Nitrogen Oxide Inhalation Lung Injury From an Industrial Explosion: A Case Report and Review of the Literature
Hitokazu Tsukao
TL;DR
A man inhaled nitrogen oxide during an industrial explosion and developed lung injury, but recovered without steroids, showing that mild cases can resolve with observation.
Contribution
This case report provides a detailed clinicoradiologic-pathologic correlation of mild nitrogen oxide-induced lung injury.
Findings
Nitrogen oxide inhalation caused centri-acinar dominant alveolitis with ground-glass nodules on CT.
Supportive care without corticosteroids resolved the condition in a patient with preserved oxygenation.
Lymphocytosis and type II pneumocyte hyperplasia were observed in bronchoalveolar lavage and biopsy.
Abstract
An industrial explosion released nitrogen oxide, which a 43-year-old man inhaled at work. He developed cough and exertional dyspnea without hypoxemia, and chest computed tomography obtained two days after exposure showed poorly defined centrilobular ground-glass nodules predominantly in the lingular and lower lobes. Bronchoalveolar lavage revealed an increased total cell count with mild lymphocytosis. Transbronchial lung biopsy demonstrated type II pneumocyte hyperplasia, mural thickening with focal fibrosis, and fibrin deposition consistent with centri-acinar dominant alveolitis. Supportive care without corticosteroids led to clinical and radiologic resolution. This case highlights the latent onset pattern after nitrogen oxide inhalation and provides clinicoradiologic-pathologic correlation for a mild presentation, suggesting that careful observation may be reasonable when oxygenation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
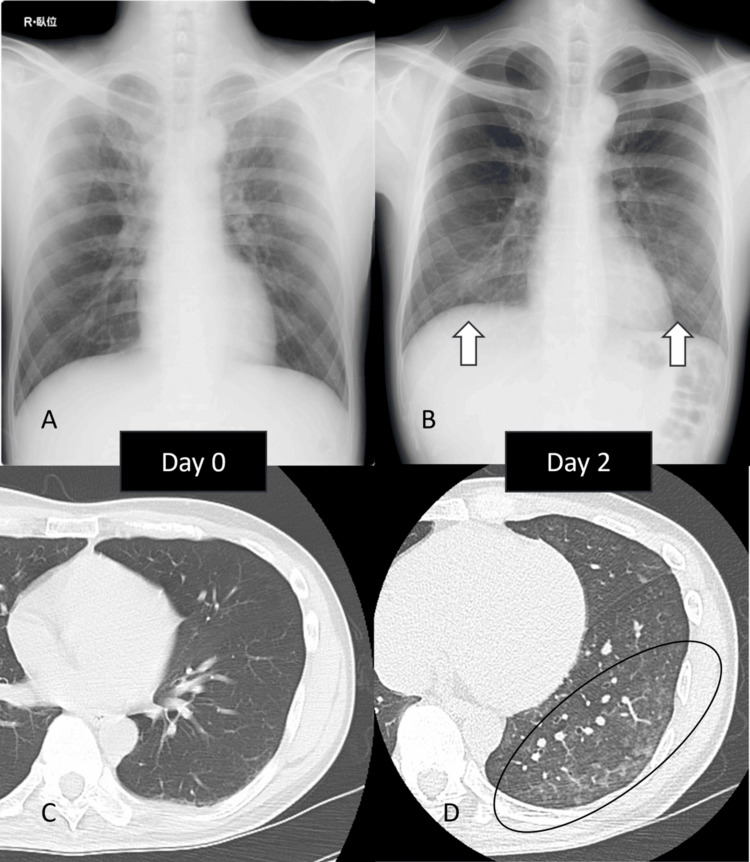 Figure 1
Figure 1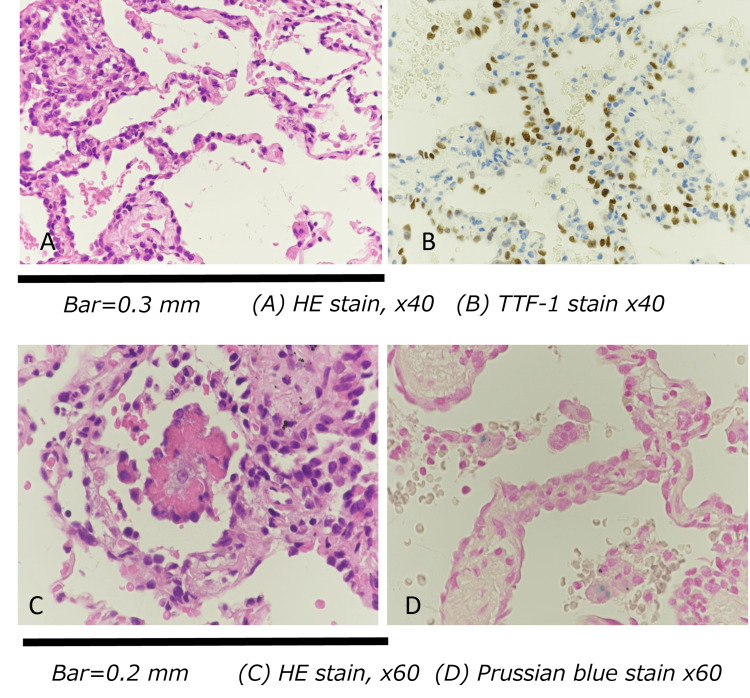 Figure 2
Figure 2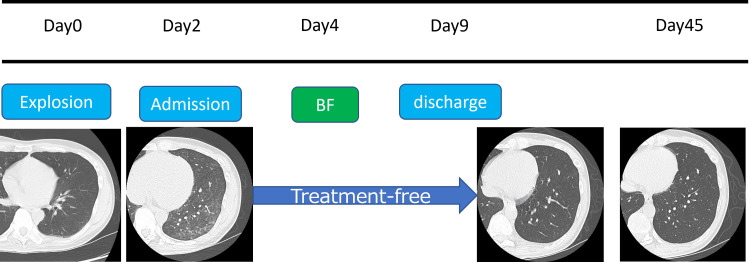 Figure 3
Figure 3| Parameter | Result | Reference range |
| WBC | 11,690 /µl | 3,500–9,000 /µl |
| Neutrophils (%) | 77.1 % | 40–70 % |
| Eosinophils (%) | 1.8 % | 1–6 % |
| Basophils (%) | 0.3 % | 0–1 % |
| Monocytes (%) | 8.1 % | 2–8 % |
| Lymphocytes (%) | 12.7 % | 20–45 % |
| RBC | 4.78 ×10^6 /µl | 4.10–5.30 ×10^6 /µl (M) |
| Hemoglobin (Hb) | 14.8 g/dl | 13.5–17.5 g/dl (M) |
| Hematocrit (Hct) | NA | 40–50 % (M) |
| Platelets (Plt) | 28.0 ×10^4 /µl | 150–350 ×10^3 /µl |
| D-dimer | 0.20 µg/l | <0.5 µg/ml |
| FiO₂ | 21 % | 21 % (room air) |
| pH | Error (unknown) | 7.35–7.45 |
| pCO₂ | 34.2 mmHg | 35–45 mmHg |
| pO₂ | 91.9 mmHg | 80–100 mmHg |
| Lactate | 7.0 mg/dl | 4.5–19.8 mg/dl (0.5–2.2 mmol/L) |
