Female donor gender is associated with a decrease in liver transplant survival of male recipients independent of donor and recipient anthropometrics
Marcio Fernandes CHEDID, Lucas PREDIGER, Gabriel LAZZAROTTO-DA-SILVA, Jane CRONST, Alexandre DE ARAUJO, Tomaz de Jesus Maria GREZZANA, Luciano Zubaran GOLDANI

TL;DR
Male liver transplant recipients who receive livers from female donors have worse survival rates, even when body size differences are not a factor.
Contribution
This study identifies female donor gender as a novel independent predictor of increased mortality in liver transplant recipients, particularly in males.
Findings
Female donor gender was the only significant predictor of increased mortality after liver transplant [HR 1.918, 95%CI 1.150–3.201, p=0.013].
Male recipients of livers from female donors had higher mortality rates, with infection being the most common cause in the first year.
Anthropometric differences between donor and recipient were not related to mortality outcomes.
Abstract
Data on the influence of donor gender on post-liver transplant outcomes is scarce and is lacking. The aim of this study was to evaluate the prognostic factors of mortality in patients undergoing liver transplantation (LT) with a thorough evaluation of the influence of the donor variables. All patients undergoing LT at a single center from December 2011 to December 2018 were included. The main outcome measure of the study was overall patient survival. The mortality predictors were evaluated using Cox regression. The study analyzed 202 patients, 118 (58.1%) being males, and the average age was 54.19±11.66 years. Post-LT survival for the entire cohort of 202 patients as assessed by the KaplanMeier method at 1, 3, 5, and 7 years was 81.6, 73.1, 67.6, and 63%, respectively. The only predictor of increased overall mortality was female donor gender [HR 1.918, 95%CI 1.150–3.201, p=0.013].…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
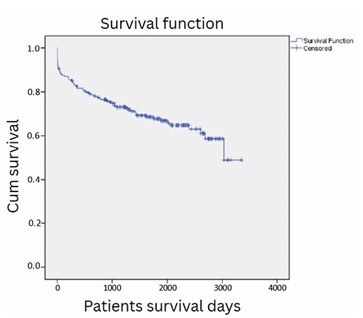 Figure 1
Figure 1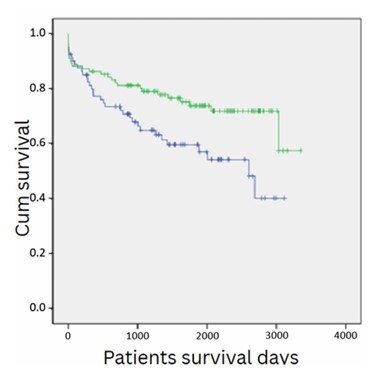 Figure 2
Figure 2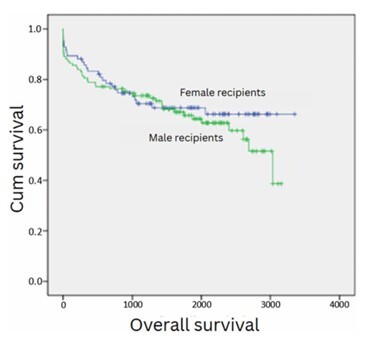 Figure 3
Figure 3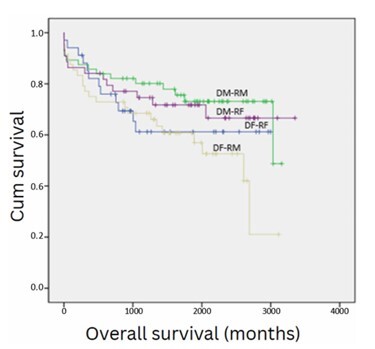 Figure 4
Figure 4| n (%) | Mean±DP | Median+IQR | |
|---|---|---|---|
| Age | 54.19±11.66 | 57 (IQR 49.75–62) | |
| Male gender | n=118 (58.4%) | ||
| Body mass index | 27.76±5.457 | 27 (IQR 24–31) | |
| MELD score | 16±9 | 13 (IQR 10–19) | |
| MELD-Na score | 16±8 | 13 (IQR 10–19) | |
| HCV infection | n=125 (61.9%) | ||
| Hepatocellular carcinoma | n=115 (56.9%) | ||
| Albumin | 3.18±0.73 | 3 (IQR 3–3.5) | |
| Bilirubin | 4.51±8.4 | 1,70 (IQR 0.9–3.22) | |
| INR | 1. 77±1,58 | 1,37 (IQR 1.21–1.68) | |
| Sodium | 139.66±4.13 | ||
| Creatinine | 1.04±0.84 | 0,8 (IQR 0.66–1.07) | |
| Diabetes | n=86 (28.3%) |
| Hazard ratio [95%CI] | p-value | |
|---|---|---|
| Age | 0.996 [0.976–1.016] | 0.677 |
| Female gender | 0.830 [0.511–1.348] | 0.451 |
| Receptor height | 1.002 [0.978–1.026] | 0.884 |
| Receptor weight | 1.006 [0.990–1.023] | 0.468 |
| Body mass index | 1.026 [0.973–1.080] | 0.342 |
| Diabetes | 1.367 [0.836–2.237] | 0.213 |
| MELD score | 1.003 [0.977–1.031] | 0.811 |
| MELD-Na score | 1.003 [0.977–1.030] | 0.840 |
| HCV infection | 0.912 [0.563–1.477] | 0.708 |
| Hepatocellular carcinoma | 1.003 [0.623–1.614] | 0.991 |
| Total bilirubin | 1.011 [0.986–1.037] | 0.389 |
