191Ali AA et al. [20]DOI: 10.47750/pnr.2023.14.S02.87.2023EgyptRandomized controlled trial,prospective, single-blinded, two groups, before and post-test analysis,’to determine how active cycle breathing affects specific pulmonary outcomes in patients having post-COVID syndrome.’ [20]2Nagy EN et al. [39]DOI: 10.2340/jrm.v54.3972.2022EgyptRandomized controlled trial,Study group and control group’to evaluate the combined effect of manual DR and IMT compared with IMT alone on selected parameters (blood pressure, dyspnoea, high serum lactate, and fatigue levels) in men with post-acute sequelae of COVID-19 syndrome.’ [39]3Nambi G et al. [19]DOI: 10.1177/0269215521103692022Saudi Arabia,Randomized, single-blinded,Low intensity aerobic training group (LAT) versus high intensity aerobic training group (HAT)prospective, clinical study’to find and compare the clinical and psychological effects of low and high-intensity aerobic training combined with resistance training in community-dwelling older men with post-COVID-19 sarcopenia symptoms.’ [19]4Rutkowski S et al. [40]DOI: 10.3389/fpubh.2023.1121554.2023Poland, United States of AmericaRandomized controlled trial;VR group versus control group both with 4 pulmonary rehabilitation models’to propose an innovative comprehensive intervention based on a pulmonary rehabilitation programme for patients with post-acute sequelae of COVID-19.’ [40]5Mayer KP et al. [21]DOI: 10.1093/ptj/pzab098.2021United States of AmericaCase Report’to present the clinical presentation and physical therapist management for a patient with post–COVID syndrome.’ [21]SARS-CoV-2: post-COVID-196Santos S et al. [24]DOI: 10.1002/pri.1938.2022PeruCase Reportdescribe ‘an intervention based on musculoskeletal physiotherapy in a post-COVID-19 adult woman with physical sequelae’. [24]
Methods
Which research methods were used in the published literature?
The majority of the studies were published in 2022 (n = 5) concentrating on ‘post-COVID-19’. No published study focusing on ‘long-COVID-19’was identified. One study used ‘SARS-CoV-2’ and defined the subtype of ‘post-COVID-19’ in the abstracts [24]. Two-thirds of the 6 included studies were randomized controlled trials (n = 4) [19, 20, 39, 40].
What population characteristics were described in the published literature?
The published population characteristics are shown in Table 5. Table 5. Population characteristics of the included studiesNo.AuthorPopulationHealthcare delivery settingPost-COVID-191Ali AA et al. [20]60 patients both sexes (31 female, 29 male), with difficulty in breathing during activities of daily living (dyspnoea, cough and sputum production)Age in years: 45.62 ± 2.47 versus 45.7 ± 2.33N. a.2Nagy EN et al. [39]52 men with post-COVID-19 syndrome,Age in years: 40.00 ± 3.36 versus 39.70 ± 3.55Outpatient3Nambi G et al. [19]65 men, post COVID 19 sarcopeniaAge in years: 63.2 ± 3.1 versus 64.1 ± 3.2N. a.4Rutkowski S et al. [40]32 patients (20 female, 12 male) with a confirmation from a primary care physician of having had COVID-19 infection,Age in years: 57,8 ± 4,92Inpatient5Mayer KP et al.[21]Woman 37 years old, day 62 after initial infectionOutpatientSARS-CoV-2: post-COVID-196Santos S et al.[24]Woman, 60 years old, 28 days after initial infectionOutpatient (home visit)
What definitions of post- and long-COVID-19 were used in the published literature?