| FCOHb | 0.9 % | <2 % |
| TP | 6.5 g/dl | 6.6–8.1 g/dl |
| Albumin | 3.3 g/dl | 4.1–5.1 g/dl |
| BUN | 0.62 mg/dl | 8–20 mg/dl |
| Creatinine | 15.4 mg/dl | 0.65–1.07 mg/dl (M) |
| Na | 139 mEq/L | 138–145 mEq/L |
| K | 4.3 mEq/L | 3.6–4.8 mEq/L |
| T-Bil | 1.3 mg/dl | 0.2–1.2 mg/dl |
| ALP | 195 IU/L | 106–322 IU/L |
| AST | 17 IU/L | 13–33 IU/L |
| ALT | 16 IU/L | 8–42 IU/L |
| LDH | 218 IU/L | 124–222 IU/L |
| γ-GTP | 14 IU/L | 13–64 IU/L |
| CPK | 275 IU/L | 45–163 IU/L |
| BNP | <5.8 pg/ml | <18.4 pg/ml |
| CRP | 1.80 mg/dl | <0.3 mg/dl |
| KL-6 | 164.2 U/ml | <500 U/ml |
| SP-A | 32.1 ng/ml | <43.8 ng/ml |
| SP-D | 65.5 ng/ml | <110 ng/ml |
| ACE | 7.0 U/L (37℃) | 8.3–21.4 U/L |
| sIL-2R | 348.3 U/ml | 122–496 U/ml |
| BAL Recovery | 106/150 ml | ≥30 % |
| BAL TCC | 5.12 ×10^5 /ml | 1–2 ×10^5 /ml |
| BAL Neutrophils (%) | 6.0 % | <3 % |
| BAL Eosinophils (%) | 7.0 % | <1 % |
| BAL Lymphocytes (%) | 36.0 % | 10–15 % |
| BAL Macrophages (%) | 51.0 % | 85–95 % |
| BAL CD4/CD8 ratio | 3.04 | 1.0–3.5 |
| BAL Cytology | Class I | Class I (normal) |
| BAL Culture | Normal flora | — |
| Author (years) | Number | Age | Sex | Severity | Occupation | Steroid use | Mechanical ventilation | Outcome/prognosis |
| Matsuzaki Y (1978) [ | 1 | 54 | M | severe | boiler maintenance | Yes | No | survived |
| Horvath (1978) [ | 2 | 63 | M | NA | non-smoking daily farmer | Yes | No | survived |
| 19 | M | severe | employee of munitions | Yes | No | survived | ||
| Araki Y (1983) [*] | 1 | 48 | M | mild | automobile mechanic | Yes | No | survived |
| Tamura N (1985) [ | 1 | 50 | M | mild | iron works | No | No | survived |
| Akamine Y (1986) [*] | 1 | 52 | M | severe | metal refining | Yes | Yes | survived |
| Kitahara (1988) [ | 1 | 33 | M | severe | metal plating factory | Yes | No | survived |
| Iwami F (1988) [ | 1 | 20 | M | severe | electric welder | Yes | No | survived |
| Shiramine K (1989) [ | 1 | 52 | M | NA | daily farmer | Yes | Yes | survived |
| Hajela (1990) [ | 3 | 36 | M | severe | pulp-mill worker | No | Yes | died |
| 44 | M | severe | pulp-mill worker | No | Yes | died | ||
| 21 | M | severe | pulp-mill worker | No | No | died | ||
| Zwemer (1992) [ | 20 | NA | NA | 10 severe | NA | Yes(7 cases)/No(3 cases) | NA | 4 died/6 survived |
| NA | NA | 10 mild | NA | Yes(6 cases)/No(4 cases) | NA | 10 survived | ||
| Suzuki K (1993) [ | 6 | 41 | M | severe | ship repairing | Yes | No | survived |
| 60 | M | severe | ship repairing | Yes | No | survived | ||
| 48 | M | NA | ship repairing | NA | No | survived | ||
