Surgical Outcome of Tethered Cord Syndrome Following Duplicate Filum Terminale Externum Resection in a Patient With Normal Conus Medullaris and Fatty Filum: A Case Report
Vanni Veronesi, Camilla Mencarani, Gianluca Bizzocchi, Carlo Sacco

TL;DR
A woman with tethered cord syndrome showed improved symptoms after multiple surgeries to address anatomical variations in her spinal cord.
Contribution
This case highlights the importance of recognizing anatomical variations like duplicated filum terminale in surgical treatment of tethered cord syndrome.
Findings
Symptoms resolved temporarily after initial surgery but recurred, necessitating further intervention.
Sectioning the intradural fatty filum led to long-term symptom resolution.
Anatomical variations like duplicated filum terminale can limit minimally invasive surgical outcomes.
Abstract
We describe the case of a 38-year-old woman who limped due to a forced antalgic posture involving plantar flexion of the left foot. She exhibited hypoesthesia on the posterior aspect of the left lower limb. The lumbar MRI showed the conus medullaris in a normal position and a fatty filum (FF) extending from L3 to L5, with a maximum diameter of 5.5 mm at L3. A transhiatal approach was performed to section the filum terminale externum (FTE) to achieve spinal cord untethering, and a duplicated FTE was found. The symptoms disappeared immediately but recurred several months later. A second surgical approach was undertaken through a partial sacrectomy via S1-S2 laminectomy, as the section of the FTE did not reveal any other anatomical variants apart from the duplicated FTE, which was sectioned near the inferior part of the dural sac. The symptoms temporarily resolved, but after a few months,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
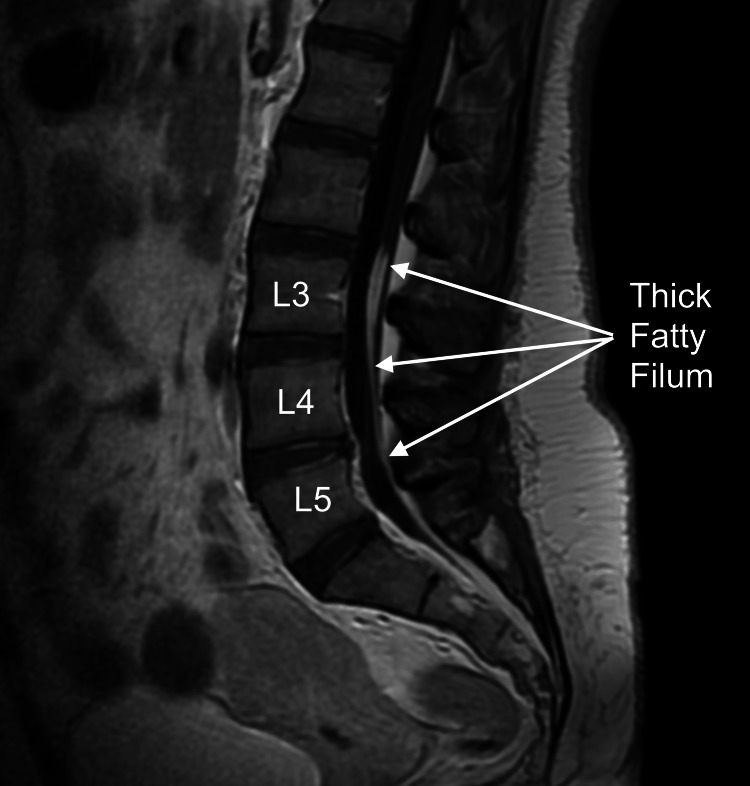 Figure 1
Figure 1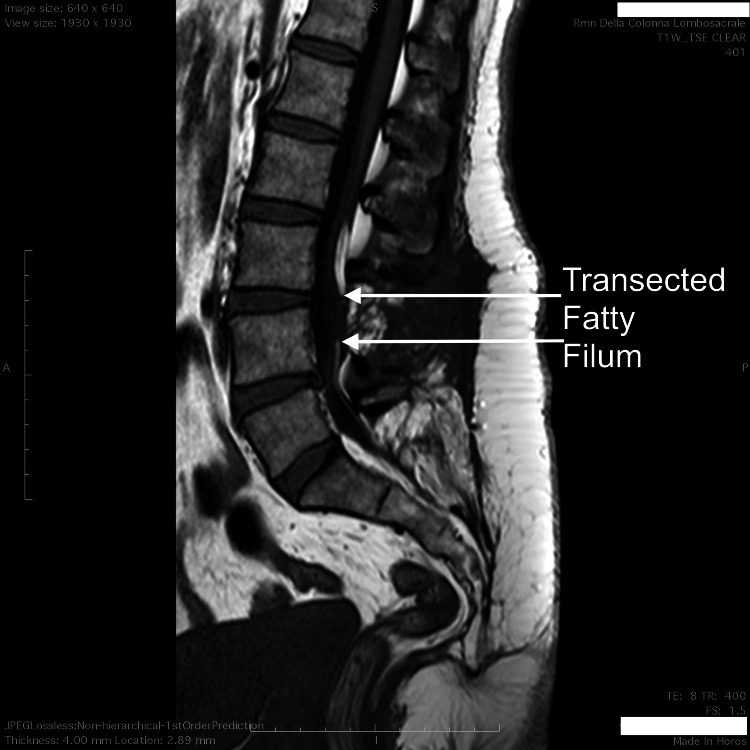 Figure 2
Figure 2| Author/ | Age years | Sex | Symptoms | FF | Level of Conus | SCM | Surgery | Outcome |
| Year | ||||||||
| Current Case | 38 | F | Patient limps due to paroxysmal pain in her left leg. Numbness and hypoesthesia in her left leg. | Yes (no duplicate FTI) | Upper part of L2 | No | Sectioning of duplicate FTE | Symptoms disappeared |
| Recurrence of symptoms with tension and stiffness radiating from her lower back to both thighs, but her gait is normal. | Reoperation for sectioning of FF | Symptoms disappeared | ||||||
| Xu et al., 2020 [ | 45 | F | Numbness in both legs and paroxysmal leg pain | No | L5-S1 disk | Yes | Sectioning of duplicate FTI | Symptoms disappeared |
