Development and validation of assistance needs assessment scale of the home-dwelling older adults
Lei Huang, Weihong Yang, Jiaqi Yang, Panpan Jing, Yuqing Ye, Yifei Zhao, Chuanwu Lyu, Xianghan Kong, Lina Wang, Peng Wang, Yan Lin, Rui Chen, Yue Yao, Yang Li

TL;DR
This study created and validated a 27-item scale to assess the assistance needs of older adults living at home, which could help improve community services and policies.
Contribution
A novel, validated assessment tool for identifying unpaid assistance needs in home-dwelling older adults with strong psychometric properties.
Findings
The scale has four dimensions: daily assistance, health maintenance, visitation and communication, and social interaction.
Confirmatory factor analysis showed good model fit (CFI=0.951, TLI=0.946, RMSEA=0.068).
The scale demonstrated excellent internal consistency with Cronbach’s α ranging from 0.943 to 0.968.
Abstract
With the acceleration of population aging, identifying and addressing the unmet assistance needs of home-dwelling older adults has become increasingly important. This study aimed to develop and validate a reliable and practical assessment tool to identify such needs. A descriptive qualitative study was conducted using semi-structured interviews with home-dwelling older adults in two communities in Wuhan, China. Based on the qualitative findings and literature review, an initial item pool was developed, followed by expert consultation to construct a draft scale. A cross-sectional survey was then conducted in communities across four central Chinese cities. Item analysis and psychometric testing were performed to finalize the scale. The finalized scale consists of 27 items across four dimensions: daily assistance, health maintenance, visitation and communication, and social interaction.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
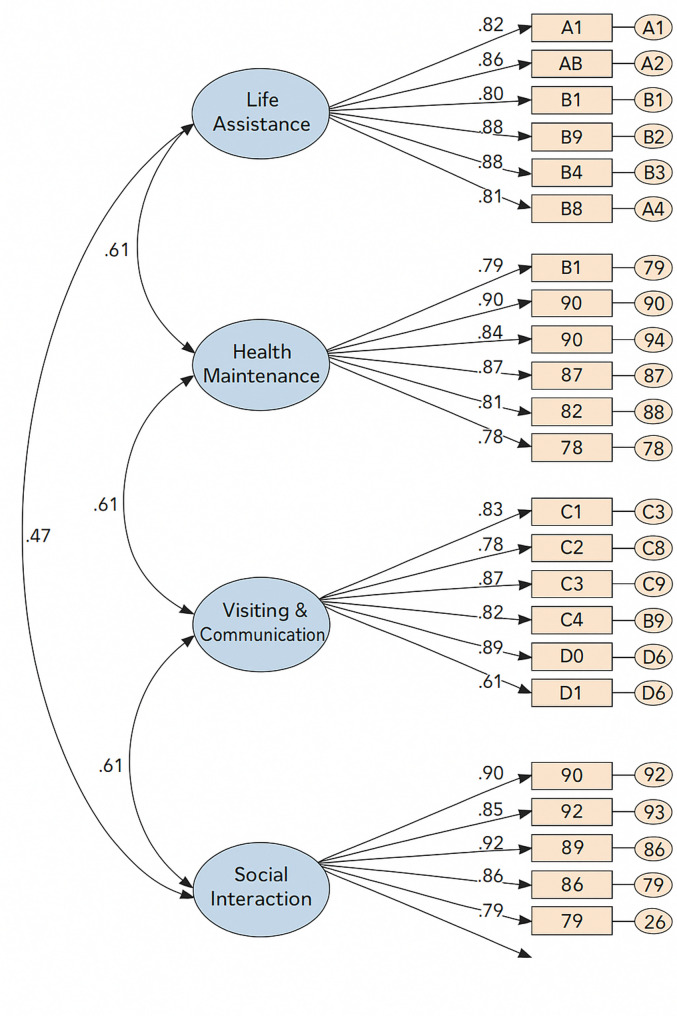 Figure 1
Figure 1- —https://doi.org/10.13039/501100017700Henan Provincial Science and Technology Research Project
- —Humanities and Social Sciences Research Project of Institutions of Higher Learning in Henan Province
- —https://doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth and Well-being Studies · Intergenerational Family Dynamics and Caregiving · Health and Wellbeing Research
Introduction
With the accelerating pace of global population aging, the aging crisis has become a major societal challenge faced by countries worldwide. According to United Nations data, the global population aged 60 and above is projected to reach 1.4 billion by 2030 and 2.1 billion by 2050 [1]. China, as the world’s most populous developing country, is experiencing particularly rapid aging due to its socioeconomic development. By the end of 2023, approximately 297 million people in China were aged 60 and above, accounting for 21.1% of the total population [2]. This rapidly growing elderly population places increasing pressure on China’s social security and healthcare systems, further widening the gap between the supply and demand for care services of older adults [3, 4].
