Management of Diabetic Kidney Disease With Persistent Hypotension: A Case of Lifestyle-Driven Renal Recovery
Sungmin Song, Okoro Obioha, Yoobin Kang

TL;DR
A woman with diabetes and low blood pressure improved kidney function through lifestyle changes when standard treatments were unsafe.
Contribution
Highlights a novel lifestyle-driven approach for managing diabetic kidney disease in patients with persistent hypotension.
Findings
Renal function improved from eGFR 55 to 69 over two years with lifestyle interventions.
Stable kidney function was maintained with continued absence of albuminuria.
Weight reduction and glycemic control correlated with eGFR recovery in a hypotensive T2DM patient.
Abstract
Diabetic kidney disease (DKD) is typically accompanied by hypertension, which enables guideline-directed renoprotective therapy. We describe a 61-year-old woman with type 2 diabetes mellitus (T2DM) and persistent hypotension (≈92/55-98/65 mmHg) without albuminuria, in whom angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs) and sodium-glucose cotransporter-2 (SGLT2) inhibitors were deemed unsafe due to baseline low blood pressure. Management, therefore, emphasized non-pharmacologic measures, tight glycemic control, weight reduction (~10 lb), hydration, and avoidance of nephrotoxins in a resource-limited setting. Renal function improved from an eGFR of 55 mL/min/1.73 m² (2023) to 69 (2024) and stabilized at 67.2 (2025) with HbA1c 6.3-6.6% and continued lack of albuminuria; neurologic and ophthalmic diabetic manifestations remained stable. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
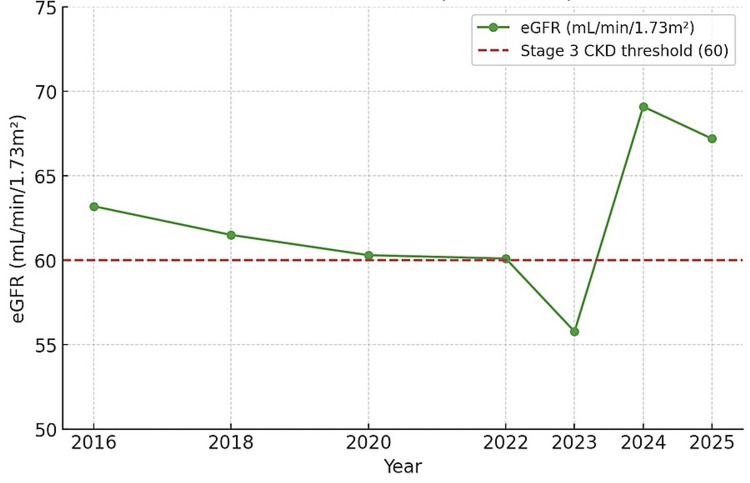 Figure 1
Figure 1| Year | HbA1c (%) | Fasting Glucose (mg/dL) | eGFR (mL/min/1.73m²) | Creatinine | Albuminuria | BMI/Weight | Notes |
| 2016 | 7.5 | 262 | 63.2 | Normal | Negative | 27.8 | Dx T2DM, poor adherence |
| 2018 | 7.8 | 271 | 61.5 | Normal | Negative | 28.2 | Chronic cough |
| 2020 | 7.6 | 265 | 60.3 | Normal | Negative | 28.3 | Poor adherence |
| 2022 | 7.4 | 244 | 60.1 | Normal | Negative | 27.7 | Neuropathy onset |
| 2023 | 7.2 | 254 | 55.78 | Normal | Negative | 27.4 | Gastritis, weight loss |
| 2024 | 6.5 | 144 | 69.1 | Normal | Negative | 24.4 | Improved control |
| 2025 | 6.3 | 120 | 67.39 | Normal | Negative | 24.2 | Stable |
| Year | Avg SBP (mmHg) | Avg DBP (mmHg) | Notes |
| 2016 | 99 | 67 | Initial diagnosis |
| 2018 | 97 | 65 | Poor adherence |
| 2020 | 98 | 66 | CKD borderline |
| 2022 | 96 | 64 | Neuropathy onset |
| 2023 | 95 | 64 | Stage 3 CKD; gastritis, weight loss |
| 2024 | 95 | 67 | Persistently hypotensive |
| 2025 | 96 | 66 | Stable |
| Test | Result | Reference range | Interpretation |
| HbA1c | 6.30% | 4.8 – 5.9 % | Mildly elevated |
| Glucose (fasting) | 120 mg/dL | 70 – 100 mg/dL | Elevated |
| eGFR (MDRD) | 67.39 mL/min/1.73m² | >60 | CKD stage 2 |
| BUN | 12 mg/dL | 8 – 20 mg/dL | Normal |
| Creatinine | 0.91 mg/dL | 0.6 – 1.2 mg/dL | Normal |
| Na | 143 mEq/L | 135 – 147 | Normal |
| K | 4.2 mEq/L | 3.5 – 5.1 | Normal |
| Cl | 106 mEq/L | 95 – 110 | Normal |
| Calcium | 9.8 mg/dL | 8.5 – 10.5 | Normal |
| Albumin | 4.4 g/dL | 3.5 – 5.5 | Normal |
| AST/ALT | 23/16 IU/L | <40 | Normal |
| Total bilirubin | 0.2 mg/dL | 0.3 – 1.2 | Slightly low |
| Lipids | LDL 62 / HDL 57 / TG 97 | LDL goal <100 | Well-controlled |
