Switching From Aflibercept 2 mg to 8 mg in Vitrectomized Eyes With Neovascular Age-Related Macular Degeneration
Ryuto Tamai, Tomohiro Nizawa, Yuto Kawamata, Takehito Iwase, Takayuki Baba

TL;DR
A higher dose of aflibercept (8 mg) may improve treatment outcomes in vitrectomized eyes with neovascular age-related macular degeneration.
Contribution
The study introduces aflibercept 8 mg as a potential treatment for vitrectomized eyes with nAMD, where conventional doses are less effective.
Findings
Switching to aflibercept 8 mg resolved fluid in all three vitrectomized nAMD eyes.
Treatment intervals could be extended without adverse events in these cases.
The 8 mg dose may offer better durability and reduce treatment burden in vitrectomized patients.
Abstract
Vitrectomy may alter intravitreal pharmacokinetics through the removal of the vitreous gel, potentially accelerating the clearance of anti-vascular endothelial growth factor (VEGF) agents. Clinical trials and most real-world studies on neovascular age-related macular degeneration (nAMD) generally exclude vitrectomized eyes, and the efficacy of anti-VEGF therapy in this subgroup remains unclear. Aflibercept 8 mg, approved in Japan in 2024, delivers four times the dose of the conventional 2 mg formulation and is designed to improve durability and extend treatment intervals. We report three vitrectomized eyes from three patients with nAMD who exhibited persistent or recurrent exudation despite short-interval (≤8 weeks) aflibercept 2 mg therapy under a treat-and-extend regimen. Switching to aflibercept 8 mg led to the resolution of fluid in all cases and enabled interval extension. No…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
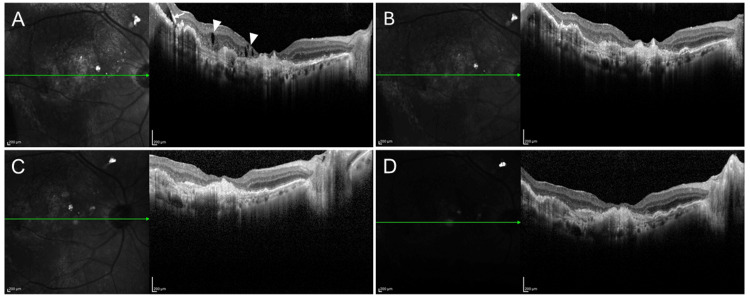 Figure 1
Figure 1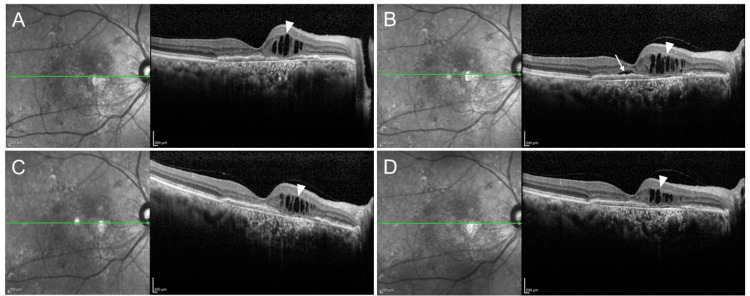 Figure 2
Figure 2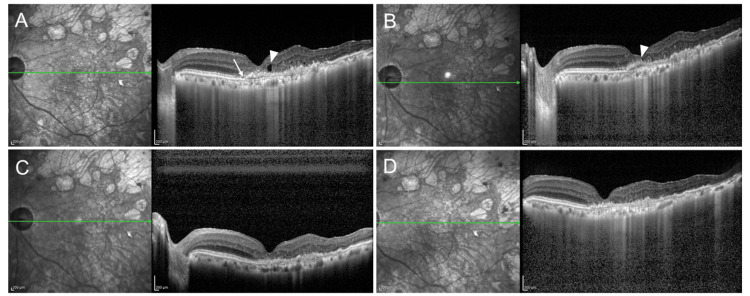 Figure 3
Figure 3| Age* | Sex | MNV subtype | Cause of PPV | Previous treatment for nAMD before PPV | Time between PPV and first injection after PPV (weeks) | Total of treatments for nAMD before switching (times) | Time between PPV and switching (weeks) | Before switching | 6 months after switching | |||||
| BCVA | Intervals (weeks) | Exudation (Y:yes, N:no) | BCVA | Intervals (weeks) | Exudation (Y:yes, N:no) | |||||||||
| Case 1 | 85 | Male | Type 1 MNV | Posterior capsule rupture | IVR ×1 | 4 | IVR ×58, IVA ×53, PDT ×1 | 610 | 20/32 | 5 | N | 20/25 | 8 | N |
| Case 2 | 78 | Male | Type 1 MNV | Lens dislocation (Zinn’s zonule rupture) | IVA ×15 | 6 | IVA ×60 | 391 | 20/32 | 8 | Y (SRF+) | 20/40 | 8 | Y (SRF-) |
| Case 3 | 84 | Female | PCV | Epiretinal membrane | None | 227 | IVF ×3, IVA ×13, PDT ×1 | 670 | 20/32 | 6 | Y | 20/25 | 8 | N |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal Diseases and Treatments · Retinal Imaging and Analysis · Retinal and Optic Conditions
Introduction