China currently promotes the “9073” care model of older adults, in which approximately 90% of older adults receive care at home, 7% rely on community-based care, and only 3% live in institutional settings [5]. Home-based care remains the dominant form of care of older adults in China. However, with the ongoing transformation of family structures toward smaller, nuclear, and empty-nest households, traditional family-based care functions are weakening. As a result, many home-dwelling older adults lack adequate family support due to factors such as living alone or having adult children occupied with work responsibilities [6, 7]. Recent studies show that the satisfaction rate of perceived care needs of older adults among community-dwelling older adults in China ranges from only 9.1% to 45.0%. In contrast, the reported demand for services is as high as 64.9% to 81.2% [8]. This indicates a significant service gap that requires urgent attention. Other studies have found that long-term unmet needs can severely compromise the physical and mental health of older adults, and in some cases, even endanger their lives [9, 10]. Therefore, it is imperative to expand the availability of community-based care resources of older adults for this population [11].
In recent years, China has actively promoted the development of volunteer services and neighborhood mutual assistance as a means to enhance the social support system for home-based care of older adults. The “14th Five-Year Plan for the Development of Aging Services and Elderly Care System” clearly advocates for the establishment of an integrated model involving social workers, neighbors, volunteers, and physicians to provide psychosocial support services to older adults with special difficulties [12]. President Xi Jinping has also emphasized the importance of strengthening public participation mechanisms and developing volunteer-based care services of older adults to address the country’s demographic aging [13]. Given these policy directions, there is an urgent need for a dedicated assessment tool to evaluate the assistance needs of home-dwelling older adults within informal and non-paid support systems, including volunteers, neighbors, and community mutual-aid networks, rather than through paid formal providers. Such a tool is essential for scientifically identifying and assessing actual support needs, thereby enabling communities to deliver more targeted and effective services.
Although several tools have been developed to assess the needs of home-dwelling older adults, most focus on medical care, functional support, or general care needs of older adults. These tools often do not specifically address unpaid assistance needs within informal care systems [14–19]. For example, Shih et al. [16] developed the Health Needs Instrument (HNI), which uses binary “yes/no” responses to evaluate older adults’ needs across five dimensions: tangible assistance, emotional support, medical help, access to health information, and participation in decision-making. However, the tool does not clearly distinguish between formal and informal support sources. Chatterjee et al. [17] developed the Integrated Care Tool-Brief (ICT-BRIEF), which includes 30 items covering physical health, functional status, geriatric syndromes, psychological well-being, and social domains. Although useful for preliminary screening and care planning, the tool is still situated within a broader health assessment framework. Some studies have touched upon volunteer service needs, but these tools are not specifically designed to assess the unpaid assistance needs of home-dwelling older adults. For instance, Zhao et al. [18] conducted a survey using a self-developed questionnaire to assess older adults’ needs for volunteer services, but the tool used binary response options and included institutionalized individuals, limiting its representativeness. Wilkinson-Meyers et al. [19] developed a questionnaire to assess support needs across seven domains (e.g., personal care, household chores, meal preparation, shopping, and transportation), evaluating assistance provided by family, friends, or paid/unpaid service providers. While partially addressing unpaid support, this instrument lacks a clear focus on home-dwelling older adults and includes paid assistance.
In summary, current assessment tools generally lack targeted focus on the concept of unpaid assistance needs, particularly in identifying the extent to which older adults expect to receive support from non-family, unpaid social resources. Therefore, it is essential to develop a scientific, systematic, and culturally adapted instrument specifically designed to assess such needs in the context of informal caregiving. This study aims to develop an assessment scale for the unpaid assistance needs of home-dwelling older adults in China by integrating literature review, qualitative interviews, and expert consultation to construct a comprehensive evaluation framework. The results will provide key stakeholders—such as communities, healthcare institutions, and volunteer organizations—with more accurate information to better match and allocate support resources, ultimately improving the quality of life for older adults [20, 21]. Furthermore, the scale will serve as a reference for other countries and regions facing similar challenges, contributing to the sustainable response to population aging and advancing the global strategy for healthy aging.