| Milic et al., 2019 [ | 3 | F | Spondylocostal dysostosis, gate disturbance, urinary incontinence | No | L4 | Yes | Duplicate FTI. Her parents refused a surgical intervention | - |
| Davanzo et al., 2016 [ | 43 | M | Lower back pain, atrophy of left calf | No | L5-S1 disk | No | Sectioning of duplicate FTI. Reoperation for repair pesudomeningocele | Significantly improved |
| Starnoni et al., 2016 [ | 47 | M | Lower back and leg pain, gait unsteadiness | One of the duplicate FTI | L3-4 disk | No | Sectioning of duplicate FTI | Improved |
| Rizk et al., 2014 [ | 8 | NM | Asymptomatic | One of the duplicate FTI | NM | No | Sectioning of duplicate FTI | NM |
| 5 | NM | Asymptomatic | Both duplicate FTI | NM | No | Sectioning of duplicate FTI | NM | |
| Salbacak et al., 2000 [ | NA | NM | NM (aborted fetus) | - | NM | NM | - | - |
| NA | NM | NM (aborted fetus) | - | NM | NM | - | - | |
| NA | NM | NM (aborted fetus) | - | NM | NM | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Spinal Cord Injury Research · Family and Disability Support Research
Introduction
Tethered spinal cord syndrome is a neurological disorder caused by an abnormal stretching of the spinal cord. Clinically, patients with tethered cord syndrome (TCS) display three groups of symptoms, which do not necessarily occur together: progressive back and leg pain, sensorimotor deficits in the lower limbs, and bowel and bladder dysfunction [1,2].
Previously, TCS was often diagnosed in children, and in the meantime, adult-onset cases were thought to be rare. In recent years, TCS has been diagnosed in an increasing number of adults. In a recent comprehensive systematic review with more than six thousand cases of TCS in pediatric and adult patients, surgical treatment involved a higher percentage of clinical improvement in adults, but also a higher complication rate in adults [1].
For the treatment of TCS, classic surgery involves sectioning of the filum terminale internum (FTI) under general anaesthesia [1,2]. Recently, a new surgical technique was introduced: the sectioning of the filum terminale externum (FTE). The initial description involved accessing the FTE via sacrectomy under general anaesthesia [3], but later, a minimally invasive technique using local anaesthesia with a transhiatal approach was developed [4,5]. Currently, no time-limiting effects on the effectiveness of FTE have been reported; none of the FTE patients previously documented in the medical literature have exhibited fatty filum (FF).
We report the case of a patient with both FF and FTE.
