Impact of statin use on survival and adverse events in patients with cancer receiving radiotherapy: a systematic review and meta-analysis
Hala Shokr, Wan-Chuen Liao, Corinne Faivre-Finn, Clare Dempsey, Kaye Janine Williams, Li-Chia Chen

TL;DR
This study finds that statin use during cancer radiotherapy does not significantly affect overall survival but may influence adverse events and outcomes depending on cancer type.
Contribution
The study provides a systematic review and meta-analysis of statin effects on cancer radiotherapy outcomes, revealing cancer-specific survival and adverse event associations.
Findings
Statin use was not associated with significant differences in overall survival rates.
Statin users had higher risks of certain adverse events like cardiac events and mucositis, but lower risks of others like stroke and rectal toxicity.
Survival outcomes varied significantly by cancer type, with both improved and reduced survival observed in specific cancers.
Abstract
Given limited and conflicting data, this systematic review and meta-analysis investigate the impacts of statin use on survival outcomes and adverse events in patients with cancer receiving radiotherapy. A comprehensive search of MEDLINE, EMBASE, Web of Science, Scopus, and PubMed (January 2000 to June 2024) included studies on adults (≥ 18 years) with histologically confirmed cancer receiving oral statins during radiotherapy. Overall survival (OS) rates and radiotherapy-related adverse effects were compared between statin users and non-users using odds ratios (ORs) and 95% confidence intervals (95%CIs). Meta-regression explored the effects of cancer type and statin intensity on OS rates, reported as coefficients (β) and 95%CI. Of 21 studies (19 cohort studies and two randomized trials), OS rates did not significantly differ between statin users and non-users (OR: 1.29; 95%CI: 0.99,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
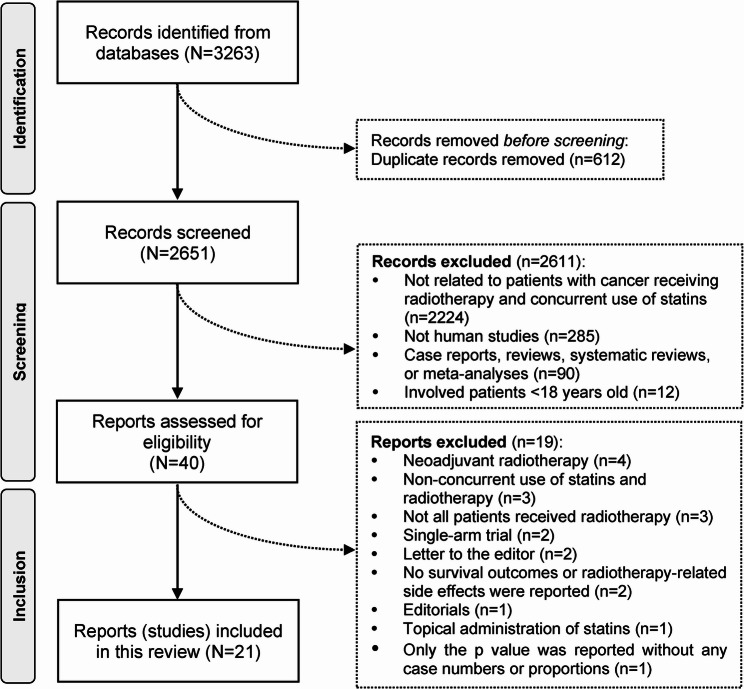 Figure 1
Figure 1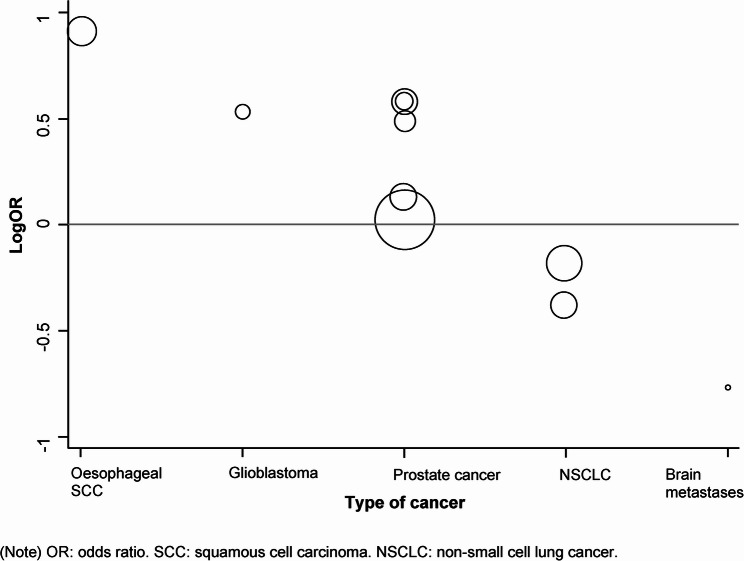 Figure 2
Figure 2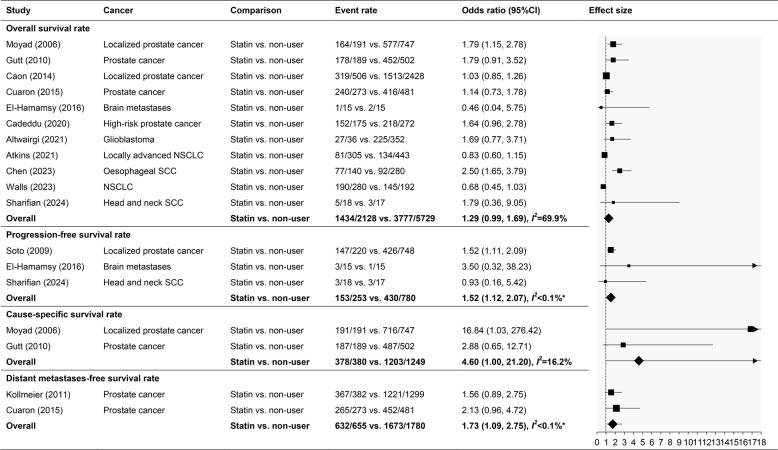 Figure 3
Figure 3- —http://dx.doi.org/10.13039/501100000289Cancer Research UK
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Lipids, and Metabolism · Chemotherapy-induced cardiotoxicity and mitigation · Lipoproteins and Cardiovascular Health
Background
Polypharmacy is prevalent among the elderly population as well as in patients with cancer [1, 2]. Balancing the risks and benefits of continuing multiple concurrent medications during cancer radiotherapy is imperative in clinical oncology. Still, a lack of data remains to inform clinical decisions [3]. Statins, cholesterol-lowering agents, are commonly prescribed long-term to middle-aged patients with hypercholesterolemia for the prevention of cardiovascular and coronary heart diseases due to their pleiotropic anti-inflammatory, antioxidant, and anti-fibrotic effects [4, 5]. In the United Kingdom, 24.6% of middle-aged adults (aged 40 and above) reported using statins in 2018 [6]. Statins are also highly prevalent in patients with cancers receiving radiotherapy [7].
Statins have diverse cellular effects, including regulating cell proliferation, differentiation, and survival [8, 9]. They inhibit 3-hydroxy-3-methylglutaryl CoA reductase, the rate-limiting enzyme in the mevalonate pathway, leading to decreased cholesterol synthesis and downstream isoprenoid intermediates [10]. These intermediates are crucial for the post-translational modification of proteins, which are involved in cell proliferation, survival, and migration. Statins can also arrest cells in the late G1 phase of the cell cycle, disrupting synchronisation during the radiosensitive phase and potentially reducing radiation resistance [11].