Method
This study adhered to the established principles and methodologies for scale development, combining literature review, qualitative research, and expert consultation. By employing a qualitative descriptive design, the study aimed to minimize researcher bias, allowing findings to emerge directly from the data [22, 23]. An initial item pool was created based on the literature review and qualitative research findings. Subsequently, expert consultations were conducted to formulate a preliminary version of the Home-Dwelling Older Adults Assistance Needs Assessment Scale. A cross-sectional survey was conducted using convenience sampling in four communities across four cities in central China (Wuhan, Ezhou, Zhengzhou, and Xinxiang). The selection of these sites was guided by several considerations, including their alignment with national development strategies for the central region, geographic accessibility, feasibility of collaboration with local institutions, and the research team’s established connections with community organizations. Based on the data collected, the scale was further refined and finalized through item screening as well as reliability and validity analyses. Participant Inclusion and Exclusion Criteria Inclusion criteria were: (1) aged 60 years or older; (2) currently residing in an urban community in China and having lived there for more than one year; (3) informed of the research purpose and voluntarily participating. Exclusion criteria: individuals with communication barriers.
Stage 1: item pool generation
A comprehensive literature search was conducted using keywords such as “older adult,” “home-dwelling,” “community-dwelling,” “assistance,” “need,” “questionnaire,” and “scale” across multiple databases (PubMed, EMBASE, CINAHL Complete, Scopus, Web of Science, CNKI, Wanfang, VIP). This search informed the development of the qualitative interview guide and the questionnaire item pool.
A descriptive qualitative research design was employed. Purposive sampling (including criterion-based and maximum variation sampling) was used to recruit home-dwelling older adults from two geographically distant communities in Wuhan, China. Maximum variation sampling ensured representation of older adults with diverse life difficulties (e.g., living alone, chronic illnesses) and various age groups. Data collection continued until saturation was achieved. Textual data were managed and analyzed using NVivo 11.0 Plus software, employing traditional content analysis methods [24]. The interview guide is detailed in Appendix 1. Findings from this qualitative study have been presented in a previously published study [25].
The initial structure and content of the scale were determined using thematic analysis based on the literature review and semi-structured interviews [26].
Stage 2: Delphi expert consultation
The Delphi method was implemented with two rounds of expert consultation to refine the preliminary scale by adding, deleting, and modifying items. The number of experts is determined based on the scale of the research project, and typically ranges from 15 to 50 [27]; this study invited 17 experts. Detailed information about the Delphi panel, including their demographic and professional characteristics, is provided in Appendix 2. The first round of expert consultation comprised four parts: (1) introduction and instructions detailing the purpose and significance of the scale; (2) expert consultation form evaluating item relevance (4-point Likert scale) and importance (5-point Likert scale) [28]; (3) expert demographic questionnaire collecting institutional affiliation, gender, age, contact information, educational background, professional title, expertise, and years of experience; (4) authority questionnaire assessing experts’ familiarity and judgment basis regarding the scale content. The second round also included four similar parts with additional descriptions of the scale’s revisions.
Both consultation rounds were conducted online via email or WeChat, requiring responses within two weeks. After the first round, the research team collected and analyzed the data, revised the items accordingly, and sent a second-round questionnaire to the same experts for reassessment. Consultation ceased once expert consensus was achieved.
Data analysis was conducted by two researchers using SPSS 22.0 software. Expert opinions and statistical analyses guided final decisions on item inclusion, deletion, or modification, ultimately producing the finalized scale. Evaluation metrics included: (1) response rate (> 70% indicating high engagement); (2) authority coefficient (Cr ≥ 0.70 indicating high expert authority); (3) opinion concentration (mean scores ≥ 4 indicating high consensus) [29]; (4) coordination of opinions (coefficient of variation Cv < 0.25 indicating minimal disagreement) [30]; and (5) content validity indices (CVI: item-level CVI ≥ 0.78, scale-level CVI ≥ 0.90) [31].
Stage 3: psychometric testing
The required sample size for scale development considered both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). Generally, the EFA sample size should be 5–10 times the total number of scale items [32]. Given the preliminary scale had 33 items across 4 dimensions, the sample size required for EFA was at least 165 cases. The CFA sample size needed to be no less than 200 and larger than the EFA sample size [33]. Accounting for a 10% rate of invalid responses, the total sample size required was at least 406.