Hardly any definitions for post- and long-COVID-19 were identified. The authors of the included literature referred to other authors and described the possible symptoms of this post infectious condition (Table 6). Table 6. Definitions of post- and long-COVID-19 used in the included studiesNo.AuthorDefinition post- and long-COVID-19Post-COVID-191Ali AA et al. [20]’ … PCS is a condition in which signs and symptoms persist for more than 4 weeks following an acute infection.’ [41]2Nagy EN et al. [39]No definition identified3Nambi G et al. [19]No definition identified4Rutkowski et al. [40]No definition identified5Mayer KP et al. [21]’two definitions of post-acute COVID-19 are given: (1) ongoing symptomatic COVID-19 for people who still have symptoms between 4 and 12 weeks after the start of acute symptoms; and (2) post-COVID-19 syndrome for people who still have symptoms for more than 12 weeks after the start of acute symptoms.’ [42]SARS-CoV-2: post-COVID-196Santos S et al. [24]No definition identified
Physiotherapy interventions
What types of physiotherapy interventions were reported in the published literature?
The research of physiotherapy management of post- and long-COVID-19 identified on the following key areas of focus: respiratory therapy [20, 21, 39, 40], aerobic training [19–21, 40] or strength training [19–21, 40]. One study reported ‘hands-on’ physiotherapy interventions like manual therapy and TENS [24]. The interventions are reported in Table 7. Table 7. Reported physiotherapy interventions and treatment parametersCategoryInterventionsFrequency and duration in therapyIntensityFrequency in generalSourceRespiratory therapyPost-COVID-19- Respiratory exercise with active cycle of breathing technique, controlled breathing,- thoracic expansion exercises, forced expiration technique,- active diaphragma release techniques,- pursed-lip abdominal breathing exercise- 2-3 times: 20–30 seconds controlled breathing, Thoracic expansion exercises 3–4 times, normal breath 20–30 seconds or 6 breaths- daily 3–4 times maximum of 3 min, 10 breaths, 20 seconds rest- 4-6 seconds1-3 sessions per week for 12 weeksAli AA et al. [20]- Diaphragm release- Inspiration muscle Training with tool2x 10 breaths, 1 minute rest4 min, twice a day 30 breaths, 2 min rest3 sessions per week for 6 weeksNagy EN et al. [39]- High-intensity pulmonary programme with breathing exercise5 sessions per week for 3 weeksRutkowski et al. [40]Diaphragm breathing techniques15 sessions in 8 weeksMayer KP et al. [21]Aerobic trainingPost-COVID-19- Treadmill20 minIncreased each day regarding to patients’ tolerability3 sessions per week for 12 weeksAli AA et al. [20]- Treadmill- Cycle ergometer20 min10 minLow-intensity aerobic training (40-60% of maximum heart rate) or high-intensity aerobic training (60-80% of maximum heart peak)4 sessions per week for 8 weeksNambi G et al. [19]- Cycle ergometer with or without Virtual RealityTwice a dayHeart rate increase of 90%/80%/70%/20-30%50-70 RPM5 sessions per week for 3 weeksRutkowski et al. [40]- Crosstrainer, treadmill, jogging, upper extremity bicycle ergometer- Dancing15-45 min3-6 min- Initial level 60-80% Heart rate max,Increased to mRPE scale 4/10 (somewhat hard) to 6/10 (hard)- cadence 80 bpm15 sessions in 8 weeksMayer KP et al. [21]Strength trainingPost-COVID-19- Active limb exercises with weight machines, free weights, elastic bands10 - 45 min3 sets of 8–12 repetition with progression to 15 repetitions, with 1 min rest1-3 sessions per week for 12 weeksAli AA et al. [20]- With weights3 times 10 repetitions, 1 min rest4 sessions per week for 8 weeksNambi G et al. [19]- General fitness exercises, resistance training and relaxation5 sessions per week for 3 weeksRutkowski et al. [40]- Weight machines, dumbbells, ankle weights, Core stability- Home workout with elastic bands10-20 min3 times per week 3x15 repetitions15 sessions in 8 weeksMayer KP et al. [21]‘Hands-on’ physiotherapyPost-COVID-19- Stretching for warm- up and cool-downNambi G et al. [19]SARS-CoV-2: post-acute COVID-19- StretchingFrom 4^th^ session on15 sessions in 5 weeks; 1:15 h - 1:50 hSantos S et al. [24]- Transcutaneous electric nerve stimulationAnalgesic type, tetrapolar, 20 min60-100Hz15 sessions in 5 weeks; 1:15 h - 1:50 hSantos S et al. [24]- Cyriax Deep Transverse Friction Massage bilateral brachial biceps and supraspinosus muscle15 sessions in 5 weeks; 1:15 h - 1:50 hSantos S et al. [24]- kinesitherapy4^th^ to 5^th^6^th^ to 10^th^11^th^ to 15thPassiveActivebody segment weight, increasing with 1/2 kg, 1 kg and up to 2 Kg15 sessions in 5 weeks; 1:15 h - 1:50 hSantos S et al. [24]- Maitlands’ manual therapy spine6^th^ to 10^th^ session15 sessions in 5 weeks; 1:15 h - 1:50 hSantos S et al. [24]
What was the reported frequency of the physiotherapeutic interventions?
