Effect of disappearing liver metastases during pre-ablation chemotherapy on the prognosis of percutaneous microwave ablation in synchronous colorectal liver metastases patients
Limei Chen, Jingwen Zhou, Rui Cui, Si Qin, Yao Chen, Yimin Wang, Guangjian Liu

TL;DR
This study shows that colorectal liver metastases that disappear during chemotherapy before microwave ablation are linked to worse liver cancer control, even though overall survival is not affected.
Contribution
The study identifies that radiographic disappearance of liver metastases during chemotherapy is a risk factor for intrahepatic recurrence after microwave ablation.
Findings
Patients with disappearing liver metastases had significantly lower intrahepatic progression-free survival compared to those without.
Disappearing metastases were found to be a risk factor for poor intrahepatic progression-free survival in multivariable analysis.
Overall survival was not significantly different between patients with and without disappearing metastases.
Abstract
Disappearing colorectal liver metastases (DLM) frequently occur during chemotherapy. However, DLM is not equivalent to pathologically complete response. This study aimed to investigate the effect of radiographic DLM on microwave ablation (MWA) in patients with synchronous colorectal liver metastases (CRLM). A retrospective review was performed for patients who accepted MWA following pre-ablation chemotherapy from January 2014 to December 2021. DLM was defined as undetectable tumors on pre-ablation contrast-enhanced imagings compared to the initial ones. Overall survival (OS) and intrahepatic progression-free survival (ihPFS) were analyzed and compared between patients with and without DLM. Univariate and multivariate cox regression were used to identify risk factors for OS and ihPFS. A propensity score matching (PSM) analysis was used to balance the patient demographics. Sixty-eight…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
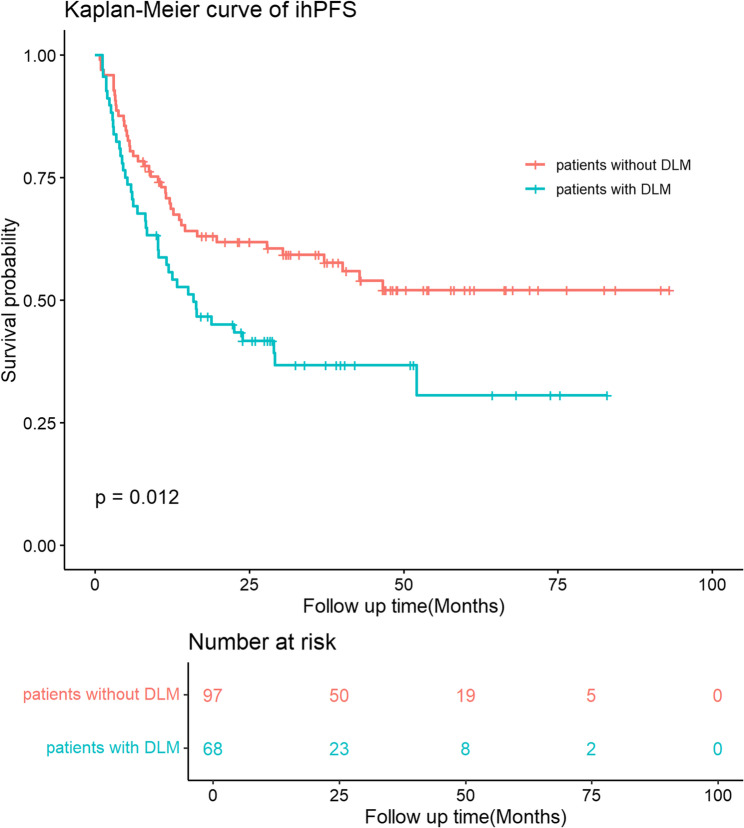 Figure 1
Figure 1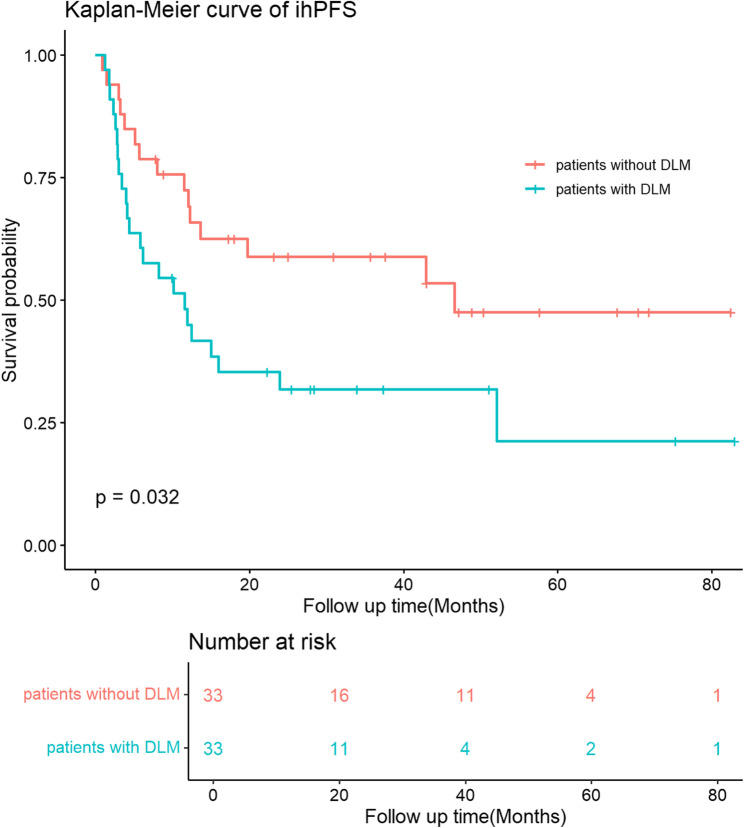 Figure 2
Figure 2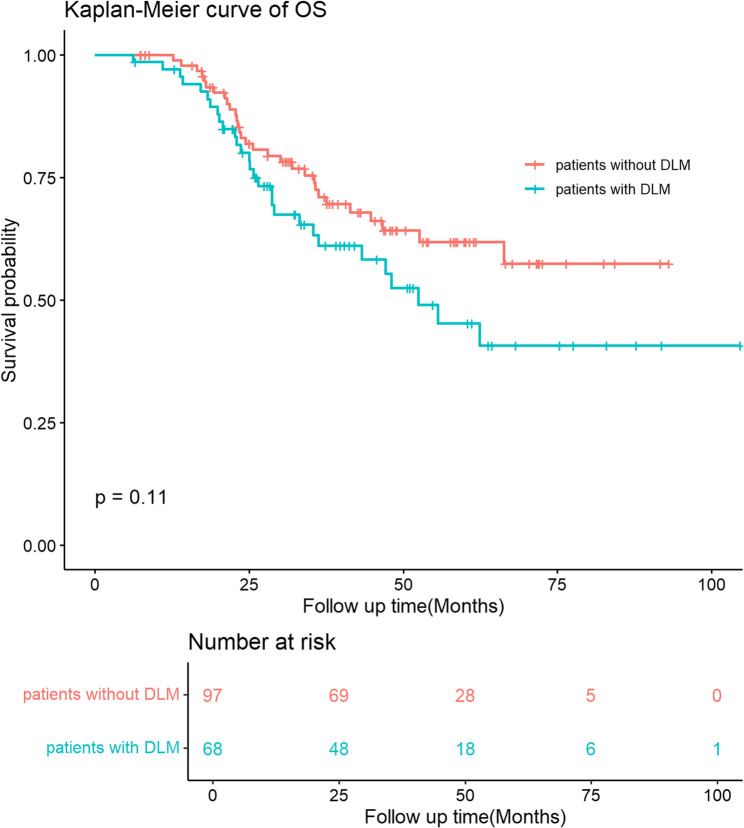 Figure 3
Figure 3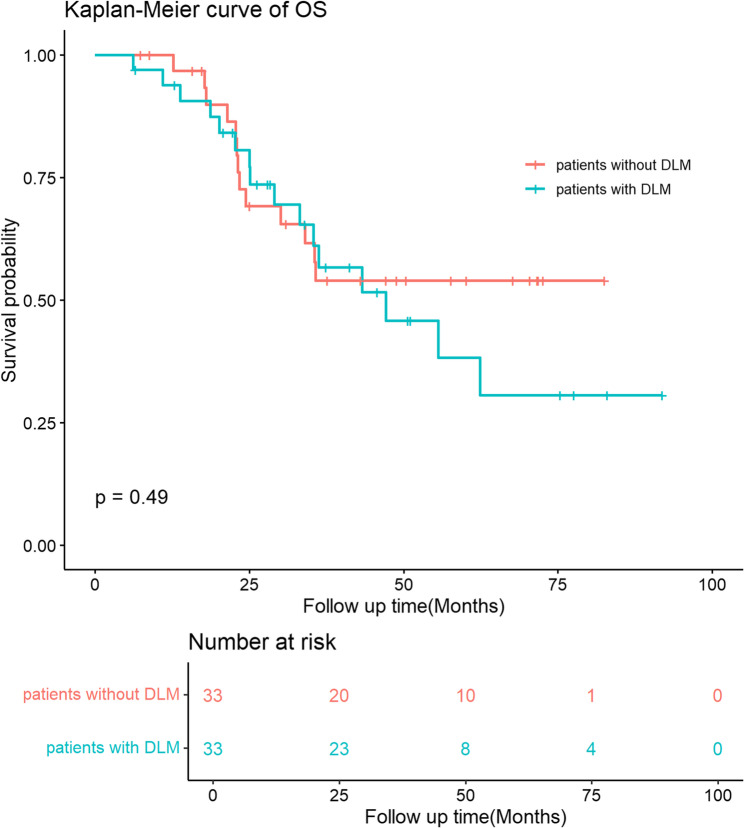 Figure 4
Figure 4- —https://doi.org/10.13039/501100001809National Natural Science Foundation of China
- —Guangdong Province Basic and Applied Basic Research Foundation Enterprise Joint Fund (Public Health and Pharmaceutical Health Field) – Key Projects
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Intraperitoneal and Appendiceal Malignancies · Gastric Cancer Management and Outcomes
Introduction
Synchronous colorectal liver metastases (sCRLM) are identified concurrently with the diagnosis of colorectal cancer, occurring in approximately 20% of patients with this malignancy [1]. The presence of sCRLM is associated with a more aggressive cancer biology and is generally linked to poorer survival outcomes compared to metachronous metastases [2, 3].