The survey consisted of two instruments: (1) a demographic questionnaire developed by the researchers to collect sociodemographic information from participants, including gender, age, education level, religious belief, previous occupation, and marital status; (2) the preliminary version of the Home-Dwelling Older Adults Assistance Needs Assessment Scale, developed by the researchers, comprising 33 items in four dimensions: life assistance (10 items), health maintenance (9 items), visiting and communication (8 items), and social interaction (6 items). Items were rated on a 5-point Likert scale ranging from 1 (not needed at all) to 5 (very much needed), with total scores ranging from 33 to 165. Higher scores indicated greater overall needs for volunteer services. A standardized instruction was provided at the beginning of the questionnaire to ensure consistent understanding. The instruction specified that the term “someone” referred to volunteers, neighbors, or other informal helpers providing unpaid support, rather than paid professional caregivers or service providers. This instruction was presented before the items to guide respondents in completing the scale. (4) the Activity of Daily Living Scale (ADL), originally developed by Mahoney and Barthel in 1965 [34], is widely used to assess the self-care ability of older adults or individuals with chronic diseases in performing everyday activities. It consists of 10 items, each scored using different ranges depending on the task. For example, some items are rated 0, 5, or 10, whereas others are rated 0, 5, 10, or 15. The total score ranges from 0 to 100, with higher scores indicating better independence in daily functioning. In the present study, the Cronbach’s alpha of the ADL scale was 0.933, suggesting excellent internal consistency. (5) the Patient Health Questionnaire (PHQ-9), developed by Kroenke and colleagues [35] based on the diagnostic criteria for depressive disorders in the DSM-IV, is commonly used for screening, diagnosis, and monitoring of depression in adults. It includes 9 items, each rated on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). The total score ranges from 0 to 27, with higher scores reflecting more severe depressive symptoms. In this study, the PHQ-9 demonstrated excellent internal reliability, with a Cronbach’s alpha of 0.939.
All researchers received standardized training to clarify study objectives and protocols. Before initiating data collection, the researchers contacted community leaders or management authorities to obtain consent and ensure smooth survey administration. A preliminary survey involving 30 older adults from the communities was conducted to refine questionnaire wording. Subsequently, the researchers obtained contact and residence information of potential participants through community management offices, contacted the older adults or their family members by phone, and verified eligibility criteria. Upon obtaining informed consent, researchers visited participants at their homes, accompanied by community staff, to administer the survey. During survey completion, researchers supervised and provided necessary explanations to ensure data quality. Completed surveys were immediately checked, and any incomplete or incorrectly filled questionnaires were returned to participants for correction. The survey adhered strictly to anonymity and confidentiality.
Statistical analysis was conducted using SPSS 26.0 and AMOS 24.0 software. (1) Descriptive analysis: normally distributed continuous data were presented as mean ± SD, and skewed data as median [M (P25, P75)]; categorical data were presented as percentages (%) and frequencies (n). (2) Item screening methods included: (a) critical ratio method: evaluating item discrimination, with items having p-values > 0.05 considered for deletion [33]; (b) correlation coefficient method: assessing correlations between individual items and total scale scores, with items having correlation coefficients < 0.4 or p-values > 0.05 considered for deletion [33]; (c) Cronbach’s alpha method: examining changes in the overall Cronbach’s alpha upon item deletion, with increases indicating poor homogeneity and thus suggesting deletion [33]; (d) exploratory factor analysis: after confirming suitability through Bartlett’s test (p < 0.05) and Kaiser-Meyer-Olkin (KMO) measure (> 0.60), factors with eigenvalues > 1 explaining at least 50% cumulative variance were extracted using principal component analysis with varimax rotation, and items with factor loadings < 0.40 were considered for deletion [36]. (3) Validity analyses: (a) construct validity assessed using CFA with fit indices (CFI > 0.90, TLI > 0.90, RMSEA < 0.08, χ²/df < 3, NFI > 0.90, IFI > 0.90), and factor loadings ideally between 0.71 and 0.95 [34]; (b) convergent validity evaluated using average variance extracted (AVE ≥ 0.50) and composite reliability (CR ≥ 0.60) [37]; (c) predictive validity preliminarily examined by testing correlations between scale scores and external indicators [38]. (4) Reliability analyses included internal consistency (Cronbach’s alpha > 0.80) and split-half reliability (> 0.80) [39]. (5) Acceptability indicators: response rate and valid response rate ≥ 85%, and an average completion time of 15–20 min recommended [40].
Results
Item pool development
The initial item pool for the Home-Dwelling Older Adults Assistance Needs Assessment Scale comprised 37 items across five dimensions: daily care (9 items), medical care (10 items), psychological comfort (10 items), cultural engagement (4 items), and social interaction (4 items). Items were rated using a 5-point Likert scale (1 = not needed at all, 2 = not really needed, 3 = uncertain, 4 = needed, 5 = very much needed) (Appendix 3).
