Retrograde gastric decompression and anterograde enteral nutrition feeding in retrosternal esophagectomy for esophageal cancer
Jingrong Yang, Wenxuan Xia, Shixin Ye, Duohuang Lian, Jie Zhu, Jian Wu, Zhiyong Zeng

TL;DR
This study compares two post-surgery methods after esophagectomy for cancer and finds retrograde gastric decompression and feeding to be safe and effective.
Contribution
The study introduces retrograde gastric decompression and feeding as a viable alternative to traditional nasogastric methods after esophagectomy.
Findings
Retrograde gastric decompression and feeding had comparable complication rates and shorter gastric tube retention.
Operative time was longer with retrograde gastric decompression and feeding, but blood loss and R0 resection rates were similar.
Tube-related complications trended lower with retrograde gastric decompression and feeding, though not statistically significant.
Abstract
Postoperative care after McKeown esophagectomy remains challenging. The aim of this study was to evaluate retrograde gastric decompression and feeding as an alternative to nasogastric decompression and nasogastric-jejunal feeding. This retrospective study analyzed 142 esophageal cancer patients undergoing McKeown esophagectomy (between June 2020 and August 2022): retrograde gastric decompression and feeding (n=74) vs. nasogastric-jejunal (n=68). Outcomes included operative parameters, complications, and recovery metrics. Retrograde gastric decompression and feeding required longer operative time (183.0±41.7 vs. 169.4±32.6 min, p=0.031) but showed comparable blood loss, R0 resection rates (95.9 vs. 97.1%), and lymph node yield. Gastric tube retention was shorter with retrograde gastric decompression and feeding (3.2±1.6 vs. 3.6±1.4 days). Complication rates (anastomotic leak: 10.8 vs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
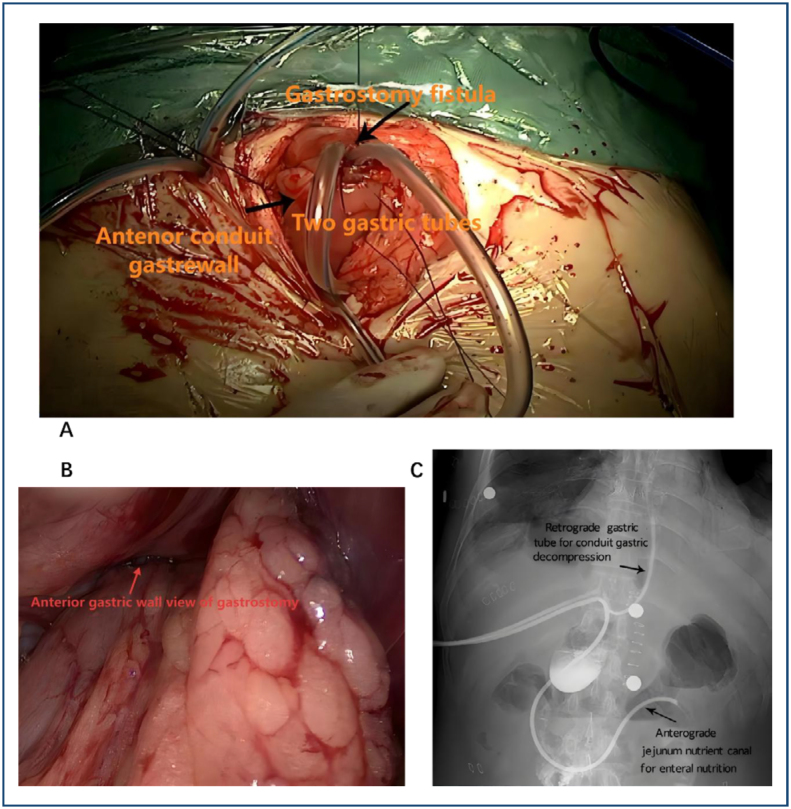 Figure 1
Figure 1| Parameters | RGDF group n=74 | NGJ group n=68 | p-value | |
|---|---|---|---|---|
| Demography | ||||
| Onset age (mean±SD) | (58.1±13.1) years | (53.7±11.2) years | 0.100 | |
| Male, n (%) | 52 (70.3%) | 44 (64.7%) | 0.501 | |
| Female, n (%) | 22 (29.7%) | 24 (35.3%) | ||
| Location of lesion | ||||
| Upper third, n (%) | 18 (24.3%) | 17 (25.0%) | 0.773 | |
| Middle third, n (%) | 43 (58.1%) | 42 (61.8%) | ||
| Lower third, n (%) | 13 (17.6%) | 9 (13.2%) | ||
| Histological type | ||||
| Squamous carcinoma, n (%) | 69 (93.2%) | 64 (94.1%) | 0.935 | |
| Adenocarcinoma, n (%) | 3 (4.1%) | 2 (2.9%) | ||
| Others, n (%) | 2 (2.7%) | 2 (2.9%) | ||
| Depth of tumor invasion | ||||
| Tis, n (%) | 3 (4.1%) | 1 (1.5%) | 0.912 | |
| T1, n (%) | 11 (14.9%) | 9 (13.2%) | ||
| T2, n (%) | 31 (41.9%) | 30 (44.1%) | ||
| T3, n (%) | 27 (36.5%) | 26 (38.2%) | ||
| T4, n (%) | 2 (2.7%) | 2 (2.9%) | ||
| Lymphatic metastasis | ||||
| N0, n (%) | 33 (44.6%) | 30 (45.6%) | 0.797 | |
