Therapeutic potential of Licochalcone A in dermatological diseases: from basic to clinical research
Deming Liu, Xue Jiang, Fujin Yang, Jingjing Zhou, Yanxi Li, Hua Yang

TL;DR
Licochalcone A, a natural compound, shows promise in treating various skin conditions by targeting multiple biological pathways.
Contribution
This review highlights Lico-A's therapeutic potential and mechanisms in dermatology, identifying research gaps and future directions.
Findings
Lico-A targets pathways like NLRP3, NF-κB, and Nrf2/HO-1 to modulate inflammation and oxidative stress.
Clinical studies confirm Lico-A's efficacy in reducing skin lesions and improving barrier function.
Current limitations include lack of high-quality trials and geographic bias in research.
Abstract
Licochalcone A (Lico-A), a flavonoid compound extracted from Glycyrrhiza uralensis, exhibiting multiple pharmacological properties including anti-inflammatory, antibacterial, antioxidant, and antitumor effects. It demonstrates significant therapeutic potential in the field of dermatological treatment. This review focuses on the efficacy of Lico-A in the treatment of acne, atopic dermatitis, rosacea, pigmentation disorders, and skin tumors. Mechanistically, Lico-A targets multiple signaling pathways such as NLRP3 inflammasome, NF-κB, PLC/ERK/STAT3, AP-1, and Nrf2/HO-1, thereby modulating inflammatory cascades, oxidative stress, melanogenesis, and tumorigenic processes. Clinical studies have also confirmed its ability to reduce inflammatory lesions, improve skin barrier function, and suppressing hyperpigmentation. However, current research is limited by geographical bias, a lack of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
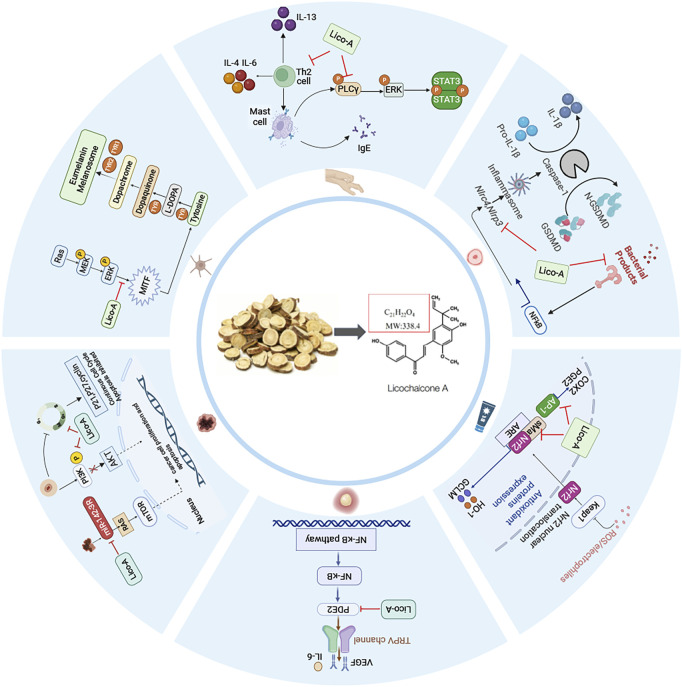 FIGURE 1
FIGURE 1| Disease | Drug | Type of study | Experimental model | Mode of drug administration | Dose range tested | Duration | Main findings | References |
|---|---|---|---|---|---|---|---|---|
| Acne | treatment group: (1) Lico-A/Salicylic acid/L-Carnitine Mixed Solution | Clinical study | 91 Acne patients | topical treatment | — | 8 weeks | A cosmetic regimen containing Lico-A significantly reduced the number of comedones and papules and markedly suppressed sebum secretion in mild acne |
|
| Acne | (1) treatment group: Lico-A/decanediol/L-carnitine/1% salicylic acid moisturizer (2) control group: moisturizer vehicle | Clinical study | 110 Acne patients | topical treatment | — | 20 weeks | Moisturizer containing Lico-A reduced acne lesions and prevented the development of new lesions during the maintenance phase |
|
| Acne | (1) treatment group | Clinical study | 20 patients with acne or seborrheic dermatitis | topical treatment | — | 8 weeks | The moisturizer containing Lico-A exhibits both sebum-suppressive and lipid-modulating effects |
|
| Acne | (1) treatment group: adapalene gel with Lico-A/l-carnitine/1,2-decanediol moisturizers | Clinical study | 120 Acne patients | topical treatment | — | 8 weeks | The combined use of adapalene gel and the moisturizer containing Lico-A demonstrates effect of reducing adverse effects while enhancing therapeutic efficacy |
|
| Acne | (1) treatment group: 7%Glycolic acid/1%salicylic acid/2%gluconolactone/0.05%Lico-A/0.1%adapalene gel cosmeceutical products | Clinical study | 25 Acne patients | topical treatment | — | 4 weeks | The Lico-A-adapalene cosmeceutical combination exhibits non-inferior therapeutic effects to adapalene alone for mild-to-moderate acne, while demonstrating superior tolerability |
|
| Acne | (1) treatment group | Clinical study | 29 Acne patients | topical treatment | — | 10 weeks | Topical application of Lico-A -based cream potentiates the therapeutic effects of photodynamic therapy on acne lesions, while concurrently mitigating post-inflammatory hyperpigmentation |
|
| Acne | (1) treatment group: broad spectrum sunscreen, containing Lico-A, l-carnitine, octocrylene, butyl methoxy dibenzoylmethane, homosalate (2) control group: | Clinical study | 59 Acne patients | topical treatment | — | 6 weeks | Topical application of Lico-A-enhanced sunscreen demonstrates significant preventive effects on post-inflammatory hyperpigmentation following picosecond laser treatment |
|
| AD | (1) treatment group | Clinical study | 55 Childhood atopic dermatitis patients | topical treatment | — | 4 weeks | For atopic dermatitis management, licorice extract exhibits non-inferior therapeutic effects to hydrocortisone butyrate 0.1% cream while demonstrating comparable cutaneous tolerability |