The frequency varied from 3 to 12 weeks, with 1 to 5 sessions weekly, respectively [19–21, 24, 39, 40]. It is shown in Table 7.
What was the reported intensity of the physiotherapeutic interventions?
The intensity was not reported in every intervention. The intensity practiced found in the included literature is shown in Table 7 [20, 21, 24, 40].
Physiotherapy and post- and/or long-COVID-19
What was the impact of physiotherapy on post- or long-COVID symptoms?
Overall physiotherapy resulted in a change in health status parameters, including a reduction in fatigue levels, an improvement in respiratory function, and an enhancement in physical capacity. Arterial oxygen saturation and partial pressure of oxygen increased [20]. However, muscle mass remained unaltered [19]. The results are shown in Table 8. Table 8. Impact of physiotherapy on health status parametersHealth status parametersOutcomeOutcome scores or scalesStatisticsSourceFatigue↓Fatigue Assessment ScaleMean difference (% of change); p-valueGroup A 14.03 (35.92); 0.001Group B 23.6 (61.05); 0.001Ali AA et al. [20]Fatigue Severity ScaleMean difference (SD); p-valueStudy group from 43.36 (±5.25) to 28.68 (±6.01); < 0.001control group from 42.47 (±5.18) to 39.77 (±5.89); 0.001Nagy EN et al. [39]Borg scale while 6-minute walk testGroup Mean (median); p-valueVR group from 3.0 (1.0) to 2.0 (1.0); 0.055Control group from 3.0 (1.0) to 2.0 (1.0); 0.010Rutkowski et al. [40]↑Subjective descriptionN. a.Mayer KP et al. [21]Walking distance↑6-minute walk testMean difference (% of change); p-valueGroup A − 53.03 (11.09); 0.001Group B − 105.27 (21.61); 0.001Ali AA et al. [20]Mean difference (SD); p-valueStudy group 56.50 m 13.53%; < 0.001Control group from 16.50 m 3.92%; < 0.001Nagy EN et al. [39]Group Mean ± SD in m; p-valueVR group from 502 ± 48.8 to 558 ± 76; 0.010Control group from 512 ± 54.3 to 552 ± 49.1; < 0.001Rutkowski et al. [40]Difference: from 312 m to 511 m (+199 m)Mayer KP et al. [21]Arterial oxygen saturation↑Arterial blood gas analysisMean difference (% of change); p-valueGroup A − 2.4 (2.70); 0.001Group B − 5.7 (6.43); 0.001Ali AA et al. [20]partial pressure of oxygen↑Arterial blood gas analysisMean difference (% of change); p-valueGroup A − 2.62 (3.50); 0.001Group B − 9.25 (12.41); 0.001Ali AA et al. [20]partial pressure of carbon dioxide↓Arterial blood gas analysisMean difference (% of change); p-valueGroup A 1.64 (4.35); 0.001Group B 3.95 (10.75); 0.001Ali AA et al. [20]Arterial blood pressure↓SphygmomanometerMean difference (% of change); p-valueStudy groupSystolic blood pressure −25.00 mmHg (16.67); < 0.001Diastolic blood pressure −17.10 mmHg (18.08); < 0.001Control groupSystolic