| 53 | M | NA | ship repairing | NA | No | survived | ||
| 39 | M | NA | ship repairing | NA | No | survived | ||
| 25 | M | mild | ship repairing | NA | No | survived | ||
| Shimatsu Y (1996) [ | 4 | 47 | M | severe | iron works | Yes | No | survived |
| 53 | M | severe | iron works | Yes | No | survived | ||
| 57 | M | mild | iron works | No | No | survived | ||
| 40 | M | mild | iron works | No | No | survived | ||
| Bur (1997) [ | 1 | 56 | M | severe | cleaning staff | Yes | Yes | died |
| Ikegami K (1998) [*] | 2 | NA | NA | mild | metal plating factory | NA | Yes | survived |
| NA | NA | NA | metal plating factory | NA | Yes | survived | ||
| Osakabe Y (2000) [ | 1 | 64 | M | severe | metal plating factory | Yes | Yes | survived |
| Kaneko Y (2006) [*] | 3 | 65 | M | severe | pump demolition work | Yes | Yes | survived |
| 51 | M | severe | pump demolition work | Yes | No | survived | ||
| 58 | M | mild | pump demolition work | Yes | No | survived | ||
| Kikuchi Y (2006) [*] | 1 | 62 | M | severe | diamond factory work | No | Yes | survived |
| Tanaka (2007) [ | 3 | 65 | M | severe | factory work | Yes | Yes | survived |
| 52 | M | severe | factory work | Yes | No | survived | ||
| 37 | F | severe | factory work | Yes | No | survived | ||
| Hino H (2009) [*] | 1 | 42 | M | NA | metalworking industry | Yes | Yes | survived |
| Ito T (2009) [*] | 1 | 68 | M | NA | metal plating work | Yes | No | survived |
| Kawaura T (2009) [*] | 1 | 21 | M | NA | shipbuilding industry | Yes | Yes | survived |
| Jayalakshmi (2009) [ | 3 | 30 | M | severe | cleaning staff | Yes | Yes | survived |
| 35 | M | mild | NA | Yes | Yes | survived | ||
| 28 | M | mild | NA | Yes | Yes | survived | ||
| Murphy (2010) [ | 1 | 66 | M | severe | tank cleaning | Yes | NA | died |
| Lee (2014) [ | 1 | 50 | M | mild | storekeeper | Yes | No | survived |
| Hayashi M (2014) [ | 1 | 43 | M | severe | metal plating factory | No | No | survived |
| Kido Y (2017) [ | 1 | 50 | M | severe | electroless nickel plating | Yes | No | survived |
| Present case (2018) | 1 | 42 | M | mild | chemical factory | No | No | survived |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCombustion and Detonation Processes · Cardiac Arrest and Resuscitation · Restraint-Related Deaths
Introduction
Nitrogen oxides (NOx) are toxic gases generated during nitric acid decomposition, industrial explosions or fires, and metal surface treatment or oxidation processes. In agriculture, NOx exposure has long been recognized as “silo-filler’s disease” [1,2].