Some review articles have addressed the ability of statins to inhibit the proliferation and induce apoptosis of tumour cells, suggesting their broader therapeutic potential as an adjuvant to cancer treatment [8, 12]. Radiotherapy may benefit from statins by potentially mitigating typical tissue damage through reductions in pro-inflammatory and pro-fibrotic cytokines, as well as moderating the DNA damage response triggered by ionising radiation [13]. However, conflicting and controversial clinical results regarding radiotherapy still exist.
Most prior research investigating the associations between concurrent statin use and various cancers in patients receiving radiotherapy was retrospective cohort observational studies. Statin use has been suggested to improve cancer outcomes in patients with head and neck cancer [7, 14], oesophageal squamous cell carcinoma (SCC) [15], and pelvic malignancies [16]. Conversely, other research has shown no effect of statin use on glioblastoma [17] and brain metastases [18]. In patients with prostate cancer and non-small cell lung cancer (NSCLC) receiving radiotherapy, both beneficial [19–26] and no effects [15, 27–30] of statin use have been reported.
In addition, recent retrospective studies revealed a dose-response relationship between statin intensity and survival outcomes in patients with NSCLC (n = 478) and oesophageal SCC (n = 420) undergoing radiotherapy or concurrent chemoradiotherapy [26, 31]. Higher cumulative daily doses or intensity of statin use were associated with reduced mortality and better overall survival [26, 31]. Conversely, a retrospective cohort study of patients with prostate cancer (n = 774) receiving external beam radiation therapy found no clear dose-response relationship for daily statin dose or duration of use [29]. Variations in follow-up periods and actual drug durations likely contribute to these differences.
Conflict ing results from prospective trials and retrospective studies highlight the need to integrate current evidence for oncology practice recommendations. Assessing and synthesizing diverse findings comprehensively is crucial to inform evidence-based clinical decisions on combining statins with radiotherapy in cancer treatment. Therefore, this systematic review and meta-analysis aimed to clarify the impact of concurrent statin use on survival outcomes and radiotherapy-related adverse events in patients undergoing radiotherapy by synthesising existing literature.
Methods
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (Appendix 1) [32]. The protocol was registered at PROSPERO (no. CRD42023487336).
Selection criteria
The inclusion and exclusion criteria of this study (Table 1) are summarised as follows.
Table 1. Inclusion and exclusion criteria of this studyComponentInclusion criteriaExclusion criteriaPopulation and conditions• Patients aged 18 years and above.• Patients diagnosed with histologically confirmed cancers (newly diagnosed or recurrent) are scheduled to receive radiotherapy.• Patients include paediatrics, children, adolescents, neonates, and infants.• Studies involved mixed-age groups.• Neoadjuvant radiotherapy or diagnostic radiology (e.g., X-rays, magnetic resonance images).• Patients with cancer types are not amenable to radiotherapy.Intervention and comparatorOral administration of statin, either alone or in combination with other drugs, such as chemotherapy.• Non-concurrent use of statin and radiotherapy (not during the radiotherapy cycles).Outcome• Survival outcomes included overall survival and other related results.• Adverse events occurred during or right after the radiotherapy.• Radiation-related toxicity occurred before the administration of statin.Study typeHuman studiesAnimal or in vitro studiesLanguageEnglishOther languages without English translationPublicationFull-text article on prospective or retrospective cohort study, cross-sectional study, and clinical trial.Case-control study, case series, case report, systematic review, meta-analysis, conference abstract, abstract without full article, editorial, letter to editors, commentary, and grey literature.
