Isolated tricuspid Libman–Sacks endocarditis in a patient with systemic lupus erythematosus and antiphospholipid syndrome: case report
Gamaliel Alejandro Velasquez-Orozco, Yancy Yuliana Erazo-Dorado, Juan Carlos Rivera Guerrero, Felipe Israel Lopez Trejo, Elias Noel Andrade-Cuellar

TL;DR
A rare case of tricuspid Libman–Sacks endocarditis in a patient with lupus and antiphospholipid syndrome is described, emphasizing diagnostic and treatment strategies.
Contribution
Highlights the rare occurrence of isolated tricuspid LSE and the use of 3-D echocardiography to guide surgical decisions in SLE/APS patients.
Findings
3-D vena-contracta area measurement confirmed massive tricuspid regurgitation despite conflicting 2-D results.
Tricuspid valve replacement with a bioprosthesis was successfully performed after a recent subarachnoid hemorrhage.
Multimodal imaging and Heart Team collaboration improved outcomes in a complex autoimmune endocarditis case.
Abstract
Libman–Sacks endocarditis (LSE) is an immune-mediated, culture-negative valvulopathy complicating systemic lupus erythematosus (SLE) and often amplified by antiphospholipid syndrome (APS). Although classically left-sided, isolated tricuspid involvement is rare. Advanced three-dimensional (3-D) quantification refines tricuspid regurgitation (TR) grading and informs surgical timing. A 41-year-old woman with 2-year SLE and triple-positive secondary APS presented with 2 weeks of fever, migratory arthralgia, and a small non-traumatic subarachnoid haemorrhage (SAH). Serial blood cultures were negative. Transthoracic echocardiography showed multiple heterogeneous vegetations (largest 20 × 12 mm) on all tricuspid leaflets; 2-D PISA-EROA was 30 mm², while 3-D vena-contracta area (VCA) measured 0.95 cm², indicating massive TR. Cardiac computed tomography corroborated leaflet thickening and poor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
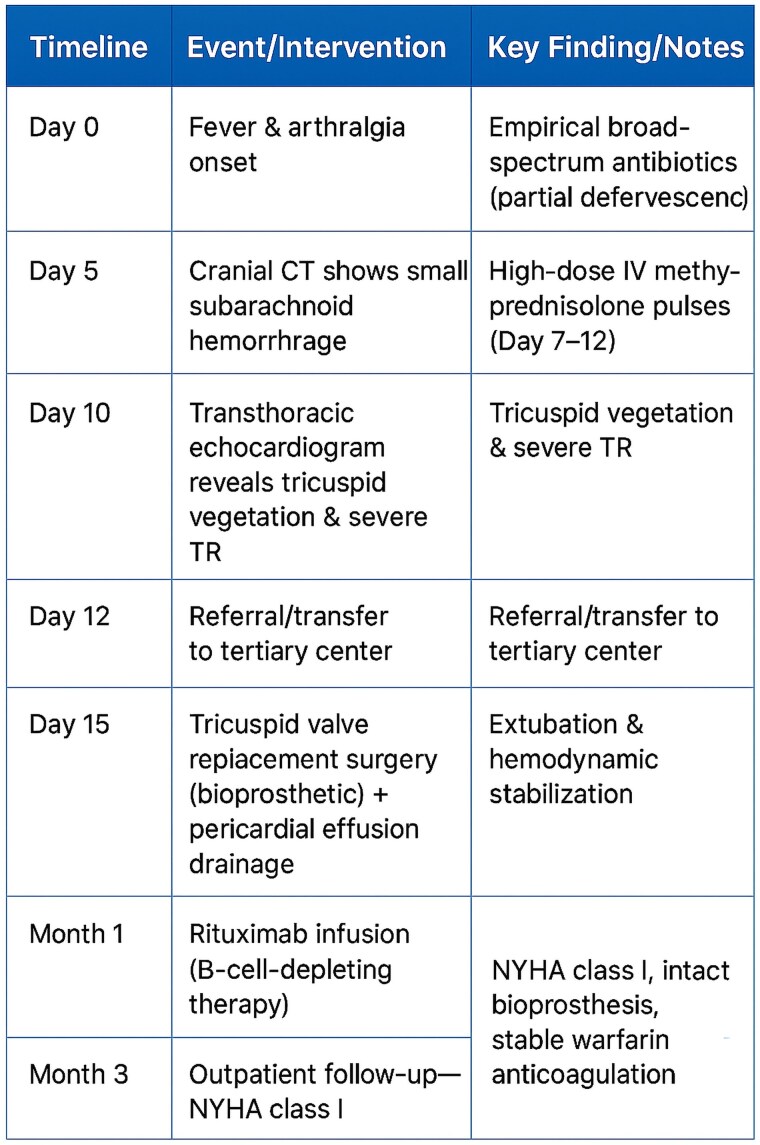 Figure 1
Figure 1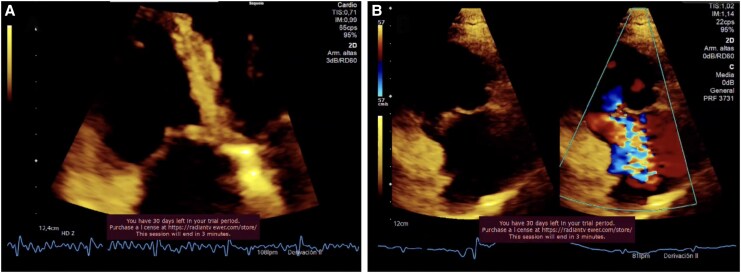 Figure 1
Figure 1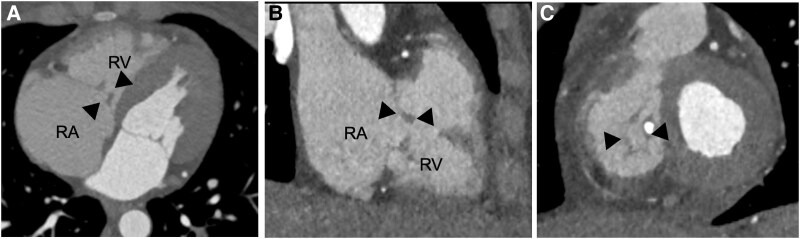 Figure 2
Figure 2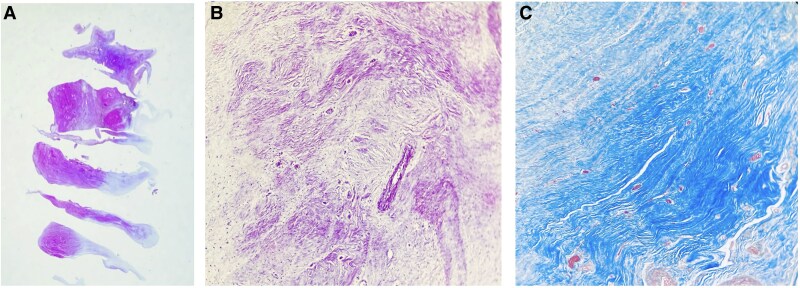 Figure 3
Figure 3| Author, year | Age/sex | APS | Clinical presentation | Echo severity | Management | Outcome |
|---|---|---|---|---|---|---|
| Mahajan 2017 | 34 F | Yes | Severe TR, dyspnoea | Torrential | TVR (bioprosthesis) | NYHA I at 12 mo |
| Unic 2017 | 60 F | Yes | Fever, emboli | Severe | TVR (mechanical) | NYHA II at 6 mo |
| Moaref 2010 | 29 F | No | Incidental murmur | Moderate | Medical | Stable at 3 yr |
| Zurick 2007 | 45 F | Yes | Right-HF/paradoxical embolism | Massive | Repair | Asymptomatic 18 mo |
