Implementation and effects of social protection programs for children, older adults, and people with disabilities in Brazil and Ecuador: A scoping review
Julia M. Pescarini, Ana L. Moncayo, Joanna M N. Guimarães, Francine S. Dias, Ronald Ruiz, Samuel A G. da Silva, Gustavo Casais, Michal Shimonovich, Valerie Wells, Mhairi Campbell, Mauricio L. Barreto, S Vittal Katikireddi, Gustavo Matta, Peter Craig

TL;DR
This study reviews social protection programs in Brazil and Ecuador to understand their effects on health and socioeconomic factors for vulnerable groups.
Contribution
The study provides a comprehensive scoping review of social protection programs in Brazil and Ecuador, highlighting gaps in evidence for older adults and people with disabilities.
Findings
Brazil's BFP has substantial evidence on planned effects for children but limited data on unplanned effects in adults.
Ecuador's BDH has some evidence on health effects but lacks data on socioeconomic determinants and unplanned effects.
Few studies in both countries use longitudinal data or comparison groups, and program coverage varies widely.
Abstract
We conducted a scoping review to investigate planned (intentional) and unplanned (not intentional) effects of social protection on socioeconomic determinants of health (SDH) and health inequalities among children, adolescents, elders and people with disabilities, and their caregivers. We reviewed seven programs in (i) Brazil (Programa Bolsa Familia (BFP) and Beneficio de Prestacao Continuada (BPC)), and (ii) Ecuador (Bono de Desarrolo Humano (BDH), Bono 1000 días, Pensión Mis Mejores Años/Pensión para Adultos Mayores, Pensión Toda una Vida/Pensión para personas con discapacidad and Bono Joaquín Gallegos Lara). We searched PubMed, EMBASE, LILACS, Scopus, Econlit, PsycINFO, Global Health, Global Index Medicus and grey literature for studies evaluating program implementation and effects on health outcomes or SDH from 1990 to 2023. We extracted data from 114 studies (84 on BFP, 17 on BDH…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
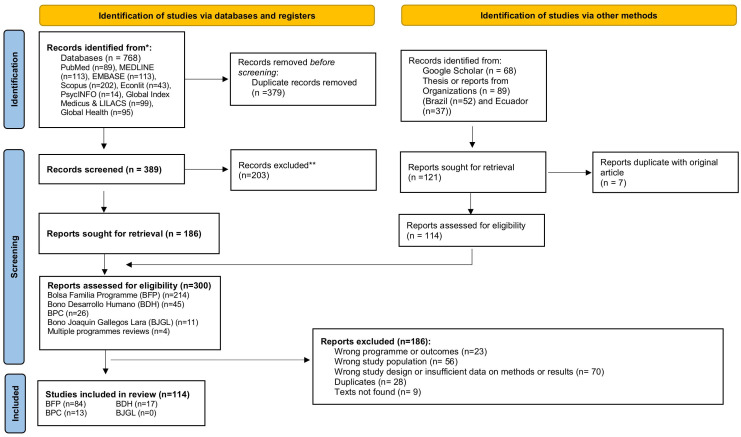 Fig 1
Fig 1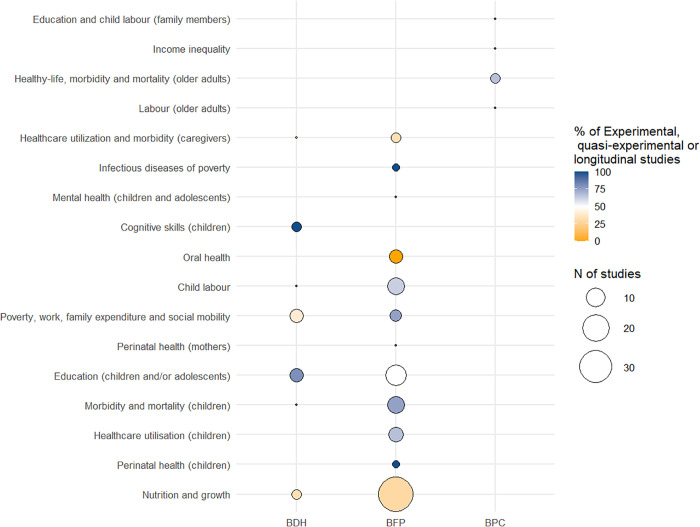 Fig 2
Fig 2- —NIHR/UK
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Palsy and Movement Disorders · Disability Rights and Representation · Poverty, Education, and Child Welfare
Introduction
There is a well-established multidimensional association between poverty and poor health outcomes [1,2]. Poverty is significant in the context of Latin America (LA) due to its history of social and political crisis and high levels of income inequality. Historical social inequalities, with a substantial number of children and older adults experiencing poverty, pushed many LA governments to invest, during the 1990s, in compensatory or pilot initiatives to address these issues [3]. These early programs laid the groundwork for later reforms, especially under progressive governments in the 2000s, that consolidated cash transfer mechanisms into broader social protection strategies aimed at alleviating poverty and improving quality of life [4,5]. Programs or policies included non-contributory pension schemes (also referred to in some contexts as “social pensions”, social allowances or, in some places, ‘bonos’) for elders or people with disabilities experiencing poverty as well as cash transfer programs targeting families facing poverty [4,6].