| INR | 0.886 [0.702–1.118] | 0.309 |
| Sodium | 1.008 [0.951–1.068] | 0.788 |
| Creatinine | 0.828 [0.573–1.196] | 0.314 |
| Platelets | 1.022 [0.960–1.088] | 0.501 |
| Albumin | 0.749 [0.546–1.027] | 0.072 |
| Albumin-bilirubin grade (ALBI) 2 — categories | 1.155 [0.668–1.995] | 0.606 |
| Pre-transplant dialisis | 1.124 [0.486–2.598] | 0.785 |
| Infection prior to LT | 1.301 [0.744–2.275] | 0.355 |
| Ascites prior to LT | 1.405 [0.876–2.253] | 0.158 |
| Donor infection | 0.956 [0.550–1.644] | 0.875 |
| Donor age | 1.011 [0.996–1.027] | 0.154 |
| Donor gender, female | 1.806 [1.091–2.988] | 0.021 |
| Donor BMI | 0.988 [0.914–1.069] | 0.771 |
| Donor height | 0.696 [0.037–13.192] | 0.809 |
| Donor weight | 0.996 [0.976–1.016] | 0.669 |
| Height difference between donor and recipient | 1.000 [0.980–1.021] | 0.964 |
| Weight difference between donor and recipient | 0.996 [0.982–1.010] | 0.545 |
| Infection, receptor during transplant hospitalization | 0.793 [0.468–1.345] | 0.390 |
| Infection during first 90 post-transplant days | 0.646 [0.403–1.035] | 0.069 |
| Infection during first year | 0.689 [0.430–1.104] | 0.121 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Liver Disease and Transplantation · Organ Donation and Transplantation
INTRODUCTION
Post-liver transplant survival has achieved little improvement over the last decade^ 22 ^. Several prognostic factors of mortality after LT have been identified, including donor age, long cold ischemia time, long warm ischemia time, moderate hepatic steatosis in the donor, and others^ 1,6,7,9,10 ^.
Data on the influence of donor gender on post-liver trans plant outcomes is scarce. The objective of this study was to iden tify the prognostic factors of mortality in patients undergoing LT.
METHODS
All adult patients who underwent a first LT at the authors’ institution from December 2011 to December 2018 were included. Pediatric patients (under 18 years of age), partial graft recipients (split livers and partial grafts from living donors), and patients with concurrent transplants (combined liver and kidney transplant) were not included in this analysis.
This study was approved by the Institution Ethics Committee (number 2017-0271). The study researchers signed a confidentiality agreement regarding the use of the collected data. Informed consent was obtained from all patients who were alive by the time of the study start.
All transplants were performed using the "piggyback" technique. Generally, the threshold for performing blood autotransfusion using blood collected by the intraoperative blood recovery device for autotransfusion was 1,000 mL of bleeding (or hemodynamic instability occurrence related to hypovolemia)^ 21 ^. Fresh frozen plasma, cryoprecipitate, and platelets were administered as needed according to thromboelastographic evaluation.
Abdominal Doppler ultrasound was performed routinely to screen for hepatic vascular complications^ 5,11 ^. Oral feeding was started in the intensive care unit shortly after extubation. Immunosuppression was based on the use of tacrolimus, mycophenolate, and steroids.
The study’s primary endpoint was overall post-LT patient survival. The patients were followed until their death or until the end of the study period. Post-LT infectious episodes also were studied and characterized. There were no follow-up losses during the study period.