blood pressure −3.73 mmHg (2.48); 0.032Diastolic blood pressure −0.90 mmHg (0.95); 0.01Nagy EN et al. [39]Serum lactate level↓Veinous blood sampleMean difference (% of change); p-valueStudy group −0.82 mmol/L (51.57); < 0.001control group −0.27 mmol/L (17.65); < 0.001Nagy EN et al. [39]Muscle mass↔Magnetic resonance imagingMRI – mid arm in cm^2^Group Mean ± SD in kg; p-valueBaseline LAT 55.9 ± 1.7, HAT 56.3 ± 1.; 0.2274 weeks LAT 57.5 ± 1.0, HAT 57.9 ± 0.9; 0.0708 weeks LAT 58.9 ± 0.6, HAT 59.0 ± 0.5; 0.4326 months LAT 61.4 ± 0.5, HAT 61.5 ± 0.2; 0.256Nambi G et al. [19]MRI – mid thigh in cm^2^Group Mean ± SD in kg; p-valueBaseline LAT 63.4 ± 0.8, HAT 63.5 ± 0.8; 0.5874 weeks LAT 65.3 ± 0.6, HAT 65.5 ± 0.6; 0.1508 weeks LAT 68.4 ± 0.6, HAT 68.5 ± 0.6; 0.4696 months LAT 72.5 ± 0.8, HAT 72.6 ± 0.8; 0.587MRI - mid calf in cm^2^Group Mean ± SD in kg; p-valueBaseline LAT 60.2 ± 1.1, HAT 60.2 ± 1.1; 1.0004 weeks LAT 65.2 ± 0.6, HAT 65.2 ± 0.6; 1.0008 weeks LAT 66.3 ± 0.5, HAT 66.4 ± 0.5; 0.3866 months LAT 68.7 ± 0.5, HAT 68.7 ± 0.5; 1.000Kinesiophobia↓Tampa scale of kinesiophobiaGroup Mean ± SD; p-valueBaseline LAT 32.1 ± 1.0, HAT 32.3 ± 0.9; 0.3624 weeks LAT 23.5 ± 0.9, HAT 29.9 ± 0.9; 0.0018 weeks LAT 18.0 ± 0.9, HAT 24.5 ± 1.4; 0.0016 months LAT 13.5 ± 1.0, HAT 18.2 ± 1.0; 0.001Nambi G et al. [19]Risk of falls↑Timed-Up and Go TestFrom 9.0 s to 7.3 sMayer KP et al. [21]Functional status↑Short Performance Physical BatteryTotal from 11 to 12Mayer KP et al. [21]Quality of life↑Sarcopenia and Quality of Life questionnaireGroup Mean ± SD; p-valueBaseline LAT 57.3 ± 1.0, HAT 57.7 ± 1.0; 0.0854 weeks LAT 63.0 ± 0.7, HAT 58.8 ± 0.9; 0.0018 weeks LAT 69.0 ± 1.0, HAT 60.5 ± 0.8; 0.0016 months LAT 72.6 ± 1.0, HAT 62.2 ± 0.8; 0.001Nambi G et al. [19]↓Health-related Quality of Life Questionnaire (Eq-5D-5 L)Eq-5D-5 L (VAS 0–100): 50 to 40Eq-5D-5 L (mean): 2.6 to 2.8Mayer KP et al. [21]Cognitive function↑Montreal Cognitive Assessment27 to 28 (out of 30)Mayer KP et al. [21]↔Time-up and Go Test with cognitive componentFrom −34% to − 21% differenceDistress↑Impact of Events Scale-RevisedTotal: from 36 to 46Mean response: from 1.6 to 2.1Intrusion mean: from 1.6 to 1.9Avoidance mean: from 0.75 to 1.25Hyperarousal mean: from 2.8 to 3.5Mayer KP et al. [21]↓Perceived Stress ScaleGroup Mean ± SD; p-valueVR group from 23.1 ± 4.2 to 20.7 ± 3.5; 0.015Control group from 23.8 ± 3.1. to 22.2 ± 3.8; 0.004Rutkowski et al. [40]Lung function↔Spirometry(expiratory volume for 1 s (FEV_1_); forced vital capacity (FVC); forced expiratory volume in one second of vital capacity (FEV_1_/VC))Group Mean ± SD (mean); p-valueFEV_1_ in lVR group from 2.8 ± 0.66 to 2.77 ± 0.68; 0.708Control group