| Migliorini 2022 | 38–45 F | Yes | Severe TR (pregnancy) | Torrential | TVR | NYHA I 6 mo |
| Vacca 2023 | 26 F | Yes | Acute presentation | Severe | TVR (not specified) | Good short-term |
| Bai 2015 | 20 F | SLE (±APS) | Acute RHF | Severe | TVR (bioprosthesis) | Good early |
- —Universidad Nacional Autónoma de México10.13039/501100005739
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood disorders and treatments · Platelet Disorders and Treatments · Immunodeficiency and Autoimmune Disorders
Introduction
Libman–Sacks endocarditis (LSE) is the most prevalent cardiac manifestation of systemic lupus erythematosus (SLE). Sterile platelet–fibrin vegetations develop on damaged endothelium and undergo immune-complex deposition and fibrous organization that ultimately distort valvular architecture and function.^1–3^ Although the mitral and aortic valves are most often affected, isolated tricuspid involvement is exceptionally rare, with scattered case reports over the last three decades.^4–9^ The coexistence of antiphospholipid syndrome (APS) is a key accelerator of valvular injury—promoting leaflet thickening, sterile vegetations, embolism, and faster progression to haemodynamically significant regurgitation.^10^
Echocardiographic surveys of unselected SLE cohorts report valvular abnormalities in up to 50%, yet true LSE vegetations are visualized in only 4%–11% on transthoracic imaging; sensitivity improves with transoesophageal and three-dimensional techniques.^1–3^ Clinically, most lesions remain silent, but a meaningful subset—particularly those with high-titre antiphospholipid antibodies—develops severe regurgitation or thromboembolic complications that may warrant surgery.^1,10^ In contemporary practice, advanced quantification such as three-dimensional vena-contracta area (VCA) helps reconcile discrepant two-dimensional measures and better reflects the actual regurgitant burden, especially in noncircular or dynamic orifices typical of tricuspid regurgitation.^4,11^
We present a rare case of isolated tricuspid LSE producing massive regurgitation, outline multidisciplinary decision-making and perioperative strategy, and integrate updated evidence on imaging, APS-related risk, and indications for intervention.
Summary figure
**
Case presentation
A 41-year-old woman with a 2-year history of SLE and triple-positive secondary APS (on azathioprine) was admitted after two weeks of intermittent fever, migratory arthralgia, and myalgia. Broad-spectrum antibiotics given elsewhere failed to achieve defervescence. On Day 7, she developed headaches; cranial computed tomography (CT) demonstrated a small non-traumatic subarachnoid haemorrhage (SAH).