|
| AD | (1) treatment group | Clinical study | 26 Childhood atopic dermatitis patients | topical treatment | — | 6 weeks | The effectiveness of LA lotion is equal to that of HC lotion for childhood atopic dermatitis |
|
| AD | (1) treatment group | Clinical study | 26 Atopic dermatitis patients | topical treatment | — | 12 weeks | Topical application of a Lico-A -based moisturizing cream demonstrates dual benefits in significantly preventing disease flares and preserving epidermal barrier function in atopic dermatitis management |
|
| Facial dermatitis | (1) treatment group: moisturizer containing 4-t-butylcyclohexanol, Lico-A | Clinical study | 80 Facial dermatitis patients | topical treatment | — | 4 weeks | While exhibiting delayed therapeutic onset relative to triamcinolone acetonide, the Lico-A-enriched moisturizer shows clinically significant advantages in erythema reduction and stratum corneum hydration improvement in facial dermatitis patients |
|
| Sensitive skin | (1) treatment group | Clinical study | 38 Sensitive skin patients | topical treatment | — | 24 h | Topical application of 4-t-butylcyclohexanol and Lico-A demonstrates synergistic efficacy in immediately alleviating neurosensory symptoms |
|
| Rosacea | (1) treatment group | Clinical study | 32 Rosacea patients | topical treatment | — | 8 weeks | A Lico-A-based skincare system significantly reduces erythema intensity and improves tactile roughness in reactive skin types |
|
| Sensitive skin | (1) treatment group: combination of trans-t-butylcyclohexanol/Lico-A | Clinical study | 1,221 patients with Sensitive skin or Rosacea | topical treatment | — | 4 weeks | The combination of trans-4-t-butylcyclohexanol and Lico-A demonstrates significant therapeutic efficacy and excellent tolerability in managing sensitive skin and rosacea |
|
| Acne | Lico-A |
| P.acnes-induced Acne mice mouse | local injection | 1.25%–2.5% | 24 h | Lico-A inhibits NLRP3 inflammasome, thereby suppressing inflammation induced by Propionibacterium acnes |
|
| AD | Lico-A |
| IgE-mediated allergic mouse models | gastric lavage | 20–80 mg/kg | 30 min | Licorice chalcone A reduces inflammation in mice, restores hypothermia caused by allergies, and reduces tumor necrosis factor and monocyte chemotactic protein |
|
| Photosensitivity disorders | Lico-A |
| HaCaT cells | - | 1.25–10 μM | 1 h | Lico-A reduces UVR-induced skin tissue damage by targeting the AP-1 transcription factor, inhibits UVR-induced COX-2 expression and PGE2 production |
|
| Photosensitivity disorders | Lico-A |
| Primary human dermal fibroblasts | - | 0.25–2 μM | 24 h | Lico-A could activate the transcription factor Nrf2, inhibit the generation of ROS induced by visible light, reduce the cellular damage caused by oxidative stress, and reduce the consumption of carotenoids in the skin by visible light |
|
| Photosensitivity disorders | Lico-A |
| Primary human fibroblasts | - | 0.25–16 μM | 6h–24 h | Lico-A induces nuclear translocation of Nrf2 and upregulates the expression of HO-1 and GCLM. |
|
| Pigmented skin diseases | Lico-A |
| B16 cells | - | 6.5–104 mg/mL | 24 h | Lico-A inhibits melanin content in B16 cells by phosphorylating ERK, downregulating MITF, and reducing tyrosinase activity |
|
| OSCC | Lico-A |
| HN22 and HSC4 cell lines | - | 0.25–1, 2 | 48 h | Licorice chalcone A significantly inhibits HN22 and HSC4 cells |
|
| OSCC | Lico-A |
| SCC4 and CAL-27 cell lines | - | 25–100 μM | 48 h | Lico-A inhibits SCC4 and CAL-27 cell proliferation |
|
| Melanoma | Lico-A |
| A375 and B16 melanoma cells | - | 5–20 μM | 24h–72 h | Lico-A activates miR-142-3p, promotes the expression of Ras homolog protein, activates the mTOR signaling pathway, inhibits the proliferation of A375 and B16 melanoma cells, and induces apoptosis |
|
| Microsporum canis | Lico-A |
| Microsporum canis ATCC 36299 | - | 0.25–1064 μM | 5–25 h | Lico-A inhibits fungal growth by suppressing ergosterol biosynthesis, reducing ATPase activity to impair energy metabolism, and inhibiting ROS-induced oxidative stress |
|
| Aspergillus fumigatus Keratitis | Lico-A |
| Aspergillus fumigatus Keratitis mice | 12–60 μM | 24h–72 h | Lico-A inhibits ergosterol biosynthesis, disrupts cell membrane integrity, and suppresses the growth of Aspergillus fumigatus |