| N1, n (%) | 30 (40.5%) | 28 (41.2%) | ||
| N2, n (%) | 8 (10.8%) | 9 (13.2%) | ||
| N3, n (%) | 3 (4.1%) | 1 (1.5%) | ||
| TNM stage | ||||
| Tis, n (%) | 3 (4.1%) | 1 (1.5%) | 0.129 | |
| I, n (%) | 25 (33.8%) | 29 (42.6%) | ||
| II, n (%) | 30 (40.5%) | 32 (47.1%) | ||
| III, n (%) | 16 (21.6%) | 6 (8.8%) | ||
| Parameters | RGDF group, n=74 | NGJ group, n=68 | p-value | |
|---|---|---|---|---|
| Blood loss (mL), mean±SD | 196.9±51.6 | 185.5±41.9 | 0.153 | |
| Operation time (min), mean±SD | 183.0±41.7 | 169.4±32.6 | 0.031 | |
| Surgical resection status | ||||
| R0 resection, n (%) | 71 (95.9%) | 66 (97.1%) | 0.877 | |
| R1 resection, n (%) | 1 (1.4%) | 1 (1.5%) | ||
| R2 resection, n (%) | 2 (2.7%) | 1 (1.5%) | ||
| Harvested lymph node, mean±SD | 13.7±5.1 | 12.5±3.9 | 0.120 | |
| Days of keeping a gastric tube for decompression, mean±SD | 3.2±1.6 | 3.6±1.4 | 0.116 | |
| Days of keeping a feeding tube, mean±SD | 23.7±7.6 | 22.5±8.1 | 0.364 | |
| ICU stay (days), mean±SD | 3.2±1.0 | 3.5±1.2 | 0.107 | |
| LOHS (days), mean±SD | 9.8±2.7 | 10.2±3.1 | 0.413 | |
| Postoperative drainage time (days), mean±SD | 2.03±0.88 | 1.98±1.23 | 0.7797 | |
| Postoperative pain score | 2.96±1.78 | 3.67±1.23 | 0.007 | |
| Surgical complications, n (%) | ||||
| Recurrent laryngeal nerve injury | 4 (5.4%) | 3 (4.4%) | 1.000 | |
| Anastomotic leak | 8 (10.8%) | 7 (10.3%) | 0.920 | |
| Anastomotic stenosis | 6 (8.1%) | 4 (5.9%) | 0.747 | |
| Postoperative hemorrhage | 1 (1.4%) | 1 (1.5%) | 1.000 | |
| Chylothorax | 2 (2.7%) | 1 (1.5%) | 1.000 | |
| Cervical wound infection | 1 (1.4%) | 1 (1.5%) | 1.000 | |
| Respiratory complications | 12 (16.2%) | 11 (16.2%) | 1.000 | |
| Respiratory infections | 8 (10.8%) | 7 (10.3%) | 0.920 | |
| Respiratory failure | 2 (2.7%) | 1 (1.5%) | 1.000 | |
| Gastric emptying disorders | 0 (0.0%) | 0 (0.0%) | 1.000 | |
| Arrhythmia and other cardiac complications | 3 (4.1%) | 3 (4.5%) | 1.000 | |
| Tube-related complications, n (%) | 4 (5.4%) | 7 (10.3%) | 0.276 | |
| Tube obstruction | 1 (1.4%) | 1 (1.5%) | 1.000 | |
| Wound infection | 1 (1.4%) | Null | Null | |
| Peripheral leakage of the nutrient canal | 2 (2.7%) | Null | Null | |
| Tube falling off | 0 (0%) | 3 (4.4%) | 0.107 | |
| Necrosis of the nasal alar | Null | 1 (1.5%) | Null | |
| Nasosinusitis | Null | 2 (2.9%) | Null | |
| In-hospital mortality, n (%) | 1 (1.4%) | 1 (1.5%) | 1.000 | |
- —Postdoctoral Workstation of the 900th Hospital of Joint Logistics Support Force
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Esophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes
INTRODUCTION
Esophageal cancer remains a major global malignancy, with approximately 511,000 new cases and 445,000 deaths annually^ 1 ^. For resectable cases, McKeown esophagectomy via retrosternal approach has emerged as a preferred surgical alternative to conventional open procedures, offering reduced operative trauma and complication rates^ 2,3 ^.