Currently, systemic chemotherapy is extensively administered to patients with sCRLM. For resectable sCRLM, up-front surgery remains the mainstream treatment, but chemotherapy before surgery has markedly extended disease survival in these patients [4, 5], especially for those with high tumor burden and risk of poor prognosis. For unresectable sCRLM, preoperative chemotherapy is offered with the goal of downsizing tumors to allow local treatment [6–8]. However, with the advance of chemotherapy, the phenomenon of disappearing colorectal liver metastases (DLM) is becoming increasingly common. Radiographic DLM is reported in 7%−48% of patients receiving chemotherapy [9], yet it does not necessarily equal to a pathologically complete remission. Studies indicated that approximately 15% to 61% of the radiographic DLM showed pathologically viable cancer cells or recurred during the follow-up [9–12].
Imaging-guided thermal ablation is widely used to treat patients with liver malignant tumors for over 20 years, with the advantage of minimal invasiveness and repeatable nature. The combined use of chemotherapy and local treatment significantly improve recurrence-free survival as well as overall survival (OS) compared to those who received chemotherapy alone [13, 14]. However, the optimal timing for neoadjuvant chemotherapy and local treatment remains an undetermined problem. Had radiographic DLM occurs during chemotherapy, percutaneous thermal ablation is limited by the resolution of imaging modalities in eliminating the micro metastases at DLM sites. Therefore, once DLM occurs during chemotherapy and is left untreated due to percutaneous approach, these patients may lose the opportunity of achieving no evidence of disease (NED).
The impact of DLM on the outcomes of MWA for patients with sCRLM remains inadequately understood. We hypothesized that DLM could negatively impact the prognosis of MWA, leading to different survival outcomes for patients with DLM compared to those without. The aim of this study was to determine the effect of DLM on MWA by comparing survival outcome of sCRLM patients with or without DLM.
Methods and materials
Study design
This retrospective study was endorsed by the Institution Ethics Committee (approved number: 2024ZSLYEC-171) and adhered to the Declaration of Helsinki and the International Conference on Harmonization-Good Clinical Practice. This retrospective study examined consecutive patients treated for synchronous CRLM at a high-volume colorectal cancer center from January 2014 to December 2021. Inclusion criteria included: 1. Diagnosis of sCRLM confirmed by at least two contrast imaging methods or liver biopsy; 2.Pathologically confirmed colorectal cancer in which the primary tumors were radically resected; 3. Patients who received pre-ablative chemotherapy without disease progression; 4. Patients who had fewer than five tumors and a maximum tumor size of 3 cm who received technically successful ultrasound-guided MWA following pre-ablative chemotherapy; 5. Availability of contrast imaging data both prior and following pre-ablative chemotherapy; 6. Regular follow-up with contrast imaging for a minimum of six months. Exclusion criteria were: (1) Presence of other primary malignant tumors; (2) Concurrent hepatectomy or transarterial chemoembolization with MWA; (3) Occurrence of new CRLM during pre-ablative chemotherapy.
According to the CRLM visualization on pre- and post- chemotherapy, patients were classified into those with DLM and without DLM. DLM was defined as the absence of tumors on pre-MWA contrast-enhanced imaging (CECT n = 125, CEMRI n = 53) compared to the initial ones. The survival outcomes and recurrence patterns were compared between patients with DLM and those without. Recurrences were categorized as either in situ or de novo. In situ recurrence included local tumor progression (LTP) and recurrence at the DLM site. LTP was identified by the presence of a hyper-enhanced nodule with washout at the edge of the ablated zone after complete ablation, as seen in contrast-enhanced imaging studies. DLM site recurrence was characterized by the presence of metastases visible on CECT or CEMRI prior to chemotherapy that subsequently disappeared following chemotherapy. De novo recurrence referred to new tumors appearing at locations distant from the initial site of metastases, identified on pre-chemotherapy imaging scans. Intrahepatic progression-free survival (ihPFS) was defined as the duration from the date of MWA to intrahepatic tumor recurrence or the last follow-up. Overall survival (OS) was defined as the duration from the date of MWA to the date of death or the last follow-up.