| |
| Leishmaniasis | Lico-A |
| leishmania | - | 5–10 μg | 20 h | Lico-A can inhibit the growth of Leishmania and Donovaniasis parasites |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacological Effects of Natural Compounds · Phytochemistry and biological activity of medicinal plants · Morinda citrifolia extract uses
1 Introduction
Skin diseases are the fourth leading cause of disability worldwide, affecting approximately one-third of the world’s population (Flohr and Hay, 2021; Trakatelli et al., 2023). In 2019, the burden of skin and subcutaneous diseases, measured in disability-adjusted life years, reached 42,883,695.48, underscoring their substantial impact on global health and the consequent need for effective therapeutic interventions (Yakupu et al., 2023). Current treatment modalities for skin diseases include antibiotics, glucocorticoids, immunosuppressants, and biologics. These agents are often limited by transient efficacy, high relapse rates upon discontinuation, and the emergence of drug resistance. Additionally, some medications are associated with hepatotoxicity and nephrotoxicity, highlighting the urgent demand for safer and more effective alternatives.
Recently, plant-derived natural compounds have emerged as promising therapeutic candidates for dermatological conditions, owing to their low skin irritancy, reduced propensity for resistance development, and ability to modulate skin microbiota (Wang et al., 2025). Among these compounds, licochalcone A (Lico-A), a flavonoid isolated from the roots and stems of Glycyrrhiza uralensis Fisch., has emerged as a promising therapeutic candidate for tumors, infectious diseases, and inflammatory disorders due to its broad-spectrum pharmacological activities including anti-inflammatory, antitumor, antimicrobial, antioxidant, and neuroprotective effects (Li et al., 2024; Liu et al., 2018; Wang et al., 2024). Preliminary clinical evidence suggests that Lico-A alleviates symptoms of acne, rosacea, and atopic dermatitis (AD) while preventing disease recurrence (Olloquequi et al., 2023). (Table 1; Figure 1). Its multi-targeted mechanism of action has further fueled interest in its application for dermatological conditions.
The main targeted signaling pathways and action mechanism of Lico-A in the treatment of dermatologic diseases.
To comprehensively evaluate the therapeutic potential and mechanistic basis of Lico-A in dermatology, we conducted a systematic review of clinical and preclinical studies published in the past decade, sourced from PubMed and Embase. Search terms included “licorice,” “Lico-A,” “skin diseases,” “inflammation,” and “tumors,” among others. This review summarizes the latest advances in the pharmacological research and clinical applications of Lico-A in dermatology, systematically analyzes the advantages and disadvantages of Lico-A in the treatment of various skin diseases and explores future research directions such as its multi-target mechanism and development of novel drug delivery systems.
2 Application of Lico-A in inflammatory dermatological diseases
2.1 Acne vulgaris
Acne vulgaris represents a chronic inflammatory condition of the pilosebaceous unit (Vasam et al., 2023), primarily associated with hyperseborrhea, Cutibacterium acnes colonization, inflammatory cascades, and follicular hyperkeratinization (Reynolds et al., 2024). Lico-A can modulate key pathogenic pathways of acne through multi-target mechanisms, demonstrating significant clinical therapeutic potential. Multiple clinical studies have used topical formulations containing Lico-A for acne patients. Results indicate that these formulations significantly suppress sebum secretion and reduce the formation of comedones, inflammatory papules, and non-inflammatory papules, preventing disease progression (Wongtada et al., 2022; Kulthanan et al., 2020; Dall'Oglio et al., 2019). A randomized controlled trial in an Asian population demonstrated that a moisturizer containing 0.5% Lico-A combined with 0.1% adapalene gel significantly reduced inflammatory and total lesion counts in mild-to-moderate acne, without the initial inflammatory exacerbation commonly observed with retinoid monotherapy (Chularojanamontri et al., 2016). This study confirmed that Lico-A not only mitigates the skin irritation associated with retinoids but also prevents the initial acne flare-up, thereby improving patient adherence.