Conditional cash transfers such as Prospera/Oportunidades in Mexico, Programa Bolsa Familia in Brazil, Bono de Desarollo Humano in Ecuador, and Juntos in Peru, have shown significant impacts in reducing poverty and inequalities, improving school attendance and narrowing educational gaps, fostering economic inclusion, and directly (i.e., through cash and/or conditionalities) or indirectly improving some health outcomes [7–10]. However, conditional cash transfers focus on early life while, by 2020, over 30% of the LA population was living below the poverty line, over 50% of the population aged 15 or older was employed in the informal sector (i.e., defined as a low-productivity), and only 46.4% were contributing to pension systems [11].
In the recent context of economic crises and political instability, with COVID-19 pandemic exacerbating levels of poverty and inequality in Latin America [12], changes that seek the efficacy or effectiveness of those programs. This scoping review draws on social protection data from Brazil and Ecuador, two Upper-middle income countries that have invested, implemented or improved the targeting of specific social protection programs focusing on families experiencing poverty but have not yet achieved universal and comprehensive models of more developed countries in LA [13]. The similarity of social protection schemes in both countries, especially those that focus on the well-being of children from families experiencing poverty and older people or people with disabilities experiencing poverty, permits a fair comparison of how countries implemented and evaluated the effects of these programs. To understand the effects of these programs and suggest areas where further research could inform changes and improvements to maximise the effects of current and future social protection programs [5], we mapped and summarised the available evidence on programs implementation and its effects on health outcomes and their socioeconomic determinants in the two countries.
Methods
The scoping review protocol was registered at the Open Science Framework (OSF) platform (https://archive.org/details/osf-registrations-zw9e5-v1). The study is reported using PRISMA and other guidelines adapted to scoping reviews [14–16].
Population, interventions, implementation and effects (PIIE)
Population: We analysed the body of literature published on the implementation and effects of programs targeting children, adolescents, elders, and people with disabilities in Brazil and Ecuador. Therefore, we have included studies looking either at the programs targeted population, i.e., children and adolescents (aged <18 years), elders (aged ≥60 years) and people with disabilities experiencing poverty; as well as their caregivers.
Interventions: We studied seven social protection programs. In Brazil, we studied the Programa Bolsa Familia (BFP) (Bolsa Familia Program) and the Beneficio de Prestacao Continuada (BPC) (Continuous Cash Benefit). In Ecuador, we studied the Bono de Desarrolo Humano (Human Development Grant), Bono 1000 días (First 1000 days Grant), Pensión Mis Mejores Años/Pensión para adultos mayores (Pension for Elderly), Pensión Toda una Vida/Pensión para personas con discapacidad (Pension for People with disabilities) and Bono Joaquín Gallegos Lara (Joaquín Gallegos Lara Allowance).
Implementation: For implementation studies, we included all research examining changes, challenges, and perceptions in implementing programs or policies at a single point in time, over time, or in specific settings. We considered measures of quality, speed, coverage, and control mechanisms across different years and contexts (e.g., levels of poverty or development, political circumstances, management levels).
Effects: For evaluation studies on the effects of social protection programs, we included outcomes that directly or indirectly affect the lives of beneficiaries and their caregivers, encompassing both socioeconomic determinants of health and a range of health outcomes. Eligible studies included: (i) qualitative research with a structured methodological framework, or (ii) quantitative evaluative studies with a comparison group of individuals, families, or aggregates (e.g., schools, municipalities) who either did not receive the benefit, received a different social protection benefit, or were assessed before and after receiving the benefit.
Detailed information is shown in S1 Table.
Inclusion and exclusion criteria
We included (i) original studies or systematic reviews, (ii) published from 1^st^ January 1990–21st November 2024, (iii) written in Portuguese, Spanish, or English, and that were either (iv) quantitative or qualitative evaluations of the implementation of the seven selected social protection programs within Brazil or Ecuador, as well as comparisons between them at national and subnational levels; or (v) individual or aggregated studies that have evaluated the effects of the programs on the selected outcomes at national and subnational levels.
