Intravenous umbilical cord-derived mesenchymal stromal cell therapy may improve overall survival in Japanese patients with idiopathic pneumonia syndrome after hematopoietic stem cell transplantation: a multicenter, single-arm, phase II trial
Noriko Doki, Nobuharu Fujii, Shinichi Kako, Emiko Sakaida, Yoshinobu Kanda

TL;DR
A clinical trial suggests that umbilical cord-derived cells may improve survival in patients with a severe lung condition following stem cell transplants.
Contribution
This study is the first to show potential efficacy of umbilical cord-derived mesenchymal stromal cells in treating refractory idiopathic pneumonia syndrome.
Findings
The survival rate at day 56 was 71.4% in patients treated with HLC-001.
HLC-001 was generally well tolerated with no serious adverse events reported.
Abstract
Idiopathic pneumonia syndrome (IPS) is a serious complication of allogeneic hematopoietic stem cell transplantation (HSCT) and has a poor prognosis. Although IPS is often treated with steroids, the disease can become resistant to or dependent on steroid treatment, and there is no effective cure for patients with refractory or steroid-dependent IPS. This multicenter, open-label, single-arm, phase II clinical trial investigated the efficacy and safety of HLC-001 (allogeneic umbilical cord-derived mesenchymal stromal cells) in patients with progressive steroid-dependent or refractory IPS after HSCT. Seven male patients (all male; mean age: 43.3 years) received HLC-001 and three completed the trial. The survival rate at day 56 (primary endpoint) was 71.4% (5/7 patients; 95% confidence interval: 29.0%–96.3%) and was sustained at day 100, suggesting that HLC-001 was more effective than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
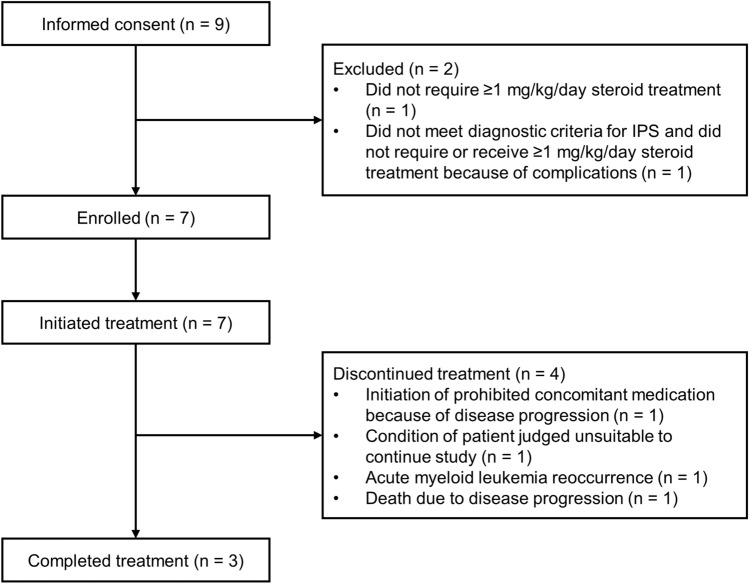 Figure 1
Figure 1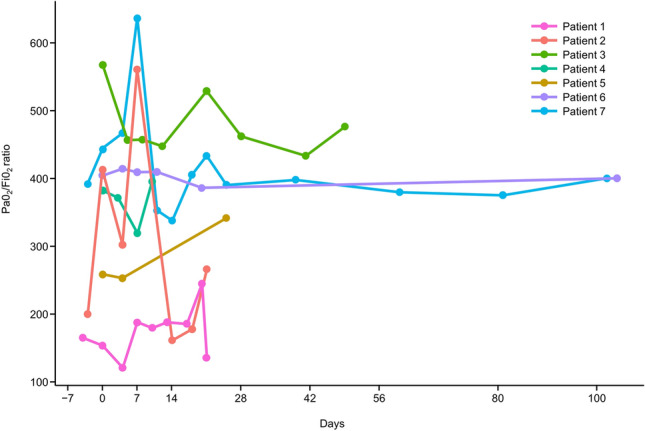 Figure 2
Figure 2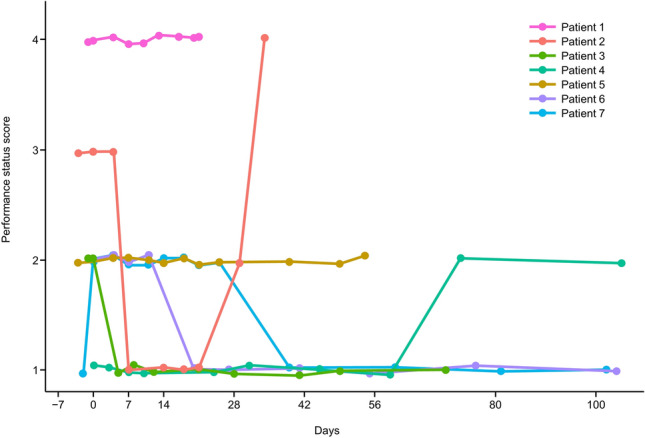 Figure 3
Figure 3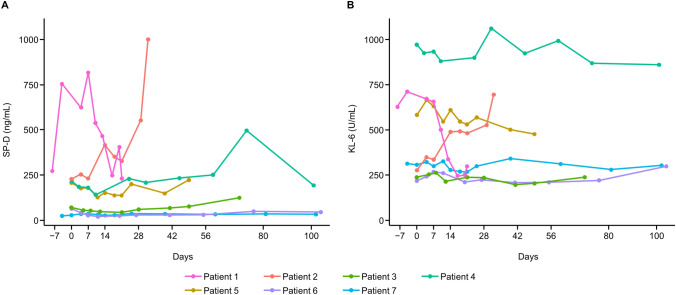 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Mesenchymal stem cell research
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) can result in serious complications with poor prognoses, including idiopathic pneumonia syndrome (IPS) [1]. IPS after allogeneic HSCT has a reported incidence of 3.7%–12.0%, and is commonly treated with steroid therapy [2–5]. However, the condition can be difficult to control and may become steroid-dependent or resistant to treatment. Multiple studies have indicated that the inflammatory cytokine tumor necrosis factor (TNF)-α plays a significant role in the onset and progression of IPS [6, 7]. A phase III, randomized, double-blind, placebo-controlled trial evaluating the efficacy of etanercept, a soluble TNF receptor, in treating IPS was conducted; however, it did not achieve its primary endpoints, failing to demonstrate significant efficacy. [8]. Neither steroid-dependent nor refractory IPS have an effective cure and are associated with rapid deterioration and a high mortality rate [1, 2, 7, 9]. Therefore, there is a need for new, effective treatment options for progressive steroid-dependent and refractory IPS.