Additionally, Lico-A has shown beneficial effects when combined with light-based therapies. The combination of Lico-A moisturizer and photodynamic therapy significantly reduced lesion counts in moderate-to-severe acne, enhanced therapeutic efficacy, minimized adverse effects, and markedly decreased post-inflammatory hyperpigmentation (Wanitphakdeedecha et al., 2020). Puaratanaarunkon T’s study further demonstrated that Lico-A cream, when used with picosecond laser treatment, reduced inflammatory papules and hyperpigmentation in acne patients (Puaratanaarunkon and Asawanonda, 2022), outperforming a control group using only conventional ultraviolet filters. These findings further support the safety and efficacy of Lico-A in combination with photodynamic therapy for moderate-to-severe acne.
Further mechanism studies confirmed that Lico-A effectively inhibits P. acnes-induced NLRP3 inflammasome activation, reduces the production of mitochondrial reactive oxygen species (ROS), and subsequently blocks caspase-1 and IL-1β secretion. In murine models, topical application of Lico-A significantly alleviated P. acnes-induced skin inflammation, erythema, and inflammatory cell infiltration, with efficacy comparable to benzoyl peroxide, a clinically standard treatment. Furthermore, Lico-A at concentrations of 10 μM and 20 μM exhibited direct antibacterial activity against P. acnes, reducing its abnormal follicular colonization (Yang et al., 2018). These findings provide a theoretical foundation for the development of Lico-A as a novel anti-acne therapeutic agent.
In summary, Lico-A demonstrates significant efficacy in preventing and treating acne by inhibiting NLRP3 inflammasome activation, reducing mitochondrial ROS production, and exerting direct antibacterial effects. However, current clinical evidence remains limited to small-scale trials with notable geographic bias and lacks long-term safety data. Future research should prioritize larger, high-quality clinical studies and broader mechanistic investigations, including Lico-A’s modulation of C. acnes biofilm formation, sebaceous gland activity, and inflammatory crosstalk.
2.2 Atopic dermatitis
AD is a common chronic relapsing inflammatory disease in dermatology, with type 2 inflammation and barrier dysfunction as important pathogenic mechanisms (Kellogg and Smogorzewski, 2023).The significant inhibition of Th2 cytokines by Lico-A also makes it a potential treatment for AD (Huang et al., 2019; Sherwani et al., 2024).
Multiple clinical studies have demonstrated the efficacy of Lico-A in alleviating AD. Research by Wananukul S et al. revealed that adult AD patients applying Lico-A formulations twice daily for 8 weeks exhibited significant reductions in SCORAD scores, with comparable efficacy to 1% hydrocortisone. Lico-A demonstrated superior outcomes in reducing transepidermal water loss (TEWL), improving skin barrier function, and lowering relapse rates. These findings align with Udompataikul M’s pediatric AD study, collectively indicating that Lico-A not only mitigates AD symptoms but also reduces corticosteroid dependency (Wananukul et al., 2023; Udompataikul and Srisatwaja, 2011). A 12-week double-blind randomized split-face relapse prevention trial further showed that Lico-A emollients reduced relapse rates by 60% in adult AD patients versus controls, significantly alleviating recurrent rash and pruritus while decreasing Staphylococcus aureus colonization and maintaining skin barrier homeostasis, highlighting Lico-A’s long-term therapeutic advantages (Angelova-Fischer et al., 2018). Additionally, a randomized prospective investigator-blinded study confirmed that Lico-A emollients exhibited superior sustained anti-inflammatory effects and skin hydration compared to 0.02% triamcinolone cream in facial AD, suggesting its potential for treating region-specific AD (Boonchai et al., 2018). Mechanistically, beyond Th2 cytokine modulation, Shu et al. (2022) demonstrated in an IgE-mediated murine allergy model that Lico-A suppresses PLC/ERK/STAT3 signaling, thereby inhibiting mast cell activation and reducing tumor necrosis factor-α (TNF-α) and MCP-1 release to attenuate inflammatory responses—further elucidating its anti-allergic mechanisms (Shu et al., 2022).
In conclusion, Lico-A alleviates AD by suppressing mast cell activation through inhibition of Th2 cytokines and the PLC/ERK/STAT3 signaling pathway, thereby reducing TNF-α and MCP-1 release. However, current clinical studies on Lico-A for AD are outdated, with a lack of recent trials. Moreover, existing mechanistic research remains limited, focusing primarily on its anti-inflammatory effects. Future studies should prioritize high-quality randomized controlled trial (RCT) and broader mechanistic investigations, including Lico-A’s effects on skin barrier function and neuroimmune interactions.