Neovascular age-related macular degeneration (nAMD), characterized by macular neovascularization (MNV), is one of the leading causes of severe visual impairment among the elderly worldwide [1]. Intravitreal injections of anti-vascular endothelial growth factor (VEGF) agents have substantially improved both visual and anatomical outcomes, as demonstrated in large randomized clinical trials [2-7]. Currently, anti-VEGF therapy is the first-line treatment for nAMD, and the treat-and-extend regimen is widely adopted to balance efficacy with a reduced treatment burden.
However, most pivotal trials and real-world studies have excluded eyes that have undergone pars plana vitrectomy (PPV), leaving uncertainty regarding treatment efficacy in this subgroup. The vitreous gel, composed of collagen and glycosaminoglycans, acts as a barrier to drug diffusion [8], and its removal may accelerate intraocular drug clearance and shorten the half-life of anti-VEGF agents. Previous reports, including those by Mun et al. [9] and several case studies [10-13], have shown that anti-VEGF therapy can still provide anatomical and visual benefits after vitrectomy; however, the evidence remains limited.
In Japan, multiple anti-VEGF agents are available, including ranibizumab [3], aflibercept (2 mg [4] and 8 mg [5]), brolucizumab [6], and faricimab [7]. The 8 mg aflibercept formulation, approved in April 2024, delivers four times the dose of the conventional 2 mg injection and has been shown in the PULSAR trial to maintain efficacy with extended dosing intervals in treatment-naïve nAMD [5]. Its high molar concentration and prolonged VEGF suppression may offer advantages in vitrectomized eyes, where drug clearance may be increased.
Here, we report three cases of vitrectomized eyes with nAMD in which switching from aflibercept 2 mg to aflibercept 8 mg improved exudative control and enabled interval extension.
Case presentation
We reviewed all vitrectomized eyes with nAMD that were treated at Chiba University Hospital between September and December 2024. During this period, 20 eyes from 20 patients received anti-VEGF therapy. Among these, three eyes of three patients were switched from aflibercept 2 mg to aflibercept 8 mg, and all were included in this report. Each patient completed at least six months of follow-up after the switch. The cases are presented in detail in Table 1.
Case 1
An 85-year-old man with type 1 MNV had received anti-VEGF therapy for approximately 11 years. During the second intravitreal injection (ranibizumab), a lens injury occurred, leading to posterior capsule rupture and cataract progression. The patient subsequently underwent cataract extraction, PPV with posterior vitreous detachment (PVD) induction, and on-the-bag intraocular lens (IOL) implantation. His treatment history included 58 ranibizumab injections, followed by 53 aflibercept injections (2 mg), and one session of photodynamic therapy (Table 1).
