Prevalence of Multidrug-Resistant Gram-Negative Bacilli Causing Neonatal Sepsis: A Retrospective Study in a Tertiary Care Hospital From Eastern India
Rajesh K Dash, Santosh K Panda, Shradha Smriti, Swarupa Mohapatra, Ipsa Mohapatra, Nipa Singh, Dipti Pattnaik, Sushree S Behura, Soumini Rath, Manas K Nayak, Subhra Snigdha Panda

TL;DR
This study found that multidrug-resistant gram-negative bacteria are a major cause of neonatal sepsis in a hospital in India, with Klebsiella pneumoniae being the most common.
Contribution
The study provides updated prevalence data and antibiotic resistance patterns of MDR gram-negative bacilli causing neonatal sepsis in a specific region of India.
Findings
Klebsiella pneumoniae was the most prevalent MDR gram-negative isolate causing neonatal sepsis.
Low and very low birth weight neonates had a higher proportion of MDR infections.
Antibiotic susceptibility varied by bacterial species, with trimethoprim/sulfamethoxazole and gentamicin showing better efficacy for K. pneumoniae.
Abstract
Background: Neonatal sepsis is considered one of the major causes of morbidity and mortality in low and middle-income countries, with a rising burden of multidrug-resistant (MDR) gram-negative bacilli (GNB). The emergence of antimicrobial resistance (AMR) has significantly compromised treatment outcomes in neonatal intensive care units (NICUs). This study aimed to determine the prevalence, antibacterial susceptibility patterns, and associated risk factors of MDR GNB among septic neonates over a four-year period. Materials and methods: A retrospective study was carried out from January 2021 to December 2024 in a tertiary care health