IPS has clinical characteristics that are very similar to graft-versus-host disease (GVHD) [10]. Mesenchymal stromal cells (MSCs) have been reported to have therapeutic effects against these conditions. Among MSCs, umbilical cord-derived MSCs have advantages over MSCs derived from other tissues: they can be harvested from tissues that are usually discarded without causing any harm or physical burden to the donor, and they have a high proliferative capacity [11, 12]. Their potential therapeutic uses have been investigated in a variety of conditions, including GVHD, hematologic disorders, neurological disorders, diabetes mellitus, and other diseases [11, 12].
HLC-001 is an allogeneic umbilical cord-derived MSC product manufactured by the Institute of Medical Science (University of Tokyo) [13]. When activated by inflammatory cytokines (such as interferon-γ and TNF-α) at the site of inflammation or tissue damage, these cells exert an anti-inflammatory effect and contribute to tissue repair [13].
HLC-001 treatment has been shown to be effective and well tolerated in patients with acute GVHD [13]. As mentioned above, because the clinical conditions of IPS are very similar to those of GVHD and acute respiratory distress syndrome, HLC-001 may be an effective treatment for IPS after HSCT. However, the effects of umbilical cord-derived MSCs on IPS are still unknown.
We conducted this trial to investigate the efficacy and safety of HLC-001 treatment in Japanese patients with progressive steroid-dependent or refractory IPS after HSCT and report the results herein. Given the absence of effective treatments for these patients and their poor prognosis, there was no placebo control in this phase II trial.
Methods
Study design and treatment
This multicenter, open-label, single-arm, phase II clinical trial was conducted in Japan. Patients (≥ 16 years) with progressive steroid-dependent or refractory IPS after HSCT were enrolled between October 2022 and June 2023. IPS was defined based on a statement from the American Thoracic Society [7]. Briefly, IPS was defined as the presence of widespread alveolar injury confirmed by chest imaging; absence of lower respiratory tract infection, as determined by bronchoalveolar lavage (BAL); and no identifiable cardiac, renal, or iatrogenic etiology. Corticosteroid-treated IPS (≥ 1 mg/kg/day prednisolone or equivalent) that deteriorated after 3 days of treatment, or did not improve after 5 days of treatment, was defined as steroid-dependent/refractory IPS. All patients were required to undergo bronchoscopy with BAL at trial entry. The detailed study design is described in the Supplementary Methods.