The following variables collected in the immediate pretransplant period were analyzed: recipient age, gender, ethnicity/race, height, weight, body mass index (BMI), presence of diabetes mellitus (DM), MELD (model for end-stage liver disease) score, hepatitis C virus (HCV) infection, presence of hepatocellular carcinoma (HCC), infection prior to LT, ascites prior to LT, dialysis prior to LT, total bilirubin (TB), international normalized prothrombin time ratio (INR), albumin, sodium, creatinine, platelets, albumin-bilirubin score (ALBI)^ 2 ^, donor gender, donor age, donor weight, donor height, recipient weight, and recipient height. Data from laboratory tests were collected up to 15 days before LT. Demographic and laboratory data of the donors were also collected and analyzed.
For the identification of the prognostic factors related to each of mortality, univariate analysis was performed using the Cox regression method using the variables described above. Variables whose p-value was <0.05 in each of the univariate analyses for the outcomes were included in multivariable Cox regressions respective to each outcome. For all analyses, p-values<0.05 were considered statistically significant. Analyses were performed using SPSS V.18 software (IBM Corporation, Armonk, New York, U.S.).
RESULTS
A total of 202 patients who underwent a first LT were included (Table 1), of which 118 (58.4%) were male, and the remaining 84 patients (41.6%) were female. The mean age was 54.19±11.66. The predominant ethnicity was Caucasian (94.7% of patients). Notably, 86 patients (28.6%) had diabetes mellitus. The main cause of end-stage liver disease was HCV infection, accounting for 125 cases (61.9%). Additionally, HCC in the setting of cirrhosis occurred in 115 patients (56.9%), being the main indication of LT in this cohort. The calculated median MELD score was 13 (interquartile range — IQR=10–19).
Post-LT survival for the entire cohort of 202 patients as assessed by the Kaplan-Meier method at 1, 3, 5, and 7 years was 81.6, 73.1, 67.6, and 63%, respectively (Figure 1). There were 18 deaths during the first 30 days post-LT days (30-day mortality of 8.9%). Between the 31st and 180th days, there were 7 deaths. Between the 181st and 365th day post-LT, 13 other deaths occurred. Overall, a total of 38 deaths occurred during the first post-LT year for the 202 transplant patients, resulting in a 1-year actual survival of 81.1%.
Survival analysis of 202 consecutive patients who underwent liver transplantation at a single center.
During the first 30 post-LT days, the main cause of death was graft dysfunction (n=12) (either primary or secondary to vascular thrombosis or large-for-size grafts). Among the patients who died during the first 30 post-LT days, 3 suffered from hepatic artery thrombose, 2 from portal vein thrombose, and 4 from hemorrhagic shock. There were three abdominal compartment syndromes caused by large-for-size liver grafts. During this period, 5 of the 18 deaths (27.78%) were due to infections.
From the 31st to 180th day post-LT, the main cause of death was infection (six of the seven deaths were caused by infection). Between days 181 and 365 post-LT, infection was also the main cause of death (8 of the 13 deaths in this period were caused by infection).
Table 2 presents the results of univariate analysis by Cox regression with the outcome of mortality occurring throughout the study follow-up. According to this analysis, female donor gender (HR 1.806, 95%CI 1.091–2.988; p=0.021, p<0.05) was the only predictor of overall post-LT mortality.
Anthropometric parameters of donor and recipient also were studied. The difference between donor and recipient weight was not related to a decreased post-LT survival (p=0.545, p>0.05). Likewise, the difference between donor and recipient height was not related to a decreased post-LT survival (p=0.964, p>0.05).
Figure 2 shows the analysis of post-transplant survival using the Kaplan-Meier method, stratified by donor gender. Post-LT survival for patients who received a liver graft from a male donor was 86.3, 79.1, 73.8 and 71.8% at 1, 3, 5, and 7 years, respectively, versus 77.4, 64.9, 59.6, and 54.2% for patients who received a liver from a female donor (p=0.013, p<0.05).
Survival analysis of 202 consecutive patients who underwent liver transplantation at a single center, stratifying by donor gender, depicting a lower survival for patients who received a liver graft from a female donor (p=0.013).
Figure 3 depicts the analysis of post-transplant survival stratified by recipient gender. Post-LT survival for male recipients was not different from that of female recipients (p=0.45, p>0.05).
Survival analysis of 202 consecutive patients who underwent liver transplantation at a single center, stratifying by recipient gender, depicting a similar survival (p=0.45).