Case presentation
A 38-year-old woman presented with persistent low back pain for six years. One year before our assessment, she experienced lumbar trauma. For approximately eight months, she experienced pain and paresthesia resembling an electric shock in the lumbar region and the left lower limb, which caused her left foot to extend onto the ground and led to difficulty walking.
On examination, the patient, in the supine position, could not dorsiflex her left foot due to pain in the lower back and left lower limb; she was unable to raise her left leg, and she could only bend her left thigh if she lay on her left side. She experienced hypo-anaesthesia in the posterior part of the left lower limb. Normal conus medullaris and FF were found on lumbar MR (Figure 1).
Lumbar magnetic resonance imaging. Sagittal T1-weighted image. Fatty filum extending from L3 to L5, with a maximum diameter of 5.5 mm at L3.
A month after her presentation, the patient underwent transhiatal transection of the FTE under local anesthesia with conscious sedation. The sectioning and removal of the superficial dorsal sacrococcygeal ligament provided access to the sacral canal, where the FTE was identified, dissected, and cut using an operating microscope. Deeper within, an abnormal and thin membrane was found inside the sacral canal. This membrane was opened, and another FTE was coagulated and cut. The day after the surgery, the patient showed a dramatic improvement. She was able to walk normally, and there were no limitations in the movements of the left lower limb (Video 1).
Transhiatal approach preoperative and postoperative assessment
She also experienced no pain in the left lower limb. Her well-being continued for about three months, until, following an abrupt twisting movement of the trunk, lumbago and pain in the left lower limb reappeared, almost as before the surgery. There were no improvements at the follow-up, so a second surgery was performed eight months after the first under general anaesthesia. A partial sacrectomy via S1-S2 laminectomy was carried out, confirming a duplicate FTE and ruling out other anatomical variants that could limit the outcome of the transhiatal approach. The duplicate FTE of equal thickness has been identified up to the inferior part of the dural sac. The duplicate FTE was sectioned (Video 2), and each piece was sent for pathology; no fat tissue was found. The symptoms disappeared immediately after surgery.
Surgical videoSection of duplicate filum terminale externum by partial sacrectomy
The patient remained asymptomatic for a few months after surgery. Then she began to develop symptoms different from her initial presentation, involving both thighs. These symptoms were mild but increased after lifting a weight. The patient walked normally and no longer limped as she did at the onset. She reported tension and stiffness radiating from the lower back to the thighs. While sitting on the bed, she was unable to lift her thighs. However, she did not experience any limitations or pain in plantar flexion and dorsiflexion movements. In a supine position with her legs straight, she could not raise them. The thighs could be rotated laterally, but the movement was reduced on the left side.
Almost two years after the second surgery, the FF section was carried out using a laminectomy approach at L4. There was no duplicate FTI. Immediately in the postoperative assessment, there were no limitations in lower limb movements and no symptoms (Video 3).
Section of fatty filum preoperative and postoperative assessment
Postoperative lumbar MRI revealed the cut of the FF (Figure 2).
Lumbar MRI after section of the fatty filum.The conus medullaris does not ascend after fatty filum sectioning, but the patient becomes asymptomatic.
At the five-year follow-up, the patient only occasionally experienced low back pain and transient episodes of pain in the left lower limb without any restriction of movement.
Discussion
Potential complications of traditional surgery by the FTI section under general anaesthesia, including the FF section, are related to the development of permanent intestinal or bladder deficits, new neurological deficits, cerebrospinal fluid leaks, pseudomeningocele, cauda equina tethering, and conus medullaris tethering, which might require additional surgical procedures [1,2]. Wound healing problems and meningitis can also occur, with associated morbidity and mortality. The list is extensive, but the incidence of such complications remains very low. The surgical procedure lasts approximately ninety minutes, and to reduce neurological complications, intraoperative electrophysiological monitoring is recommended, which extends the duration of general anaesthesia. Patients stay in the hospital for two to three days.
When we use minimally invasive surgery with a transhiatal approach in local anaesthesia for the FTE section, the potential complications are limited to wound healing issues. In case of infection, there is no risk of meningitis, with its associated morbidity and mortality, because the meninges are absent at the operative site. The surgery is brief, lasting about 30 minutes, and allows quick patient mobilisation within a few hours. The patient can be discharged on the same day or the next.