Patients received HLC-001 intravenously at a dose of 2 × 10^6^ cells/kg, once daily, for two doses per cycle at intervals between 2 and 7 days, for a maximum of four cycles and eight doses. The dose of HLC-001 was determined based on the results of a phase I trial of HLC-001 in patients with acute GVHD [13]. This dose was tolerated in the previous study and is equivalent to the clinical dose of Temcell^®^ HS (JCR Pharmaceuticals Co., Ltd., Ashiya, Japan) injection, which is a bone marrow-derived mesenchymal stem cell treatment.
The trial was approved at participating sites (Table S1) by the relevant institutional review boards, registered with the Japan Registry of Clinical Trials (jRCT2063220014), and conducted in accordance with the principles of the Declaration of Helsinki, Good Clinical Practice, and applicable local regulations. Patients or their legal guardian provided written informed consent prior to enrollment.
Study endpoints
The primary endpoint was overall survival at 56 days after treatment initiation. Secondary endpoints were overall survival at day 100; percentage of patients not undergoing mechanical ventilation at days 28, 56, and 100; number of days without mechanical ventilation from treatment initiation to days 28, 56, and 100; percentage of patients who did not require an increase in oxygen dose, percentage of patients not requiring oxygen treatment and percentage of patients with oxygen dose reduced by ≥ 50% on days 28, 56, and 100; number of days in which increased oxygen administration was not required, time period during which oxygen administration was not required and period during which the reduction in oxygen dose by ≥ 50% was achieved on days 28, 56, and 100; percentage of patients with corticosteroid dose decreased to < 1 mg/kg/day and the amount reduced; partial pressure of oxygen in arterial blood (PaO_2_) and fraction of inspired oxygen (FiO_2_) ratio; evaluation of chest X-ray/computed tomography (CT) scans; Eastern Cooperative Oncology Group performance status (ECOG-PS) scores [14]; surfactant protein-D (SP-D) and Krebs von den Lungen-6 (KL-6) levels at each time point up to day 100; and adverse events (AEs) and their severity according to the Common Terminology Criteria for Adverse Events. Exploratory endpoints included changes in cytokines, chemokines, and immune cells before each dose and on days 28 and 56. Further details are described in the Supplementary Methods.
Statistical methods
This analysis was conducted based on the Thall & Simon Bayesian design (TS design) [15] (described in the Supplementary Methods). A sensitivity analysis was performed for the primary endpoint, including calculation of survival rates and their 95% Clopper–Pearson confidence intervals (CIs) and the 95% highest posterior density intervals for the posterior distribution of the survival probability of the treatment under an uninformed prior distribution. According to the TS design criteria, the minimum number of survivors required to indicate that HLC-001 was more effective than existing therapies is summarized in Table 1. The planned sample size ranged from a minimum of six to a maximum of twenty patients. Summary statistics were calculated for patient backgrounds and secondary endpoints. Statistical analyses were conducted using R Statistical Software (v4.3.0) [16].Table 1. Minimum number of survivors required to demonstrate efficacy (Thall & Simon Bayesian design)Enrolled number67891011121314151617181920Minimum number of survivors5556667788899910
Results
Patients and HLC-001 treatment
The patient disposition is shown in Fig. 1. Nine patients provided informed consent, and two patients were withdrawn during the screening period as they did not meet the eligibility criteria. Seven patients were enrolled, received HLC-001, and were included in the analysis population. Of these, four withdrew after treatment and three completed the trial.Fig. 1. Patient disposition. IPS, idiopathic pneumonia syndrome
