The Prevalence Rates of Colistin Resistance Among Third-Generation Cephalosporin-Resistant E. coli Isolates From Thai Patients
Siriporn Kowaboot, Nipaporn Tewawong, Apichai Sreepian, Preeyaporn M. Sreepian, Utsanee Supcharoengoon, Aunchalee Tonsomboon, Naiyana Watanagul, Pannamthip Pitaksajjakul

TL;DR
This study found a low but notable rate of colistin resistance among E. coli isolates from Thai patients, with specific resistance genes identified.
Contribution
The study reports the prevalence of colistin resistance and identifies specific mcr genes in E. coli isolates from Thailand.
Findings
1.45% of third-generation cephalosporin-resistant E. coli isolates showed colistin resistance.
Five isolates carried mcr-1 or mcr-3 resistance genes, with one carrying both.
The findings highlight the importance of monitoring resistance genes in public health.
Abstract
Drug-resistant infections, such as colistin resistance, are reportedly increasing due to the inappropriate use of antibiotics, lack of good control, and the use of excessive quantities of antibiotics. Colistin resistance has been observed in bacteria of the order Enterobacterales exhibiting resistance to third-generation cephalosporins or carbapenems. Currently, the prevalence of colistin resistance in third-generation cephalosporin-resistant E. coli obtained from patients at Nopparat Rajathanee Hospital, Thailand, in 2023 was determined by broth microdilution. Among 343 isolates, 1.45% (95% CI: 0.19%–2.73%, n = 5/343) exhibited a minimum inhibitory concentration (MIC) of colistin between 4 and 8 μg/mL, indicating colistin-resistant E. coli. Nevertheless, five isolates were positive for resistant genes by multiplex PCR: two isolates for mcr-1, two isolates for mcr-3, and one isolate for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
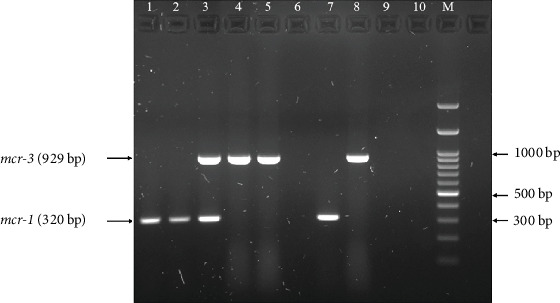 Figure 1
Figure 1- —Rangsit University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Escherichia coli research studies · Urinary Tract Infections Management
1. Introduction
Globally, the escalating number of infections arising from antimicrobial-resistant organisms presents a major public health challenge. One primary driver of this trend is the misuse and overuse of antimicrobial agents, often due to poor infection control and the unnecessary prescription of antimicrobial drugs. These factors have accelerated the spread of resistance, limiting the effectiveness of available treatments and allowing resistant bacteria to persist in the environment. In Thailand, antimicrobials are commonly applied in healthcare settings, agriculture, and animal production systems. Gram-negative bacteria, especially members of the Enterobacterales order, such as Escherichia coli (E. coli), are frequently responsible for hospital-acquired infections. These organisms frequently demonstrate resistance to broad-spectrum antibiotics, encompassing β-lactams, aminoglycosides, fluoroquinolones, and carbapenems. The rise of multidrug-resistant strains has led to colistin's reintroduction as a treatment option [1].
Colistin (Polymyxin E) is a potent antibiotic that is effective against gram-negative bacteria, including Enterobacterales and nonfermentative species [2]. The bactericidal effect of colistin, a polymyxin, involves binding to the lipopolysaccharide of gram-negative bacteria. The interaction of the positively charged polypeptide of colistin with the membrane compromises its integrity, ultimately causing cell lysis. As the use of colistin has increased, the occurrence of colistin resistance among gram-negative bacteria has also increased globally, with resistance rates steadily increasing [3].
In 2015, the discovery of the mcr-1 gene, representing the first known instance of a plasmid-mediated colistin resistance gene in colistin-resistant E. coli, which was isolated from Chinese pig meat, marked a significant advancement [4]. Since this initial discovery, a series of related gene variants, designated mcr-1 through mcr-10, have been identified on plasmids in colistin-resistant Enterobacterales strains [5–10]. Among the mcr genes, mcr-1 is the most frequently observed, especially in environments related to farm animals and in patients with Enterobacterales infections [11]. In Thailand, the initial identification of mcr-1 occurred in E. coli isolates exhibiting resistance to colistin. In addition, all of them also presented resistance to third-generation cephalosporins [12]. Recently, the mcr-3 gene has been increasingly identified in E. coli strains derived from human clinical samples [13]. Therefore, the objective of this study was to ascertain the prevalence of both mcr-1 and mcr-3 genes exhibiting colistin resistance in third-generation cephalosporin-resistant E. coli isolated from patient samples in Thailand between March and September 2023. The findings of this study will provide the essential data to elucidate the prevalence of resistance genes, thereby enabling the surveillance of antibiotic resistance patterns, guiding therapeutic strategies, and supporting the development of effective public health measures to control the dissemination of antibiotic-resistant bacteria.