Qualitative evaluation
In the first Delphi expert consultation round, 17 experts were invited, and 15 valid responses were collected. Experts were from seven provinces (Hubei, Henan, Jiangsu, Sichuan, Chongqing, Guangdong, Fujian), representing various fields including geriatric nursing, community nursing, social security, clinical nursing, psychological nursing, and nursing management. The mean expert age was 51.33 ± 7.08 years, with an average of 27.93 ± 11.11 years of relevant experience. Further details of the expert consultation are provided in Appendix 2. The response rates for the first and second rounds were 88.2% (15 out of 17) and 100.0% (15 out of 15), respectively, indicating high expert engagement (> 70%). The authority coefficient (Cr) was consistently high at 0.86 across both rounds. Mean importance ratings ranged from 4.13 to 4.60 in the first round and 4.00–4.93 in the second round, demonstrating a high concentration of expert opinions (Appendices 4 and 5). Coefficients of variation ranged from 0.14 to 0.23 (round 1) to 0.05–0.23 (round 2), indicating strong expert consensus (Appendices 4 and 5). Item-level content validity indices (I-CVI) improved from 0.47 to 0.93 (round 1) to 0.80–1.00 (round 2), with the scale-level content validity index (S-CVI) increasing from 0.84 to 0.96. After two rounds of consultation, all items met the required standards, indicating that the content validity aligns with the requirements for scale development. Detailed results are presented in Appendix 6 and 7. In addition, during the first round of expert consultation, a total of 31 revision suggestions were collected, of which 25 were adopted or thoroughly considered. Based on expert recommendations, corresponding items in the scale were deleted, modified, or added. In the second round, 6 suggestions were received, all of which were accepted or fully taken into account. The scale items were revised accordingly based on these expert inputs. The detailed revision process is presented in Appendix 8.
Quantitative evaluation
A total of 440 questionnaires were distributed, with 394 returned (89.5% response rate). After excluding invalid responses, 380 valid questionnaires were analyzed (86.4% valid response rate). Participants’ ages ranged from 60 to 98 years, with a median age of 72 (66, 80) years (Appendix 9). From this dataset, 170 randomly selected cases were used for item analysis, reliability testing, and exploratory factor analysis (EFA), while the remaining 210 cases underwent confirmatory factor analysis (CFA).
Item selection
Using the critical ratio method, 170 cases were divided into high- and low-scoring groups (top and bottom 27%, n = 46 each). Independent-sample t-tests showed significant differences between the two groups, with t-values ranging from 7.307 to 24.318 (all p < 0.001), indicating excellent item discrimination (Table 1). In the correlation analysis, item-total correlation coefficients ranged from 0.548 to 0.864, demonstrating high internal consistency (Table 2), and all items were retained based on this result. According to the Cronbach’s alpha method, the overall Cronbach’s alpha was 0.974. Deletion of any single item did not significantly increase the alpha value. The corrected item-total correlations ranged from 0.523 to 0.852, and the dimension-level Cronbach’s alpha coefficients remained similarly stable, ranging from 0.704 to 0.887, further confirming strong internal consistency (Appendices 8 − 1 and 8 − 2). In the exploratory factor analysis, the Kaiser-Meyer-Olkin (KMO) measure was 0.929, and Bartlett’s test of sphericity was significant (χ² = 5409.043, p < 0.001), indicating the dataset’s suitability for factor analysis. Four factors with eigenvalues greater than 1 were extracted, explaining a cumulative variance of 79.6%. Six items (a7, a8, b8, b9, c2, c3) showed ambiguous loadings on multiple factors and were removed following team discussion. The final factor loadings for retained items ranged from 0.560 to 0.909.