Initial laboratory work-up revealed bicytopenia attributable to active SLE. Pulse methylprednisolone (1 g day⁻¹ for 3s days) was started, yet fevers persisted and repeated blood cultures were negative. Transthoracic echocardiography (TTE) identified multiple heterogeneous masses on all three tricuspid leaflets—the largest 20 × 12 mm—with an effective regurgitant orifice area (EROA) by 2-D PISA of 30 mm² and a regurgitant volume of 26 mL, suggestive of at least moderate–severe regurgitation.
On transfer to our tertiary centre, she was afebrile but displayed jugular venous distension and a holosystolic murmur accentuated by inspiration. Repeat TTE confirmed right-sided volume overload and normal left ventricular ejection fraction (55%). Three-dimensional vena contracta area (3-D VCA) was 0.95 cm² (Figure 1 and Supplementary material online, Videos 1 and 2), classifying the lesion as massive tricuspid regurgitation under the extended grading system of Utsunomiya et al. (massive ≥ 0.75–<1.0 cm²). Cardiac CT angiography excluded coronary disease and corroborated irregular thickening of the tricuspid leaflets (Figure 2).
Transthoracic echocardiogram with a four-chamber view focusing on the right ventricle (A) and the right ventricular inflow tract (B). Thickening of the septal leaflet of the tricuspid valve with severe regurgitation is observed. RV, right ventricle.
Cardiac computed tomography in four-chamber view (A), two-chamber view (B), and short-axis view (C). Dilation of the right-sided chambers, including the right atrium and right ventricle, is noted (A). The arrows indicate significant thickening of all three leaflets, with calcification of the septal leaflet and central coaptation defect. RA, right atrium; RV, right ventricle.
Considering the recent SAH, transoesophageal echocardiography (TEE) was deferred. A Heart Team (cardiology, cardiac surgery, rheumatology, neurology) favoured LSE over infective endocarditis owing to sterile cultures, APS background, and imaging findings. Corticosteroids were tapered to physiologic dose and surgery was electively scheduled 21 days after the SAH, in accordance with current guidance to delay cardiopulmonary bypass 2–4 weeks after minor intracranial bleeding.
The patient underwent tricuspid valve replacement with a 31-mm bovine pericardial bioprosthesis. Cardiopulmonary bypass was conducted with standard heparinization (activated clotting time target ≈380 s) and intra-operative antifibrinolytic therapy (tranexamic acid). Inspection revealed friable vegetations on all three native leaflets and a 400-mL serous pericardial effusion. Histopathology confirmed sterile platelet–fibrin vegetations, consistent with LSE (Figure 3).