2. Materials and Methods
2.1. Sample Collection and Identification
Previous microbiological analyses resulted in the successful isolation and identification of 343 E. coli via matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) at Nopparat Rajathanee Hospital, Thailand. The isolates were obtained from patients from March to September 2023. The confirmation of all isolates as E. coli was performed by 16S rRNA PCR amplification [14].
2.2. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing of E. coli was done by the Sensititre ARIS 2X (Thermo Fisher Scientific, United Kingdom) as part of routine microbiology, according to the guidelines of Clinical and Laboratory Standards Institute (CLSI) [15]. The antibiotics evaluated in this study were ampicillin (AMP), amoxicillin–clavulanate (AMC), cefoxitin (FOX), cefotaxime (CTX), ceftriaxone (CRO), ceftazidime (CAZ), imipenem (IMP), meropenem (MEM), ertapenem (ETP), gentamicin (CN), amikacin (AK), netilmicin (NET), ciprofloxacin (CIP), levofloxacin (LEV), and trimethoprim/sulfamethoxazole (SXT). Colistin resistance was manually determined by broth microdilution. Colistin dilutions ranging from 0.25 to 128 μg/mL were prepared in cation-adjusted Mueller–Hinton Broth (Oxoid, United Kingdom). The results were subsequently analyzed in accordance with the guidelines of the European Committee on Antimicrobial Susceptibility Testing [16]. The isolates exhibiting MICs of 4 μg/mL or greater were categorized as colistin-resistant E. coli. This study used E. coli ATCC 25922 as a reference strain for drug susceptibility testing. Tests were repeated independently three times. Multidrug resistance (MDR) was defined as nonsusceptibility to at least one agent in three or more antimicrobial categories [17].
2.3. Detection of Colistin Resistance Genes via Multiplex PCR
In this study, the boiling method was used to extract the genomic DNA of E. coli for the PCR assay [18]. The concentrations of DNA were measured using Nano-400A (Allsheng, Hangzhou, China). The colistin resistance genes, including mcr-1 and mcr-3, were identified through multiplex PCR. A 25 μL of PCR reaction mixture was prepared, including 0.4 μM of each primer (Table 1), 100 ng DNA template, and 1× AccuStart II Geltrack PCR Supermix (Quantabio, Beverly, Massachusetts, United States). The amplification steps were conducted as previously described [19]. Briefly, the thermal cycling started with an initial denaturation (94°C for 3 min), followed by 25 cycles (denaturation: 94°C, 30 s; annealing: 58°C, 90 s; and extension: 72°C, 60 s), and a final extension (72°C, 5 min). The visualization of the PCR products was performed using GelDoc Go after separation by 1.5% agarose gel electrophoresis. Control strain of E. coli ATCC25922 was used as a negative control.
2.4. Nucleotide Sequence Accession Numbers
The 16S rRNA nucleotide sequences of E. coli and colistin resistance genes, mcr-1and mcr-3, are accessible via GenBank accession numbers PV453565, PV449191, and PV469330, respectively.
2.5. Data Analysis
The descriptive analysis of the categorical variables, along with their 95% confidence intervals (CIs), was determined using SPSS Version 21.0 (IBM, United States).
2.6. Ethical Approval
The current study was approved by the Ethics Review Board of Rangsit University, under the approval number designated as RSUERB 2022/070.
3. Results
3.1. Isolation and Characterization of E. coli
The demographics and characteristics of the patients infected with E. coli admitted to Nopparat Rajathanee Hospital between March and September 2023 are displayed in Table 2. The sample population comprised 54.8% (188/343) females and 45.2% (155/343) males. The age group of 25–60 years represented almost the entire population (87.8%; 301/343). Nearly half of the collected samples were catheterized urine (46.4%; 159/343), followed by blood (16.0%; 55/343) and sputum (13.1%; 45/343). The 16S rRNA gene analysis by PCR amplification confirmed that all 343 isolates were E. coli.
3.2. Antimicrobial Susceptibility Test
Table 3 presents a comprehensive overview of the resistance percentages observed in the antibiotics tested in this study. The results indicated that all bacterial isolates (343 isolates) in this study were resistant to AMP and three cephalosporin antibiotics, including cefazolin (1st gen), CTX (3rd gen), and CRO (3rd gen). The percentage of bacterial resistance to CIP, LEV, SXT, CAZ, and CN was 78.1%, 75.2%, 63.3%, 44.0%, and 41.1%, respectively. Interestingly, among 343 isolates, colistin resistance was detected in five (1.5%) isolates via the broth microdilution method, with MICs ranging from 4 to 8 μg/mL.