We excluded papers that did not match our aims in terms of (i) study design: simulation studies, commentaries, literature reviews or scoping reviews, (ii) study programs: studies comparing any of the seven selected programs with others not included in this scoping review, (iii) study population: studies that do not refer to evaluations performed specifically or partially on children or adolescents, elders and people with disabilities as well as on their caregivers, and (iv) comparison groups: effect evaluation studies without a counterfactual group (i.e., a comparison group that did not receive the intervention, that received a different amount of the intervention or a control period) or that included only a description of beneficiaries.
Databases and search strategy
We searched PubMed, EMBASE, LILACS, Scopus, Econlit, PsycINFO, Global Health and Global Index Medicus for original papers, working papers, reports, theses, and official documents. We included search terms in Portuguese, Spanish and English as they comprise both countries’ official and second languages (See the Search Strategy in S2 Table). A simplified search was also performed on Google Scholar. We hand-searched for key documents in the Brazilian and Ecuadorian Ministries of Health and Economic Affairs, the United Nations (UN) Economic Commission for Latin America and the Caribbean (ECLAC) and Pan American Health Organization (PAHO), Inter-American Development Bank, World Bank and Organisation for Economic Co-operation and Development (OECD) Latin America & the Caribbean. Finally, we checked the reference list of all identified studies and reports for additional references.
Selection of studies, data extraction and synthesis
Studies identified were compiled, deduplicated and screened with Rayyan by two researchers in duplicate [17]. In cases of disagreement during title/abstract or full-text screening, the two researchers discussed the conflict. If consensus could not be reached, a third senior researcher was consulted. The key guiding principle for conflict resolution was strict adherence to the inclusion and exclusion criteria defined a priori in the OSF protocol. These criteria included specific definitions regarding target populations (children and adolescents, elders, people with disabilities, and their caregivers), study design (quantitative or qualitative evaluations), comparison groups (evaluation studies without a counterfactual group), and the focus on one of the seven selected social protection programs. Additionally, two experienced researchers from Brazil and one from Ecuador searched the grey literature of their country.
The core data of each selected social protection program was extracted by one policy specialist for each country (i.e., investigators of this scoping review) [18] following an adapted version of the TIDieR-PHP template [19]. We extracted (i) basic information on each program, including the name of the program, main aim, intended short, medium and longer-term impacts, dates that the program was implemented and ended; (ii) information on program delivery, including mechanism of assessing eligibility, eligibility, enrolment, benefits, conditionalities, infrastructure and support provided as part of the intervention, combination with other programs, delivery, ways of monitoring eligibility and conditionalities as well its sanctions when failing to meet conditionalities; and (iii) Implementation characteristics, including who is responsible for the program implementation in each country, speed and coverage of implementation, and planned and unplanned variations.
Data was extracted by one researcher using a standardised form containing data on the aims of the study, study design, study setting, year, population and size, methodology, intervention and comparator descriptions, outcome description, effect direction and main results.
We followed the Synthesis Without Meta-analysis (SWiM) guidelines to report our findings [20] using tables, a narrative synthesis of the available evidence by program and the planned (or intentional) and unplanned (not intentional) outcomes. Planned and unplanned outcomes were defined based on available data on the program’s aims (official documents) and targeted populations. The amount of evidence was summarised into few, some or large, depending on the number of studies and their design, and evidence was further grouped into those with longitudinal or experimental/quasi-experimental designs.
Importantly, throughout the manuscript, we refer to ‘programs’ as the operational expressions of broader ‘policies’. For instance, BPC is not a program but a policy included in Brazilian legislation. However, we referred to BPC as a program. Additionally, we use ‘effects’ to generally describe observed specific associations between programs and outcomes.
The visualisation was done in R Studio, version 4.2.2, using “ggplot”. We used discussions with health and social protection managers to translate the available evidence, and to inform future research.
Results
Search results
We summarized data of all the programs and reviewed 114 studies, of which 84 were on the Bolsa Familia Program from Brazil, 17 on Bono de Desarrollo Humano from Ecuador and 13 on the Continuous Cash Benefit from Brazil (See Fig 1 and Table 1 for programs descriptions). No studies were identified for Bono 1000 días, Pensión Mis Mejores Años (previously named Pensión para adultos mayores), Pensión Toda una Vida (previously named Pensión para personas con discapacidad) or Bono Joaquín Gallegos Lara.
Table 1: Social protection programs eligibility criteria, benefits, conditionalities and main variations over time.
PRISMA flowchart for the selection of the studies.
Data availability, approaches and study designs
Bolsa Familia Program.