Figure 4 shows recipient survival stratified in four groups by donor and recipient gender. The highest survival occurred for male patients receiving a liver from a male donor (1 year=85.7%, 3 years=80.1%, 5 years=73.1%, and 7 years=73.1%), whereas the lowest survival occurred for male patients receiving a liver graft from female donors (1 year=75%, 3 years=68.5%, 5 years=60.8%, and 7 years=52.6%) (p=0.028, p<0.05).
Survival analysis of 202 consecutive patients who underwent liver transplantation at a single center, stratifying in four groups by donor and recipient gender.DM: donor male; DF: donor female; RM: recipient male; RF: recipient female.
Analyzing only male gender recipients, receiving a liver from a female gender donor as compared with receiving a liver from a male donor was associated with an increase of 2.26 times in overall post-LT mortality (95%CI 1.149–4.315, p=0.018, p<0.05).
No statistically significant survival difference was detected for the comparisons between all the other donor-recipient gender comparisons (female donor to female recipient vs. male donor to male recipient, p=0.213, p>0.05), (female donor to female recipient vs. female donor to male recipient, p=0.466, p>0.05, female donor to female recipient vs. male donor to female recipient, p=0.513, p>0.05, male donor to male recipient vs. male donor to female recipient, p=0.689, p>0.05, female donor to male recipient vs. male donor to female recipient, p=0.12, p>0.05).
Additional analyses were performed in the group that had the lowest overall survival (male recipients receiving livers from female donors). Among that subgroup of patients, the difference in donor and recipient weight was not related to a decreased post-LT survival (p=0.425, p>0.05). Likewise, the difference between donor and recipient height was not related to a decreased post-LT survival (p=0.114, p>0.05).
As an attempt to quantify the weight mismatches between donor and recipients, we calculated the difference between the weight of the donor and that of the recipient (donor weight — recipient). Thus, we have grouped the donor-to-recipient weight differences into three groups. The first group included individuals with donor-recipient weight differences of more than 10 kg (the recipient weighed 10 or more kilos than the donor); for the second group donor-recipient, weight difference was between -10 and +10 kg; the third group had a donor-recipient weight difference of more than 10 kg (the recipient weighed 10 or less kilos than the donor). Post-LT survival for the three groups was not statistically different (p=0.399, p>0.05).
In order to quantify the height mismatches between donor and recipients, we calculated the difference between the height of the donor and that of the recipient (donor height — recipient height). For quantifying the height differences between the donor and the recipient, we also grouped the height differences into three groups. The first group encompassed individuals with donor-recipient height differences of less than 10 cm (the recipient was 10 or more centimeters taller than the donor); for the second group, donor-recipient height differences were between -10 and +10 cm; the third group had patients with donor weight-recipient height differences of 10 or more kilograms (the recipient was 10 or more centimeters shorter than the donor). Post-LT survival for the three groups was not statistically different (p=0.772, p>0.05).
Among the group of 46 male patients receiving livers from female donors, 12 deaths occurred during the first year (mortality rate of 26.1%) as compared to a 14% 1-year mortality rate of male recipients who received livers from male donors. The causes of death of the 12 male recipients who received livers from female donors included infection (n=7, 58.3%), hemorrhagic shock (n=1), hepatic artery thrombosis (n=1), portal vein thrombosis (n=1), and unknown (n=2). In contrast, in the group of male patients who received liver allografts from male donors, only 12.5% of the deaths occurring during the first post-LT year were caused by infection.
DISCUSSION
In the present study, the outcomes of 202 consecutive adult patients undergoing LT at a single center are analyzed. The main cause of end-stage liver disease in this cohort was cirrhosis secondary to HCV infection, which occurred in 125 out of 202 cases (61.9%). The main indication for LT was HCV cirrhosis with or without HCC. Post-LT survival at 1, 3, 5, and 7 years was comparable to international parameters^ 15,24 ^, being comparable to that of other international centers.
Among all parameters studied, female donor gender was the only predictor of post-LT mortality, being associated with an increase of 81.6% in overall post-LT mortality. Remarkably, the association of female donor gender to post-LT recipient mortality was detected in both male and female recipients. Moreover, this association of female donor gender and mortality was stronger for male recipients. Thus, male recipients who received LT from female donors experienced a 2.2 times increase in overall mortality as compared to male recipients who received livers from male donors (12% higher mortality at 5 years and 21% higher at 7 years post-LT).
Notably, neither weight nor height incompatibilities were related to inferior outcomes in this cohort. Thus, this is the first study showing that the deleterious association of female liver donors-male recipients is not related either to weight or to height incompatibility between donor and recipient.