The full analysis set, per-protocol set, and safety analysis set were identical populations, and the baseline characteristics are shown in Table 2. All patients were male, and the mean ± standard deviation (SD) age of patients was 43.3 ± 14.5 years. The rates of acute myeloid leukemia, acute lymphoblastic leukemia, and non-Hodgkin lymphoma were 57.1% (4/7), 28.6% (2/7), and 14.3% (1/7), respectively.Table 2. Patient characteristicsCharacteristicPatientsMale7 (100.0)Age, years43.3 ± 14.543.0 (21–64)Height, cm166.63 ± 5.02166.20 (158.0–171.8)Weight, kg53.40 ± 6.8251.50 (46.1–66.9)White blood cells, × 10^3^/µL9.830 ± 5.72610.510 (4.20–19.90)CRP, mg/dL0.896 ± 0.8790.620 (0.05–2.22)KL-6, U/mL472.1 ± 289.8307.0 (218–971)SP-D, ng/mL224.10 ± 247.91208.00 (27.8–754.0)PaO_2_/FiO_2_, mmHg374.81 ± 133.21404.80 (154.0–566.7)Corticosteroid dose, mg/kg/day1.44 ± 0.831.28 (0.4–3.0)Hematopoietic malignancy type Acute myeloid leukemia4 (57.1) Acute lymphoblastic leukemia2 (28.6) Non-Hodgkin lymphoma1 (14.3)Pre-treatment conditioning regimen Myeloablative conditioning6 (85.7) Non-myeloablative conditioning1 (14.3)Chemotherapy Busulfan3 (42.9) Fludarabine7 (100.0) Melphalan3 (42.9) Other6 (85.7)Donor and recipient HLA types Mismatched related donor2 (28.6) Matched unrelated donor4 (57.1) Mismatched unrelated donor1 (14.3)Hematopoietic stem cell source Peripheral blood5 (71.4) Bone marrow2 (28.6)Acute GVHD6 (85.7)Chronic GVHD3 (42.9)Prophylaxis for GVHD2 (28.6)ECOG performance status 11 (14.3) 24 (57.1) 31 (14.3) 41 (14.3)Oxygen therapy4 (57.1) Oxygen therapy without mechanical ventilation or non-invasive positive pressure ventilation3 (42.9) Mechanical ventilation or non-invasive positive pressure ventilation1 (14.3)n = 7, unless otherwise stated. Data are shown as n (%) or mean ± standard deviation and median (range)CRP c-reactive protein, ECOG Eastern Cooperative Oncology Group, FiO2 fraction of inspired oxygen, GVHD graft-versus-host disease, HLA human leukocyte antigen, KL-6 Krebs von den Lungen-6, PaO2 partial pressure of oxygen in arterial blood, SP-D surfactant protein-D, SpO2 saturation of peripheral oxygen
The types of conditioning regimen were myeloablative conditioning in 85.7% (6/7) of patients and non-myeloablative conditioning in 14.3% (1/7). The donor and recipient human leukocyte antigen types were mismatched related donor in 28.6% (2/7) of patients, matched unrelated donor in 57.1% (4/7), and mismatched unrelated donor in 14.3% (1/7). The hematopoietic stem cell source was peripheral blood in 71.4% (5/7) of patients and bone marrow in 28.6% (2/7). Six (85.7%) patients developed acute GVHD between HSCT and their participation in the trial. Three (42.9%) patients developed chronic GVHD between HSCT and their participation in the trial. Three (42.9%) patients were administered oxygen without mechanical ventilation or non-invasive positive pressure ventilation, and one (14.3%) patient underwent mechanical ventilation.
The median number of HLC-001 doses was 6 (range: 4–8), and the median total dose was 640.0 × 10^6^ cells (range: 368–1064 × 10^6^ cells). All patients (7/7) completed two cycles of treatment. For patients who received additional doses, 57.1% (4/7) of patients received treatment up to the fifth administration (cycle 3), 57.1% (4/7) received up to the sixth administration (cycle 3), 42.9% (3/7) received up to the seventh administration (cycle 4), and 28.6% (2/7) received up to the eighth administration (cycle 4). After IPS was evaluated as steroid-dependent or refractory, HLC-001 was administered on the same day or the following day for all subjects.
Overall survival
The survival rate at day 56 (primary endpoint) was 71.4% (5/7) (95% CI: 29.0%–96.3%). As the primary endpoint was met in at least five patients, the trial was terminated at the end of the final observation of the seven patients, which suggested that HLC-001 was more effective than the existing therapy, according to the TS design.