2.3 Rosacea and sensitive skin
Rosacea and sensitive skin are common chronic inflammatory dermatoses whose pathogenesis involves skin barrier dysfunction, neurovascular dysregulation, and immune-inflammatory responses (Geng et al., 2024; Sharma et al., 2022; Goh et al., 2023). In recent years, Lico-A has demonstrated unique therapeutic potential for these conditions due to its multi-target pharmacological activities.
Sulzberger et al. (2016); Kolbe et al. (2006) established post-shaving skin irritation models to evaluate the anti-irritant and skin-soothing effects of Lico-A-containing formulations. Their findings revealed that these formulations promoted erythema resolution and significantly reduced inflammatory responses within 24 h post-shaving, demonstrating notable skin-calming properties (Sulzberger et al., 2016; Kolbe et al., 2006). Schoelermann et al. (2016) conducted a clinical study in which skincare products containing Lico-A were applied to patients with mild-to-moderate rosacea. After 4 weeks, the treatment led to significant improvements in facial erythema, telangiectasia, roughness, and tightness, accompanied by reduced TEWL, increased skin hydration, and enhanced barrier function (Schoelermann et al., 2016). To further validate these observations, a large-scale study involving 1,221 patients with sensitive skin and rosacea was conducted to assess the efficacy and tolerability of Lico-A-containing cosmetics. Consistent with previous findings, the results confirmed not only clinical symptom relief but also excellent tolerability with no significant adverse effects (Jovanovic et al., 2017).
Mechanistic studies revealed that even at low concentrations (1.5 μM), Lico-A markedly suppresses TNF-α-induced NF-κB pathway activation and reduces the secretion of inflammatory mediators such as prostaglandin E2 (PGE2). This mechanism is particularly critical, as PGE2 not only directly participates in inflammatory responses but also sensitizes sensory neurons via TRPV1 channel activation, thereby inducing the release of TNF-α, interleukin-6, and vascular endothelial growth factor, which exacerbate vasodilation and non-neurogenic inflammation (Sulzberger et al., 2016). By disrupting this vicious cycle, Lico-A alleviates neurovascular hyperreactivity at its source.
In summary, Lico-A alleviates erythema and dryness in rosacea and sensitive skin by suppressing neurovascular inflammation through inhibition of the NF-κB pathway, thereby reducing PGE2 secretion. However, current clinical studies primarily evaluate Lico-A in combination formulations, with a lack of research on its efficacy as a standalone treatment. Additionally, mechanistic investigations remain limited. Future research should prioritize high-quality RCTs focusing on Lico-A monotherapy, along with further exploration of its mechanisms in neurovascular inflammation regulation.
2.4 Photodermatoses
Photodermatoses are a group of olar radiation-induced or exacerbated cutaneous disorders, including chronic actinic dermatitis, juvenile spring eruption, actinic prurigo and so on (Burfield et al., 2023). Ultraviolet radiation (UVR) and visible light (VIS) serve as primary etiological factors for these photosensitivity disorders (McDonald et al., 2023), inducing pathological consequences through DNA damage, oxidative stress, and inflammatory cascades (Tang et al., 2024). Lico-A has emerged as a promising candidate for photoprotection and photo-dermatoses management due to its dual anti-inflammatory and antioxidant properties.
Molecular studies have elucidated Lico-A’s mechanisms of action. Song et al. (2015) demonstrated that Lico-A specifically targets the AP-1 transcription factor, significantly suppressing UVR-induced COX-2 expression and PGE2 production. Importantly, this mechanism not only attenuates photoinflammatory responses but also disrupts the vicious cycle between inflammation and oxidative stress (Song et al., 2015). Mann et al. (2020) established a high-energy visible light-induced oxidative stress model, confirming that Lico-A’s photoprotective effects involve activation of the nuclear factor erythroid-2-related factor 2 (Nrf2) pathway. This activation mitigates ROS-mediated lipid peroxidation, DNA/protein damage, and prevents VIS-induced cutaneous carotenoid depletion (Mann et al., 2020). Kühnl et al. (2015) further elucidated the antioxidant mechanism of Lico-A, demonstrating its capacity to induce Nrf2 nuclear translocation and subsequent upregulation of critical antioxidant enzymes, including heme oxygenase-1 (HO-1) and glutamate-cysteine ligase (GCLM). Mechanistically, the catalytic products of HO-1 (biliverdin and carbon monoxide) exhibit synergistic antioxidant and anti-inflammatory properties, whereas GCLM maintains cellular redox homeostasis by regulating glutathione biosynthesis (Kühnl et al., 2015). These molecular mechanisms were clinically validated by Lim et al., 2022 demonstrating that Lico-A-containing formulations significantly reduce UVR/VIS-induced ROS generation while improving clinical manifestations including erythema and hyperpigmentation (Lim et al., 2022).