(A) Haematoxylin-eosin staining of the tricuspid valve. (B) Negative Gram stain showing no evidence of microorganisms. (C) Masson’s trichrome staining revealing fibrohyaline degenerative changes (blue deposits).
Post-operative recovery was uneventful; fever resolved and right-sided pressures normalized. Warfarin (target INR 2.5–3.5) was begun and bridged with unfractionated heparin. Persistent serological activity (high anti-dsDNA, low complement) at 1 month prompted B-cell depletion with rituximab plus hydroxychloroquine and tapering prednisone.
At 3-month follow-up, the patient was asymptomatic (NYHA class I). Transthoracic echocardiography showed a competent prosthetic valve with normal right-sided dimensions and no recurrent vegetations.
Discussion
Libman–Sacks endocarditis is the most frequent valvular manifestation of SLE and results from endothelial injury with immune-complex deposition and sterile platelet–fibrin thrombi that can distort valve architecture and embolize. Although left-sided valves predominate, isolated tricuspid involvement is exceptional and has been documented mainly as case reports across the last decades (see Table 1). The clinical spectrum ranges from incidental murmur to right-sided heart failure, culture-negative fever, or embolic events and is observed predominantly in women with SLE/APS, consistent with our patient.^1–3,10^
Distinguishing LSE from infective endocarditis is critical because management and prognosis diverge. In LSE, blood cultures are typically negative; vegetations tend to be sessile/heterogeneous and often multiple; and autoimmune/APS activity is common. Three-dimensional TEE (3-D TEE) improves detection of small lesions and defines their relationship to the subvalvular apparatus, while cardiac CT offers complementary anatomic information when TEE is deferred (e.g. after recent intracranial haemorrhage), as in this case.^1^
Two-dimensional measures (e.g. PISA-based EROA) may underestimate tricuspid regurgitation (TR) severity when the regurgitant orifice is noncircular and dynamic. Three-dimensional vena-contracta area (3-D VCA) correlates better with true regurgitant burden and has enabled extended grading (including ‘massive’ and ‘torrential’). In our patient, a 3-D VCA of 0.95 cm² reclassified the lesion as massive TR despite a modest 2-D EROA (30 mm²), supporting surgical referral.^4,11^
The 2021 ESC/EACTS and 2020 ACC/AHA guidelines support intervention for symptomatic isolated TR of massive or greater severity, irrespective of aetiology, with Heart Team deliberation to individualize timing and strategy—particularly when autoimmune and neurovascular issues coexist.^5,6^ In the present case, the combination of large right-sided vegetations, haemodynamically significant TR, and right-sided volume overload prompted surgical management once neurovascular risk was acceptable.
Tricuspid repair is preferable when feasible; however, in LSE, the diffuse leaflet thickening, friability, and destruction often preclude durable repair. Comparative evidence specific to tricuspid valve replacement (TVR) shows no survival advantage of mechanical over bioprosthetic valves at 30 days or long term, while highlighting the vulnerability of mechanical prostheses to valve-related events (thrombosis/embolism/bleeding) in the low-flow right heart. Contemporary bioprostheses demonstrate acceptable durability in this position. Even in patients who already require lifelong anticoagulation for APS, a bioprosthesis may mitigate tricuspid-position thrombosis risk while systemic anticoagulation is maintained for APS. Our decision reflected non-repairable anatomy, the lower thrombogenicity of bioprostheses at the tricuspid position, and the need for vitamin K antagonist (VKA) therapy for APS regardless of prosthesis type.^7,8^
In high-risk (triple-positive) APS, EULAR 2019 recommendations favour VKA—INR target 2–3 (or 3–4 in selected arterial events)—and advise against routine DOAC use. The TRAPS trial in triple-positive APS was stopped early due to excess events with rivaroxaban vs. warfarin. In the context of bioprosthetic TVR, valvular guidelines recommend VKA for at least the first 3 months; in our patient, APS warranted indefinite VKA irrespective of prosthesis type.^5,6,9,12^
Cardiac surgery with cardiopulmonary bypass (CPB) after recent intracranial haemorrhage carries a risk of rebleeding. Contemporary neuro–cardiac literature supports deferring ∼2–4 weeks when clinically feasible, guided by serial neuroimaging and meticulous intraoperative anticoagulation protocols. We delayed 21 days after a small, stable SAH, used standard heparinization (target ACT ≈ 380 s) and tranexamic acid, and observed no rebleeding—consistent with multicentre and systematic data.^13,14^
Long-term immunomodulation and surveillance
Beyond the success of surgery, disease control is essential to reduce inflammatory activity and the risk of new valvular lesions. Corticosteroids, hydroxychloroquine, and B-cell depletion with rituximab have been associated with improved disease control and, in case series, lower recurrence. Given the possibility of subclinical recurrence, we recommend serial imaging (TTE ± 3-D/TEE) at 6–12 months to assess prosthetic integrity and screen for new lesions, along with lifelong VKA in APS.^1–3,10^
Clinical implications
This case underscores three practical messages: (i) maintain a high index of suspicion for LSE in SLE/APS patients with culture-negative right-sided vegetations; (ii) use 3-D VCA to reconcile discrepant 2-D metrics and substantiate surgical indications; and (iii) after recent SAH, timed surgery with careful anticoagulation and selection of a bioprosthesis in the tricuspid position can achieve excellent outcomes when integrated with long-term anticoagulation and modern immunomodulation.