Inhalation typically causes cough, dyspnea, and fever after a latent period of several hours up to 72 hours and may progress to acute respiratory distress syndrome (ARDS) in severe cases [3,4]. At the pathophysiological level, NOx generates reactive nitrogen species that damage the alveolar epithelium and capillary endothelium, leading to increased permeability and inflammation. Late complications, including bronchiolitis obliterans, organizing pneumonia, or pulmonary fibrosis, have also been reported [5].
Exposure scenarios are diverse, including industrial explosions, tank-cleaning accidents, and chemical reaction incidents [6-8]. More recently, a single severe case managed with veno-venous extracorporeal membrane oxygenation (VV-ECMO) has also been reported [9]. Radiologically, poorly defined centrilobular nodules and ground-glass opacities are characteristic findings [10].
Most previously reported cases were moderate-to-severe, and fatalities are not uncommon [11]. Corticosteroids are often administered [12], but consensus regarding optimal dose or duration is lacking. Furthermore, therapeutic strategies for mild cases remain uncertain, and spontaneous improvement without corticosteroid therapy has been observed [13,14].
Reports that correlate a mild clinical course with pathological findings are scarce. We present a case of mild NOx inhalation injury following an industrial explosion, in which we were able to demonstrate concordant radiologic and histopathologic features. This case may provide new insights into the diagnosis and management of mild NOx lung injury.
Case presentation
A 43-year-old male chemical plant worker, a non-smoker with no passive smoking exposure, presented after an industrial explosion in July 2018. At the time of the accident, a chemical reaction involving 67.5% nitric acid, 4-t-butylcyclohexanol, and ammonium metavanadate was ongoing. An orange-colored gas cloud was documented in on-site photographs. Without respiratory protection, he entered the site and developed malaise. Approximately three hours later, he was transported to the emergency department. Initial chest CT showed no abnormalities, and he was discharged home.
On days 1-2 (18-42 hours after exposure), cough and dyspnea worsened. Chest radiography revealed patchy bilateral opacities, and high-resolution computed tomography (HRCT) demonstrated poorly defined centrilobular ground-glass nodules in the lingular and lower lobes (Figure 1).
Radiographic and HRCT findings of nitrogen oxide inhalation injury(A) Chest radiograph on Day 0 showing no abnormalities. (B) Chest radiograph on Day 2 demonstrating new patchy bilateral opacities (arrows). (C) HRCT on Day 0 showing normal lung fields. (D) HRCT on Day 2 revealing poorly defined centrilobular ground-glass nodules in the lingula and bilateral lower lobes (circle).HRCT: high-resolution computed tomography
On admission, vital signs were stable (peripheral oxygen saturation (SpO₂) 98% on room air). Laboratory testing revealed leukocytosis with a left shift, elevated C-reactive protein (CRP), and mild increases in lactate dehydrogenase (LDH) and creatine phosphokinase (CPK), while angiotensin-converting enzyme (ACE) and soluble interleukin-2 receptor (sIL-2R) levels were within normal limits (Table 1).