In conclusion, Lico-A exerts therapeutic effects on photodermatoses through dual modulation of Nrf2 activation and AP-1 suppression. However, current research has primarily focused on elucidating its molecular mechanisms, with limited clinical validation. Future studies should prioritize well-designed clinical trials to evaluate the therapeutic potential of Lico-A in photosensitive disorders, thereby providing an evidence-based foundation for its clinical application in photodermatoses.
3 Application of Lico-A in pigmented skin diseases
Excessive melanin production represents the central pathogenic mechanism in cutaneous pigmentation disorders. The microphthalmia-associated transcription factor (MITF) serves as the master regulator of melanogenesis, controlling expression of key enzymes including tyrosinase (TYR), tyrosinase-related protein 1 and tyrosinase-related protein 2. TYR is the key enzyme in melanin synthesis (Qu et al., 2023). And natural skin-lightening agents exert depigmenting effects through multiple pathways, including TYR inhibition, suppression of MAPK signaling, and interference with melanosome transport (Liu et al., 2024).
Hong et al. (2018) applied different concentrations (6.5–104 mg/mL) of Lico-A on melanoma cells B16 to evaluate the role of Lico-A in pigmentary diseases. The results showed that after 24 h, the amount of melanin in B16 cells was significantly reduced and the tyrosinase activity was significantly attenuated. Mechanistically, Lico-A activates ERK phosphorylation, leading to MITF downregulation and consequent tyrosinase inhibition (Hong et al., 2018). Studies indicate that Lico-A exerts its skin-whitening effects primarily through suppression of MITF expression rather than via direct inhibition of tyrosinase enzymatic activity, which is consistent with the findings reported by Jung et al. (2025). The depigmentation mechanism of Lico-A circumvents the pigmentary rebound effect associated with direct tyrosinase inhibition, thereby conferring therapeutic advantages for treating pigmentary disorders.
Wang et al. (2021) developed a Lico-A-loaded glycyrrhiza acid (GA + Lico-A) micelles with enhanced epidermal delivery and depigmentation efficacy, while systematically evaluating the depigmentation efficacy of GA + Lico-A micelles through both in vitro and in vivo experiments. The results demonstrated that GA + Lico-A micelles exhibited superior tyrosinase inhibitory effects and melanin-reducing capacity in B16 cells compared to Lico-A alone. Furthermore, animal studies demonstrated that 12-day consecutive topical application of both (GA + Lico-A) micelles and Lico-A significantly attenuated UVB-induced hyperpigmentation in murine models, within MAPK/ERK pathway distribution patterns correlating precisely with areas of decreased tyrosinase activity (Wang et al., 2025).
Further supporting evidence emerged from a comprehensive comparative analysis of flavonoid compounds conducted by Fu et al., 2005 which identified Lico-A as a particularly potent tyrosinase inhibitor among five tested flavonoids. Structure-activity relationship studies highlighted the critical importance of hydroxyl group positioning for optimal enzyme inhibition, providing molecular-level insights into Lico-A’s depigmentation mechanism (Fu et al., 2005).
While these preclinical studies establish Lico-A as a promising multi-target depigmenting agent through MITF downregulation and tyrosinase inhibition, clinical study remains limited (Figure 1). Further investigation is required to validate its efficacy, safety profile, and precise mechanisms of action in human pigmentation disorders.
4 Application of Lico-A in skin tumors
Cancer represents a group of malignant diseases that pose serious threats to human health and life. Its hallmark characteristics include rapid proliferation, invasion, and migration of abnormal cells (White et al., 2024). Lico-A has been shown to significantly inhibit proliferation and promote apoptosis in various cancer cell types. In dermatological oncology, Lico-A demonstrates particular therapeutic potential for oral squamous cell carcinoma (OSCC) and melanoma.
Lico-A exhibits distinct anti-OSCC mechanisms across different SCC models. In SCC-25 cells, Lico-A inhibits proliferation by inducing cell cycle arrest at S and G2/M phases. Conversely, in HN22 and HSC4 cell lines, Lico-A exerts its anticancer effects through suppression of specificity protein 1 (Sp1) and its downstream targets, including p27, p21, cyclin D1 and surviving (Cho et al., 2014). Further investigations by Hao et al. (2019) revealed that Lico-A exerts antiproliferative effects on SCC4 and CAL-27 OSCC cell lines through modulation of the PI3K/AKT signaling pathway. In vivo studies showed that Lico-A administration significantly reduced tumor burden in murine models of squamous cell carcinoma, concomitant with downregulation of metastasis-associated markers MMP-2 and MMP-9 (Hao et al., 2019). In a parallel study focusing on melanoma, Zhang et al. (2020) demonstrated that Lico-A enhances the expression of Ras homologous protein enriched in the brain by activating miR-142-3p, thereby activating the mTOR signaling pathway, inhibiting proliferation, reducing melanin production, and inducing apoptosis in A375 and B16 melanoma cells (Zhang et al., 2020).