| CBC | Hb 12.6 g/dL / WBC 4.4 x10⁶/µL / Plt 223 | Within normal limits | Normal |
| Urinalysis: Negative for protein, glucose, blood; SG 1.005 (dilute but no proteinuria). | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies · Blood Pressure and Hypertension Studies · Cardiovascular Syncope and Autonomic Disorders
Introduction
Diabetic kidney disease (DKD) is the leading global cause of chronic kidney disease and end-stage kidney disease, contributing substantially to cardiovascular morbidity and mortality [1], and patients with DKD experience an elevated risk of premature death compared with diabetes alone [2]. Hypertension is the predominant hemodynamic phenotype in DKD, and the presence of albuminuria and/or reduced eGFR identifies individuals at greater severity and risk of progression [3], whereas a non-albuminuric phenotype is increasingly recognized and has been associated with adverse outcomes despite the absence of proteinuria [4]. Guidelines emphasize renin-angiotensin system blockade with ACE inhibitors or ARBs once albuminuria is present or eGFR falls below 60 mL/min/1.73 m² [5], yet controversies in chronic kidney disease (CKD) blood pressure management persist, particularly when hypotension complicates therapeutic decision-making [6]. The large hypertension guidelines further caution that aggressive pharmacologic lowering may be unsafe in patients with already low baseline blood pressure [7]. From a pathophysiologic standpoint, diabetes-related autonomic neuropathy with impaired baroreflexes can contribute to chronic hypotension, narrowing the therapeutic window for renoprotective agents [8]. In such cases, especially when albuminuria is absent, individualized care emphasizing glycemic optimization, lifestyle measures, and nephrotoxin avoidance becomes central, as highlighted in the present case of a woman with DKD and chronic hypotension without albuminuria who could not receive standard agents yet experienced renal improvement from stage 3 to stage 2, illustrating a real-world gap in current recommendations.
Case presentation
A 61-year-old Asian woman, a never-smoker, who denies alcohol use, had long-standing T2DM. Family history included maternal hypotension and paternal T2DM with laryngeal cancer. She lived in a rural industrial area with limited medical oversight and long-standing misconceptions that low blood pressure (BP) was protective, contributing to poor adherence. At baseline in 2016, renal function was preserved with an eGFR of 63 mL/min/1.73m² and normal serum creatinine. Glycated hemoglobin (HbA1c) was 7.5%, and serum electrolytes (sodium, potassium, chloride, calcium, and bicarbonate) were consistently within normal limits, thereby excluding secondary metabolic or endocrine causes of hypotension. In particular, the absence of electrolyte derangements ruled out adrenal insufficiency, thyroid dysfunction, and renal tubular acidosis as contributors. The chronic course of low blood pressure, absence of systemic symptoms, and positive maternal history of lifelong hypotension suggested a constitutional predisposition. Furthermore, in the context of long-standing diabetes, autonomic dysfunction with impaired baroreflexes was considered a likely mechanism, accounting for the patient’s persistent low BP despite otherwise stable metabolic status (Table 1).