The majority of studies used survey data collected once or repetitively across several study years (See Table 2 and S3 Table and S4 Table), whilst some studies used individual-level primary or secondary data on health linked to socioeconomic data from the Unified Registry for Social Programs (Cadastro Unico para Programas Sociais, CadUnico) that is the main mechanism of accessing eligibility for social programs in Brazil. Study designs included (i) an ecological approach with municipality-level data over time using data on BFP coverage and health or SDH data in Brazilian municipalities since BFP implementation; (ii) cross-sectional studies using individual-level data collected through small studies or survey data to analyse the association between BFP and health or SDH at one-time point (i.e., without taking into account when BFP benefit started); (iii) difference-in-difference designs using individual-level data collected through survey data to analyse the association between BFP and health or SDH but taking into consideration multiple time points; (iv) regression discontinuity designs using income as a cutoff point, or (v) cohorts with individual-level data with detailed information on benefit receipt (e.g., cohorts containing BFP data or cohorts of linked data).
Table 2: Main sources of data, outcomes measured, indication of overall results and amount of evidence.
Bono de Desarollo Humano.
Most studies on the BDH analysed secondary data from surveys, and few studies used data from the Social Registry or the information system of the Ministry of Social Development (see S5 Table). Individual studies mostly used regression discontinuity and the Social Registry Index score to assign treatment and control groups. Additionally, two studies were randomised clinical trials, which involved selecting parishes whose households had not received the transfer at baseline but were eligible to receive it to constitute the intervention and control groups. Finally, only one study used a mixed ecological design with counties as the unit of analysis for the period from 2009 to 2014.
Continuous cash benefit.
Similar to BFP, BPC studies on implementation mainly mixed qualitative and quantitative analysis of survey and primary collected data (see S6 Table). Only one study used de-identified data from Single Registry for Beneficiary Information (Sistema Único de Informações de Benefícios – SUIBE), which is the primary registry used by the Instituto Nacional do Seguro Social (INSS, Brazil’s National Institute of Social Security) to assess potential beneficiaries’ eligibility for BPC along with Cadastro Unico. To analyse the effects, there was one cross-sectional survey data from PNAD or semi-structured interviews with beneficiaries and with beneficiaries and stakeholders (i.e., primary data), one study using difference-in-difference designs using municipal-level data BPC coverage data over time, and one study applying regression discontinuity design with age as the cut-off point to survey data containing family level BPC benefit receipt. Similar to BDH, no study evaluated the effects of BPC using linked individual records.
Programme implementation
Bolsa Familia Program.
We found three studies highlighting aspects such as programme implementation, coverage and focus of the programme in those groups, of which one also explored BFP effects on health. In 2007, three years after BFP implementation, BFP coverage (% of eligible people receiving the benefit) already reached 77.6% of eligible families in Brazil, which at that time included families with monthly per capita income < 100 Brazilian reais (BRL) [21]. By analysing BFP coverage and focalisation (% of people receiving the benefit that are eligible) among families enrolled in the “Pelotas Birth Cohort” at birth (i.e., in 2004) and at age 6 years (in 2011) [22], it was found that considering the same income threshold (i.e., BRL100 in 2004 and BRL140 in 2011), BFP coverage increased from 42.8% in 2004 and 70.9% in 2010, while the focalisation of the programme decreased from 77.9% in 2004 to 32.4% in 2010 [22]. However, qualitative research suggested a lack of trained personnel to effectively manage the program and ensure compliance with its conditionalities [23]. Those include shortages of trained personnel to operate the program, lack of intergovernmental cooperation and intersectoral coordination, insufficient space for experience sharing, disorganisation and poor and coercive management of conditionalities (e.g., leading to temporary disruptions unrelated to family circumstances but rather to the monitoring system itself), and poor attendance and effectiveness of the PBF Social Control Commission [23].
Bono de Desarollo Humano.
We found only two studies focusing on implementing the BDH in Ecuador. A first study conducted by the ECLAC suggested a decrease in the coverage of social programs, particularly in Ecuador, since the early 2000s[24]. In Ecuador, the coverage of CCTs dropped from 44% in 2000 to 13% in 2015, a decline attributed to changes in the Human Development Bonus (BDH) program starting from 2013 [24]. Due to fiscal constraints, the target population shifted from people living in poverty and extreme poverty to only those in extreme poverty, and a process was introduced to phase households out of the program. The BDH budget also decreased from 1.062 million dollars in 2013–651 million in 2015 [24]. A study using a mixed-method approach, incorporating both qualitative and quantitative analysis, assessed the effect of costs on the take-up of BDH and suggested that travel costs, personal identity stigma, and dissatisfaction with the government pose important obstacles to take up, after controlling for program design and household poverty [25]. Programs’ take-up was lower in households considered to be “not poor” than among households considered “more or less poor”, “poor”, or “very poor” (43% vs 65% in other households) [25]. Finally, interviews with BDH-eligible Ecuadorians, particularly in remote areas, suggested that the lack of documentation (i.e., birth certificates, identification documents, among others) could be a major obstacle to take up [25].