Types of studies
Original articles of prospective and retrospective cohort studies, cross-sectional studies, and clinical trials were included. Case-control studies, case series, case reports, systematic reviews, meta-analyses, conference abstracts, editorials, letters to editors, commentary, and grey literature were excluded (Table 2).Table 2. Characteristics of included studiesAuthor, year, countryCancerTypes of radiationRadiation dose (Gy)Number of patientsAge of patients (year)Outcome categoryTotalStatin usersNon-users Moyad, 2006, US [30]Localized prostate cancerBrachytherapyNA938191747Mean ± SD: 66.1 ± 7.2Survival outcomes Soto, 2009, US [18]Localized prostate cancerDefinitive RTMedian (range): 75.8 (45, 153)968220748Mean ± SD: 68.2 ± 7.3Survival outcomes Gutt, 2010, US [20]Prostate cancerEBRT and/or brachytherapyMedian (range): 72 (NA)691189502Median (range): statin user: 69 (42, 83); non-user: 68 (44, 83)Survival outcomes Kollmeier, 2011, US [22]Prostate cancerRTMedian (range): 81 (75.6, 86.4)16813821299NASurvival outcomes Alizadeh, 2012, Canada [19]Prostate cancerEBRT or brachytherapyNA381172209Mean ± SD: statin user: 66.0 ± 6.0; non-user: 65.9 ± 7.4Survival outcomes Wedlake, 2012, UK [16]Pelvic malignanciesRadical pelvic RTMedian (range): statin user: 64 (36, 74); non-user: 55.8 (20, 74)23738199Median (range): statin user: 73.5 (59, 86); non-user: 67 (29, 88)RT-related side effects Chao, 2013, US [29]Prostate cancerEBRTNA774401373Mean ± SD: 68.4 ± 7.0Survival outcomes Caon, 2014, Canada [28]Localized prostate cancerEBRTMedian (range): 70 (52.50, 78)29345062428Mean (range): 70.3 (45, 88)Survival outcomes Cuaron, 2015, US [15]Prostate cancerBrachytherapyMedian: patients received either LDR (144) or HDR (38) monotherapy or LDR (110) or HDR (19.5) in combination with supplemental EBRT (50.4)754273481NASurvival outcomes Oh, 2015, US [24]Prostate cancerBrachytherapyBrachytherapy: 145 or 110; EBRT: range: 22, 4624717473Median (range): 62 (45.6, 81.94)Survival outcomes El-Hamamsy, 2016, Egypt [33]Brain metastasesWhole-brain RTMedian (range): 30 (NA)301515Mean ± SD: 54.4 ± 11.1Survival outcomes Liu, 2017, US [23]Prostate cancerRTMedian (range): 2000–2005: 75.6 (NA); 2009–2012: 80.3 (NA)381146235Mean ± SD: 74.4 ± 6.0Survival outcomes Palumbo, 2017, Italy [25]Prostate cancerHypofractionated intensity-modulated RTMedian (range): 74.25 (NA)19555140Median (range): 74 (57, 85)RT-related side effects Boulet, 2019, Canada [7]Thorax, head and neck cancerRTNA571841661552Mean ± SD: 75 ± 6.1Survival outcomesRT-related side effects Cadeddu, 2020, Spain [27]High-risk prostate cancerRTRange: 72, 76447175272Median (range): 70 (46, 83)Survival outcomesRT-related side effects Altwairgi, 2021, Saudi Arabia [17]GlioblastomaRTMedian (range): 12 (NA)38836352Median (range): statin user: 52 (20, 69); historical control: 56 (19, 70); control trial: 47 (18, 81)Survival outcomes Atkins, 2021, US [34]Locally advanced NSCLCThoracic RTMedian (IQR): statin user: 64 (56, 66), non-user: 64 (54, 66)748305443Median (IQR): statin user: 67 (61, 75); non-user: 62 (55, 71)Survival outcomesRT-related side effects Chen, 2023, Taiwan [31]Oesophageal SCCCRTTotal dose: 50.4420140280Mean ± SD: statin user: 64.23 ± 11.93; non-user: 64.53 ± 13.27Survival outcomes Walls, 2023, UK [26]NSCLCRTNA478283195Median (IQR): 70 (64, 76)Survival outcomesRT-related side effects Lin, 2024, Taiwan [14]Advanced nasopharyngeal carcinomaRTRange: 70, 70.2502225152507Median (IQR): statin user: 51.30 (46.07, 59.01); non-user: 51.11 (43.91, 59.15)RT-related side effectsSharifian, 2024, Iran [33]Locally advanced head and neck SCCCRTTotal dose: 70351817Mean: statin user: 57.9; non-user: 57.2Survival outcomesRT-related side effectsUS United States, UK United Kingdom, NSCLC non-small cell lung cancer, SCC squamous cell carcinoma, RT radiotherapy, EBRT external beam radiation therapy, CRT chemoradiotherapy, NA not available, LDR low dose rate, HDR high dose rate, IQR interquartile range, SD standard deviation
Types of participants
Studies enrolled participants aged 18 and above with histologically confirmed cancer undergoing various radiotherapy doses and regimens were included. Studies involving individuals under 18 years or mixed-age groups, those undergoing neoadjuvant radiotherapy or diagnostic radiology, and those with cancer not indicated for radiotherapy were excluded.