Bronchoscopy revealed no endobronchial abnormalities. Bronchoalveolar lavage fluid was turbid and yellowish, with an increased cell count but negative cultures. Transbronchial lung biopsy demonstrated type II pneumocyte hyperplasia and alveolar wall thickening with fibrosis. Lesions were predominantly distributed around muscular pulmonary arteries, suggesting an airway-centered pattern. Intra-alveolar eosinophilic material consistent with fibrin deposition and early organization was also identified. Collectively, these findings supported a diagnosis of centriacinar-dominant mural alveolitis with focal fibrin deposition (Figure 2).
Histopathological findings from transbronchial lung biopsy(A, C) Alveolar septal thickening with type II pneumocyte hyperplasia adjacent to a muscular pulmonary arteriole (hematoxylin and eosin stain, ×200). (B) Thyroid transcription factor-1 (TTF-1) staining positive in hyperplastic alveolar epithelial cells. (D) Intra-alveolar eosinophilic material consistent with fibrin deposition and early organization.
The patient was managed supportively without corticosteroids. Oxygenation remained stable throughout hospitalization. Radiographic opacities gradually improved, and he was discharged on day 9. He subsequently developed transient depressive symptoms, which improved with psychiatric intervention. These psychiatric manifestations were interpreted as stress-related reactions to the industrial accident rather than direct toxic effects of NOx exposure. Follow-up CT scans on days 15 and 45 showed marked resolution (Figure 3).
Clinical course Follow-up CT on day 45 after exposure demonstrating resolution of the previously noted centrilobular ground-glass opacities.
Discussion
Inhalational injuries may be caused by gases such as chlorine, phosgene, sulfur dioxide, hydrogen sulfide, NOx, ozone, and ammonia [15]. Highly water-soluble gases (chlorine, ammonia, sulfur dioxide) tend to dissolve in the upper airway, whereas poorly soluble gases (phosgene, NOx, ozone) reach the lower respiratory tract and exert delayed effects [16]. Accordingly, highly soluble gases cause acute upper-airway symptoms immediately, while poorly soluble gases cause delayed onset symptoms after a latent period. In our patient, initial imaging was normal, but infiltrates appeared on day 2, consistent with the typical pathophysiology of NOx injury.
The most severe complication is ARDS, usually developing within 24 hours of high-concentration exposure [3]. Late complications, such as organizing pneumonia, bronchiolitis obliterans, and pulmonary fibrosis, have also been documented [5,13]. Thus, attention is required not only in the acute phase but also during long-term follow-up.
Previous reviews have summarized English-language cases, but numerous cases have also been reported in Japanese literature [12]. To contextualize our case within the broader spectrum of NOx inhalation injury, we reviewed 64 cases reported between 1978 and 2018, encompassing both international and domestic reports while excluding duplicates and abstracts (Table 2) [17-26].
Table 2: Reported cases of NOx inhalation injury, 1978–2018This table summarizes reported cases of nitrogen oxide (NOx) inhalation injury published in the English- and Japanese-language literature. Twenty-nine references were included; duplicates and abstracts were excluded. A severe case was defined as PaO₂ < 60 mmHg on room air or the requirement for supplemental oxygen at the initial assessment.Rows marked with an asterisk (*) indicate cases cited from secondary Japanese sources because the original pre-Internet articles were inaccessible.Secondary sources used for data abstraction:Araki Y (1983), Akamine Y (1986): Data abstracted from secondary source: Osakabe Y, et al. [25]Ikegami K (1998), Kaneko Y (2006), Kikuchi Y (2006), Hino H (2009), Ito T (2009), Kawaura T (2009): Data abstracted from secondary source: Hayashi M, et al. [26]Original reports are cited whenever accessible.WBC, white blood cell count; RBC, red blood cell count; Hb, hemoglobin; Hct, hematocrit; Plt, platelet count; PSL, prednisolone; mPSL, methylprednisolone; ECMO, extracorporeal membrane oxygenation; NA, not available
In total, 64 cases of NOx inhalation injury have been reported, with a mean age of 46.3 years (based on 42 cases with available demographic data). Severe cases, defined as those with PaO₂ <60 mmHg on room air or requiring supplemental oxygen, accounted for 34 (53.1%), whereas 21 (32.8%) were mild and 9 (14.1%) were unspecified. Overall, 55 patients (85.9%) survived and 9 (14.1%) died.