Continuous cash benefit.
We found eight studies looking at the implementation of the BPC in Brazil, including (i) studies of take-up and coverage [26], (ii) on the claiming process and administration [27–29], (iii) on the effect of introducing after the introduction of the International Classification of Functioning, Disability and Health (ICF) [30,31], and (iv) studies of participation in schooling by BPC beneficiaries [32,33].
Between 2004–2014, the number of people applying for BPC regardless of their income was 2% of the total population aged ≥65 and 0.25% among people under 65 with disabilities (i.e., people reporting great difficulty or impairment to vision, hearing, or mobility, as well as mental disability) [26]. The proportion of BPC benefits granted through legal concessions (i.e., denied by INSS but further approved after judicialisation) was 17% of all benefits for people with disabilities and 4% for elders [26]. Studies pointed to the lack of formal institutionalised collaborations between INSS and municipal social and health management, coordination or monetary incentives to adhere to federal policies to reduce barriers to people accessing BPC [28], with low participation of medical experts (3.3% of benefits between 2006 and 2015) and reduced participation of social welfare professionals in the process of granting the BPC during the same time [29]. In addition, the program’s complexity, the lack of information by applicants and health professionals, the nature of the target population and the lack of interaction between social and health services pose several barriers to its access [27,28].
After the introduction of the ICF, which served as the basis for the preparation of the Brazilian assessment instrument used by the INSS since 2009: the Brazilian Functionality Index (IF-Br) [34], studies found a 22% increase in the percentage of BPC concession for eligible people with disabilities [30], but with differences depending on the age group [30]. In addition, from 1998 to 2014, the incorporating the new classification, the speed of granting benefits has not increased and BPC may not have been able to reach all the target population, with men 1.5 times more likely than women to have their application deferred [31].
Finally, a study looking at participation and barriers in schooling by BPC beneficiaries showed that, in 2008, 7.9% of children aged 12 never attended school, of which 71,6% were because the caregivers never looked for access for children at school [32]. In 2012, a second study found that the number of individuals under 18 years who are beneficiaries from BPC who were not enrolled at a school was 28.84% in 2012 [33]. Both studies pointed out that children with disabilities face difficulties attending school [32], including those related to care of the individual, insertion of children and adolescents into teaching and learning activities and lack of public policies necessary to make it possible to stay at school [33]. In addition, among caregivers who tried to enrol their children at school, 18.1% cited that schools refused to enrol the children/adolescent [32].
Effects on socioeconomic determinants of health and health
Bolsa Familia Program.
We included 81 studies looking at the effects of BFP on health and socioeconomic determinants of health, of which 22 investigated the effects of BFP on the socioeconomic determinants of health and 59 the effects of BFP on health outcomes (See Table 2, 23 Table, S4 Table and Fig 2). We considered as planned effects those that were aligned to the program objectives, such as the effects of the cash on improving food security and nutrition, reducing poverty, fomenting education of children and reducing child labour, fomenting intergenerational social mobility and wealth; and those directly affected by conditionalities such as health indicators of children under 5, perinatal outcomes of mothers and newborns, and education of children and adolescents. We considered the effects on other health outcomes as unplanned (See Table 2).
Evidence map for the effects of social protection programs targeted to children (Bolsa Familia Programme – BFP, or Bono de Desarrollo Humano – BDH) and to elders and people with disabilities experiencing poverty (Beneficio de Prestacao Continuada – BPC) on health and social determinants of health of children.
Twelve studies analysed the effect of BFP on educational indicators such as school enrolment and attendance, dropout rates, grade progression, grade repetition or age-grade distortion [35–46], of which one was a systematic review [45]; and one paper investigating if BFP could mitigate shocks that might affect educational outcomes, such as rainfall [41]. Seven studies analysed the effect of the program on child and adolescent labour [41,43,47–51]. Five studies looked at the effect of BFP on the work or employment of caregivers, poverty, social cohesion or other markers of improved socioeconomic conditions and social mobility [52–56], of which one investigated social inclusion, exclusion and social cohesion using a qualitative approach [53]. Although most studies attempted to apply quasi-experimental designs (i.e., including regression discontinuity around the income threshold or propensity score methods), only two studies extracted information before and after receiving BFP [43,52].