Treatment strategy
All patients underwent chemotherapy prior to percutaneous US-guided MWA, with the chemotherapy regimens and cycles determined by the oncologists at our hospital. After chemotherapy, a multidisciplinary team—including an experienced medical oncologist, radiation oncologist, gastrointestinal surgeon, hepatobiliary surgeon, radiologist, interventionist, and pathologist—evaluated the feasibility of ablating sCRLM. Patients with a maximum of five tumors and tumor size no larger than 3 cm, were eligible for percutaneous US-guided MWA.
Before performing MWA, ultrasound examination with convex probe was performed to detect CRLM initially. We read the pre- and post-chemotherapy CECT or CEMRI for reference. Once lesions on pre-chemotherapy could not be detected by ultrasound scanning with convex probe, high-frequency ultrasound and contrast enhanced ultrasound (CEUS) using linear probe were combined with conventional convex probe US and CEUS to maximize the detection of tumors after chemotherapy [15]. All identified lesions were treated with MWA, while DLMs were unablated and no anatomical orientated approach was applied. The MWA procedures utilized a 2450-MHz microwave ablation system (KY2000; Nanjing Kangyou Biological Energy Co. Ltd, Nanjing, China), as previously detailed by our center [16, 17]. In brief, a 15 G dual-channel antenna was positioned 5 mm beyond the deep margin of the lesion under ultrasound guidance (LOGIQ E9; GE Healthcare, Milwaukee, WI, USA). The ablation strategies depended on the size of the lesions: a single antenna was used for lesions ≤ 2.0 cm, while 1–2 antennas were applied for lesions measuring 2.0–3.0 cm, with energy output adjusted between 45 and 60 W for 5–15 min. Throughout the procedure, the temperature of each antenna was kept below 40 °C by circulating cold saline. The needle track was also ablated to reduce the risk of bleeding and tumor seeding. Each procedure was conducted by the same interventionist, who has over 20 years of experience in liver cancer ablation.
Since all MWA procedures in the recruited patients were performed via a percutaneous approach, simultaneous open or laparoscopic MWA during colorectal cancer resection was not conducted. In this study, three timing strategies for MWA and colorectal resection in sCRLM patients were defined. The concurrent strategy was characterized by an interval of ≤ 14 days between MWA treatment of sCRLM and resection of the primary tumor. The bowel-first approach involved initial resection of the primary lesion followed by liver ablation after an interval of > 14 days. Conversely, the liver-first approach entailed MWA of liver metastases followed by resection of the primary tumor after an interval exceeding 14 days.
Follow-up
CEUS was performed 30 min and 24 h after MWA, followed by CEUS and CECT/MRI one-month post-MWA. Recurrence and survival data were then monitored using contrast-enhanced imaging techniques every three months for the first six months and every six months thereafter for follow-up according to the standard care protocol for CRLM patients of our center.
Statistical analysis
Categorical variables were presented as counts (percentages), while continuous variables were summarized as median (1st quartile, 3rd quartile) or mean ± standard deviation. The chi-squared test was employed to compare categorical data, and the T-test was utilized for the comparison of continuous data. Survival outcomes, including ihPFS and OS, were analyzed using Kaplan–Meier methods and compared with the log-rank test. Univariate and multivariate Cox regression analyses were conducted to identify significant factors associated with ihPFS and OS. Variables with a p-value less than 0.2 in univariate analysis were considered eligible for inclusion in the multivariable Cox regression. Multivariable Cox proportional hazards regression was then performed to obtain adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for ihPFS and OS. To reduce the impact of baseline differences in demographic, the 1:1 propensity score matching (PSM) method was used to match the patients with and without DLM. The PSM method confirms background differences by standardized differences. A p-value of less than 0.05 was deemed statistically significant. Statistical analyses were conducted using IBM SPSS Statistics version 25.0 (International Business Machines Corporation, New York) and R Statistical Software version 4.3 (Foundation for Statistical Computing, Vienna, Austria).
Results
Patient demographics
A total of 165 patients with sCRLM who met the inclusion criteria were included in this study. After pre-ablative chemotherapy, 68 patients had at least one DLM and 97 showed no DLM. Of 165 patients, 32 (19.4%) underwent a liver-first approach, 69 (41.8%) a concurrent approach and 64 (38.8%) a bowel-first approach. The patient demographics of patients with and without DLM were summarized in Table 1. The median follow-up period was 48.2 months (95% CI: 41.9–54.5 months). The median age in patients with and without DLM were 60 (53, 65) and 58 (52, 64), respectively. Patients with more than two sCRLM at the time of diagnosis and more than two sCRLM at the time of MWA were found more prevalent in patients with DLM than those without DLM (p < 0.001 and p = 0.010, respectively). No significant differences were observed in other factors between the two groups (all p > 0.050).