from 2.72 ± 0.60 to 2.76 ± 0.61; 0.879FVC in lVR group from 3.46 ± 0.78 to 3.56 ± 0.8; 0.087Control group from 3.49 ± 0.86 to 3.5 ± 0.85; 0.168FEV_1_/VC in %VR group from 84.3 (6.89) to 81.4 (7.77); 0.028Control group from 82.4 (5.32) to 83.2 (10.1); 0.130Rutkowski et al. [40]Plethysmography(total lung capacity (TLC))Group Mean ± SD in l; p-valueVR group from 5.18 ± 1.2 to 5.39 ± 1.1; 0.288Control group from 4.9 ± 1.2 to 5.27 ± 1.0; 0.070Dyspnoea↓Modified Medical Research CouncilMean difference; p-valueStudy group 48.89%; p < 0.001control group 12.81%; 0.001Nagy EN et al. [39]From 2 to 1Mayer KP et al. [21]Borg scale while 6-minute walk testGroup Mean (median); p-valueVR group from 2.0 (3.0) to 0.0 (2.0); 0.033Control group from 2.0 (2.75) to 0.5 (2.0); 0.004Rutkowski et al. [40]Muscle strength↑Medical Research Council sum scoreFrom 55 to 59Mayer KP et al. [21]↑Lower extremity unilateral leg press2-lb resistance (Watts): from 14.3 to 17.710% of body weight resistance (Watts): from 88 to 134↑↓Handgrip dynamometerRight: from 24 kg to 33 kgLeft: from 36 kg to 34 kgMayer KP et al. [21]↑Group Mean ± SD in kg; p-valueBaseline LAT 28.4 ± 0.7, HAT 28.5 ± 0.6; 0.5054 weeks LAT 29.4 ± 0.5, HAT 29.2 ± 0.6; 0.1188 weeks LAT 31.5 ± 0.6, HAT 29.8 ± 0.5; 0.0016 months LAT 34.3 ± 0.8, HAT 30.4 ± 0.8; 0.003Nambi G et al. [19]Fatigue↓N. a.N. a.Santos S et al. [24]Muscle strength↑Daniels ScaleFrom 2 to 4 out of 5Santos S et al. [24]Pain reduction↓Numeric Pain ScaleFrom 10 to 3 out of 10Santos S et al. [24]Range of motion↑GoniometerShoulder movements in ° Right pre/post physiotherapy; Left pre/post physiotherapyFlexion 100/160; 120/160Extension 20/40; 30/40Abduction 90/150; 120/160Adduction 10/20; 30/30External rotation 60/80; 80/80Internal rotation 50/55; 60/60Elbow movements in ° Right pre/post physiotherapy; Left pre/post physiotherapyFlexion 120/130; 130/140Extension 0/0; 0/0Santos S et al. [24]Balance↑Unipodal Station TestFrom 3 s to 8 sSantos S et al. [24]Basic activities of daily living↑N. a.N. a.Santos S et al. [24]Instrumental activities of daily living↑N. a.N. a.Santos S et al. [24]Legend↑ increasing↔ unchanged↓ decreased
Were adverse events reported for physiotherapeutic interventions in patients with post- or long- COVID syndrome?
In one case report the quality of life decreased [21]. But in most cases patients felt better regarding the quality of life [19, 20, 24, 39, 40].
Were negative influences reported for parallel, applied physiotherapeutic interventions in patients with post- or long-COVID syndrome?
Due to a lack of information, it is not possible to make a statement on this issue.
Were differences reported inpatient and out patient interventions?