Table 1. Critical ratio analysis resultsDimensionItemLevene’s Test for Homogeneity of VarianceEqual Variancet P F P Daily Living Assistancea11.3350.251Yes16.990<0.001a20.4610.499Yes15.057<0.001a330.704<0.001No11.105<0.001a439.549<0.001No9.283<0.001a50.0050.942Yes17.796<0.001a64.3870.039No20.857<0.001a78.1940.005No12.378<0.001a83.6110.061Yes24.318<0.001a95.8350.018No14.850<0.001a101.2080.275Yes12.559<0.001Health Maintenanceb123.059<0.001No11.636<0.001b243.545<0.001No11.172<0.001b340.959<0.001No11.566<0.001b420.858<0.001No13.294<0.001b55.1760.025No14.746<0.001b659.538<0.001No9.544<0.001b77.4980.007No14.525<0.001b820.137<0.001No10.687<0.001b916.307<0.001No11.001<0.001Visiting and Communicationc11.3860.242Yes15.202<0.001c20.1320.717Yes11.872<0.001c30.2230.638Yes12.732<0.001c410.0740.002No12.647<0.001c57.5270.007No11.530<0.001c68.6460.004No12.457<0.001c712.4670.001No9.620<0.001c82.2480.137Yes14.318<0.001Social Engagementd111.0330.001No8.826<0.001d214.075<0.001No8.183<0.001d321.372<0.001No7.471<0.001d413.546<0.001No7.307<0.001d56.9010.010No8.491<0.001d612.9870.001No8.236<0.001
Table 2. Correlation analysis between scale items and total scoresItem r
P Item r
P Item r
P a10.789<0.001b20.739<0.001c40.743<0.001a20.761<0.001b30.759<0.001c50.736<0.001a30.635<0.001b40.788<0.001c60.761<0.001a40.623<0.001b50.812<0.001c70.678<0.001a50.821<0.001b60.720<0.001c80.775<0.001a60.796<0.001b70.803<0.001d10.562<0.001a70.750<0.001b80.766<0.001d20.548<0.001a80.864<0.001b90.774<0.001d30.548<0.001a90.772<0.001c10.803<0.001d40.567<0.001a100.698<0.001c20.758<0.001d50.592<0.001b10.744<0.001c30.761<0.001d60.634<0.001
Validity analysis
Construct validity was supported by confirmatory factor analysis (CFA), which demonstrated good model fit indices (CFI = 0.951, TLI = 0.946, RMSEA = 0.068, χ²/df = 1.971, NFI = 0.906, IFI = 0.952), indicating that the hypothesized model aligned well with the observed data (Fig. 1). In terms of average variance extracted (AVE) and composite reliability (CR), standardized factor loadings ranged from 0.67 to 0.94. The CR values ranged from 0.945 to 0.967, and AVE values ranged from 0.685 to 0.832, confirming strong convergent validity of the scale (Table 3). Regarding predictive validity, Spearman correlation analysis showed that scale scores were moderately and positively correlated with depressive symptoms (r = 0.384, p < 0.001) and weakly and negatively correlated with activities of daily living (r = − 0.170, p = 0.013), consistent with theoretical expectations.
Fig. 1. Confirmatory Factor Analysis Model
Table 3. Average variance extracted and composite reliabilityItemDimensionStandardized Factor LoadingSignificanceComposite ReliabilityAverage Variance Extracteda1Daily Living Assistance0.820.9450.685a20.86a30.86a40.88a50.84a60.87a90.67a100.80b1Health Maintenance0.880.9630.788b20.88b30.92b40.90b50.91b60.84b70.88c1Visiting and Communication0.830.9510.764c40.89c50.83c60.92c70.87c80.90d1Social Engagement0.900.9670.832d20.92d30.93d40.94d50.89d60.89******indicates P<0.001
Reliability analysis
The finalized scale’s Cronbach’s alpha was 0.968 overall and ranged from 0.943 to 0.967 across dimensions. Split-half reliability was 0.969 overall, with dimensions ranging from 0.914 to 0.948, indicating excellent reliability.
Acceptability analysis
The questionnaire achieved a response rate of 89.5% and a valid response rate of 86.4%, reflecting strong acceptability. The finalized Home-Dwelling Older Adults Assistance Needs Assessment Scale comprises 27 items across four dimensions: life assistance (8 items), health maintenance (7 items), visiting and communication (6 items), and social interaction (6 items) (Table 4).
Table 4. Finalized scale items for Home-Dwelling older adults assistance needs assessment (Instruction: please read the following items and indicate how much you would need such assistance in your daily life. In this questionnaire, “someone” specifically refers to volunteers, neighbors, or other informal helpers providing unpaid support, rather than paid professional caregivers or service providers.)Dimensions and ItemsItem ContentDimension 1Daily Living Assistancea1How would you feel if someone could assist you with grocery shopping or other purchases?a2How would you feel if someone could deliver meals to you and improve your diet?a3How would you feel if someone could help you maintain personal hygiene, such as washing, bathing, or changing clothes?a4How would you feel if someone could assist you with indoor mobility?a5How would you feel if someone could accompany you for outdoor walks?a6How would you feel if someone could help you with house cleaning?a9How would you feel if someone could teach you how to use a smartphone or access the internet to enrich your life and increase enjoyment?a10How would you feel if someone could accompany you to the bank to handle deposits, withdrawals, or financial matters?Dimension 2Health Maintenanceb1How would you feel if someone could come to your home to check your blood pressure, blood sugar, and conduct other physical examinations?b2How would you feel if someone could provide you with medication guidance?b3How would you feel if someone could offer you health care and disease prevention advice?b4How would you feel if someone could give you fall prevention guidance?b5How would you feel if someone could accompany you to hospital visits or health check-ups?b6How would you feel if someone could respond promptly and provide help when you actively seek assistance?b7How would you feel if someone could guide and accompany you in rehabilitation and functional exercises?Dimension 3Visiting and Communicationc1How would you feel if someone could chat with you?c4How would you feel if someone could listen to your past experiences and praise or affirm your achievements?c5How would you feel if someone could celebrate your birthday?c6How would you feel if someone could recognize your negative emotions during conversations and offer appropriate advice?c7How would you feel if someone made you feel respected and appreciated during visits?c8How would you feel if someone could show concern for your family and help ease your worries about their difficulties?Dimension 4Social Engagementd1How would you feel if someone could register or help you join social activities?d2How would you feel if someone could accompany you to social activities?d3How would you feel if someone could organize social or group activities for older adults?d4How would you feel if someone could help you meet more friends or connect with organizations and groups?d5How would you feel if someone could accompany you in doing things you enjoy?d6How would you feel if someone could provide a platform for you to showcase or develop your interests and hobbies?