Despite these benefits, esophageal cancer management requires meticulous postoperative care to mitigate complications associated with conventional tube placements^ 4 ^. Current practice predominantly utilizes nasogastric-jejunal (NGJ) tubes^ 5 ^, which carry substantial risks of nasal injury, tube dislodgement, and sinusitis^ 6 ^.
We developed a modified retrograde gastric decompression and feeding (RGDF) technique during McKeown procedures. By establishing a gastrostomy fistula for simultaneous decompression and jejunal feeding, this approach aims to eliminate nasal trauma while maintaining nutritional efficacy.
This study retrospectively evaluated the feasibility, safety, and short-term efficacy of the RGDF technique in patients undergoing McKeown-type esophagectomy. Specifically, we aimed to assess its impact on postoperative recovery, complication rates, and overall patient outcomes.
METHODS
Patients
This retrospective study analyzed 142 esophageal cancer patients undergoing McKeown esophagectomy with retrosternal reconstruction (between June 2020 and August 2022). Patients were stratified into RGDF (n=74) and NGJ (n=68) groups based on postoperative management. Inclusion criteria required: histopathologically confirmed esophageal cancer, clinical stage T1-3M0 (AJCC 7th ed.^ 7 ^), adequate cardiopulmonary function, and absence of severe comorbidities or adhesions. The Ethics Committee of Fuzhou General Hospital approved the protocol, with written consent obtained.
Surgical procedures
The procedure followed Yang et al.'s VATS approach^ 8 ^, comprising three phases:
(1) Thoracic: pulmonary ligament division, esophageal mobilization, azygos vein ligation, and mediastinal lymphadenectomy; (2) Abdominal: laparoscopic gastric mobilization with lymph node dissection and creation of a 40–50 mm gastric conduit; and (3) Cervical: left neck incision with esophageal transection and end-to-end anastomosis (EEA). Figure 1 shows the gross anterior view (1A), intraperitoneal view (1B), and plain abdominal radiograph (1C) after tube placement.
Gross anterior view (A), intraperitoneal view (B), and plain abdominal radiograph (C) after tube placement.
The RGDF group received an additional gastrostomy: Two tubes (16 Fr, 125 cm in length, 5.3 mm in diameter; TERUMO Medical Products Co., Ltd., Hangzhou, China) were inserted through a 1 cm incision, 3 cm to the right of the midline. A double purse-string suture was placed 5 cm proximal to the pylorus, with one tube advanced 10 cm retrogradely and another 40 cm anterogradely into the jejunum. The placement was confirmed radiographically.
The NGJ group received standard nasogastric (35–40 cm) and nasojejunal (80–100 cm) tube placement.
Intraoperative and postoperative parameters were collected to evaluate surgical outcomes, including blood loss, operative time, extent of resection (R0, R1, and R2), harvested lymph nodes, and recovery metrics such as intensive care unit (ICU) stay, hospital stay, and duration of gastric and feeding tube placement. Postoperative complications were categorized into surgical and tube-related complications. In-hospital mortality was also recorded. Postoperative drainage volumes were recorded, and pain scores were evaluated by visual analog scale methods.
Postoperative management
Both groups received standardized decompression using Fr14 negative-pressure suction devices (Shandong Baiduoan Medical). Enteral nutrition was initiated on postoperative day (POD) 1 through a stepwise protocol: Phase 1 (POD1): 5% glucose solution at 20 mL/h; Phase 2 (POD2–3): Transition to Peptisorb^®^ liquid (25 mL/h); Phase 3 (POD4–7): Progressive escalation to 200 mL/h.
Nutritional tubes were flushed with 30 mL warm water before/after each infusion to maintain patency. Patients achieving stable tolerance of 200 mL/h feeding without complications (e.g., diarrhea requiring rate adjustment) were discharged. All enteral tubes were electively removed 14 days post-discharge following outpatient confirmation of oral intake adequacy.