Types of interventions
Studies of patients receiving oral statins alone or combined with other drugs (e.g., chemotherapy) during radiotherapy were included. Studies of patients not using statins concurrently during radiotherapy cycles were excluded.
Types of outcome measures
Included were studies measuring survival outcomes (e.g., overall survival rate or survival time) and radiotherapy-related side effects occurring during or immediately after radiotherapy. Excluded were studies that reported only radiation-related toxicity occurring before statin administration.
Data sources and search strategies
A comprehensive search of electronic databases, including MEDLINE, EMBASE, Web of Science, Scopus, and PubMed, was conducted from January 2000 to June 2024. The search was restricted to studies published from January 2000 onward, focusing on research conducted in the context of established statin use, following landmark trials such as the Heart Protection Study [35], which significantly influenced clinical practice starting in 2002. This approach aimed to capture literature reflecting current prescribing patterns and clinical relevance. The initial exploration revealed pertinent literature published after 2000, prompting the commencement of the review in July 2024. This was achieved by applying structured search strategies (Appendix 2), which incorporated controlled vocabulary and keywords aligned with predefined inclusion and exclusion criteria (Table 1). Additionally, the search was restricted to English-language publications and human studies.
Study selection
Two reviewers (WCL and HS) independently screened titles and abstracts of articles retrieved from the electronic database search using a pre-designed form and categorised studies as “included,” “further check,” or “excluded.” Prior to the screening, a calibration exercise was conducted where both reviewers independently screened a sample of records. Consistency between reviewers was evaluated using the intraclass correlation coefficient (two-way mixed effect model with absolute agreement) [36]. Disagreements were resolved through discussion between reviewers, and a third reviewer (LCC) was consulted if needed to reach a consensus. Potentially eligible articles underwent further independent review by both reviewers (WCL and HS) to finalise inclusion decisions.
Data extraction and management
Two reviewers (WCL and HS) independently used a standardized electronic data extraction form to extract study data. Disagreements were resolved by a third reviewer (LCC). Extracted information included study details such as title, lead author, country, publication year, study design, setting, targeted population (disease and cancer stages), intervention (type and dosage of statin), comparison, outcome measures, and follow-up period. Study results were retrieved, including survival outcomes and adverse events during or immediately after radiotherapy. If raw data were unavailable, mean (with standard deviation) or median (range) values were extracted. Statin intensity was categorised based on the guidelines into low, medium, and high [37, 38].
Risk of bias assessment
All included studies underwent quality assessment using the Cochrane Risk of Bias Assessment Tool (RoB 2) [39] for randomized controlled trials and the Risk of Bias in Non-randomized Studies of Interventions tool (ROBINS-I) [40] for non-randomized studies. Studies were classified as having a low risk of bias, some concerns, or high risk of bias according to RoB 2 and low, moderate, serious, or critical risk of bias based on ROBINS-I.
Data analysis
Survival outcomes and radiotherapy-related side effects were compared between statin users and non-users. If studies reported survival outcomes at various time points, priority was given to the closest censoring year to the five-year mark, as the five-year survival rate is widely acknowledged as a critical measure of cancer care quality and long-term outcomes [41].
Overall survival rate, as well as the progression-free, cause-specific, and distant metastasis-free survival rates, were synthesized using a random-effects model (Der-Simonian and Laird method [42]), and the pooled effect size was presented as odds ratio (OR) with 95% confidence interval (95%CI). Heterogeneity was assessed using the I^2^ test (%). Meta-regression was used to analyse factors (the type of cancers and intensity of statins) associated with effect size, presenting the results as coefficient (β) and 95%CI.
The median survival times were reported by subtracting between statin users and non-users to demonstrate the difference. The effect size (OR and 95%CI) of radiotherapy-related side effect rate was reported for different types of cancers. STATA (Release 14, College Station, TX: StataCorp LLC) was used for meta-analysis and meta-regression, with statistical significance set at p < 0.05.
Results
Selection of study
Of the 3263 records identified from electronic database searches, 40 studies were assessed for eligibility after removing duplicates (n = 612) and irrelevant records (n = 2611), such as those unrelated to patients with cancer receiving radiotherapy and concurrent use of statins (n = 2224), non-human studies (n = 285), case reports, reviews, systematic reviews, or meta-analyses (n = 90), and studies involving patients under 18 years old (n = 12). During the full-text screening, 19 studies were excluded, leaving 21 studies (23467 patients) for analysis (Fig. 1). The intraclass correlation coefficient was 0.961 (95%CI: 0.957, 0.965) between the two reviewers, indicating a good consistency.
Fig. 1. Selection of studies
Characteristics of included studies
Most of the 21 included studies (19 cohort studies [7, 14–20, 22–31, 41] and two randomised trials [33, 43]) targeted patients with prostate cancer (n = 12) [15, 18–20, 22–25, 27–30], followed by NSCLC (n = 2) [26, 34], thorax, head, and neck cancer (n = 2) [7, 43], pelvic malignancies (n = 1) [16], brain metastases (n = 1) [33], glioblastoma (n = 1) [17], oesophageal SCC (n = 1) [31], and nasopharyngeal carcinoma (n = 1) [14]. Overall, 10,400 statin users and 13,067 non-users were included in this review.