Table 9 summarizes the identified practiced interventions and treatment parameters as the general frequency in mean. Only the 6 studies focusing on the subtype post-COVID-19 were considered because they provided enough information. Table 9. Summarization on identified practised therapy interventions, their parameters and general frequency in mean for post-COVID-19Healthcare delivery settingTherapy categoryInterventionTreatment parametersGeneral frequency(in mean)StudyInpatient andOutpatientRespiratory therapyDiaphragma releaseBreathing exercises3 sessions per weekfor 7 weeksAli AA et al. [20]Nagy EN et al. [39]Rutkowski et al. [40]Mayer KP et al. [21]Inpatient andOutpatientAerobic trainingTreadmill;Cycle ergometer3–20 minutes40–60% of maximum heart rate3 sessions per week for 9 weeksAli AA et al. [20]Nambi G et al. [19]Mayer KP et al. [21]Inpatient andOutpatientStrength trainingFree exercises, weights or weight machines3 sets of 8–20 repititions, 1 minute rest3 sessions per week for 9 weeksAli AA et al. [20]Nambi G et al. [19]Mayer KP et al. [21]
Critical appraisal
The studies selected for inclusion were subjected to critical appraisal by two independent researchers with extensive experience in the field of rehabilitation research, utilizing the JBI critical appraisal tools [37, 43]. The quality assessment was conducted to evaluate the methodological quality of the data to be extracted from the included articles. No manuscript was excluded during the critical appraisal process. The overall quality of the included literature was determined to be moderate. An overview of the critical appraisal is provided in Table 10. Table 11. Overview on critical appraisal of the case reports following JBI critical appraisal tools [37]ItemMayer et al. [21]Santos et al. [24]1Patient characteristics clearly describedyy2Patient history clearly describedyy3Current clinical condition clearly describedyy4Diagnostic tests/assessment methods clearly describedyy5Intervention clearly describedyn6Post-interventional clinical condition clearly describedyy7Adverse/unanticipated events identified and describedyn8Take-away lessons providedyyTotal86Legendy = yesn = nouc = unclearTable 10Overview on critical appraisal of the randomized controlled trials following JBI critical appraisal tools [43]DomainSelection and allocationAdministration of intervention/exposureAssessment, detection, and measurement of the outcomeParticipant retentionStatistical conclusion validityAuthorQuestion no.12345678910111213Nagy et al. [39]Dyspnoea: Modified Medical Research CouncilyyyynyyyyyyyyFatigue: Fatigue Severity ScaleyyyWalking distance: 6-minute walk testyyyArterial blood pressure SphygmomanometeryyySerum lactate level: Veinous blood sampleyyyNambi et al. [19]Kinesiophobie: Tampa scale of kinesiophobiayyyyyyyyyyyyyMuscle mass: Magnetic resonance imagingyyyMuscle strength: Handgrip dynamometeryyyQuality of life: Sarcopenia and Quality of Life questionnaireyyyRutkowski et al. [40]Fatigue: Borg scale while 6-minute walk testyynnnnucyyyyyyWalking distance: 6-minute walk testyyyDistress: Perceived Stress ScaleyyyLung function:a) Spirometryb) Plethysmographya) yb) ya) yb) ya) yb) yDyspnoe: Borg scale while 6-minute walk testyyyAli et al. [20]Fatigue: Fatigue Assessment ScaleyucyucucnucyynyyyWalking Distance: 6-minute walk testnyyArterial oxygen saturation: Arterial blood gas analysisnyyPartial pressure of oxygen: Arterial blood gas analysisnyyPartial pressure of carbon dioxide: Arterial blood gas analysisnyyTotal4332112441217174Legendy = yesn = nouc = unclear
Discussion
This scoping review aimed to give an overview on physiotherapeutic interventions and treatment parameters published in the scientific literature. The number of identified studies shows a gap in research on the topic which is contradictory to the recommendations of physiotherapy in the treatment of post- and long-COVID condition and the high number of prescribed physiotherapeutic remedies in the treatment of post- and long-COVID-19.