Key take-home messages
Isolated tricuspid LSE should be considered in culture-negative right-sided endocarditis with autoimmune features; 3-D quantification can alter management; and integrated Heart Team care enables timely surgery, pragmatic selection of a bioprosthesis to minimize tricuspid-position thrombosis, lifelong VKA for APS, and sustained immunomodulation to prevent recurrence.
Conclusion
Isolated tricuspid LSE is a rare but treatable entity. Early Heart Team evaluation, multimodality imaging and timely surgery—combined with tailored immunosuppression and lifelong anticoagulation—can achieve excellent functional recovery and prevent thromboembolic complications.
Lead author biography
Dr Gamaliel Alejandro Velasquez-Orozco is a cardiology fellow at the National Medical Center ‘20 de Noviembre’, affiliated with the National Autonomous University of Mexico (UNAM). He completed his residency in internal medicine at Hospital General San Juan de Dios in Guatemala City, under the Universidad de San Carlos de Guatemala. His clinical and research interests include advanced heart failure, cardiac imaging, and coronary syndromes
Supplementary Material
ytaf493_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roldan CA, Tolstrup K, Macias L, Qualls CR, Maynard D, Charlton G, et al Libman-sacks endocarditis: detection, characterization, and clinical correlates by three-dimensional transesophageal echocardiography. J Am Soc Echocardiogr 2015;28:770–779.25807885 10.1016/j.echo.2015.02.011PMC 4592775 · doi ↗ · pubmed ↗
- 2Moyssakis I, Tektonidou MG, Vasilliou VA, Samarkos M, Votteas V, Moutsopoulos HM. Cardiac involvement in systemic lupus erythematosus: a three-year prospective study. Rheumatology 2007;46:1765–1768.
- 3Zavaleta ME, Montenegro-Rodríguez J, Flores-Montejano E, Campos-Caro D, García-Rodríguez A, Ríos-Mercado M. Echocardiographic findings in systemic lupus erythematosus: a prospective study. Eur J Echocardiogr 2017;18:1149–1156.
- 4Utsunomiya H, Itabashi-Takahashi N, Kakuta T, Morita Y, Komatsu M, Kaneko M, et al Three-dimensional vena-contracta area for grading tricuspid regurgitation. J Am Soc Echocardiogr 2019;32:1213–1222.
- 5Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 6Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, Gentile F, et al 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol 2021;77:e 25–e 197.33342586 10.1016/j.jacc.2020.11.018 · doi ↗ · pubmed ↗
- 7Negm S, Jepson N, Hancock J, Ingram SO, Summers R, Brothers K, et al Bioprosthetic versus mechanical tricuspid valves: a systematic review and meta-analysis. Heart Lung Circ 2021;30:1193–1201.33229238 10.1016/j.hlc.2020.03.011 · doi ↗ · pubmed ↗
- 8Roberts WC, Ko JM, Chang S, Vinteiro R, Choi JW, Singal GP, et al Thrombosis in mechanical tricuspid valve prostheses: clinicopathologic correlations. Am J Cardiol 2020;125:115–121.