Table 1. Demographics of patients with and without DLM before propensity score matchingCharactersPatients without DLM (n = 97)Patients with DLM (n = 68)p-valueAge,** median(quartile)**58 (52,64)60(53,65)0.180 Gender (%) 1.000 Female26.8% (26/97)27.9% (19/68) Male73.2% (71)72.1% (49/68) Plasma CEA (%) 0.282 ≤10 µg/L77.3% (75/97)85.3% (58/68) >10 µg/L22.7% (22/97)14.7% (10/68) Primary cancer
Location (%) 1.000 Left88.7% (86/97)88.2% (60/68) Right11.3% (11/97)11.8% (8/68) Pathologic tumor category (%) 1.000 ypT0 – ypT382.5% (80/97)82.4% (56/68) ypT417.5% (17/97)17.7% (12/68) Pathologic lymphatic spread (%) 0.317 N030.9% (30/97)39.7% (27/68) N1 or N269.1% (67/97)60.3% (41/68) Extrahepatic metastasis (%) 0.522 No76.3% (74/97)70.6% (48/68) Yes23.7% (23/97)29.4% (20/68) Initial CRLM
Number (%)
< 0.001 ≤ 277.3% (75/97)16.2% (11/68) > 222.7% (22/97)83.8% (57/68) Maximum diameter (%) 0.885 ≤ 3 cm74.2% (72/97)76.5% (52/68) > 3 cm25.8% (25/97)23.5% (16/68) Ablated CRLM
Number (%)
0.010 ≤ 277.3% (75/97)57.4% (39/68) 3–522.7% (22/97)42.6% (29/68) Maximum diameter (%) 0.428 ≤ 16 mm64.9% (63/97)72.1% (49/68) > 16 mm, ≤ 30 mm35.1% (34/97)27.9% (19/68) Distribution (%) 0.716 unilobar71.1% (69/97)66.2% (45/68) bilobar28.9% (28/97)33.8% (23/68) Timing of MWA for sCRLM 0.354 Bowel-first39.2% (38/97)38.2% (26/68) Liver-first22.7% (22/97)14.7% (10/68) Concurrent38.1% (37/97)47.1% (32/68)DLM Disappearing colorectal liver metastases, CRLM Colorectal liver metastases, CEA Carcinoembryonic antigen, MWA Microwave ablation
The characteristics of pre-ablative chemotherapy were listed in Table 2. Patients with DLM underwent more cycles of pre-ablative chemotherapy than those without DLM (median cycles: 6 (4, 8) vs. 4 (3, 6), p < 0.001). There were no significant differences regarding the pre-ablative chemotherapy regimens used.
Table 2. Characteristics of pre-ablative chemotherapyCharacteristicsPatients without DLMPatients with DLMP-valueNumber of chemotherapy cycles Median (quartile)4(3,6)6(4,8)< 0.001Chemotherapy regimens used0.957Oxaliplatin-based6443Oxaliplatin &Irinotecan3123Other32DLM Disappearing colorectal liver metastases
The 1:1PSM analysis was also performed between the groups of patients to reduce the impact of bias. Ultimately, 66 patients were assessed and each subgroup included 33patients. The P-values for all covariates were greater than 0.05, indicating that propensity scores for the two groups significantly overlapped (Table 3).
Table 3. Demographics of patients with and without DLM after propensity score matchingCharactersPatients without DLM (n = 33)Patients with DLM (n = 33)p-value Age 0.806 ≤6048.5% (16/33)51.5% (17/33) >6051.5% (17/33)48.5% (16/68) Gender (%) 0.100 Female36.4% (12/33)18.2% (6/33) Male63.6% (21/33)81.8% (27/33) Plasma CEA (%) 1.000 ≤10 µg/L81.8% (27/33)81.8% (27/33) >10 µg/L18.2% (6/33)18.2% (6/33) Primary cancer
Location (%) 0.672 Left87.9% (29/33)93.9% (31/33) Right12.1% (4/33)6.1% (2/33) Pathologic tumor category (%) 1.000 ypT0 – ypT384.8% (28/33)84.8% (28/33) ypT415.2% (5/33)15.2% (5/33) Pathologic lymphatic spread (%) 0.605 N030.3% (10/33)39.4% (13/33) N1 or N269.7% (23/33)60.6% (20/33) Extrahepatic metastasis (%) 0.605 No69.7% (23/33)60.6% (20/33) Yes30.3% (10/33)39.4% (13/33) Initial CRLM
Number (%) 1.000 ≤ 233.3% (11/33)33.3% (11/33) > 266.7% (22/33)66.7% (22/33) Maximum diameter (%) 0.789 ≤ 3 cm66.7% (22/33)72.7% (24/33) > 3 cm33.3% (11/33)27.3% (9/33) Ablated CRLM
Number (%) 1.000 ≤ 266.7% (22/33)66.7% (22/33) 3–533.3% (11/33)33.3% (11/33) Maximum diameter (%) 1.000 ≤ 16 mm30.3% (10/33)30.3% (10/33) > 16 mm, ≤ 30 mm66.7% (23/33)66.7% (23/33) Distribution (%) 0.622 unilobar48.5% (16/33)57.6% (19/33) bilobar51.5% (17/33)42.4% (14/33)DLM Disappearing colorectal liver metastases. CRLM Colorectal liver metastases. CEA Carcinoembryonic antigen
Intrahepatic recurrence free survival for patients with and without DLM
During follow-up, intrahepatic disease progression occurred in 79.4% (54/68) and 45.4% (44/97) of patients with and without DLM, respectively (p < 0.001). The recurrence patterns for patients with and without DLM were shown in Table 4. For patients with DLM, in situ recurrence occurred in 31 patients (including 8 LTP, 23 DLM site recurrences). For patients without DLM, in situ recurrence occurred in 13 patients who developed LTP. The in situ recurrence rate was significantly higher for patients with DLM than those without DLM (45.6% (31/68) versus 13.4% (13/97), p < 0.001). There was no statistical difference of de novo recurrence between two groups (33.8% (23/68) versus 31.9% (31/97), p = 0.802).