The included literature referring to physiotherapy interventions focus on respiratory therapy, aerobic and strength training. This scoping review reveals that the different interventions and techniques of respiratory therapy, aerobic and strength training were combined in each separate session. The majority of studies employed a set of three, with 10 to 15 repetitions and a one-minute rest interval between sets.
Only one of the included studies documented the practice of traditional physiotherapy techniques, including transcutaneous electrical nerve stimulation, friction massage and manual therapy [21]. This finding points out a research gap concerning the diversity of physiotherapeutic interventions in the treatment of patients with post-and long-COVID-19.
The assessments used in the studies were standardized assessments. Some of them do not meet the profile of physiotherapy, like spirometry or blood serum analysis. Others are highly practicable in the setting of outpatient physiotherapy, like the Borg scale or the 6-minute walk test. The included studies indicate reduction in fatigue, enhancements in respiratory function, and improvements in physical function. The quality of life increased in most cases, with the exception of one patient in one case report [21]. Pain is only assessed in one case report [24]. This finding raises the question whether pain reduction is a relevant outcome for post- and long-COVID-19 patients.
Medical guidelines and recommendations emphasize the treatment of physiotherapy [9, 44–46]. Several studies and reviews have demonstrated the positive impact of multidisciplinary rehabilitation programmes, even in infectious diseases [47, 48]. The post- and long-COVID-19 physiotherapy is based on the treatment of symptoms associated with certain diseases such as pain in fibromyalgia, cancer related fatigue or dyspnea in chronic obstructive pulmonary disease [10, 15]. Exercise programmes have been evaluated in post- and long-COVID research [18–21]. Commonly exercise programmes are carried out by sports and physiotherapists. A ‘slow progressive approach’ [18] or ‘pacing’ [44] is required in the treatment implying that therapeutic interventions must be introduced gradually and cautiously to promote adaption and minimize the risk of adverse reaction or symptom exacerbation [18, 28]. This therapeutic approach is demonstrated in the included case reports as they provide concrete insights to the physiotherapy treatment in time course [21, 24]. Further studies focusing on gradual adaption of therapeutic interventions are needed as they are recommended for practice [45].
The definitions of post- and long-COVID syndrome vary slightly with respect to the onset of symptoms following an acute infection [49]. Authors refer to the work of other authors or focus on describing the complex symptoms of this condition. This circumstance appears to influence the synthesis of physiotherapeutic interventions as the treatments provided were not aligned with the ICD-10 diagnosis.
Study limitations can be identified on the search strategy as no professional librarian supported the literature search. The involvement of a librarian could have improved the methodological quality of the literature search. as the literature research was limited to studies German and English published studies it may have led to the exclusion of relevant studies in other languages. Furthermore, grey literature was not considered, as it is only partially accessible and not published in a standardized manner. To ensure transparency and reproducibility the literature search was limited to peer-reviewed sources from established academic databases.
The number of identified studies publish until February 2023 addressing physiotherapy in post- and long-COVID-19 is very limited which also influences the statistical reporting. Study designs, outcomes and involved patient characteristics are very heterogenous making a direct comparison and quantitative synthesis difficult. The data was summarized descriptively which inhibits to draw conclusions about effectiveness of physiotherapy treatment in post- and long-COVID patients. Furthermore, treatment interventions were not described adequately detailed. For those reasons case reports were also included in the search beneath the low level of evidence, as they provide detailed insights on common therapeutic interventions applied from session to session.
However, from the findings of this scoping review objectives for further research can be derived as the gap in research is evident. Physiotherapy interventions addressing symptoms need to be evaluated with a higher methodological design and a higher sample size. A concrete definition of the included post- or long-COVID-19 diagnosis to specify the indication of physiotherapy is mandatory. Therefore, the ICD-10 codes could be useful. Nevertheless, influencing characteristics, especially in case reports, should be considered in health research as they provide a holistic picture of the participants. Therefore, the International Classification of Functioning, Disability and Health (ICF) contextual factors are appropriate [50]. Collecting these variables allows a more comprehensive understanding of participant profiles and the differentiation of treatment effects. These findings may contribute the development of clinical prediction rules by generating relevant predictors associated with treatment response within the specific clinical context.
