A duodenal tumor near the major duodenal papilla treated using a new thin therapeutic endoscope following pancreatic and biliary stenting
Hitoshi Mori, Koh Kitagawa, Satoshi Iwai, Yukihisa Fujinaga, Akira Mitoro, Hitoshi Yoshiji

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
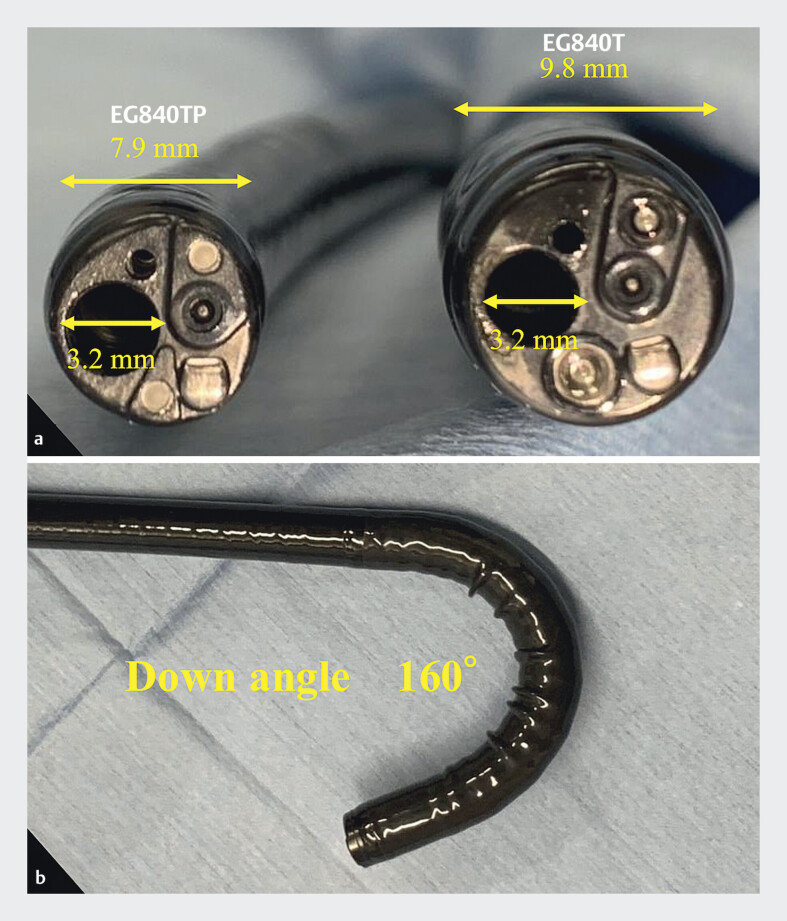 Fig. 1
Fig. 1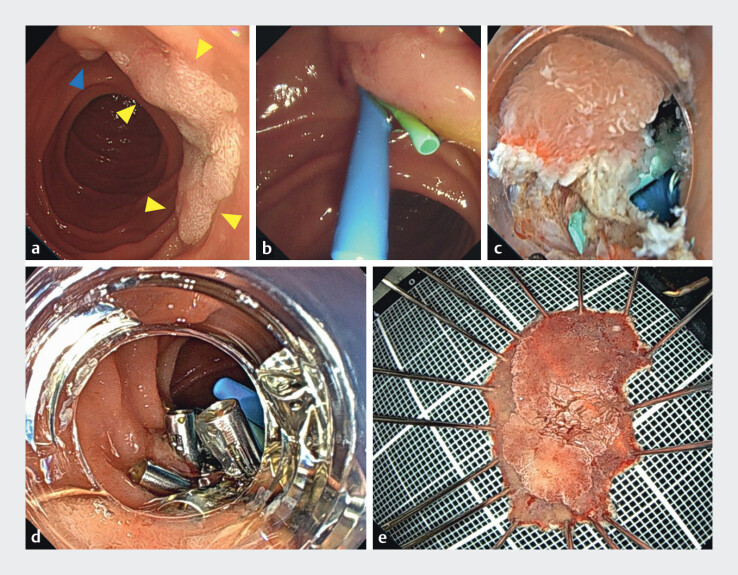 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Gastrointestinal Bleeding Diagnosis and Treatment · Gastrointestinal Tumor Research and Treatment
Duodenal endoscopic submucosal dissection (ESD) is technically challenging due to the complex anatomy of the duodenum 1 . In particular, when the lesion is close to the major duodenal papilla, the risk of pancreatitis and cholangitis increases. A recently introduced thin therapeutic endoscope (EG-840TP; Fujifilm, Tokyo, Japan) is reportedly useful for performing ESD in anatomically narrow spaces ( Fig. 1 ) 2 3 .