3.3. Molecular Identification of mcr
In this study, a multiplex PCR analysis was conducted on 343 isolates of E. coli exhibiting cephalosporin resistance to identify mcr-1 and mcr-3 genes. The results demonstrated that the mcr genes were detected in 1.45% (95% CI: 0.19%–2.73%, n = 5/343). In addition, the mcr genes were detected in 100% (5/5) of the isolates, which demonstrated colistin resistance (Figure 1). The information regarding E. coli isolates that show positive results for mcr-1 and mcr-3 is shown in Table 4. The positive isolates were collected from various departments. It was observed that most isolates were derived from patients older than 60 years, except for Isolate Number 176. According to the EUCAST guidelines, all mcr gene–positive isolates exhibited colistin MIC values ≥4 μg/mL, which is indicative of colistin resistance. Isolate Numbers 22 and 162 were positive for mcr-1 from March to May, whereas Isolate Numbers 177 and 182 were positive for mcr-3 from August to September. Notably, Isolate Number 176 was positive for both mcr-1 and mcr-3 in August. The mcr genes were undetectable in E. coli isolates with colistin MIC lower than 2 μg/mL.
Following identification as mcr-positive, the five bacterial strains were assessed for antibacterial susceptibility to various antibiotics. Among these five strains, three strains exhibited MDR, while the remaining two strains demonstrated MDR in addition to carbapenem resistance. All five isolates were resistant to antimicrobial classes with different patterns (Table 5).
4. Discussion
Colistin may be reserved as a final treatment option for E. coli infections that have developed resistance to multiple antibiotics, including those in the third-generation cephalosporins, which are among the commonly used antibiotics. The rise of third-generation cephalosporin-resistant E. coli infection has directly contributed to the faster emergence of colistin resistance. The bacteria used in this study were E. coli strains that exhibited resistance to third-generation cephalosporins. Our observations revealed a high resistance rate among E. coli to fluoroquinolones, ranging from 75% to 78%, which is higher than that reported previously [20–22]. One to two-thirds of Enterobacteriaceae that produce extended-spectrum β-lactamases are resistant to fluoroquinolone [23]. Fluoroquinolone-resistant E. coli isolated from a UTI patient in Thailand revealed that the presence of the PMQR gene is related to ESBL strains [24]. Nevertheless, our study revealed that 55 E. coli isolates were susceptible to fluoroquinolones (CIP and LEV).
This study revealed a low prevalence of E. coli isolates exhibiting resistance to colistin, with 1.46%. A similar result has been reported in previous studies [25–28]. In addition, in our study, the prevalence rate of E. coli exhibiting colistin resistance was lower than that reported by Boonyasiri et al. in 2023 in Thailand, who found that the prevalence rates of colistin-resistant E. coli in patients, healthy farmers, and pigs were 12.1%, 10.2%, and 68.4%, respectively [13].
In this study, plasmids encoding mcr-1, mcr-3, or a combination of the two genes were identified in E. coli with existing colistin resistance. Two isolates carried a single mcr-1 gene, two carried a single mcr-3 gene, and one carried both genes. Several previous studies have indicated that mcr-1 is more common than other mcr genes [26, 29–31]. Furthermore, a significant finding from recent research indicates that the mcr-3 gene was detected at a high rate (54%) within colistin-resistant E. coli samples obtained from various pig farms in Thailand [19]. The prevalence of the mcr-1 gene reported by Boonyasiri et al. [13] was 52.9% in colistin-resistant E. coli isolated from porcine fecal samples and 87.5% in those from human fecal samples.
In contrast, the mcr-3 gene was found in 37.5% of human fecal isolates and up to 96.1% of pig fecal isolates. These findings reveal that mcr-1 is more commonly found in E. coli from human fecal samples than in those from porcine fecal samples, whereas mcr-3 is more common in isolates from porcine fecal samples than in those from human feces. A 2017 study on antibiotic usage revealed that small to medium-sized pig farms in the northeastern region of Thailand were increasingly using amoxicillin and colistin [32]. Colistin is currently banned as a feed additive in Thailand. Nevertheless, the prolonged and cumulative selective pressure from its prior use may have contributed to the development of bacterial resistance to the drug. This effect may explain the occurrence of colistin-resistant E. coli carrying the mcr-3 gene, suggesting the possibility of transmission from animals to humans. The discovery of the mcr-3 gene underscores the potential for the development of colistin resistance within the healthcare settings in Thailand. In addition, the co-occurrence of two mcr plasmids has rarely been reported. However, we found one isolate that carried both mcr-1 and mcr-3. The co-occurrence of the mcr-1 and mcr-3 genes within a single isolate of E. coli from human patients has also recently been reported in China and New Zealand [33, 34].