In conclusion, Lico-A demonstrates multi-target anticancer potential in oral squamous cell carcinoma and melanoma through Sp1 suppression, PI3K/AKT pathway blockade, and mTOR pathway modulation (Figure 1). However, its mechanistic variability across models underscores the need for: (1) unified mechanistic studies, (2) advanced in vivo models, (3) early-phase clinical trials to evaluate human safety and efficacy.
5 Application of Lico-A in infections
Microbial infections represent a major etiological factor in dermatological pathologies (Hansen et al., 2022). Lico-A shows broad-spectrum antimicrobial activity against fungi, bacteria, and parasites via multi-target mechanisms.
5.1 Antifungal activity and mechanisms
Lico-A exhibits potent inhibitory activity against Microsporum canis (MIC = 4 μg/mL), with activity significantly superior to that of fluconazole compared to fluconazole (MIC = 64 μg/mL). Its multifaceted mechanism involves ergosterol biosynthesis inhibition-mediated membrane disruption, ATPase activity reduction impairing energy metabolism, and ROS-induced apoptotic oxidative stress. Transcriptomic analyses further reveal that Lico-A modulates critical pathways including cell wall biosynthesis, tricarboxylic acid cycle, and oxidative phosphorylation, resulting in comprehensive fungal growth suppression (Sun et al., 2025). Against Candida albicans and Aspergillus fumigatus, Lico-A inhibits biofilm formation, reduces host cell adhesion, and exerts direct killing effects through hyphal deformation and mitochondrial damage, while activating the host Nrf2/HO-1 pathway to mitigate inflammatory responses (Tian et al., 2024; Li et al., 2022).
5.2 Antibacterial and wound healing properties
Beyond its antifungal effects, Lico-A demonstrates substantial antibacterial activity against Escherichia coli and Staphylococcus aureus. When incorporated into chitosan-hyaluronic acid hydrogels, Lico-A maintains sustained-release properties and antimicrobial efficacy while accelerating wound healing through attenuation of inflammation, promotion of collagen synthesis, and stimulation of angiogenesis (Hou et al., 2024; Qu et al., 2023).
5.3 Antiparasitic efficacy
Lico-A displays potent activity against both promastigote and amastigote forms of Leishmania species. Experimental evidence demonstrates its capacity to significantly reduce infection rates in macrophages and U937 cells, while in vivo administration markedly decreases parasitic burden in hepatic and splenic tissues and prevents cutaneous lesion development in murine models (Chen et al., 1993).
In summary, Lico-A represents a promising antimicrobial agent with broad-spectrum antibacterial activity that exhibits significant antibacterial effects against fungal, bacterial, and parasitic pathogens through membrane disruption, bioenergetic interference, and immune regulation. Future investigations should focus on delivery system optimization to enhance bioavailability and targeting specificity, potentially positioning Lico-A as a next-generation antimicrobial for dermatological applications.
6 Discussion
Lico-A has demonstrated significant therapeutic potential across multiple dermatological conditions including acne vulgaris, AD, and rosacea, with mechanisms of action involving anti-inflammatory, antimicrobial, antioxidant, and antitumor. Clinical studies have confirmed its efficacy in reducing acne lesions, improving skin barrier function, and alleviating erythema, while exhibiting superior tolerability compared to conventional therapies such as corticosteroids and retinoids. These properties have positioned Lico-A as a compound of particular interest to dermatology specialists. However, several limitations persist in current research.
A critical issue is the geographical restriction of clinical evidence, with most studies conducted in Asian populations, raising questions about the generalizability of findings to other ethnic groups. The field also suffers from a paucity of high-quality randomized controlled trials, as existing clinical data primarily derive from small-scale, short-term studies with limited sample sizes. This gap is particularly evident in long-term safety assessments and relapse prevention studies. Furthermore, mechanistic understanding of Lico-A remains largely dependent on preclinical models including in vitro cell cultures and murine studies, which may not fully recapitulate the complexity of human skin pathophysiology. The therapeutic performance of Lico-A is additionally influenced by delivery system selection. While topical formulations such as creams and moisturizers minimize systemic side effects, their efficacy is constrained by poor skin penetration and short residence time. Microemulsion-based systems can enhance epidermal delivery efficiency but face challenges in stability and large-scale production. Hydrogels offer sustained antimicrobial release and wound healing benefits, though their high water content may compromise drug loading capacity.