Four studies provided information on statin dosage and intensity, with two focusing on high-intensity statins [17, 33], one using moderate-intensity lovastatin [43], and one covering low, medium, and high intensities [26]. The most frequently reported survival outcome is the overall survival rate (n = 11) [15, 17, 20, 26–28, 30, 31, 33, 34, 43].
The radiotherapy-related adverse events were cancer-specific and reported in patients with prostate cancer (n = 2) [25, 27], NSCLC (n = 2) [26, 34], thorax, head, and neck cancer (n = 2) [7, 43], nasopharyngeal carcinoma (n = 1) [14], and pelvic malignancies (n = 1) [16].
Quality assessment
According to RoB 2, two included randomised trials showed a high risk of bias. One was due to the heterogeneity of primary tumour origin, limited follow-up, and the severe cognitive impairment of the patients, which would affect the accuracy of self-rated quality-of-life assessments [33]. The other was missing outcome data in a small sample size trial [43] (Appendix 3).
Among the 19 cohort studies, nine had serious bias [7, 15–17, 19, 22, 26, 29, 30].
and ten had moderate bias [14, 18, 20, 23–25, 27, 28, 31, 34] (Appendix 4). Serious biases included neglecting to report radiation dose (n = 5) [7, 19, 26, 29, 30], cancer stage (n = 3) [7, 16, 17], follow-up period (n = 2) [16, 19], and population age (n = 2) [15, 22]. One study had a serious bias in outcome measurement when comparing prospectively collected data with retrospective statistics [17]. Confounding bias existed in statin administration, cancer stage, and patients’ comorbidities.
Survival outcomes
The overall survival rate did not significantly differ between statin users and non-users (OR: 1.29; 95%CI: 0.99, 1.69; I^2^ = 69.9%) in the pooled results of 11 studies. Statin users had a significantly better progression-free survival rate (OR: 1.52; 95%CI: 1.12, 2.07; I^2^ < 0.1%) based on three studies and a distant metastases-free survival rate (OR: 1.73; 95%CI: 1.09, 2.75; I^2^ < 0.1%) according to two studies. Although not significantly different, statin users had a slightly better cause-specific (death from prostate cancer) survival rate, pooled from two studies, with a wide 95%CI (OR: 4.60; 95%CI: 1.00, 21.20; I^2^ = 16.2%) (Table 3).
Table 3. Survival outcome of overall, progression-free, cause-specific, and distant metastases-free survival rateNSCLC non-small cell lung cancer, SCC squamous cell carcinoma, CI confidence interval*Significant difference
Meta-regression analysis revealed that the type of cancer significantly affects the overall survival rate (β: −0.29; 95%CI: −0.45, −0.13; p < 0.01). Statin users had better survival in oesophageal SCC, head and neck SCC, glioblastoma, and prostate cancer, but worse in NSCLC and brain metastases (Fig. 2). Statins did not significantly affect the overall survival rate (β: 0.20; 95%CI: −1.22, 1.62; p = 0.60).
Fig. 2. Meta-regression of log odds ratios of overall survival rate and type of cancer
Statin users showed significantly better outcomes in several measures: prostate-specific antigen level > 20 ng/mL rate (OR: 0.29; 95%CI: 0.08, 0.83) [19], prostate cancer-specific survival rate (OR: 1.53; 95%CI: 1.03, 2.28) [28], the cumulative biochemical failure rate in prostate cancer (OR: 0.18; 95%CI: 0.07, 0.50) [24], freedom from biochemical failure in prostate cancer (OR: 4.16; 95%CI: 1.31, 13.18) [24], all-cause mortality in oesophageal SCC (OR: 0.33; 95%CI: 0.21, 0.53) [31], oesophageal SCC-specific survival rate (OR: 2.25; 95%CI: 1.49, 3.40) [31], and oesophageal SCC-specific mortality (OR: 0.45; 95%CI: 0.30, 0.68) [31] compared to non-users (Table 4). Notably, each measure was reported by a single study.