Only a limited number of the identified publications provide detailed information regarding the specific treatment modalities practiced. The treatment methods and parameters vary across studies. For reproducibility, further research and translation into the health system it is necessary to provide detailed descriptions of the processes and the applied interventions. For example, there is a need to distinguish between a passive mobilization of the spine in general or a mobilization of a specific vertebral segment or a manipulation of a specific vertebral segment. Functional exercises need to be described more detailed additionally with pictures or videos. Standardized assessments need to be validated in the context of post- and long-COVID-19.
As physiotherapy comprises a broader spectrum of interventions beyond respiratory therapy, aerobic exercise, and strength training there are further physiotherapeutic approaches that need to be evaluated in pilot studies and randomized controlled trials. Future research should examine the efficacy of interventions such as manual therapy, passive mobilization, massage techniques, lymphatic drainage, relaxation therapies and neuromuscular treatment strategies in the context of different COVID-19 subtypes. Educational material used for training the therapists and assessors in the study also need to be provided in the publications for reproducibility and in particular to ensure the translation into practice.
Conclusions
This scoping review highlights a high demand for research in the treatment of post- and long-COVID patients for the in-person physiotherapy setting. To ensure reproducibility and clinical applicability, a detailed description of all practiced physiotherapy techniques is essential. However, the results of this scoping review provide physiotherapists treatment options for patients with post- and long-COVID-19 as physiotherapy demonstrated to have positive trends in supporting health outcomes among patients with post- and long-COVID condition.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Institute for Health and Care Excellence (NICE). COVID-19 rapid guideline: managing the long-term effects of COVID-19. 2020, 2025. https://www.nice.org.uk/guidance/ng 188. Accessed 4. June 2025.33555768 · pubmed ↗
- 2Kuz U, Maliuvanchuk S, Herych R, Herych P. Efficacy and safety of physical therapy in patients with stage III COPD during ambulatory rehabilitation. J Med Life. 2023, Dec;16(12):1769–75. 10.25122/jml-2023-023710.25122/jml-2023-0237 PMC 1099462638585540 · doi ↗ · pubmed ↗
- 3World Health Organization (WHO). Clinical management of COVID-19: living guideline. 2023. https://www.who.int/publications/i/item/WHO-2019-n Co V-clinical-2023.2. Accessed 15 March 2025, 7th.35917394 · pubmed ↗
- 4Joana Briggs Institute (JBI). JBI manual for evidence synthesis. https://jbi-global-wiki.refined.site/space/MANUAL/355862497/10.+Scoping+reviews. Accessed 1 Nov 2023.
- 5Rutkowski S, Bogacz K, Rutkowska A, Szczegielniak JCR, Casaburi R. Inpatient post-COVID rehabilitation program featuring virtual reality-preliminary results of randomized controlled trial. Front Public Health. 2023;11:1121554. 10.3389/fpubh.2023.112155410.3389/fpubh.2023.1121554 PMC 993963936815161 · doi ↗ · pubmed ↗
- 6Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF). S 1-Leitlinie Long/Post-COVID (Stand 30.05. 2024) https://register.awmf.org/assets/guidelines/020-027l_S 1_Long-Post-Covid_2024-06_1.pdf. Accessed 8. July 2025.
- 7Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF). Position statement on physical therapy during COVID-19. https://www.kngf.nl/binaries/content/assets/kennisplatform/onbeveiligd/guidelines/kngf-position-statement-on-physical-therapy-during-covid-19.pdf. Accessed 28 June 2024.
- 8Chiaramonte R, D’amico S, Marletta C, Grasso G, Pirrone S, Bonfiglio M. Impact of clostridium difficile infection on stroke patients in rehabilitation wards. Infect Dis Now. 2023;53(5). 10.1016/j.idnow.2023.10468510.1016/j.idnow.2023.10468536841431 · doi ↗ · pubmed ↗