Despite continuous administration of aflibercept 2 mg every five weeks, persistent exudation remained, and best-corrected visual acuity (BCVA) was 20/32 (Figure 1A). Switching to aflibercept 8 mg led to complete resolution of exudation at the same five-week interval, and the BCVA improved to 20/25 (Figure 1B-1C). A dry macula and a BCVA of 20/25 were maintained after extending the interval to eight weeks (Figure 1D).
OCT images of a vitrectomized eye with nAMD(A) Five weeks after the administration of aflibercept 2 mg, IRF (arrowheads) and SRF (arrow) were observed; VA was 20/32.(B) Five weeks after switching to aflibercept 8 mg, no IRF or SRF was observed; the VA was 20/25.(C) Five weeks after the second aflibercept 8 mg injection: a dry macula was achieved; the VA was 20/25.(D) Eight weeks after the third aflibercept 8 mg injection: a dry macula was maintained; the VA was 20/25.IRF, intraretinal fluid; SRF, subretinal fluid; OCT, optical coherence tomography; nAMD, neovascular age-related macular degeneration; VA, visual acuity
Case 2
A 77-year-old man with a type 1 MNV underwent PPV with intrascleral IOL fixation for zonular rupture. Over 7.5 years of nAMD treatment, he received 45 aflibercept 2 mg injections. At six-week intervals, no subretinal fluid (SRF) was observed, and BCVA was 20/40 (Figure 2A); however, SRF recurred and BCVA improved to 20/32 when the interval was extended to eight weeks (Figure 2B). After switching to aflibercept 8 mg, the SRF resolved at the same eight-week interval, and BCVA was maintained at 20/32 (Figure 2C). The absence of SRF was preserved, and BCVA was stable at 20/40 after the second injection (Figure 2D).
OCT images of a vitrectomized eye with nAMD(A) Six weeks after aflibercept 2 mg administration: IRF (arrowhead) was observed, SRF was absent; VA was 20/40.(B) Eight weeks after aflibercept 2 mg administration: SRF (arrow) appeared; VA was 20/32.(C) Eight weeks after switching to aflibercept 8 mg: SRF resolved; VA was 20/32.(D) Eight weeks after the second aflibercept 8 mg injection: absence of SRF was maintained; VA was 20/40.IRF, intraretinal fluid; SRF, subretinal fluid; OCT, optical coherence tomography; nAMD, neovascular age-related macular degeneration; VA, visual acuity
Case 3
An 83-year-old woman underwent PPV and cataract surgery for an epiretinal membrane secondary to a branch retinal vein occlusion. Ten years later, she was diagnosed with polypoidal choroidal vasculopathy and received 10 injections of aflibercept 2 mg over 1.5 years. At eight-week intervals, both SRF and intraretinal fluid (IRF) were present, and BCVA was 20/32 (Figure 3A). Shortening the interval to six weeks reduced IRF, eliminated SRF, and maintained the BCVA at 20/32 (Figure 3B). Switching to aflibercept 8 mg resulted in complete IRF resolution at eight-week intervals, with BCVA of 20/32 (Figure 3C). A dry macula and a BCVA of 20/40 were maintained after the second injection (Figure 3D).
OCT images of a vitrectomized eye with nAMD(A) Eight weeks after aflibercept 2 mg administration: IRF (arrowhead) and SRF (arrow) were observed; VA was 20/32.(B) Six weeks after aflibercept 2 mg administration: IRF decreased compared to the 8-week interval; SRF was absent; VA was 20/32.(C) Eight weeks after switching to aflibercept 8 mg: IRF resolved; VA was 20/32.(D) Eight weeks after the second aflibercept 8 mg injection: a dry macula was maintained; VA was 20/40.IRF, intraretinal fluid; SRF, subretinal fluid; OCT, optical coherence tomography; nAMD, neovascular age-related macular degeneration; VA, visual acuity
Discussion
We report three vitrectomized eyes with nAMD in which switching from aflibercept 2 mg to aflibercept 8 mg resulted in anatomical improvement and allowed interval extension. These findings suggest that aflibercept 8 mg can provide enhanced durability even in eyes in which drug clearance may be accelerated.