On day 100, the survival rate remained 71.4% (5/7) (95% CI: 29.0%–96.3%). Among the five patients evaluated for survival after 100 days of treatment, three deaths occurred (caused by worsening IPS, relapse of acute myeloid leukemia, and an unknown cause). The total number of days of survival for these patients was 155, 204, and 246 days, respectively (Table 3).Table 3. Individual patient backgrounds and outcomesPatient 1Patient 2Patient 3Patient 4Patient 5Patient 6Patient 7Age64214349563634Hematopoietic malignancy typeAMLAcute lymphoblastic leukemiaAMLAMLAcute lymphoblastic leukemiaAMLNon-Hodgkin lymphomaPre-treatment conditioning regimen (TBI)Myeloablative procedures (No)Myeloablative procedures (12 Gy)Myeloablative procedures (4 Gy)Myeloablative procedures (4 Gy)Myeloablative procedures (4 Gy)Myeloablative procedures (4 Gy)Non-myeloablative procedures (2 Gy)Hematopoietic stem cell sourcePeripheral bloodPeripheral bloodBone marrowPeripheral bloodBone marrowPeripheral bloodPeripheral bloodDonor and recipient HLA typesMatched unrelated donorMismatched related donorMatched unrelated donorMismatched related donorMismatched unrelated donorMatched unrelated donorMatched unrelated donorTime from HSCT to HLC-001 administration, days109158148239189128687Acute GVHDYes^a^YesYesYesYesNoYesChronic GVHDNoNoYesYes^a^NoNoYes^a^Corticosteroid dose^b^ (mg/kg/day)25.127.31.3≧ 1.01.11.31.0P/F ratio154413566.7382.1258.3404.8444.8Oxygen therapyYesYesNoYesYesNoNoInitial oxygen doseWith mechanical ventilation30 L/min–2 L/min4 L/min––Mechanical ventilationYesNoNoNoNoNoNoOutcomeDied on day 50 (IPS)Died on day 35 (IPS)Died on day 204 (relapsed AML)Died on day 246 (unknown cause)Died on day 155 (IPS)Alive on day 485Alive on day 729AML acute myeloid leukemia, GVHD graft-versus-host disease, HLA human leukocyte antigen, HSCT hematopoietic stem cell transplantation, IPS idiopathic pneumonia syndrome, P/F ratio partial pressure of oxygen in arterial blood (PaO_2_) and fraction of inspired oxygen (FiO_2_) ratio, TBI total body irradiation^a^Acute or chronic GVHD was observed at the time of HLC-001 administration^b^Maximum dose (prednisolone or equivalent) before HLC-001 administration
Mechanical ventilation and oxygen treatment
The percentage of patients who were not receiving mechanical ventilation was 85.7% (6/7) at all evaluated time periods (95% CI: 42.1%–99.6%). The mean ± SD number of days during which mechanical ventilation was not used at days 28, 56, and 100 were 24.0 ± 10.6 days, 44.9 ± 21.2 days, and 65.9 ± 38.6 days, respectively (Table 4).Table 4. Days without mechanical ventilationAssessment periodDays without mechanical ventilationDay 0 to day 2824.0 ± 10.628.0 (0–28)Day 0 to day 5644.9 ± 21.256.0 (0–56)Day 0 to day 10065.9 ± 38.671.0 (0–100)n = 7. Data are shown as mean ± standard deviation, or median (range). Data from patients who died or discontinued before each evaluation time period were imputed using the data up to the time of death or discontinuation
The percentages of patients who did not require an increase in oxygen dose on days 28, 56, and 100 were 85.7% (6/7) (95% CI: 42.1%–99.6%), 71.4% (5/7) (95% CI: 29.0%–96.3%), and 71.4% (5/7) (95% CI: 29.0%–96.3%), respectively.
The percentage of patients who did not require oxygen administration was 57.1% (4/7) (95% CI: 18.4%–90.1%) on days 28, 56, and 100. Among patients who required oxygen administration (3/7), the percentages of patients who had oxygen treatment reduced by ≥ 50% on days 28, 56, and 100 were 100.0% (3/3) (95% CI: 29.2%–100.0%), 66.7% (2/3) (95% CI: 9.4%–99.2%), and 66.7% (2/3) (95% CI: 9.4%–99.2%), respectively.
The mean ± SD number of days on which an increase in oxygen dose was not required (n = 7) were 24.0 ± 10.6 days, 44.3 ± 21.6 days, and 65.3 ± 39.1 days at days 28, 56, and 100, respectively. The mean ± SD number of days on which oxygen administration was not required were 15.4 ± 14.5 days, 31.4 ± 29.4 days, and 52.4 ± 50.0 days at days 28, 56, and 100, respectively. Among patients who required oxygen administration (n = 3), the mean ± SD number of days for which a ≥ 50% reduction in oxygen dose was possible were 19.3 ± 9.9 days, 34.0 ± 15.7 days, and 48.7 ± 41.0 days on days 28, 56, and 100, respectively.