Table 1: Laboratory trends (2016–2025). Albuminuria assessed by dipstick/ACR; “negative” indicates ACR <30 mg/g or negative dipstick.eGFR: Estimated glomerular filtration rate, BMI: Body mass index
T2DM was recognized in 2016 (glucose >250 mg/dL). Metformin was prescribed at that time, but adherence was poor and limited to episodes of severe hyperglycemia. Baseline eGFR was 63.2 mL/min/1.73m² with elevated HbA1c (7.6); BP averaged approximately 90/60 mmHg. From 2018 to 2021, she presented sporadically with hyperglycemia. Investigations for chronic cough were unrevealing, and treatment adherence remained poor.
In 2022, she developed peripheral neuropathic symptoms, including facial tingling and distal sensory changes, which improved over three months with better glycemic control. By 2023, she developed diabetic gastritis, presenting with poor appetite and weight loss. Renal function declined to eGFR 55.7 mL/min/1.73m² (stage 3 CKD). At that point, she was counseled on disease progression and began taking metformin consistently for the first time (Figure 1). Given persistent hypotension and absence of albuminuria, angiotensin-converting enzyme inhibitor (ACEi) or ARB therapy was not initiated. Management, therefore, focused on glycemic control and lifestyle measures.
Longitudinal eGFR values abstracted from clinic records (2016–2025).The image is created by the author.eGFR: Estimated glomerular filtration rate
In early 2024, her diabetic gastritis worsened, further reducing food intake and indirectly improving glycemic control through sustained weight loss. Endoscopic evaluation confirmed chronic gastritis without malignancy. Omeprazole was initiated at that time, leading to symptomatic improvement by mid-2024. Laboratory evaluation revealed renal recovery: eGFR 69 mL/min/1.73m² (stage 2 CKD), HbA1c 6.5%, normal creatinine, and absent albuminuria. BP remained between 88/55 and 95/65 mmHg (Table 2).
By mid-2025, she remained clinically stable with sustained metformin use, omeprazole therapy, and dietary adherence. At her most recent follow-up in June 2025, her weight was 64 kg (body mass index [BMI], approximately 24.7). She continued to report persistent polyuria without incontinence, distal sensory decrease without progression, and preserved vision despite vitreous floaters. Laboratory evaluation demonstrated stable renal function with eGFR 67 mL/min/1.73m², serum creatinine 0.91 mg/dL, and blood urea nitrogen (BUN) 12 mg/dL. Electrolytes were normal (sodium 143 mEq/L, potassium 4.2 mEq/L, chloride 106 mEq/L, calcium 9.8 mg/dL), as were liver function tests (aspartate aminotransferase (AST) 23 U/L, alanine aminotransferase (ALT) 16 U/L, albumin 4.4 g/dL). HbA1c was 6.3% with fasting glucose 120 mg/dL, while the lipid panel showed low-density lipoprotein (LDL) 62 mg/dL, high-density lipoprotein (HDL) 57 mg/dL, and triglycerides 97 mg/dL. Urinalysis remained negative for proteinuria or hematuria. Collectively, these findings confirmed stable stage 2 CKD with preserved electrolyte balance despite persistent hypotension (Table 3).
Yearly averages in Tables 1-3 and Figures 1 were derived from 2-3 outpatient clinic visits per year, with values abstracted directly from the patient’s chart. These have been summarized into aggregate tables for clarity. Original clinic notes are available to the editorial office upon request.
Discussion
Clinical dilemma
Persistent hypotension in T2DM is rarely described, whereas hypertension predominates. Most patients with T2DM and CKD develop hypertension, and ACEi or ARB therapy is recommended, particularly at eGFR <60 or with albuminuria. In this patient, T2DM was first recognized in 2016 with glucose >250 mg/dL. In 2022, she developed peripheral neuropathic symptoms, which improved with better glycemic control. By 2023, she had developed diabetic gastritis with weight loss. Her renal function declined to an eGFR of 55 mL/min/1.73m² in 2023, ordinarily warranting ACEi or ARB therapy, but chronic hypotension contraindicated their use, and the absence of albuminuria further reduced the rationale. Management, therefore, focused on intensive metabolic control and lifestyle modification, leading to partial renal recovery (eGFR 69 in 2024 and 67 in 2025), indicating the potential for renal stabilization through non-pharmacologic measures when guideline-directed therapy cannot be applied.