Table 4. Other survival outcomes reported by only one study in each indicatorSurvival outcomeStudyComparisonEvent rateOdds ratio (95%CI)Prostate cancer Biochemical progression-free survival rateMoyad (2006)Statin vs. non-user188/191 vs. 711/7473.17 (0.97, 10.42) Freedom from distant metastasesGutt (2010)Statin vs. non-user185/189 vs. 482/5021.92 (0.65, 5.69) Prostate-specific antigen level > 20 ng/mL rateAlizadeh (2012)Statin vs. non-userNA/172 vs. NA/209 ^§^0.29 (0.08, 0.83) * Prostate cancer recurrence rateChao (2013)Statin vs. non-user81/401 vs. 64/3731.22 (0.85, 1.76) Prostate cancer-specific survival rateCaon (2014)Statin vs. non-user476/506 vs. 2214/24281.53 (1.03, 2.28) * Cumulative biochemical failure rateOh (2015)Statin vs. non-user6/174 vs. 12/730.18 (0.07, 0.50) * Freedom from biochemical failureOh (2015)Statin vs. non-user169/174 vs. 65/734.16 (1.31, 13.18) * Prostate-specific antigen relapse-free survival rateCuaron (2015)Statin vs. non-user231/273 vs. 424/4810.74 (0.48, 1.14) Biochemical failure-free survival rateCadeddu (2020)Statin vs. non-user137/175 vs. 221/2720.83 (0.52, 1.33) Disease-specific survival rateCadeddu (2020)Statin vs. non-user172/175 vs. 265/2721.51 (0.39, 5.94) Distant failure-free survival rateCadeddu (2020)Statin vs. non-user158/175 vs. 239/2721.28 (0.69, 2.38)Thorax, head and neck cancers Myocardial infarction/stroke/death rateBoulet (2019)Statin vs. non-user376/4166 vs. 160/15520.86 (0.71, 1.05) Stroke rateBoulet (2019)Statin vs. non-user110/4166 vs. 56/15520.72 (0.52, 1.00)Oesophageal SCC All-cause mortality rateChen (2023)Statin vs. non-user87/140 vs. 233/2800.33 (0.21, 0.53) * Oesophageal SCC-specific survival rateChen (2023)Statin vs. non-user82/140 vs. 108/2802.25 (1.49, 3.40) * Oesophageal SCC-specific mortality rateChen (2023)Statin vs. non-user66/140 vs. 186/2800.45 (0.30, 0.68) SCC squamous cell carcinoma, NA not available, CI confidence interval^§^The case number was not provided, but the odds ratio and 95% confidence interval were reported in the included studySignificant difference
In statin users with brain metastases [33] and head and neck SCC [43], median overall survival and progression-free survival times were longer by less than a month and five months, respectively, compared to non-users. Conversely, in patients with glioblastoma, statin users had a longer median overall survival but shorter median progression-free survival time [17]. Statin users with NSCLC had a median locoregional control of 10.8 months shorter and a median distant control of 17.8 months shorter than non-users [26] (Table 5). Additionally, the mean prostate-specific antigen level was lower in statin users with prostate cancer than in non-users [23].
Table 5. Survival outcomes of median survival timeStudyCancerComparisonNumber of patientsMedian time (months)Median time differences between exposed and non-exposed groups (months)Overall survival time El-Hamamsy (2016) [33]Brain metastasesStatin vs. non-user15 vs. 153.4 vs. 30.4 Altwairgi (2021) [17]GlioblastomaStatin vs. non-user36 vs. 35219.9 vs. 19.60.3 Sharifian (2024) [43]Head and neck SCCStatin vs. non-user18 vs. 1722 vs. 175Progression-free survival time El-Hamamsy (2016) [33]Brain metastasesStatin vs. non-user15 vs. 151.6 vs. 1.470.13 Altwairgi (2021) [17]GlioblastomaStatin vs. non-user36 vs. 3527.6 vs. 7.8−0.2 Sharifian (2024) [43]Head and neck SCCStatin vs. non-user18 vs. 1720 vs. 155Locoregional control Walls (2023) [26]NSCLCStatin vs. non-user283 vs. 19529.7 vs. 40.5−10.8Distant control Walls (2023) [26]NSCLCStatin vs. non-user283 vs. 19534.1 vs. 51.9−17.8SCC squamous cell carcinoma, NSCLC non-small cell lung cancer
Radiotherapy-related adverse events
Statin users had a significantly higher risk of major adverse cardiac events in patients with NSCLC (OR: 2.22; 95%CI: 1.38, 3.59) [34] and ≥ grade 2 mucositis (OR: 26.00; 95%CI: 4.09, 165.1) in head and neck SCC, but a lower risk with ischemic stroke (OR: 0.80; 95%CI: 0.67, 0.95) in patients with nasopharyngeal carcinoma [14] and rectal toxicity (OR: 0.45; 95%CI: 0.23, 0.88) in those with prostate cancer [25] compared to non-users (Table 6). Additionally, statin users with pelvic malignancies had higher inflammatory bowel disease questionnaire-bowel scores, indicating fewer symptoms [16].