A study on fresh-frozen cadaveric specimens concluded that FTE sectioning might not be effective in treating spinal cord untethering in patients with tethered cord syndrome [6]. Veterinary literature reports multiple cases of FTE sectioning in dogs with excellent outcomes [7,8]. One study has shown remarkable results using pre- and post-operative videos [9]. The medical literature reports the sectioning of the FTE in a small group of patients using either the transhiatal [4,5] or sacrectomy [3] approaches. In one case, both the FTE and FTI were sectioned [10]. Currently, no time-limiting effects on the effectiveness of FTE have been reported; none of the patients previously documented in the medical literature have exhibited FF.
Duplicate FTI is rare, with only six cases documented [11-15]. An additional three cases were identified in medically or spontaneously aborted fetuses [16]. No duplicate FTI associated with a duplicate FTE was observed in our case. Table 1 shows the comparison between the results of this study and other previously published literature on duplicated filum terminale. No patient with a duplicate FTE has been reported in the literature, and no duplicate FTE was found in the anatomical studies of cadavers [17-21]. In our personal experience, this is the only case of a duplicate FTE in the more than 400 patients we have operated on (unpublished data).
In this case, two approaches were adopted for the FTE section to exclude other anomalies or divisions at the level of the FTE emergence from the dural sac that could not be assessed with the initial transhiatal approach. Still, no anatomical variants other than the duplication were identified. The initial clinical picture, characterised by symptoms distal to the left lower limb with significant difficulty walking, disappeared after the FTE section. Subsequently, the residual subclinical spinal cord traction later became clinically evident when there was a sudden traction of the spinal cord caused by the abrupt twisting of the spinal canal or after lifting a weight. When the symptoms returned, they were located proximal to the lower limbs, but this was accompanied by regular walking. In this case, the section of the FTE, in the presence of a very thick FF, did not allow for adequate release of the spinal cord to achieve definitive healing.
Conclusions
In this case, the potential limitations of the therapeutic capabilities of minimally invasive surgery for section FTE by transhiatal approach, related to the anatomical variation of the duplicate FTE, were eliminated by sectioning the duplicated FTE at the point where the dural sac emerges and by excluding the presence of a duplicate FTI during the section of the FF. The presence of the FF with significant thickness and extending from L3 to L5 is a limitation to the effectiveness of the FTE section in treating TCS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tethered cord syndrome from pediatric and adult perspectives: a comprehensive systematic review of 6135 cases Neurosurg Focus He K Wang K Liu Z 056202410.3171/2024.3.FOCUS 2389938823051 · doi ↗ · pubmed ↗
- 2Surgical treatment of tethered cord syndrome in adults: a systematic review and meta-analysis World Neurosurg O'Connor KP Smitherman AD Milton CK 041137202010.1016/j.wneu.2020.01.13132001403 · doi ↗ · pubmed ↗
- 3Results of the section of the filum terminale in 20 patients with syringomyelia, scoliosis and Chiari malformation Acta Neurochir (Wien) Royo-Salvador MB Solé-Llenas J Doménech JM González-Adrio R 51552314720051572315610.1007/s 00701-005-0482-y · doi ↗ · pubmed ↗
- 4Transhiatal approach to filum terminale externum sectioning in adult patient with tethered cord syndrome: case report Oper Neurosurg Veronesi V Sacco C Mastronicola C Staffa G 0415201810.1093/ons/opx 18828961973 · doi ↗ · pubmed ↗
- 5Prone position magnetic resonance imaging and transhiatal approach to filum terminale externum sectioning in adolescents with occult tethered cord syndrome: report of four cases Pediatr Neurosurg Veronesi V Calderone M Sacco C Donati R 4324385520203340127210.1159/000512471 · doi ↗ · pubmed ↗
- 6Mechanical relationship of filum terminale externum and filum terminale internum: is it possible to detether the spinal cord extradurally?Childs Nerv Syst Patel M Vetter M Simonds E 176717703420182979706310.1007/s 00381-018-3837-3 · doi ↗ · pubmed ↗
- 7Dynamic lumbosacral magnetic resonance imaging in a dog with tethered cord syndrome with a tight filum terminale Front Vet Sci De Decker S Watts V Neilson DM 134420172886830110.3389/fvets.2017.00134 PMC 5563312 · doi ↗ · pubmed ↗
- 8Tethered cord syndrome associated with a thickened filum terminale in a dog J Vet Intern Med De Decker S Gregori T Kenny PJ Hoy C Erles K Volk HA 4054092920152558655010.1111/jvim.12522 PMC 4858091 · doi ↗ · pubmed ↗