Statistical analysis
Statistical analyses used SPSS 25 with continuous variables presented as mean±standard deviation (SD) (t-test/Mann-Whitney U test) and categorical variables as percentages (χ^ 2 ^/Fisher's exact test). Significance threshold was p<0.05. Post-hoc power analysis assessed sample adequacy.
RESULTS
Baseline demographics and clinicopathological features
The study included 142 patients (RGDF=74 and NGJ=68) with comparable baseline profiles (Table 1). Both groups predominantly comprised males (RGDF 70.3% vs. NGJ 64.7%, p=0.501) and squamous carcinoma histology (93.2 vs. 94.1%). Tumor distribution showed similar patterns, with the middle esophagus being the most frequent (58.1 vs. 61.8%). Tumor-Node-Metastasis (TNM) staging revealed 95.9% of RGDF and 90% of NGJ patients in stages I–III (p=0.129).
Peri-operative outcomes and complications
RGDF required longer operative time (183.0±41.7 vs. 169.4±32.6 min, p=0.031) but showed comparable blood loss (196.9±51.6 vs. 185.5±41.9 mL) and R0 rates (95.9 vs. 97.1%). Both groups had similar lymph node yield (13.7±5.1 vs. 12.5±3.9), hospital stay (9.8±2.7 vs. 10.2±3.1 days), and gastric decompression duration (3.2±1.6 vs. 3.6±1.4 days, p=0.116). There was no difference in the mean drainage time between the RGDF and NGJ groups (2.03±0.88 vs. 1.98±1.23). The pain score of the NGJ group was significantly higher than that of the RGDF group (2.96±1.78 vs. 3.67±1.23) but with only a small increase. Postoperative complications within 3 weeks are summarized in Table 2. The overall incidence of complications was similar between the RGDF and NGJ groups, with anastomotic leakage (10.8 vs. 10.3%), respiratory complications (16.2 vs. 16.2%), and respiratory infections (10.8 vs. 10.3%) being the most frequent. RGDF showed a clinically relevant 48% reduction in tube-related complications (5.4 vs. 10.3%, p=0.276). In the RGDF group, the most common tube-related complications were obstruction (1.4%), wound infection (1.4%), and leakage around the nutrient canal (2.7%). In the NGJ group, tube dislodgement (4.4%), nasal alar necrosis (1.5%), and nasosinusitis (2.9%) were more frequently observed. Gastric emptying disorders were not observed in either group. Mortality rates were equivalent (1.4 vs. 1.5%) (Table 2).
DISCUSSION
Surgical resection remains the cornerstone treatment for resectable esophageal cancer, yet postoperative management of gastric conduit decompression and enteral nutrition continues to pose significant challenges. This study addresses the limitations of conventional NGJ tube placement by proposing RGDF as a dual-function alternative. Our findings demonstrate that RGDF, when applied to McKeown esophagectomy via the retrosternal route, achieves surgical outcomes comparable to those of NGJ while potentially reducing tube-related complications.
Nasogastric drainage is commonly used after esophagectomy to prevent gastric distension, which can significantly increase postoperative complications such as aspiration pneumonitis and mechanical strain on the anastomotic stoma. These issues may result in conduit gastric ischemia and impaired healing of the anastomosis^ 9 ^. Despite their benefits, nasogastric tubes are associated with various complications, including pharyngitis, sinusitis, nasal alar necrosis, accidental dislodgment, gastrointestinal bleeding, and aspiration pneumonia^ 10 ^. During the perioperative period, maintaining adequate nutrition is equally important, as the majority of patients with esophageal cancer present with preoperative malnutrition. Enteral nutrition has been shown to significantly reduce postoperative complications, including infectious complications such as anastomotic fistulas and intra-abdominal abscesses^ 11-13 ^. Common postoperative enteral nutrition methods include oral intake, nasointestinal tubes, and jejunostomy. However, each method has its limitations: early oral intake may increase the risk of anastomotic fistulas and aspiration pneumonia^ 14 ^; nasointestinal tubes can impede effective coughing and compromise pulmonary hygiene^ 15 ^; and jejunostomy may lead to complications such as wound infection, volvulus, hernia, and bowel obstruction^ 16 ^.