a Specifications of the thin therapeutic endoscope. It has an accessory channel with a diameter of 3.2 mm and an outer diameter of only 7.9 mm. b The thin therapeutic endoscope allows an extended downward angulation of up to 160°.
Herein, we report a case of duodenal ESD performed with a novel thin endoscope following pancreatic and biliary stenting. A 77-year-old woman was diagnosed with a 20-mm in diameter duodenal tumor located near the major duodenal papilla and was referred to our hospital for endoscopic treatment ( Fig. 2 a ). First, pancreatic stenting and biliary stenting were performed to minimize the risk of thermal damage to the orifice of the major duodenal papilla ( Fig. 2 b ). Subsequently, ESD was performed using the thin therapeutic endoscope ( Fig. 2 c ). To prevent cholangitis and pancreatitis after ESD caused by air insufflation, the water exchange method was used. The lesion was completely resected using ESD, and the mucosal defect was closed using the reopenable-clip over-the-line method ( Fig. 2 d, e , Video 1 ) 4 . On the day following the procedure, the patient developed mild acute pancreatitis, which quickly resolved with conservative treatment. The pancreatic duct stent was endoscopically removed on postoperative day 7, and the patient was discharged 8 days after the duodenal ESD. The final pathological diagnosis was high-grade adenoma with negative margins. Two months later, the biliary stent had passed spontaneously. This new thin therapeutic endoscope has a 3.2-mm accessory channel, a waterjet function, and an extended down angle of up to 160°. Therefore, it is useful for treating lesions near the major duodenal papilla, even when pancreatic stenting and biliary stenting are in place.
a Endoscopic view of the lesion. A Paris IIa 20 mm in diameter non-ampullary duodenal adenoma (yellow arrowheads) located near the major papilla (blue arrowhead). Endoscopic findings suggested the possibility of an adenoma. b Endoscopic retrograde cholangiopancreatography was performed. Pancreatic and biliary plastic stents were placed before endoscopic submucosal dissection to prevent thermal injury to the orifice of the major duodenal papilla. c Endoscopic submucosal dissection was performed using a thin therapeutic endoscope fitted with a small-caliber transparent tip hood (DH-083ST; Fujifilm). d Mucosal defect closure using the reopenable-clip over the line method. e Resected specimen.
A duodenal tumor near the major duodenal papilla treated using a new thin therapeutic endoscope following pancreatic and biliary stenting.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yahagi N Kato M Ochiai Y Outcomes of endoscopic resection for superficial duodenal epithelial neoplasia Gastrointest Endosc 20188867668210.1016/j.gie.2018.05.00229753040 · doi ↗ · pubmed ↗
- 2Miura Y Fukuda H Ueno T Endoscopic submucosal dissection of gastric neoplasms with severe fibrosis using a new thin-therapeutic endoscope and a dedicated conical cap Endoscopy 202355 E 872E 87337442164 10.1055/a-2106-0688 PMC 10344623 · doi ↗ · pubmed ↗
- 3Hashimoto K Fukuda H Fujinuma T Combination of the saline-immersion technique and a new thin therapeutic endoscope for endoscopic submucosal dissection of a duodenal subepithelial tumor Endoscopy 202557 E 3E 410.1055/a-2497-238639809287 PMC 11732377 · doi ↗ · pubmed ↗
- 4Nomura T Sugimoto S Tsuda N Mucosal defect closure after duodenal endoscopic submucosal dissection using the reopenable-clip over the line method JGH Open 2021583183310.1002/jgh 3.1257734263081 PMC 8264231 · doi ↗ · pubmed ↗