Corticosteroid dose
The mean ± SD corticosteroid dose was 1.2 ± 1.9 mg/kg/day, and the mean ± SD total corticosteroid dose was 2607.5 ± 3310.2 mg. The percentage of patients who were able to reduce their corticosteroid dose to < 1 mg/kg/day was 83.3% (5/6) (95% CI: 35.9%–99.6%). One patient was not included in this analysis because the daily corticosteroid dose was < 1 mg/kg/day at treatment initiation. The mean ± SD reduction in corticosteroid dose was 0.96 ± 0.42 mg/kg.
Oxygen saturation
The PaO_2_/FiO_2_ ratio is shown in Fig. 2. A temporary improvement in PaO_2_/FiO_2_ ratio was observed for two patients (Patient 2 and Patient 7) during the early stages of administration. Although overall fluctuations in values were noted, corresponding to the patients’ conditions, no cases showed a marked worsening in PaO_2_/FiO_2_ during the evaluation period.Fig. 2. Partial pressure of oxygen in arterial blood and fraction of inspired oxygen ratio over time. Change over time in the ratio of partial pressure of oxygen in arterial blood and fraction of inspired oxygen of HLC-001-treated patients with idiopathic pneumonia syndrome after hematopoietic stem cell transplantation. PaO_2_, partial pressure of oxygen in arterial blood; FiO_2_, fraction of inspired oxygen
Imaging results and ECOG-PS scores
Improvements were seen on chest X-ray images in 66.7% (4/6) of patients on day 28 and 60.0% (3/5) of patients on day 56. At day 100, 33.3% (1/3) of patients had improvements on their chest x-ray images and 66.7% (2/3) had no changes.
Regarding chest CT images, improvements were seen in 66.7% (4/6) of patients on day 28 and 40.0% (2/5) of patients on day 56. At day 100, 66.7% (2/3) of patients had improvements on their CT images and 33.3% (1/3) had no changes.
Three patients had improved ECOG-PS scores over time (Patients 3, 6, and 7), and two patients had no change in ECOG-PS scores (Patients 1 and 5). Worsened ECOG-PS scores were observed in two patients (Patients 2 and 4). For one patient (Patient 2), the ECOG-PS score temporarily improved and then deteriorated at treatment discontinuation (Fig. 3).Fig. 3. Eastern Cooperative Oncology Group performance status scores^a^ over time. Change over time in Eastern Cooperative Oncology Group performance status scores of HLC-001-treated patients with idiopathic pneumonia syndrome after hematopoietic stem cell transplantation. ^a^0 = Fully active, able to carry on all pre-disease performance without restriction; 1 = Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light housework, office work; 2 = Ambulatory and capable of all selfcare but unable to carry out any work activities, up and about more than 50% of waking hours; 3 = Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours; 4 = Completely disabled, cannot carry out any selfcare, totally confined to bed or chair
Serum biomarkers
Changes in SP-D and KL-6 levels over time are shown in Fig. 4. SP-D and KL-6 levels increased over time in one patient (Patient 2) and decreased over time in another patient (Patient 1). There were no notable changes over time observed in the other patients.Fig. 4SP-D and KL-6 levels over time. Change over time in (A) SP-D levels and (B) KL-6 levels of HLC-001-treated patients with idiopathic pneumonia syndrome after hematopoietic stem cell transplantation. SP-D, surfactant protein-D; KL-6, Krebs von den Lungen-6
Safety
All patients experienced AEs, and a total of 57 AEs were reported (Table 5). A total of 30 adverse drug reactions (ADRs) were reported, and 71.4% (5/7) of patients experienced at least one ADR (Table S2). No AEs of Grade 4 or 5 severity were observed. Regarding Grade 3 events, there were eight infusion-related events (14.3%) (1/7 patients), four pneumothorax events (28.6%) (2/7 patients), one hyperglycemia (14.3%), one pneumonia (14.3%), one COVID-19 infection (14.3%), one decreased platelet count event (14.3%), and one hypertension event (14.3%). Of these, the infusion-related reactions and hypertension were judged to be ADRs. Six serious AEs occurred in 57.1% (4/7) of patients (four pneumothorax events in two [28.6%] patients, one COVID-19 infection in one [14.3%] patient, and one