Discussion
With the accelerating trend of population aging and the continued promotion of home-based care of older adults, the demand for informal care at the community level has become increasingly prominent [41]. A European study revealed that 40.0% of older adults reported not receiving timely assistance, and for nearly all of them, the family was the only source of support, with few reporting the use of other community service resources [42]. A scientifically sound and systematic assessment tool is essential for accurately identifying the assistance needs of home-dwelling older adults and enhancing the efficiency of resource allocation. However, existing assessment tools for older adults’ service needs [14–19] primarily focus on medical care, functional support, or unmet needs. To date, no dedicated tool has been developed to evaluate the unpaid assistance needs specific to community-dwelling older adults.
To fill this research gap, the present study developed and validated a psychometrically robust assistance needs assessment scale. The scale consists of 27 concise and well-structured items. With a completion time of approximately 10 min, the content is accessible and easy to understand, making it suitable for older adults with varying levels of education. Covering multiple dimensions—including daily living assistance, health maintenance, emotional support, and social participation—the scale accommodates the needs of healthy, sub-healthy, and partially functionally limited older adults, aligning well with the growing demand for personalized, multi-level care services of older adults. The scale was developed through a comprehensive multi-phase process involving literature review, qualitative interviews, expert consultation, pilot testing, and quantitative validation [43, 44]. This ensured the multidimensional nature of assistance needs was thoroughly reflected. The results demonstrated strong reliability, content validity, and structural validity, indicating stable and interpretable psychometric properties.
Notably, this scale distinguishes itself from existing tools by focusing not only on unmet or general care needs of older adults but also on older adults’ expectations regarding socially engaged caregiving. It emphasizes the value of informal support networks and highlights the importance of participation, autonomy, and emotional well-being in later life. The tool offers a scientific foundation for community health workers, healthcare professionals, and volunteer organizations to assess needs and allocate support resources more effectively through stratified interventions [45, 46]. Furthermore, this instrument provides essential data for evaluating and improving care policies of older adults under the aging population context. Its application supports the optimization of community support systems, improves responsiveness, and reduces the duplication or misallocation of public welfare resources. Ultimately, it contributes to enhancing older adults’ sense of support, well-being, and security in home-based settings.
The development of this scale strictly followed standard procedures and principles for scale construction. First, relevant domestic and international literature and books were reviewed, and findings from the previous phase of qualitative research were integrated. Based on this, a preliminary structure and content of the scale were drafted through group discussions to ensure both the breadth and depth of the item pool. To enhance the scientific rigor, accuracy, comprehensiveness, and operational feasibility of the items, two rounds of expert consultation were conducted to refine and improve the scale. A pilot survey was then used to optimize item wording for better readability and to identify potential problems and challenges in the implementation process, thereby ensuring the feasibility of the formal study. After completing the formal survey, item analysis, reliability analysis, validity analysis, and acceptability analysis were conducted to further refine and finalize the scale.