Possible mechanisms
Several mechanisms may explain this patient’s persistent hypotension. From the clinical data, serum electrolytes (sodium, potassium, chloride, calcium, and bicarbonate) remained consistently within normal limits, effectively excluding metabolic or endocrine causes such as adrenal insufficiency, thyroid dysfunction, and renal tubular acidosis. The chronic, asymptomatic low BP course and maternal history of lifelong hypotension further suggest a constitutional predisposition. In the context of long-standing diabetes, autonomic dysfunction with impaired baroreflexes is a plausible mechanism, supported by evidence that diabetic autonomic neuropathy can disrupt cardiovascular autonomic regulation and cause hypotension [9]. Cardiac autonomic neuropathy (CAN), a subset of diabetic autonomic neuropathy, is well described in the literature and may manifest as orthostatic hypotension, resting low BP, and impaired heart rate variability [10].
Therapeutic considerations
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are a cornerstone in diabetic CKD and reduce kidney disease progression [11,12]. However, they also lower BP modestly by ~2-4 mmHg, which may be undesirable in baseline hypotension [13]. Glucagon-like peptide-1 (GLP-1) receptor agonists reduce major cardiovascular events [14] and, in meta-analyses, improve cardiovascular mortality and renal outcomes [15], with clinically meaningful glycemic and weight benefits that appear pronounced in Asian populations. Although not used in this case, GLP-1 receptor agonists remain a reasonable future option, with clinically meaningful glycemic and weight benefits that appear especially pronounced in Asian populations [16].
Management and literature context
In this patient, non-pharmacologic strategies were not merely supportive but appeared central to renal recovery. Sustained weight loss (~10 lb), strict dietary adherence, and consistent glycemic control coincided with an improvement in eGFR from 55 to 69 mL/min/1.73m², which then stabilized over two years. While causality cannot be definitively proven, recent studies suggest that lifestyle interventions, such as weight reduction, dietary optimization, and improved glycemic management, can attenuate CKD progression and, in select cases, improve renal indices independent of pharmacotherapy. This underscores the significance of lifestyle-driven management as a pragmatic alternative when guideline-directed renoprotective agents are contraindicated, particularly in hypotensive, non-albuminuric DKD phenotypes [17].
Conclusions
In summary, this case highlights the management challenges of T2DM complicated by CKD and persistent hypotension. At an eGFR of 55 mL/min/1.73m² in 2023, ACEi or ARB therapy would usually be indicated, but chronic hypotension and absent albuminuria made renoprotective pharmacotherapy unsafe. With lifestyle modification, strict glycemic control, and patient education, renal function improved to stage 2 CKD and remained stable through 2025. The case underscores the need for individualized care and clearer guidance for hypotensive diabetic CKD phenotypes. This case further highlights the correlation between glycemic control, as measured by HbA1c, and kidney function, as measured by eGFR, even when BP is not elevated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease Kidney Int KDIGO Diabetes Work Group 0102202210.1016/j.kint.2022.06.00836272764 · doi ↗ · pubmed ↗
- 2Introduction and methodology: standards of care in diabetes-2024 Diabetes Care American Diabetes Association Professional Practice Committee 04472024
- 3Albuminuria is an appropriate therapeutic target in patients with CKD: the pro view Clin J Am Soc Nephrol Gansevoort TR Heerspink LJH 1079108810(6)2015 https://pubmed.ncbi.nlm.nih.gov/25887073/2588707310.2215/CJN.11511114 PMC 4455219 · doi ↗ · pubmed ↗
- 4Non-albuminuric diabetic kidney disease phenotype: beyond albuminuriatouch REV Endocrinol D'Marco L Guerra-Torres X Viejo I 1021051820223669488910.17925/EE.2022.18.2.102PMC 9835813 · doi ↗ · pubmed ↗
- 5Kidney disease and increased mortality risk in type 2 diabetes J Am Soc Nephrol Afkarian M Sachs MC Kestenbaum B 3023082420132336231410.1681/ASN.2012070718 PMC 3559486 · doi ↗ · pubmed ↗
- 6Blood pressure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference Kidney Int Cheung AK Chang TI Cushman WC 102710369520193101047810.1016/j.kint.2018.12.025 · doi ↗ · pubmed ↗
- 72017 ACC/AHA/AAPA/ABC/ACPM/AGS/A Ph A/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines Hypertension Whelton PK Carey RM Aronow WS 071201810.1161/HYP.000000000000006529133356 · doi ↗ · pubmed ↗
- 8Cardiac autonomic neuropathy in diabetes mellitus Methodist Debakey Cardiovasc J Agashe S Petak S 2512561420183078801010.14797/mdcj-14-4-251PMC 6369622 · doi ↗ · pubmed ↗