However, the pharmacokinetic effects of vitrectomy on intravitreal anti-VEGF agents remain unclear. Although some animal studies have reported unchanged clearance [14,15], others have reported significantly faster clearance after PPV [16,17]. These discrepancies may stem from differences in PVD completeness, residual vitreous gel, surgical techniques, or concomitant lensectomy [9]. All our patients underwent complete PVD induction and lens extraction, potentially increasing the clearance risk; however, aflibercept 8 mg achieved sufficient VEGF suppression.
The PULSAR trial demonstrated the non-inferiority of aflibercept 8 mg administered every 12 or 16 weeks compared with 2 mg every eight weeks in treatment-naïve nAMD, with over 80% of patients maintaining ≥12-week intervals [5]. Real-world data have also indicated significant efficacy and durability in reducing exudative changes and extending treatment intervals with 8 mg [18,19]. However, vitrectomized eyes were excluded, and our cases suggest that, despite possible accelerated clearance, a higher dose can maintain efficacy in this subgroup.
No ocular inflammation was observed, alleviating concerns about higher molar concentrations and increased inflammatory risk. In addition, long-term follow-up is warranted to monitor the development and progression of macular atrophy. Our study was limited by its retrospective, single-center design, small sample size, and short follow-up period. Larger prospective studies are required to validate these findings.
Conclusions
In our small series, switching from aflibercept 2 mg to aflibercept 8 mg in vitrectomized eyes with nAMD resulted in both anatomical improvement and treatment interval extension without safety concerns. Aflibercept 8 mg may be a viable strategy for patients requiring frequent injections after vitrectomy to reduce the treatment burden. Larger prospective studies are required to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study Lancet Glob Health GBD 2019 Blindness and Vision Impairment Collaborators Vision Loss Expert Group of the Global Burden of Disease Study 06092021
- 2Visual acuity outcomes of anti-VEGF treatment for neovascular age-related macular degeneration in clinical trials Jpn J Ophthalmol Yamashiro K Oishi A Hata M Takahashi A Tsujikawa A 7417606520213449147410.1007/s 10384-021-00869-x · doi ↗ · pubmed ↗
- 3Ranibizumab for neovascular age-related macular degeneration N Engl J Med Rosenfeld PJ Brown DM Heier JS Boyer DS Kaiser PK Chung CY Kim RY 1419143135520061702131810.1056/NEJ Moa 054481 · doi ↗ · pubmed ↗
- 4Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration Ophthalmology Heier JS Brown DM Chong V 2537254811920122308424010.1016/j.ophtha.2012.09.006 · doi ↗ · pubmed ↗
- 5Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (Pulsar): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial Lancet Lanzetta P Korobelnik JF Heier JS 1141115240320243846184110.1016/S 0140-6736(24)00063-1 · doi ↗ · pubmed ↗
- 6HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration Ophthalmology Dugel PU Koh A Ogura Y 728412720203098644210.1016/j.ophtha.2019.04.017 · doi ↗ · pubmed ↗
- 7Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and Lucerne): two randomised, double-masked, phase 3, non-inferiority trials Lancet Heier JS Khanani AM Quezada Ruiz C 72974039920223508550210.1016/S 0140-6736(22)00010-1 · doi ↗ · pubmed ↗
- 8Vitreous humor: composition, characteristics and implication on intravitreal drug delivery Curr Eye Res Mishra D Gade S Glover K Sheshala R Singh TR 2082184820233603647810.1080/02713683.2022.2119254 · doi ↗ · pubmed ↗