setting in India. Data regarding septic neonates were retrieved from NICU records, and culture details were retrieved from the LIS (laboratory information system). Blood and cerebrospinal fluid (CSF) samples from neonates with clinically suspected sepsis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
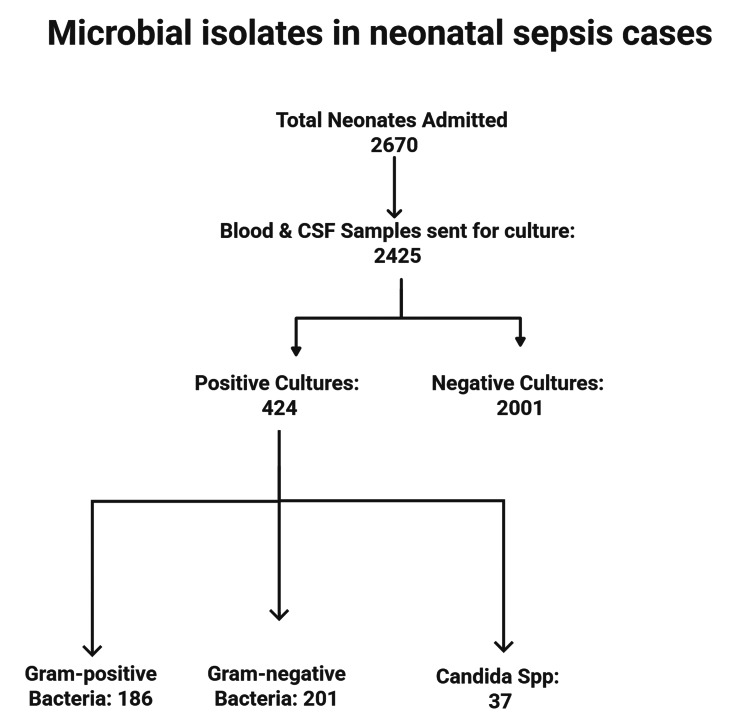 Figure 1
Figure 1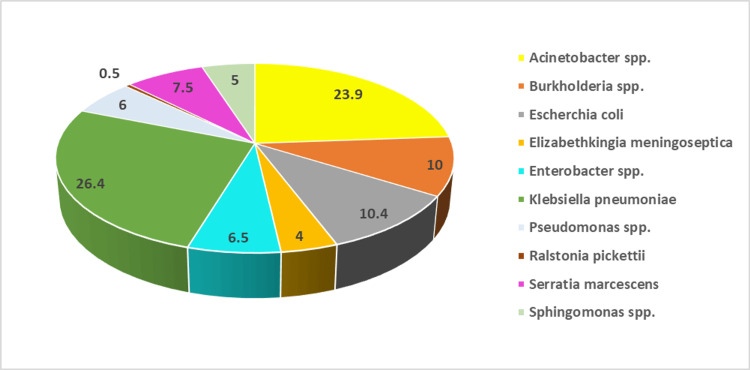 Figure 2
Figure 2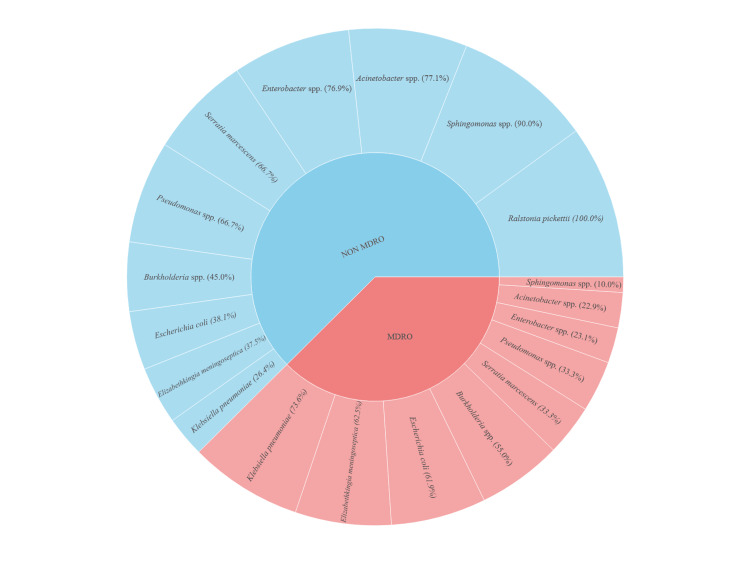 Figure 3
Figure 3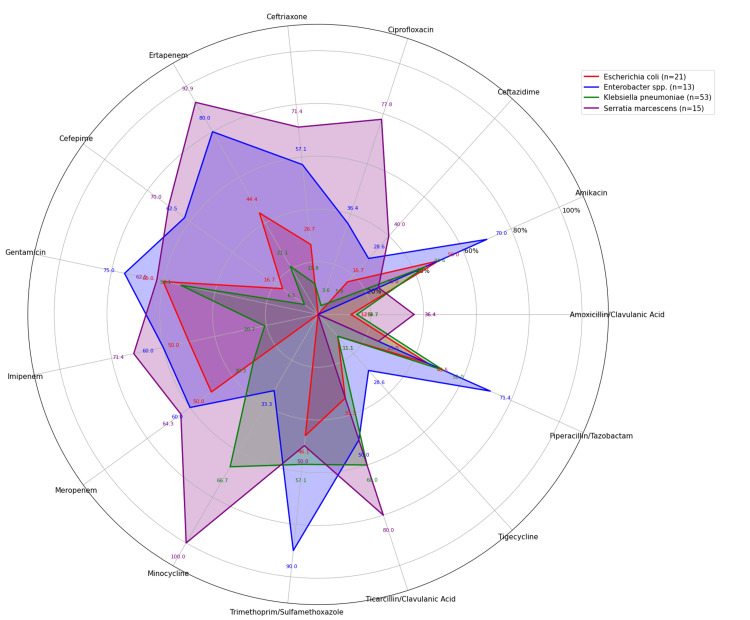 Figure 4
Figure 4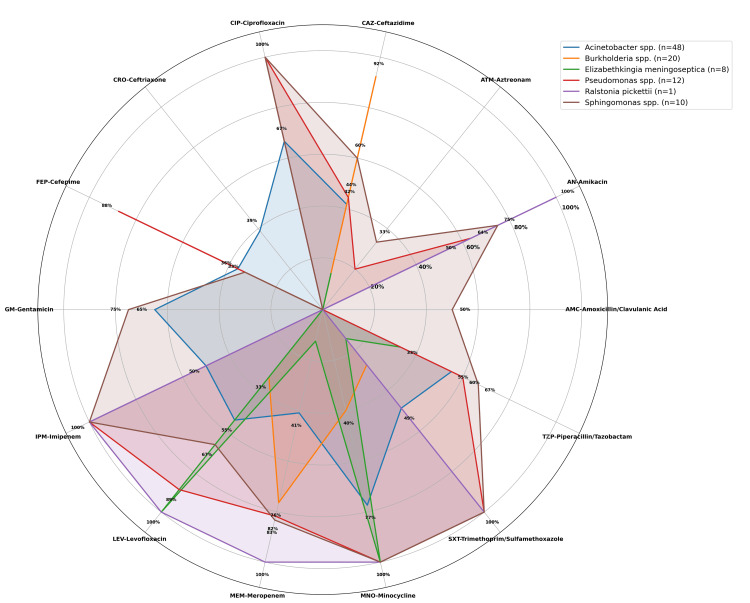 Figure 5
Figure 5| Variable | Category | Frequency (Percentage) |
| Gender | Male | 122 (60.7%) |
| Female | 79 (39.3%) | |
| Gestational Age | Preterm | 151 (75.1%) |
| Term | 49 (24.4%) | |
| Post-term | 1 (0.5%) | |
| Birth Weight | Extremely low birth weight | 49 (24.4%) |
| Very low birth weight | 72 (35.8%) | |
| Low birth weight | 43 (21.4%) | |
| >2500 g | 37 (18.4%) | |
| Mode of Delivery | Lower segment caesarean section | 106 (52.7%) |
| Vaginal Delivery | 95 (47.3%) | |
| Place of Birth | Inborn | 94 (46.8%) |
| Outborn | 107 (53.2%) | |
| Outcome | Discharged | 160 (79.6%) |
| Death | 41 (20.4%) |
| Variables | MDR (n = 92), n (%) | Non-MDR (n = 109), n (%) | Total ( n=201), n (%) | Test of association | p-value | |
| Gender | Female | 33 (35.9%) | 46 (42.2%) | 79 (39.3%) | Chi-square value: 0.59 Df=1 | 0.36* |
| Male | 59 (64.1%) | 63 (57.8%) | 122 (60.7%) | |||
| Gestational age at birth | Preterm | 62 (67.4 %) | 89 (81.7%) | 151 (75.1%) | F- value: 0.45 Df=2 | 0.62** |
| Term | 30 (32.6%) | 19 (17.4%) | 49 (24.4%) | |||
| Post Term | 0 | 1(0.9%) | 1 (0.5%) | |||