Effects of BFP on health are analysed in 59 studies, but few have drawn on longitudinal data or applied quasi-experimental designs to find comparable interventions and comparison groups (See Fig 2). Regarding the planned effects, nutritional and growing monitoring outcomes were the most frequently studied [22,57–88]. Still, the evidence of its beneficial effects on reducing malnutrition and improving growth outcomes was not consistent across studies, age groups and study designs. This was further evidenced in a 2009 systematic review, which included data from social protection programs in Brazil, Ecuador, and other countries [87]. Other planned effects of BFP included maternal mortality [89–91]; mortality and morbidity of children, including for different age groups and by causes such as diarrhoea [62,91–98], healthcare utilisation, monitoring and vaccination [70,81,85,96,99–101]. In terms of unplanned effects, some studies looked at oral health of beneficiaries and non-beneficiaries of BFP [58,102–105], one looked at mental health of children of beneficiary families of BFP over time [106], two studies looked at the effect of BFP on leprosy incidence and treatment outcomes among children/adolescents under 15 years [107,108], and three looked healthcare of caregivers or women at reproductive age, including cervical cancer screening, non-communicable diseases prevalence and adolescent pregnancy (i.e., aged 15–18 years) [109–111]
Bono de Desarrollo Humano.
Fifteen studies investigated the effects of BDH on SDH or health outcomes, four assessing their effects on health and eleven on SDH (See S5 Table and Fig 2). Twelve were observational studies data on coverage of BDH and health or educational indicators, using either households or areas as the unit of analysis; two were randomized control trials using primary data and one was a qualitative study. Among the studies that assessed the effects on health or SDH (N = 15), the majority (93%) were quantitative studies and assessed the effect on nutrition and growth (e.g., exclusive breastfeeding, food insecurity, height-for-age z-score and haemoglobin concentration) [112–114], one on morbidity and mortality of children by all-causes and specific causes [115], four on school enrolment and delay [116–119], three on cognitive achievement and skills [114,120,121], four on poverty and social mobility [122–125], and one on child labour [118]. The only qualitative study evaluated the effect on women’s rights, in terms of their quality of life, access to basic social services, visibility, and empowerment. Similar to the Brazilian BFP, BDH includes health and education conditionalities for children and breastfeeding women (See Table 1 and Table 2). Therefore, observed effects on child nutrition, development, morbidity and mortality and education of children were considered planned effects; whereas more general effects on poverty reduction and gender inequalities were considered unplanned effects (See Table 2).
Most studies effects evaluated the effect of BDH on health or SDH indicators used regression discontinuity designs based on the unified vulnerability assessment index (i.e., SELBEN points cutoff point for eligibility of 50.65 [113,117,120]), or the Social Registry scores (cutoff points for eligibility of 34.68). Some were also randomized trials with baseline and follow-up surveys conducted by the World Bank and the government of Ecuador [114,116,118], used a difference-in-difference approach with individual-level data [117,122,124], and one an ecological study applying a time series in Ecuadorian counties between 2009 and 2014 [115]. Two descriptive studies used ENEMDU (Encuesta Nacional de Empleo, Desempleo y Subempleo), and looked at the effects of receiving BDH on poverty [123]; and estimated what the poverty rates would have been in the absence of the program [125]. Finally, one study evaluated the effect of the BDH on gender inequalities using a qualitative methodology, including focus groups, workshops with stakeholders, and semi-structured interviews in three counties of Ecuador [126].
Continuous cash benefit.
Five studies analysed the effects of BPC on health or SDH (See S6 Table and Fig 2). Two studies evaluated the effects of BPC on the socioeconomic determinants of health (i.e., municipality health inequality measured by the Gini Index and individual and labour force participation in the month or week before the benefit receipt of the beneficiary and co-residents aged 18-49y, 18-29y and of children aged 10-15y (i.e., child labour) and school attendance of children aged 10-15y) [127,128] and three evaluated the effects on healthy (one on healthy life expectancy [129], one on nutrition and food security [130] and one on all cause hospitalization and mortality) [131] (See Table 2). The latter also evaluated the effect of BFP but included both programme coverages in the same analysis [131]. The definition of beneficiaries in each study varied but only one contained information on benefit receipt, while the others were either conducted at ecological level or based on proxies such as age and income. Only one study applied a difference-in-difference approach using repetitive individual level measurements from PNAD data for 1995 and 2006 [128], while two explored the age as a cutoff using a regression discontinuity design (RDD) [127,130].