Table 4. Intrahepatic recurrence patterns of patients with or without DLMRecurrence patternsPatients without DLMPatients with DLMP-valueRecurrence insitu (%)13.4% (13/97)45.6% (31/68)< 0.001LTP (n)138DLM site recurrence (n)NA23Recurrence de novo (%)31.9% (31/97)33.8% (23/68)0.802DLM Disappearing colorectal liver metastases, LTP Local tumor progression
Before PSM, the 1-year, 3-year, and 5-year ihPFS rates for patients with DLM were 55.7%, 36.8%, and 30.6%, respectively, which is significantly lower than patients without DLM whose 1-year, 3-year, and 5-year ihPFS were 70.8%, 59.3%, and 52.0%, respectively. (p-value = 0.012, Fig. 1). After PSM, the ihPFS rates for patients with DLM were 44.9%, 31.8%, and 21.2% at 1-year, 3-year, and 5-year, respectively, which is significantly lower than patients without DLM whose 1-year, 3-year, and 5-year ihPFS were 72.3%, 58.8%, and 47.5%, respectively. (p-value = 0.039, Fig. 2).
Fig. 1ihPFS of patients with and without DLM before propensity score matching
Fig. 2ihPFS of patients with and without DLM after propensity score matching
On univariable cox regression, extrahepatic metastasis (HR: 1.7; 95% CI: 1.1–2.6; p = 0.029), ablated tumor number (HR: 1.6; 95% CI: 1.0–2.5.0.5; p = 0.036), and DLM (HR: 1.7; 95% CI: 1.1–2.7; p = 0.013) were identified as three independent factors associated with poor ihPFS. On multivariable analyses, extrahepatic metastasis (HR: 1.8; 95% CI: 1.1–2.8; p = 0.018), T4 stage primary cancer (HR: 1.8; 95% CI: 1.0–3.0; p = 0.043), tumor size > 16 mm (HR: 1.9; 95% CI: 1.2–3.0.2.0; p = 0.007), and DLM (HR: 2.2; 95% CI: 1.1–4.1; p = 0.009) were identified as risk factors associated with ihPFS (Table 5).
Table 5. Univariate and multivariate Cox regression for IhPFS in sCRLM patients received pre-ablative chemotherapyCharactersCategory N Univariate analysisMultivariate analysisHR (95%CI)p-valueHR (95%CI)p-value Age ≤ 6092Reference> 60731.1 (0.7–1.7)0.606GenderFemale45ReferenceMale1201.1 (0.7–1.8)0.636 Plasma CEA ≤ 10 µg/L133Reference> 10 µg/L320.7 (0.4–1.3)0.289 Primary cancer
Location Left146ReferenceRight190.9 (0.5–1.9)0.905 Pathologic tumor category ypT0 – ypT3136ReferenceypT4291.5 (0.9–2.6)0.1391.8 (1.0–3.0) 0.043
Pathologic lymphatic spread Negative57ReferencePositive1081.2 (0.7–1.8)0.522 Extrahepatic metastasis No122ReferenceYes431.7 (1.1–2.6) 0.029 1.8 (1.1–2.8) 0.018
Initial CRLM Number≤ 286Reference> 2791.4 (0.9–2.2)0.0950.6 (0.3–1.3)0.190Maximum diameter≤ 3 cm124Reference> 3 cm411.2 (0.7–1.9)0.493 Ablated CRLM Number≤ 2114Reference> 2511.6 (1.0–2.5.0.5) 0.036 1.8 (0.9–3.5)0.074Maximum diameter≤ 16 mm112Reference> 16 mm, ≤ 30 mm531.6 (0.9–2.4)0.0551.9 (1.2–3.0.2.0) 0.007 Distributionunilobar113Referencebilobar521.1(0.7–1.7)0.768 DLM No97ReferenceYes681.7 (1.1–2.7) 0.013 2.2 (1.1–4.1) 0.009
Timing of MWA for sCRLM Bowel-first64ReferenceLiver-first320.8 (0.5–1.6)0.602Concurrent691.2 (0.7–1.9)0.530DLM disappearing colorectal liver metastases, CRLM colorectal liver metastases, CEA carcinoembryonic antigen
Overall survival for patients with and without DLM
Before PSM, the difference of OS was not statistically significant between patients without and with DLM (100% vs. 97.0%, 72.5% vs. 63.3%, and 61.8% vs. 45.2% for 1-year, 3-year and 5-year OS, respectively, p-value = 0.11, Fig. 3). After PSM, the difference of OS was still not statistically significant between patients without and with DLM (100% vs. 93.8%, 53.9% vs. 61.1%, and 53.9% vs. 38.2% for 1-year, 3-year and 5-year OS, respectively, p-value = 0.49, Fig. 4).