Our patient thus represents a rare category of steroid-free survival. Importantly, most previously reported survivors received corticosteroid therapy, whereas our case demonstrated full recovery without it, reinforcing the potential for conservative management in carefully monitored mild cases. Compared with previously reported severe or fatal cases, our patient presented with a milder course characterized by preserved oxygenation, radiologic-pathologic correlation, and recovery without corticosteroid therapy. This contrast underscores the clinical spectrum of NOx injury and highlights the importance of individualized management strategies.
More recent reports underscore the broad severity spectrum: dose-dependent severe cases after NO₂ explosion [9], delayed onset after occupational exposure [27], histologically confirmed secondary organizing pneumonia [28], and VV-ECMO-supported survival in severe ARDS [9,11,29]. Additional case reports have described severe lung injury and acute respiratory distress syndrome following nitric acid fume exposure [7,8]. These highlight both the life-threatening potential and the variability of NOx injury. Our case lies at the mild end of this spectrum, emphasizing the need for individualized management.
While steroids are frequently recommended, their optimal regimen remains uncertain. Some authors suggest courses of ≥4 weeks [12], yet mild cases may improve spontaneously. Lee described late-onset bronchiolitis obliterans after nitric acid exposure [5], though whether early steroids would have prevented this remains unclear. Our case suggests that in carefully monitored mild cases with preserved oxygenation, conservative management without steroids may be a reasonable option.
Imaging-pathology correlation is also noteworthy. Tanaka reported centrilobular ground-glass nodules, interlobular septal thickening, and absence of lymphadenopathy as typical HRCT features [10]. Our patient demonstrated similar CT findings, with histology showing centriacinar-dominant mural alveolitis with fibrin, closely matching radiology. Such concordance in a mild case is rarely documented and enhances understanding of NOx pathology.
Conclusions
This case illustrates mild NOx inhalation injury following an industrial explosion, with radiologic and pathologic concordance of centriacinar-dominant mural alveolitis. It is among the very few steroid-free survivors reported. Clinically, this underscores that mild cases may resolve spontaneously, yet vigilance is essential due to potential delayed complications such as bronchiolitis obliterans and pulmonary fibrosis. Long-term follow-up is indispensable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silo-filler's disease: nitrogen dioxide-induced lung injury. Long-term follow-up and review of the literature Ann Intern Med Ramirez J Dowell AR 569576741971 https://doi.org/10.7326/0003-4819-74-4-569557315810.7326/0003-4819-74-4-569 · doi ↗ · pubmed ↗
- 2Silo filler's disease Chest Scott EG Hunt WB Jr 701706631973 https://doi.org/10.1378/chest.63.5.701470362310.1378/chest.63.5.701 · doi ↗ · pubmed ↗
- 3Fatal pulmonary edema due to nitric acid fume inhalation in three pulp-mill workers Chest Hajela R Janigan DT Landrigan PL Boudreau SF Sebastian S 487489971990 https://doi.org/10.1378/chest.97.2.487215351010.1378/chest.97.2.487 · doi ↗ · pubmed ↗
- 4Fatal pulmonary edema after acute occupational exposure to nitric acid J Emerg Med Murphy CM Akbarnia H Rose SR 3943392010 https://doi.org/10.1016/j.jemermed.2008.03.0111884238310.1016/j.jemermed.2008.03.011 · doi ↗ · pubmed ↗
- 5Bronchiolitis obliterans organizing pneumonia following nitric acid fume exposure Occup Med (Lond) Lee LT Ho CH Putti TC 136138642014 https://doi.org/10.1186/1745-6673-9-82431904910.1093/occmed/kqt 147 · doi ↗ · pubmed ↗
- 6Dose-dependent pulmonary injury following nitrogen dioxide inhalation from Kinepak™ detonation J Emerg Med Perez-Lauterbach D Nahum R Ahmad H Topeff JM Dossick D Cole JB Arens AM 177180572019 https://doi.org/10.1016/j.jemermed.2019.03.0283106084210.1016/j.jemermed.2019.03.028 · doi ↗ · pubmed ↗
- 7Severe lung injury following inhalation of nitric acid fumes Indian J Crit Care Med Pillai LV Ambike DP Husainy S Vishwasrao S Pataskar S Kulkarni SD 24424792005 https://doi.org/10.4103/0972-5229.19766
- 8Acute lung injury following exposure to nitric acid Lung India Jayalakshmi TK Shah S Lobo I Uppe A Mehta A 149151262009 https://doi.org/10.4103/0970-2113.563542053200210.4103/0970-2113.56354 PMC 2876705 · doi ↗ · pubmed ↗