To advance the clinical translation of Lico-A in dermatology, future investigations should prioritize global multicenter randomized controlled trials incorporating diverse patient populations, long-term follow-up, and rigorous methodological standards. Concurrent optimization of Lico-A formulations - including monotherapy trials and advanced delivery systems such as nanoparticles - is necessary to clarify its standalone therapeutic profile. A paradigm shift toward systems biology and network pharmacology approaches will be crucial to comprehensively elucidate Lico-A’s pleiotropic mechanisms and refine clinical applications. Given the multifactorial etiology of many dermatoses, integrating Lico-A into multimodal combination therapies shows particular promise. Such combinatorial strategies may not only amplify therapeutic outcomes but also mitigate resistance development, a persistent challenge in chronic dermatological management. Finally, clinical implementation must prioritize safety and efficacy evaluations across special populations, particularly vulnerable groups including pediatric and geriatric patients, where careful benefit-risk assessment remains essential.
In summary, realizing the full therapeutic potential of Lico-A in dermatology requires an integrated approach combining systems biology, advanced drug delivery technologies, and innovative combination therapies. Meanwhile, standardized regulatory frameworks and enhanced strategic industry partnerships should be pursued to facilitate commercialization, establishing a clear translational pathway from mechanistic insights to clinically viable therapies. By addressing current gaps, Lico-A may emerge as a cornerstone treatment for diverse dermatological conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angelova-Fischer I.Rippke F Fau - Richter D.Richter D Fau - Filbry A.Filbry A Fau - Arrowitz C.Arrowitz C Fau - Weber T.Weber T. F. A. U. (2018). Stand-alone emollient treatment reduces flares after discontinuation of topical steroid treatment in atopic dermatitis: a double-blind, randomized, vehicle-controlled, left-right comparison study. Acta Derm. Venereol. 98 (5), 517–523. 10.2340/00015555-2882 29335742 · doi ↗ · pubmed ↗
- 2Boonchai W.Varothai S.Winayanuwattikun W.Phaitoonvatanakij S.Chaweekulrat P.Kasemsarn P. (2018). Randomized investigator-blinded comparative study of moisturizer containing 4-t-butylcyclohexanol and licochalcone A versus 0.02% triamcinolone acetonide cream in facial dermatitis. J. Cosmet. Dermatol 17 (6), 1130–1135. 10.1111/jocd.12499 29411520 · doi ↗ · pubmed ↗
- 3Burfield L.Rutter K. J.Thompson B.Marjanovic E. J.Neale R. E.Rhodes L. A.-O. (2023). Systematic review of the prevalence and incidence of the photodermatoses with meta-analysis of the prevalence of polymorphic light eruption. J. Eur. Acad. Dermatol Venereol. 37 (3), 511–520. 10.1111/jdv.18772 36433668 · doi ↗ · pubmed ↗
- 4Chen M.Christensen Sb Fau - Blom J.Blom J Fau - Lemmich E.Lemmich E Fau - Nadelmann L.Nadelmann L Fau - Fich K.Fich K Fau - Theander T. G. (1993). Licochalcone A, a novel antiparasitic agent with potent activity against human pathogenic protozoan species of leishmania. Antimicrob. Agents Chemother. 37 (12), 2550–2556. 10.1128/AAC.37.12.2550 8109916 PMC 192736 · doi ↗ · pubmed ↗
- 5Cho J. J.Chae J. I.Yoon G.Kim K. H.Cho J. H.Cho S. S. (2014). Licochalcone A, a natural chalconoid isolated from Glycyrrhiza inflata root, induces apoptosis via Sp 1 and Sp 1 regulatory proteins in oral squamous cell carcinoma. Int. J. Oncol. 45 (2), 667–674. 10.3892/ijo.2014.2461 24858379 · doi ↗ · pubmed ↗
- 6Chularojanamontri L.Tuchinda P.Kulthanan K.Varothai S.Winayanuwattikun W. (2016). A double-blinded, randomized, vehicle-controlled study to access skin tolerability and efficacy of an anti-inflammatory moisturizer in treatment of acne with 0.1% adapalene gel. J. Dermatol. Treat. 27 (2), 140–145. 10.3109/09546634.2015.1079298 26293170 · doi ↗ · pubmed ↗
- 7Dall'oglio F.Fabbrocini G.Tedeschi A.Donnarumma M. A.-O.Chiodini P.Micali G. A.-O. (2019). Licochalcone A in combination with salicylic acid as fluid based and hydroxy-complex 10% cream for the treatment of mild acne: A multicenter prospective trial. Clin. Cosmet. Investig. Dermatol 12, 961–967. 10.2147/CCID.S 206935 32099436 PMC 6997230 · doi ↗ · pubmed ↗
- 8Flohr C. A.-O.Hay R. A.-O. (2021). Putting the burden of skin diseases on the global map. Br. J. Dermatol 184 (2), 189–190. 10.1111/bjd.19704 33544440 · doi ↗ · pubmed ↗