Discussion
In this study, we have summarised the scope of evidence on the implementation and effects on the socioeconomic determinants of health and health conditions of key social protection programs or policies targeting children, pregnant women, elders and people with disabilities experiencing poverty in Brazil and Ecuador. In Brazil, we found substantial literature on the planned effects of the Brazilian conditional cash transfers targeting children and pregnant women but little evidence for unplanned effects on those groups. In addition, we found very little evidence of the effects of the continuous cash benefit targeting elders and no evidence for people with disabilities. In Ecuador, only the BDH was evaluated. There were few individual-level studies, mostly in the early years of the programme implementation, with only ecological data available to study long-term effects.
When looking at social protection for children and pregnant women, the Brazilian BFP programme has been extensively researched regarding its effects on reducing poverty and inequality, improving the socioeconomic determinants of malnutrition, and morbidity and mortality among children and mothers. However, only few studies adequately compare beneficiaries with non-beneficiaries who were eligible for the programme, suggesting that further research should use longitudinal studies and with adequate intervention and comparison groups to provide better evidence regarding possible causal links between the intervention and the studied outcome. The BDH has been evaluated using individual data in the first years of implementation in villages that were randomised to receive the intervention. Long-term or unplanned effects of BDH have only been evaluated at the ecological level, which limits the scope of analysis for specific subgroups. Our review also highlights that while there is some evidence of the BDH program having positive effects, particularly on reducing under-5 mortality and poverty, its effects on other health and educational outcomes are less conclusive. There is no individual-level data available to understand further the overall unplanned effects and long-term planned effects of BDH on the SDH and health outcomes (See Box 1).
In relation to implementation, we found that successful delivery of both BFP and BDH depends on the presence of complementary, but relevant initiatives [132], such as better coordination between the bodies responsible for providing the cash with those providing health and education conditionalities. For instance, whilst BDH enables the maintenance of a certain level of consumption for the poorest households [126], the pressure of the conditionalities, including the penalty of withdrawing the cash transfer, can be a source of daily confrontations within households that undermine women’s abilities to achieve their own well-being and of their children [126]. These tensions in family relationships can have negative effects on the emotional well-being of mothers and children that can, in many cases, nullifies the potential positive impacts of the transfer [126].
Therefore, the absence of coordinated actions or programs that work in conjunction with cash transfers limits the effects of programs such as the BDH on improving the quality of life and access to social services [126]. Social protection programs are often implemented alongside other social and health interventions, but there is limited research on how these programs interact and their combined effects on health outcomes. Future studies should investigate the interaction between different programs to identify potential synergies and optimize their impact.
We found no studies looking at the effects of social protection for elders and people with disabilities in Ecuador. However, the Brazilian BPC was found to have the potential to alleviate poverty and improve the quality of life of elders and people with disabilities experiencing poverty in Brazil, given its targeted eligibility and high levels of benefits. The few studies available on the program indicate that BPC can reduce income inequality, improve the quality of life and increase participation in work and education among eligible elders and their household members. However, limited research is available on the effects of BPC on morbidity and mortality in elders or people with disabilities, suggesting that further studies of both its broader planned and unplanned effects would be useful (See Box 1). Finally, although BPC coverage and instruments that adequately measure disabilities have improved over time, the barriers to accessing BPC can limit the planned and unplanned effects of BPC on the social determinants of health and the health of targeted populations.
Our scoping review has some limitations. First, we might not have captured all the literature about program implementation or effects, especially in the context of Brazil, as we may not have identified studies that were not focused on children, older people, people with disabilities and their caregivers. Second, our search might not have captured the effects of global economic crises and the COVID-19 pandemic on the implementation of social programs and their impact on population well-being. However, we conducted a comprehensive search, including grey literature, and summarised a large amount of evidence regarding the seven social protection programs focusing on the most vulnerable people in Ecuador and Brazil.
Conclusions
In conclusion, our scoping review identifies the need for more research on the unplanned effects of BFP on health outcomes, as well as on the implementation and planned and unplanned effects of BPC, BDH, and other social protection programs focusing on elders and people with disabilities in Ecuador and Brazil. Most importantly, the lack of individual-level data and studies investigating planned and unplanned health effects in Ecuador prevents us from understanding its long-term effects. Because randomized controlled trials are often not feasible, studies could more frequently and better utilize quasi-experimental designs, simulations, and forecasting models to determine the most impactful and cost-effective interventions. In addition, we highlight the importance of more standardised approaches to investigating the effects of social protection on health outcomes, with more detailed socioeconomic data that allow the construction of better and more comparable control groups. Recent legal and policy frameworks in both Brazil (Presidential Decree No. 11.353/2023 [133] and a proposed bill PL 3083/2022) and in Ecuador’s constitution [134] have reinforced the importance of monitoring and evaluating social programs aiming to promote transparency, efficiency, and alignment with stated objectives. However, our review shows that systematic evaluations remain scarce, often constrained by limited data availability, methodological capacity, and political or institutional priorities that emphasises program expansion or operational continuity over rigorous impact assessment. Furthermore, qualitative research should play a complementary role in supporting and interpreting quantitative findings.