recurrent acute myeloid leukemia event in one [14.3%] patient). All serious AEs were considered unrelated to HLC-001 treatment.Table 5. Adverse eventsEventNumber of eventsPatientsAny adverse events577 (100.0)Metabolism and nutrition disorders44 (57.1) Hypokalemia22 (28.6) Hyperglycemia11 (14.3) Hyperuricemia11 (14.3)Respiratory, thoracic and mediastinal disorders53 (42.9) Pneumothorax42 (28.6) Pneumomediastinum11 (14.3)Vascular disorders63 (42.9) Hypotension41 (14.3) Hypertension11 (14.3) Phlebitis11 (14.3)General disorders and administration site conditions43 (42.9) Pyrexia22 (28.6) Catheter site pain11 (14.3) Edema11 (14.3)Infections and infestations33 (42.9) Pneumonia22 (28.6) COVID-1911 (14.3)Injury, poisoning and procedural complications112 (28.6) Infusion-related reaction81 (14.3) Procedural pain31 (14.3)Nervous system disorders82 (28.6) Headache41 (14.3) Head discomfort41 (14.3)Cardiac disorders22 (28.6) Palpitations11 (14.3) Sinus tachycardia11 (14.3)Psychiatric disorders22 (28.6) Insomnia22 (28.6)Skin and subcutaneous tissue disorders22 (28.6) Rash11 (14.3) Skin exfoliation11 (14.3)Investigations51 (14.3) Oxygen saturation decreased41 (14.3) Platelet count decreased11 (14.3)Blood and lymphatic system disorders11 (14.3) Thrombotic microangiopathy11 (14.3)Ear and labyrinth disorders11 (14.3) Ear discomfort11 (14.3)Gastrointestinal disorders11 (14.3) Hematochezia11 (14.3)Immune system disorders11 (14.3) Seasonal allergy11 (14.3)Neoplasms benign, malignant and unspecified (including cysts and polyps)11 (14.3) Recurrent acute myeloid leukemia11 (14.3)n = 7. Data are shown as n or n (%). Events are described by System Organ Class and Preferred Term according to the Medical Dictionary for Regulatory Activities, Japanese version 26.0
Exploratory endpoints: cytokines, chemokines, and cell assessments
As an exploratory study, an examination of blood cytokines, chemokines, and immune cells was conducted in five patients. These parameters varied among the patients based on their conditions and the number of doses of HLC-001 administered, making it difficult to identify consistent trends. However, natural killer (NK) cell counts tended to increase up to day 28, except for one patient (Patient 2), who died on day 35 due to worsened IPS.
Discussion
IPS is a rare and fatal non-infectious pulmonary complication occurring after HSCT. It is characterized by extremely high short-term mortality and a poor prognosis. Steroid therapy is commonly administered, but the response rate is poor, and there is no established treatment, highlighting the need for developing new therapies. In this clinical trial, the efficacy and safety of HLC-001, an allogeneic umbilical cord-derived MSC, were evaluated as a potential treatment for IPS.
The primary endpoint of this clinical trial was the overall survival rate at day 56 following the initiation of HLC-001 administration. In a frequentist fixed sample size design, the anticipated survival probability at day 56 after the onset of IPS due to HLC-001 would need to be pre-specified, and the corresponding sample size required to detect a significant difference would be estimated. However, there were insufficient data to predict the magnitude of the effect that HLC-001 might have in comparison to existing treatments. Furthermore, when calculating the required sample size based on frequentist methods, a substantially larger sample would have been necessary, which, given the rarity of IPS, was deemed impractical. A key advantage of utilizing a TS design is that it obviates the need to predefine a precise expected survival probability for the study treatment at day 56 after the onset of IPS. Additionally, it is expected that the required sample size to achieve comparable power would be smaller than that of a frequentist fixed sample size design. Moreover, the results of the trial can be summarized as a posterior distribution, allowing for robust inferences within the framework of the prior distribution, even in cases where statistical significance is not achieved, in contrast to the hypothesis testing framework of frequentist designs. For these reasons, we selected a TS design for this phase II trial.