The rationale for selecting the McKeown esophagectomy with retrosternal reconstruction lies in its anatomical suitability for RGDF, particularly in the context of esophageal cancer epidemiology in China. Middle esophageal cancer accounts for the majority of cases in China^ 17 ^, and the retrosternal pathway in McKeown esophagectomy provides optimal exposure for mid-thoracic tumors while minimizing anastomotic tension. This anatomical alignment not only facilitates radical resection of middle-third lesions but also enables simultaneous gastrostomy-based decompression and feeding tube placement. Specifically, the retrosternal route offers direct access to the gastric conduit, allowing for precise positioning of retrograde and anterograde tubes without compromising thoracic cavity integrity—a critical advantage for RGDF implementation. This approach eliminates nasal trauma—a well-documented drawback of NGJ tubes^ 10 ^—and aligns with prior studies advocating retrograde decompression as a safer alternative^ 18 ^. Notably, our cohort exhibited a clinically relevant 48% reduction in tube-related complications with RGDF (5.4 vs. 10.3%, p=0.276), albeit without statistical significance. This trend mirrors findings by Puri et al.^ 18 ^, who reported fewer complications with retrograde jejunogastric decompression compared to nasogastric drainage. However, our study extends these observations by integrating enteral feeding into the same gastrostomy site, a novel modification that may streamline postoperative care.
Furthermore, the shorter duration of gastric tube retention in the RGDF group (3.2±1.6 vs. 3.6±1.4 days) may contribute to earlier patient mobilization and reduced anastomotic strain, though direct causal evidence remains to be established. Mechanistically, retrograde decompression combined with anterograde feeding may synergistically promote bowel function recovery through gravitational drainage and peristaltic stimulation—a hypothesis supported by the absence of gastric emptying disorders in both groups.
Despite these benefits, RGDF is not without limitations. The procedure required a longer operative time (183.0±41.7 vs. 169.4±32.6 min, p=0.031), likely due to the technical complexity of dual-tube placement. Challenges such as pyloric sphincter spasm and anatomical angulation between the conduit stomach and duodenum occasionally hindered tube advancement, underscoring the need for advanced surgical expertise. Additionally, while our data suggest RGDF's safety, the retrospective design introduces potential selection bias, and the lack of long-term nutritional follow-up limits conclusions about sustained efficacy. Future prospective studies with standardized nutritional assessments are warranted to validate these findings.
RGDF appears to be a safe and feasible method for enteral nutrition and decompression following McKeown esophagectomy. Its ability to mitigate nasal complications while maintaining nutritional efficacy positions it as a promising alternative to NGJ, particularly in centers proficient in minimally invasive techniques. Further research should focus on cost–benefit analyses, patient-reported outcomes, and comparisons with jejunostomy-based approaches to refine postoperative care protocols.
CONCLUSION
RGDF is a safe, simple, and effective method for the enteral nutrition and decompression of the conduit stomach in patients who have undergone esophagectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 202474322926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Shemmeri E Wee JO Minimally invasive modified Mc Keown esophagectomy Surg Oncol Clin N Am 202433350951710.1016/j.soc.2023.12.02038789193 · doi ↗ · pubmed ↗
- 3Zheng XD Li SC Lu C Zhang WM Hou JB Shi KF Safety and efficacy of minimally invasive Mc Keown esophagectomy in 1023 consecutive esophageal cancer patients: a single-center experience J Cardiothorac Surg 2022171363610.1186/s 13019-022-01781-235292067 PMC 8922768 · doi ↗ · pubmed ↗
- 4Watkins AA Kent MS Wilson JL Surgical adjuncts during esophagectomy Thorac Surg Clin 202030331532010.1016/j.thorsurg.2020.04.00932593364 · doi ↗ · pubmed ↗
- 5Weijs TJ Berkelmans GH Nieuwenhuijzen GA Ruurda JP Hillegersberg R Soeters PB Routes for early enteral nutrition after esophagectomy A systematic review. Clin Nutr 20153411610.1016/j.clnu.2014.07.01125131601 · doi ↗ · pubmed ↗
- 6Guo R Shao L Li B Sun Y Hu H Zhang Y Safety of omitting nasogastric decompression after esophagectomy: a propensity score-matched study J Thorac Dis 202315116000600810.21037/jtd-23-84438090308 PMC 10713308 · doi ↗ · pubmed ↗
- 7Edge SB Compton CC The American Joint Committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM Ann Surg Oncol 20101761471147410.1245/s 10434-010-0985-420180029 · doi ↗ · pubmed ↗
- 8Yang J Xu C Lian D Ye S Zeng Z Liu D Esophageal reconstruction: posterior mediastinal or retrosternal route J Surg Res 2016201236436910.1016/j.jss.2015.11.03027020820 · doi ↗ · pubmed ↗