Table 6. Radiotherapy-related adverse eventsAdverse eventStudyComparisonFollow-up (months)Event rateOdds ratio (95%CI)NSCLC ≥ 1 major adverse cardiac events rateAtkins (2021)Statin vs. non-userMedian (IQR): 20.4 (8.4, 45.0)45/305 vs. 32/4432.22 (1.38, 3.59) * Cardiac events rateWalls (2023)Statin vs. non-userMedian (range): 21.1 (NA)50/283 vs. 29/1951.23 (0.75, 2.02)Thorax, head and neck cancers Hepatitis rateBoulet (2019)Statin vs. non-userMean ± SD: statin user: 1.63 ± 1.93; non-user: 1.46 ± 1.8820/4332 vs. 2/13863.21 (0.75, 13.75) Transaminitis rateBoulet (2019)Statin vs. non-userMean ± SD: statin user: 1.63 ± 1.93; non-user: 1.46 ± 1.8816/4332 vs. 1/13865.13 (0.68, 38.75) Myositis/myalgia rateBoulet (2019)Statin vs. non-userMean ± SD: statin user: 1.63 ± 1.93; non-user: 1.46 ± 1.8823/4332 vs. 4/13861.84 (0.64, 5.34) Rhabdomyolysis rateBoulet (2019)Statin vs. non-userMean ± SD: statin user: 1.63 ± 1.93; non-user: 1.46 ± 1.881/4332 vs. 0/13860.64 (0.02, 19.09) ≥Grade 2 mucositisSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)16/18 vs. 4/1726.00 (4.09, 165.10) * ≥Grade 2 dermatitisSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)11/18 vs. 14/170.34 (0.07, 1.61) ≥Grade 2 dysphagiaSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)7/18 vs. 6/171.17 (0.30, 4.61) ≥Grade 2 anaemiaSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)2/18 vs. 2/170.94 (0.12, 7.52) ≥Grade 2 leukopeniaSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)2/18 vs. 2/170.94 (0.12, 7.52) ≥Grade 2 thrombocytopeniaSharifian (2024)Statin vs. non-userMedian (range): statin user: 22 (NA); non-user: 17 (NA)3/18 vs. 5/170.48 (0.09, 2.43)Nasopharyngeal carcinoma Ischemic stroke rateLin (2024)Statin vs. non-userMedian (range): 90 (NA)273/2515 vs. 332/25070.80 (0.67, 0.95) Prostate cancer Rectal toxicityPalumbo (2017)Statin vs. non-userMedian (range): 26 (3, 60)15/55 vs. 64/1400.45 (0.23, 0.88) * Acute genitourinary toxicityCadeddu (2020)Statin vs. non-userMedian (range): 88 (1, 194)NA/175 vs. NA/272 ^§^1.20 (0.40, 1.00) Chronic genitourinary toxicityCadeddu (2020)Statin vs. non-userMedian (range): 88 (1, 194)NA/175 vs. NA/272 ^§^1.00 (0.60, 1.50) Acute gastrointestinal toxicityCadeddu (2020)Statin vs. non-userMedian (range): 88 (1, 194)NA/175 vs. NA/272 ^§^1.10 (0.70, 1.80) Chronic gastrointestinal toxicityCadeddu (2020)Statin vs. non-userMedian (range): 88 (1, 194)NA/175 vs. NA/272 ^§^1.50 (0.70, 2.90)NSCLC non-small cell lung cancer, IQR interquartile range, NA not available. SD standard deviation, CI confidence interval^§^The case number was not provided, but the odds ratio and 95% confidence interval were reported in the included studySignificant difference Estimate for ≥ Grade 2 mucositis is derived from a single small RCT with high risk of bias and low certainty
Discussion
This study found no significant difference in overall survival rates between statin users and non-users among patients with cancer receiving radiotherapy. However, progression-free and distant metastasis-free survival rates favoured statin users, albeit based on limited studies. The type of cancer influenced survival rates: statin use was associated with improved survival in oesophageal SCC, head and neck SCC, glioblastoma, and prostate cancer, but with poorer outcomes in NSCLC and brain metastases.
No correlation was found between the intensity of statin use and survival outcomes. Statin users had a higher incidence of major adverse cardiac events in NSCLC and ≥ grade 2 or greater mucositis in head and neck SCC, but a lower risk of ischemic stroke in nasopharyngeal carcinoma and rectal toxicity in prostate cancer. However, given that most of the included studies were observational, these findings demonstrate associations rather than causation.
This review found that the current evidence is limited in determining the impact of concurrent statin use on survival outcomes and radiotherapy-related adverse events. Moreover, many confounding factors were either not reported or could not be adequately controlled in regression analyses. The diverse biological characteristics, aggressiveness, and prognoses of different cancers may influence the effects of statins.
For example, statins inhibit the mevalonate pathway, leading to decreased cholesterol synthesis and the subsequent reduction of downstream isoprenoid intermediates, which can disrupt cancer cell signalling and tumour growth. However, the extent and nature of this disruption depend largely on the tumour’s genetic and molecular profile. NSCLC, for instance, frequently involves KRAS mutations and EGFR pathway alterations [11], which may interact differently with statin-induced modulation of signalling pathways compared to prostate cancer, where androgen receptor signalling and lipid metabolism are more prominent [12]. These molecular differences may partly explain why statins show anti-tumour effects in some cancers but not others. Additionally, factors such as the tumour microenvironment, immune modulation, and variations in statin lipophilicity and dosing could further contribute to the observed variability in outcomes [11, 12].
Patient characteristics (e.g., demographics, obesity, or smoking), cardiovascular conditions, comorbidities, and patient compliance also play significant roles [7, 17, 27, 29, 34]. Age is a crucial factor, as ischemic heart disease is more common in older patients [44] In some studies, statins users were significantly older [28] and had more comorbidities [7, 28]. In contrast, another study found that statin users had better disease characteristics, such as lower initial prostate-specific antigen levels [18], which may have impacted survival outcomes. Although some studies used propensity score matching or demographic analysis, they focused on cancer treatment effects, not statins [14, 19, 21, 31]. The duration of statin use is crucial, as cardiovascular benefits typically appear within a year, with significant effects after 3–4 years. Long-term benefits might result from cardiovascular effects rather than anti-cancer properties, and patients with certain cancers might not live long enough to experience these advantages [45].