Fig. 3OS of patients with and without DLM before propensity score matching
Fig. 4OS of patients with and without DLM after propensity score matching
On univariable cox regression, age over 60 (HR: 2.0; 95% CI: 1.2–3.3; p = 0.009) and right colon cancer (HR: 2.5; 95% CI: 1.3–5.0.3.0; p = 0.008) were identified as independent factors associated with poor OS. On multivariable analyses, age over 60 (HR: 2.3; 95% CI: 1.4–4.0.4.0; p = 0.002), right colon cancer (HR: 2.5; 95% CI: 1.2–5.2; p = 0.011) were identified as risk factors associated with OS (Table 6).
Table 6. Univariate and multivariate Cox regression for OS in sCRLM patients received pre-ablative chemotherapyCharactersCategory N Univariate analysisMultivariate analysisHR (95%CI)p-valueHR (95%CI)p-value Age ≤ 6092Reference> 60732.0 (1.2–3.3) 0.009 2.3 (1.4–4.0.4.0) 0.002 GenderFemale45ReferenceMale1200.9 (0.5–1.5)0.784 Plasma CEA ≤ 10 µg/L133Reference> 10 µg/L320.7 (0.4–1.4)0.303 Primary cancer
Location Left146ReferenceRight192.5 (1.3–5.0.3.0) 0.008 2.5 (1.2–5.2) 0.011
Pathologic tumor category ypT0 – ypT3136ReferenceypT4291.7 (0.9–3.1)0.1251.7 (0.9–3.3)0.110 Pathologic lymphatic spread Negative57Positive1081.2 (0.7–2.0.7.0)0.588 Extrahepatic metastasis No122ReferenceYes431.5 (0.9–2.7)0.1451.8 (1.0–3.2.0.2) 0.055
Initial CRLM Number≤ 286Reference> 2791.7 (1.0–2.8.0.8)0.0491.2 (0.5–3.0.5.0)0.700Maximum diameter≤ 3 cm124Reference> 3 cm430.9 (0.5–1.8)0.816 Ablated CRLM Number≤ 2114Reference> 2511.5 (0.9–2.6)0.1181.3 (0.6–2.7)0.550Maximum diameter≤ 16 mm112Reference> 16 mm, ≤ 30 mm530.8 (0.4–1.5)0.492Distributionunilobar113Referencebilobar521.2 (0.7–1.9)0.597 DLM No97ReferenceYes681.5 (0.9–2.5)0.1141.2 (0.6–2.5)0.590 Timing of MWA for sCRLM Bowel-first64ReferenceLiver-first320.7 (0.4–1.4)0.344Concurrent690.7 (0.4–1.2)0.226DLM Disappearing colorectal liver metastases. CRLM Colorectal liver metastases. CEA Carcinoembryonic antigen
Discussion
Pre-ablative chemotherapy commonly results in DLM, making it challenging to eradicate micro metastases at DLM sites. Gaining insight into how DLM affects the outcomes of percutaneous MWA is crucial for determining the optimal timing for MWA in conjunction with systemic therapy. Our findings demonstrate that patients with unablated DLM are associated with poorer ihPFS than those without DLM, although it does not significantly influence OS.
It is noteworthy that radiographic identified DLM does not necessarily correspond to a pathologically complete remission, with approximately 42.3% to 50% of the DLM detected on preoperative CT showed pathologically viable cancer cells or recurred during the follow-up [9, 10]. Studies using MRI reported complete remission at DLM sites occurred in 39%−85% of cases [11, 12]. These undetected tumors might still be viable but could not be detected and ablated for percutaneous MWA. Therefore, it resulted in a high recurrence rate at one-third of DLM sites and worse ihPFS rates for patients with DLM in the present study.