In this study, five of the seven patients who received HLC-001 were alive 56 days after the start of treatment (overall survival rate: 71.4% [95% CI: 29.0%–96.3%]). Based on the TS design, this suggests that HLC-001 was more effective than the existing treatments. In the TS design, the survival probability at 56 days after the onset of IPS with existing treatments was estimated to be 24.5% based on a mathematical integration of results from 126 cases [3–5]. The 95% CI for the overall survival rate at day 56 after HLC-001 administration exceeded this 24.5% estimate for existing treatments. Furthermore, the survival rate at day 100 after administration remained comparable to that at day 56, indicating sustained survival up to day 100 after administration. According to other studies, approximately 80% of patients with IPS die within 100 days of onset [2–5]. When compared to these studies, HLC-001 appeared to improve survival rates up to 100 days after IPS onset. Of the patients in our study who we were able to observe past 100 days, there were three deaths within a year of HLC-001 administration, attributed to worsening of IPS (Patient 5), relapse of acute myeloid leukemia (Patient 3), and an unknown cause (Patient 4). The 1-year survival rate after HLC-001 administration was 28.6% (2 out of 7 cases). Literature reports indicate that deaths due to causes other than worsening of IPS increase after 100 days from onset [5, 17]. Given the rapid progression and high mortality rate for IPS within the first 100 days of symptom onset, improving survival rates up to this time point is clinically significant, as deaths due to causes other than worsening of IPS increase after 100 days from onset.
In this study, the need for mechanical ventilation among patients was low, with only one patient requiring mechanical ventilation during the trial. Additionally, four of the seven patients (57.1%) did not require oxygen administration on days 28, 56, or 100. Patients with IPS who require mechanical ventilation have a poor prognosis, with a reported 90% mortality rate [7, 18]. Given that most patients in this trial did not require mechanical ventilation or an increase in oxygen support, HLC-001 may help prevent the progression of IPS and reduce the need for mechanical ventilation. Moreover, the steroid dose was reduced to < 1 mg/kg in five out of six patients, and most patients who were still alive at day 100 showed either improvements or stability in PaO_2_/FiO_2_, imaging findings, PS scores, SP-D, and KL-6 levels. Together, these findings suggest that HLC-001 may help prevent progression of IPS.
In the safety evaluation of HLC-001, all patients experienced AEs and 71.4% of patients experienced ADRs. There were no Grade 4 or 5 events. Grade 3 events included infusion-related reactions (eight events; one patient), pneumothorax (four events; two patients), and one event each of hyperglycemia, pneumonia, COVID-19, decreased platelet count, and hypertension. Both the infusion-related reactions and hypertension were considered related to the study drug. The infusion-related reactions occurred in one patient on the day of HLC-001 administration, and this was managed by adjusting the infusion rate and temporarily suspending drug administration. Hypertension occurred in one patient 14 days after the first administration of HLC-001; however, it was not possible to follow up on the outcome as the patient subsequently died due to worsening of IPS. The serious AEs were pneumothorax in two patients, COVID-19 (one patient), and relapsed acute myeloid leukemia (one patient), but no serious AEs were related to HLC-001. As an important point, all AEs were manageable, suggesting HLC-001 is generally well tolerated in patients with IPS.
Additionally, exploratory studies were conducted to measure blood cytokines, chemokines, and immune cells. In the patients who were alive at day 100, there was a trend towards an increase in NK cells. This is consistent with the results of a phase I trial of HLC-001 for acute GVHD [13], which also reported a trend towards increased NK cell count in the patients who responded to treatment. Although the clinical significance of this increase in NK cell count in patients who responded favorably to HLC-001 is unknown, it is a very interesting finding and further research is expected in the future.
This trial had some limitations, including the small population size (seven patients). Additionally, all patients included in this trial were male; therefore, any potential sex differences could not be evaluated. In this clinical trial, only patients capable of receiving an explanation and providing informed consent were enrolled. Finally, the use of BAL at study entry could have influenced disease severity. When compared with retrospective studies and data, these factors could have potentially introduced selection bias. Despite these limitations, the reported findings are clinically important as steroid-dependent and refractory IPS currently has no cure.
In conclusion, this trial found that HLC-001 treatment was effective and generally well tolerated in Japanese patients with steroid-dependent or refractory IPS after HSCT. As there is no effective cure for IPS once it becomes steroid-dependent or resistant, our findings indicate that HLC-001 may be a promising treatment option for affected patients; however, further clinical evaluation is warranted to gather more robust evidence supporting its efficacy and safety.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 40 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eastern Cooperative Oncology Group. Common Toxicity Criteria Version 2.0. 1999. https://jcog.jp/assets/ctcv 20_4-30-992.pdf. Accessed 17 Jan 2025.
- 2R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2023. https://www.R-project.org/.