Despite limited evidence, our study found that statin use is associated with higher overall survival in oesophageal SCC, head and neck SCC, glioblastoma, and prostate cancer. Previous studies suggest statins may benefit hormone-dependent cancers [10], such as prostate cancer after radical prostatectomy [46] or androgen deprivation therapy [47], and breast cancer undergoing various treatments [48, 49]. Statin users can benefit from the cholesterol-lowering effects, as cholesterol is a precursor to steroid hormones such as oestrogen and androgen, which play a role in developing various malignancies [10] However, statin use was associated with poorer outcomes in brain metastases patients, likely due to the worse prognosis of their cancer [33].
Furthermore, past studies have proposed a dose-response relationship, which is supported by two studies in our review: higher cumulative doses and intensities of statins are linked to lower oesophageal SCC-specific mortality during chemoradiotherapy [31] and higher overall survival in patients with NSCLC undergoing curative radiotherapy [26]. However, many included articles did not specify statin intensity or dosage, preventing a detailed analysis of this correlation. Consequently, only non-significant results were found regarding dose and overall survival rate.
Long-term statin therapy reduces major cardiovascular disease in patients with hypercholesterolemia [50, 51], but contrasting findings emerged in this review. Statin users with NSCLC, on the contrary, showed a significantly higher risk of major adverse cardiac events [34], whereas those with nasopharyngeal carcinoma had a lower rate of ischemic stroke [14]. Although statin users with head and neck SCC presented significantly more ≥ grade 2 mucositis, it was only reported by one study with a very wide 95%CI [43]. Other radiotherapy-related side effects associated with statin use were mainly non-significant or underreported in the studies included. Notably, this study found statin use was linked to reduced radiotherapy-related rectal toxicity in patients with prostate cancer, aligning with previous research on pravastatin’s potential to mitigate radiation proctitis [52].
This review systematically synthesised contemporary evidence using meta-analysis to investigate the impact of statin use on survival outcomes in patients with cancers undergoing radiotherapy, providing a comprehensive overview beyond individual studies. Meta-regression analysis examined the relationships between cancer type, statin intensity, and overall survival rates, aiming to identify relevant factors. However, the study is limited by confounding variables, including cancer type, stage, cardiovascular health, statin characteristics (type, dose, and duration), adherence, and follow-up period. Retrospective study designs may inadequately control for these factors, potentially introducing bias into the findings - heterogeneous reporting of adverse events restricted pooled meta-analysis. Furthermore, despite including two randomised clinical trials, both exhibited a high risk of bias, necessitating cautious interpretation of the study’s conclusions.
In the context of patients with cancers receiving radiotherapy, this study did not find a significant impact of statin use or intensity on overall survival outcomes. However, the analysis revealed an association between overall survival and specific types of cancer. Notably, statin users showed reduced rates of ischemic stroke in nasopharyngeal carcinoma and lower rectal toxicity in prostate cancer compared to non-users.
Based on these findings, several actionable clinical recommendations can be considered. For cancers such as prostate cancer, where evidence suggests potential benefits, clinicians might consider evaluating the use of statins as an adjunct to standard therapies, particularly in patients who have existing indications for lipid management or cardiovascular risk reduction. In head and neck squamous cell carcinoma (SCC), caution is warranted, and the decision to initiate or continue statins should involve a multidisciplinary assessment, considering factors such as tumour stage, patient comorbidities, and potential drug interactions.
In practice, for patients already receiving statins for cardiovascular indications, continuing therapy during radiotherapy appears reasonable, given the potential benefits and the importance of managing cardiovascular risk. In cases where statins are being considered solely for potential oncological benefit, personalised assessment of the risk-benefit ratio is essential, factoring in tumour type, molecular profile, and individual patient health status. Tailoring statin intensity and duration, starting with moderate doses and adjusting based on response and tolerability, may optimise outcomes while minimising adverse effects.
Furthermore, the variability in toxicity and cardiovascular outcomes across different tumour types underscores the importance of integrated cardio-oncology care. Future research, particularly prospective trials, is critical to identify specific patient subgroups, such as those with hormone-sensitive tumours like prostate cancer or specific molecular alterations, who may derive the most benefit from adjunctive statin therapy. Establishing evidence-based guidelines will ultimately facilitate more precise and effective utilisation of statins in oncology settings.
Future research is needed to explore molecular and mechanism-based biology to elucidate these findings further and enhance clinical understanding. Although randomised controlled trials are regarded as the best evidence to clarify the impact of statins on cancer radiotherapy, potential ethical and recruitment challenges are expected in patients with cancer. Alternatively, well-designed prospective cohort studies could offer valuable insights into statins’ influence, aiding causal inference. Our findings underscore the importance of refining inclusion criteria related to cardiovascular disease, cancer stage, statin characteristics (type, intensity, and duration), and follow-up period using propensity score matching to mitigate confounding bias.
Conclusions
Clinically, while concurrent statin use did not significantly affect survival outcomes in cancer radiotherapy, clinicians may consider potential overall survival benefits in patients with oesophageal SCC, head and neck SCC, glioblastoma, and prostate cancer. Moreover, statin use may be associated with reduced rates of ischemic stroke in nasopharyngeal carcinoma and lower rectal toxicity in patients with prostate cancer. These findings highlight avenues for future research to explore and optimise statin therapy in the context of cancer treatment.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The National Institute for Health and Care Excellence. Cardiovascular disease: risk assessment and reduction, including lipid modification. 2023. Available from: https://www.nice.org.uk/guidance/ng 238/chapter/recommendations#low-intensity-statin 32200592 · pubmed ↗