Our study revealed that E. coli strains displaying either mcr-1 or mcr-3 presented a moderate level of colistin resistance, with MICs ranging from 4 to 8 μg/mL. This finding aligns with those of previous studies conducted in China and Nepal [35, 36]. These results suggest that the simultaneous presence of mcr-1 and mcr-3 does not increase colistin resistance. One notable difference between the mcr-1 and mcr-3 genes is that mcr-3 has greater heat stability. This fact could explain why, even if the mcr-1 gene is destroyed, resistance is not eliminated, as the resistance phenotype is maintained through the properties of the *mcr-*3 gene [37]. Our study has several limitations. The current study was limited to mcr-1 and mcr-3. According to other research, mcr-1 was mostly carried by conserved epidemic plasmids, while mcr-3 was located on a more diverse set of plasmid types [38]. However, isolation and characterization of mcr-2 and mcr-4 to mcr-10 are suggested in future studies to predict the role of genes in conferring resistance. Our analysis revealed no association between infections caused by mcr-1- or mcr-3-carrying E. coli and the infection site, time period, or specific wards. However, multilocus sequence typing (MLST) or whole-genome sequencing (WGS) would provide a higher level of resolution for species confirmation and for understanding the evolution of these mcr-carrying E. coli within the hospital. As the present study was conducted in a single hospital, the reported rates correspond to a limited geographical area and may not be directly extrapolated.
5. Conclusion
A global distribution of the mcr gene has been observed, with surveillance efforts encompassing E. coli from human, animal, and environmental samples. The occurrence of colistin resistance and the presence of the mcr gene in clinical isolates from our study represent a considerable public health concern in hospitals. Therefore, the prompt implementation of antibiotic stewardship programs is essential for controlling infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li J. Nation R. L. Turnidge J. D. Colistin: The Re-Emerging Antibiotic for Multidrug-Resistant Gram-Negative Bacterial Infections Lancet Infectious Diseases 20066958960110.1016/S 1473-3099(06)70580-12-s 2.0-3374736287016931410 · doi ↗ · pubmed ↗
- 2Tan T. Y. Ng S. Y. The In-Vitro Activity of Colistin in Gram-Negative Bacteria Singapore Medical Journal 200647762162416810437 · pubmed ↗
- 3Gales A. C. Jones R. N. Sader H. S. Contemporary Activity of Colistin and Polymyxin B Against a Worldwide Collection of Gram-Negative Pathogens: Results From the SENTRY Antimicrobial Surveillance Program (2006-09) The Journal of Antimicrobial Chemotherapy 20116692070207410.1093/jac/dkr 2392-s 2.0-8005170136621715434 · doi ↗ · pubmed ↗
- 4Liu Y. Y. Wang Y. Walsh T. R. Emergence of Plasmid-Mediated Colistin Resistance Mechanism MCR-1 in Animals and Human Beings in China: A Microbiological and Molecular Biological Study Lancet Infectious Diseases 201616216116810.1016/S 1473-3099(15)00424-72-s 2.0-8495743350826603172 · doi ↗ · pubmed ↗
- 5Xavier B. B. Lammens C. Ruhal R. Identification of a Novel Plasmid-Mediated Colistin-Resistance Gene, mcr-2, in Escherichia coli, Belgium, June 2016 Eurosurveillance: European communicable disease bulletin/European Communities. Commission; Communautés européennes. Commission.-Saint-Maurice, 1995, currens 201621273028010.2807/1560-7917.ES.2016.21.28.302822-s 2.0-8502031614827416987 · doi ↗ · pubmed ↗
- 6Duggett N. A. Randall L. P. Horton R. A. Molecular Epidemiology of Isolates With Multiple mcr Plasmids From a Pig Farm in Great Britain: The Effects of Colistin Withdrawal in the Short and Long Term Journal of Antimicrobial Chemotherapy 201873113025303310.1093/jac/dky 2922-s 2.0-8504976933630124905 · doi ↗ · pubmed ↗
- 7Abu Oun M. Stubberfield E. J. Duggett N. A. mcr-1 and mcr-2 (mcr-6.1) variant genes identified in Moraxella species isolated from pigs in Great Britain from 2014 to 2015 Journal of Antimicrobial Chemotherapy 201772102745274910.1093/jac/dkx 2862-s 2.0-8503065856129091227 PMC 5890717 · doi ↗ · pubmed ↗
- 8Yang Y. Q. Li Y. X. Lei C. W. Zhang A. Y. Wang H. N. Novel Plasmid-Mediated Colistin Resistance Gene mcr-7.1 in Klebsiella pneumoniae Journal of Antimicrobial Chemotherapy 20187371791179510.1093/jac/dky 1112-s 2.0-8504785002029912417 · doi ↗ · pubmed ↗