Box 1. Suggested priorities and potentialities to study the effects of social protection programs on health or Socioeconomic determinants of health outcomes based on this review and discussions with stakeholders.Brazilian Bolsa Familia Programme (BFP)
- Unplanned effects on infectious diseases of poverty in targeted groups (e.g., infant tuberculosis)
- Unplanned effects on violence and pregnancy in children and adolescents
- Effects of changes in the BFP conditionalities monitoring on food and nutritional insecurity, growth curve and others
- Mitigation effects of climate change on health events
- Interaction of BFP with other social protection and health programmes Brazilian Beneficio de Prestacao Continuada (BPC)
- Effects on all-cause and cause-specific mortality and morbidity of older adults
- Effects on all-cause and cause-specific mortality of people with different grades and types of disabilities
- Unplanned effects on health status (morbidity and mortality) of people living with BFP beneficiaries
- Interaction of BPC with other social protection and health programmes Ecuadorian Bono de Desarrollo Humano (BDH)
- Unplanned effect on the mental health of children and their caregivers, health behaviours and gender dynamics.
- Effects on premature and all-age cardiovascular mortality
- Effects on maternal mortality
- Effects on mitigating the impact of economic crises/ economic downturn.
- Interaction of BDH with other social protection and health programmes
Supporting information
S1 TableEligibility criteria for selecting papers.(DOCX)
S2 TablePIIE (Population, Intervention, Implementation and Effects) search terms.(DOCX)
S3 TableStudies on the effects of the Bolsa Familia Programme on socioeconomic determinants of health (N = 22)(Brazil).(DOCX)
S4 TableStudies on the effects of the Bolsa Familia Programme on health outcomes (N = 59) (Brazil).(DOCX)
S5 TableStudies on the effects of the Bono de Desarollo Humano on socioeconomic determinants of health or health outcomes (N = 15) (Ecuador).(DOCX)
S6 TableStudies on the effects of the Continuous cash benefit on socioeconomic determinants of health or health outcomes (N = 5)(Brazil).(DOCX)
S1 FilePRISMA P Checklist.(DOCX)
S2 FileAcknowledgment.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Muntaner C, Solar O, Vanroelen C, Martínez JM, Vergara M, Santana V. Unemployment, informal work, precarious employment, child labor, slavery, and health inequalities: pathways and mechanisms. Int J Health Serv. 2010;40(2):281–95.20440971 10.2190/HS.40.2.h · doi ↗ · pubmed ↗
- 2Horton R. Offline: Why have we forgotten about poverty?. Lancet. 2024;403(10445):2678. doi: 10.1016/S 0140-6736(24)01297-2 38908865 · doi ↗ · pubmed ↗
- 3Economic Commission for Latin America and the Caribbean ECLAC. Social Panorama of Latin America 2019. Santiago. 2019. https://repositorio.cepal.org/server/api/core/bitstreams/411976 dd-6221-43de-a 9a 2-a 17449 c 905fe/content
- 4Bastagli F. From social safety net to social policy? The role of conditional cash transfers in welfare state development in Latin America. 2009. https://www.econstor.eu/handle/10419/71826
- 5Papadopoulos T, Velázquez Leyer R. Two Decades of Social Investment in Latin America: Outcomes, Shortcomings and Achievements of Conditional Cash Transfers. Social Policy & Society. 2016;15(3):435–49. doi: 10.1017/s 1474746416000117 · doi ↗
- 6Ullmann H, Atuesta B, Rubio M, Cecchini S. Non-contributory cash transfers: An instrument to promote the rights and well-being of children with disabilities in Latin America and the Caribbean. SSRN Journal. 2021.
- 7Gil-GarcíaÓF. The Prospera conditional cash transfer program and its impact on education, labor, and migration in an indigenous Mayan community in Chiapas, Mexico. J Prev Interv Community. 2021;49(1):60–80. doi: 10.1080/10852352.2019.1633068 31282309 · doi ↗ · pubmed ↗
- 8Martínez-Martínez OA, Coronado-García M, Orta-Alemán D. The effect of cash transfers from the PROSPERA programme (formerly Oportunidades) on poverty in urban households in Northeast Mexico. J int comp soc policy. 2020;36(2):142–58. doi: 10.1080/21699763.2019.1641133 · doi ↗