However, the difference of OS was not statistically significant between patients with or without DLM in our study. These results were consistent with a systematic review showing that patients with resected DLM experienced longer disease-free survival compared to those with DLM left in situ, although differences in OS were not observed [9]. We suppose that the reasons for comparable OS for patients with DLM may lie in their favorable tumor biology with better response to chemotherapy. Moreover, most tumor recurrences can be re-treated with radical local treatment, potentially leading to comparable OS outcomes of patients with DLM. In addition, the median follow-up of 48.2 months may be insufficient to demonstrate OS distinction.
DLM refers to lesion visible on baseline CEMRI that disappears following chemotherapy [18]. After chemotherapy, the sensitivity of CEMRI, CEUS, CECT and PET/CT for diagnosing CRLM was 90%, 79%, 77% and 48%, respectively, whereas CEMRI showed significantly highest sensitivity and was recommended as first choice for patients receiving chemotherapy [19]. Most institutions use CECT only for assessment due to its ability to complete evaluation for intrahepatic metastases and extrahepatic disease. However, the sensitivity of CECT in patients with chemotherapy was significantly worse than those without (77% vs. 91%, P = 0.024) [19], leading to elevated observation rates of DLM [20, 21]. Intraoperative CEUS (IOCEUS) proved equivalent in sensitivity to MRI (95% and 90%). An additional 40% and 46% of tumors invisible on preoperative imaging might be detected using IOCEUS [22, 23]. Regrettably, IOCEUS can only be performed during the operation. Radiographic DLM is currently managed conservatively by regular follow-up for patients underwent percutaneous MWA in our center. One primary limitation of imaging-guided percutaneous MWA is that current imagings are powerless to detect all residual lesions. To compensate this limitation, we used high-frequency US and CEUS to maximize the CRLM detection and guide ablation. Our previous study demonstrated that application of trans-abdominal high-frequency US and CEUS could significantly improve the detection rate of superficial lesions and small CRLM than convex probe CEUS, especially for patients after chemotherapy [15].
The optimal strategy for employing thermal ablation combined with systemic therapy in CRLM is under debate. In our previous study, we investigated how the timing of ablation during chemotherapy affects oncologic outcomes and revealed that disease-free survival or progression-free survival were significantly worse in delayed versus the upfront MWA groups [24, 25], suggesting to early and completely ablate tumors. We believe that chemotherapy-induced liver damage and tumor shrinkage may obscure tumor margins, resulting in inaccurate antenna positions under imaging guidance, contributing to incomplete ablation. In the present study, patients with DLM received more cycles of pre-ablative chemotherapy, resulting in a delay in the timing of MWA compared to those without DLM. Our finding also demonstrated DLM as a risk factor for ihPFS after MWA. Given that DLM is frequently associated with systemic therapy and tends to lead to a higher rate of intrahepatic recurrence, it is reasonable to speculate that radiological DLM during delayed ablation contributes to the decrease in disease-free survival as compared to up-front ablation, which eliminates tumor early and completely. Therefore, we advocate for a more proactive approach to eliminate tumor early and completely, ideally before they become radiographic undetectable. This strategy may help reduce the risk of recurrence, enhance patient outcomes, minimize the need for repeated local interventions, and subsequently conserve medical resources.
This study has several limitations. Firstly, the retrospective design led to variability in the imaging modalities used to identify DLM, as not all patients underwent MRI examinations before and after chemotherapy. However, despite this variability, the patients with DLM in this study represent those who could not achieve NED through ultrasound-guided percutaneous MWA. Thus, whether CT or MRI was used to define DLM is unlikely to affect the results. Secondly, the chemotherapy regimens and durations varied among patients. As chemotherapy protocols have evolved over the study period, some patients received targeted biological therapies in addition to chemotherapy. Lastly, patients with DLM or disease progression who opted for supportive care instead of local treatment were excluded from the analysis, which may have introduced selection bias. Lastly, patients with new lesions during chemotherapy were excluded from the analysis, which may have introduced selection bias. It is reported that patients with one or more new lesions at disease progression were associated with significantly worse survival [26]. Including these patients in the group without DLM could confound the results.
In conclusion, patients with DLM presented worse ihPFS, suggesting that to eradicate visible tumors before disappearance may be advantageous when synchronous CRLM is ablatable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adam R, Delvart V, Pascal G et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: a model to predict long-term survival. Ann Surg 2004;240:644 – 57; discussion 57 – 8.10.1097/01.sla.0000141198.92114.f 6PMC 135646615383792 · doi ↗ · pubmed ↗
- 2Ruers T, Van Coevorden F, Punt CJ, et al. Local treatment of unresectable colorectal liver metastases: results of a randomized phase II trial. J Natl Cancer Inst. 2017;109(9):djx 015. 10.1093/jnci/djx 015.10.1093/jnci/djx 015PMC 540899928376151 · doi ↗ · pubmed ↗