Throughout the scale development process, quality control was implemented at every stage by the research team and supervisors. The expert consultation was carried out strictly in accordance with established procedures. All participating experts held at least a bachelor’s degree and a senior professional title (associate professor or above), with an average of more than 27 years of work experience, indicating high credibility. The experts came from multiple provinces and research fields, demonstrating broad representativeness. The valid response rates for the two rounds of expert consultation were 88.2% and 100.0%, significantly exceeding the 70% benchmark, indicating a high level of expert engagement. The authority coefficient of the experts was 0.86, reflecting a high degree of expertise and credibility. A total of 31 suggestions were collected in the first round of consultation, and 6 suggestions in the second round, indicating a convergence of expert opinions. After two rounds, the mean importance scores for all items were above 4.00, suggesting high consensus among experts. The coefficient of variation for all items was below 0.25, indicating strong agreement. The item-level content validity index (I-CVI) for all items exceeded 0.78, and the scale-level content validity index (S-CVI) was above 0.90, demonstrating good content validity. All items showed item-total correlation coefficients above 0.40, indicating high internal consistency. The overall Cronbach’s alpha coefficient of the scale was 0.974, confirming excellent internal reliability. Bartlett’s test of sphericity indicated that the scale was suitable for factor analysis. After further refinement and item screening, confirmatory factor analysis showed good model fit with the following indices: CFI = 0.971, TLI = 0.968, RMSEA = 0.053, CMIN/DF = 1.580, NFI = 0.926, and IFI = 0.972, indicating the scale also possesses strong structural validity. furthermore, preliminary evidence of predictive validity was found, with scale scores showing a moderate positive correlation with depressive symptoms and a weak negative correlation with activities of daily living. These findings align with theoretical expectations, suggesting that the scale reflects important psychosocial and functional aspects of older adults and may help identify vulnerable groups. Future longitudinal studies are needed to further confirm its predictive value for outcomes such as hospitalization, social isolation, or caregiver burden.
In addition to its policy implications, the findings can be better understood when viewed through established theoretical perspectives on aging. The principle of aging in place emphasizes supporting older adults to remain safely and independently in their familiar communities, which has become a central goal of aging policy worldwide [47]. By identifying unmet assistance needs within home and community settings, the scale provides practical evidence to inform strategies that promote aging in place. From the perspective of social capital, strong community ties and reciprocal support are essential for maintaining well-being and reducing isolation among older adults [48]. The scale’s focus on unpaid assistance directly reflects this dimension, highlighting the importance of mobilizing community and volunteer resources as social capital to improve care. Finally, caregiving frameworks emphasize that care involves not only physical support but also psychosocial and emotional aspects [49]. By capturing both functional and psychosocial needs, the scale contributes to more comprehensive caregiving approaches that integrate family, community, and volunteer systems.
Limitation
This study has several limitations. First, convenience sampling may have introduced selection bias and affected sample representativeness. Second, participants were recruited exclusively from urban communities in central China, which may limit the generalizability of the findings to rural or economically disadvantaged regions where assistance needs could differ substantially. Future studies should expand the geographic scope and adopt more representative sampling strategies to improve external validity. Third, since most of the supporting literature and validation data are derived from Chinese contexts, the cross-national generalizability of the scale may be limited. Replication and validation in different cultural and healthcare settings are needed to establish its broader applicability. Fourth, the study excluded high-risk groups such as the functionally impaired, socially isolated, or low-income older adults living alone, limiting the scale’s applicability in these populations. Lastly, while the scale underwent expert consultation, pilot testing, and psychometric validation, its predictive validity and long-term utility require further large-scale and longitudinal studies.
Conclusion
This study followed a standardized scale development process, integrating literature review, qualitative research, Delphi expert consultation, and a formal questionnaire survey to develop and validate a 27-item assessment tool for evaluating the assistance needs of home-dwelling older adults. The scale demonstrated strong scientific rigor, reliability, validity, and practical applicability. The finalized version comprises four dimensions: life assistance, health maintenance, visiting and communication, and social interaction. The results indicated that the scale has good reliability and validity. This tool is a reliable and effective instrument for assessing unpaid assistance needs among older adults living at home and provides a scientific basis for the planning, allocation, and optimization of community-based care services of older adults and related policy development.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Ageing and health. (2022-10-01)(Accessed Aug 24, 2025, at https://www.who.int/news-room/fact-sheets/detail/ageing-and-health?
- 2Zhong YQ, Wang J, Nicholas S. Social support and depressive symptoms among family caregivers of older people with disabilities in four provinces of urban china: the mediating role of caregiver burden. BMC Geriatr. 2020;20(1):3. 10.1186/s 12877-019-1403-9. 10.1186/s 12877-019-1403-9PMC 694126431898490 · doi ↗ · pubmed ↗
- 3Central People’s Government of the People’s Republic of China. 14th Five-Year Plan for the Development of National Aging Undertakings and Elderly Care Service System. (2021-12-30)(Accessed Oct 14, 2024, at https://www.gov.cn/gongbao/content/2022/content_5678066.htm?eqid=a 5ba 8e 4a 0001795200%20000004646 c 6b 5a).
- 4Central People’s Government of the People’s Republic of China. Eight Departments Issue Opinions on Supporting and Developing Volunteer Service Organizations. (2016-07-13)(Accessed Oct 14, 2024, at https://www.gov.cn/xinwen/2016-07/13/content_5090720.htm).