The few available literature studies on the subject exhibit conflicting results^ 3,4,8,12,13,16,20,23,25 ^. While some studies^ 4,16,20,25 ^ revealed that livers from female donors pose an increased risk of death, other studies do not share the same results^ 3,18 ^. A recent systematic review and meta-analysis showed that female donors in male recipients was associated with an 83% decrease in post-LT survival^ 19 ^.
To date, the reason for this inferior survival for males receiving livers from female donors has not been elucidated. Although it could be related to different sizes among human males and females (a small-for-size effect), the present study did not detect any association of weight and height mismatch to a decrease in overall post-LT survival. Moreover, even in the group of male recipients who received a liver from female donors, neither weight nor height differences accounted for any increase in mortality.
As an attempt to elucidate the reasons for the death of males receiving livers from female donors, a search for the reasons for graft failures was carried out. Interestingly, 58% of all first-year mortality in this group was caused by infection. In contrast, infection was responsible for only 12.5% of all first-year deaths of males who received livers from male donors.
Post-transplant infection was not a predictor of mortality in this study. However, infection was associated with a significant increase in post-transplant hospital stay. It is possible that greater rigor in immunosuppression could prevent the occurrence of infection in patients undergoing LT, positively impacting the long-term survival. The most common site for infection in our series was sepsis without a defined infectious site, with a total of 20 episodes (31.8%). The abdomen, the most common site of infection in literature studies, was only the third most common site of infection in the present study (20.6% of cases). These data differ in relation to two recent review articles, which establish the abdomen as the most common site of infection in LT recipients^ 14,17 ^.
The present study has some limitations. The main one is the retrospective design. The nature of retrospective studies increases the chance of measurement biases. The absence of randomization is another limitation. However, it would be impossible to randomize LT patients to receive a liver graft from a specific deceased donor gender.
CONCLUSIONS
In summary, female donor gender was associated with an increase in overall post-LT mortality, especially for male recipients. The reason for those inferior outcomes of males receiving livers from female donors was not related to anthropometric differences. For male patients receiving livers from female donors, infection was the most common cause of mortality occurring in the first year following LT. Thus, future studies are needed to elucidate whether immune discrepancies would be accountable for the increased mortality of males receiving livers from female donors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adam R Sanchez C Astarcioglu I Bismuth H Deleterious effect of extended cold ischemia time on the posttransplant outcome of aged livers Transplant Proc 1995271118137878841 · pubmed ↗
- 2Bernardi N Chedid MF Grezzana-Filho TJM Chedid AD Pinto MA Leipnitz I Pre-transplant ALBI grade 3 is associated with increased mortality after liver transplantation Dig Dis Sci 2019646169570410.1007/s 10620-019-5456-630637547 · doi ↗ · pubmed ↗
- 3Berrevoet F Hesse UJ de Laere S Jacobs B Pattyn P de Hemptinne B Impact of donor and recipient gender on liver transplantation Transplant Proc 19972983431210.1016/s 0041-1345(97)00966-49414778 · doi ↗ · pubmed ↗
- 4Brooks BK Levy MF Jennings LW Abbasoglu O Vodapally M Goldstein RM Influence of donor and recipient gender on the outcome of liver transplantation Transplant Proc 1997291-2475610.1016/s 0041-1345(96)00212-69123090 · doi ↗ · pubmed ↗
- 5Capra RP Lazzarotto-da-Silva G Grezzana-Filho TJM Viana GS Prediger JE Rabolini B Low hepatic artery resistive index on Doppler ultrasound performed on the first post-liver transplant day is associated both with hepatic artery thrombosis and decreased graft survival Langenbecks Arch Surg 2023408123110.1007/s 00423-023-02971-937306803 · doi ↗ · pubmed ↗
- 6Chedid MF Rosen CB Nyberg SL Heimbach JK Excellent long-term patient and graft survival are possible with appropriate use of livers from deceased septuagenarian and octogenarian donors HPB (Oxford)2014169852810.1111/hpb.1222124467292 PMC 4159459 · doi ↗ · pubmed ↗
- 7Cronst J Prediger L Pinto MA Ferraz J Mattos AZ Alvares-DA-Silva MR Prognostic factors of liver transplantation for acute-on-chronic liver failure Arq Bras Cir Dig 202336 e 177910.1590/0102-672020230061 e 177938088725 PMC 10712924 · doi ↗ · pubmed ↗
- 8Croome KP Segal D Hernandez-Alejandro R Adams PC Thomson A Chandok N Female donor to male recipient gender discordance results in inferior graft survival: a prospective study of 1,042 liver transplants J Hepatobiliary Pancreat Sci 20142142697410.1002/jhbp.4024123790 · doi ↗ · pubmed ↗