| Birth weight | >2500 g | 20 (21.7%) | 17 (15.6%) | 37 (18.4%) | Chi-square value: 10.31 Df=3 | 0.02* |
| Low birth weight | 27 (29.3%) | 16 (14.7%) | 43 (21.4%) | |||
| Very Low birth weight | 29 (31.6%) | 43 (39.4%) | 72 (35.8%) | |||
| Extremely Low birth weight | 16 (17.4%) | 33 (30.3%) | 49 (24.4%) | |||
| Mode of delivery | Lower segment caesarean section | 47 (51.1%) | 59 (54.1%) | 106 (52.7%) | Chi-square value: 0.08 Df=1 | 0.66* |
| Vaginal Delivery | 45 (48.9%) | 50 (45.9%) | 95 (47.3%) | |||
| Sepsis onset | Early onset Sepsis | 35 (38%) | 36 (33%) | 71 (35.3%) | Chi-square value: 0.35 Df=1 | 0.55* |
| Late onset sepsis | 57 (62%) | 73 (67%) | 131 (64.7%) | |||
| Birth Place | Inborn | 38 (41.3%) | 56 (51.4%) | 94 (46.8%) | Chi-square value: 1.65 Df=1 | 0.15* |
| Out born | 54 (58.7%) | 53 (48.6%) | 107 (53.2%) | |||
| Outcome | Death | 14 (15.2%) | 27 (24.8%) | 41 (20.4%) | Chi-square value: 2.25 Df=1 | 0.13* |
| Discharge | 78 (84.8%) | 82 (75.2%) | 160 (79.6%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Streptococcal Infections and Treatments · Antibiotics Pharmacokinetics and Efficacy
Introduction
Neonatal sepsis is a systemic pathological condition that occurs within 28 days of age after birth involving pathogenic microorganisms. It results in various hemodynamic changes and clinical manifestations. In developing nations, neonatal sepsis accounts for about 36% of all neonatal deaths and may go up to one million deaths annually [1-3]. Depending upon onset, neonatal sepsis is classified as early-onset sepsis (EOS) occurring in less than 72 hours after birth and late-onset sepsis (LOS) when it manifests beyond 72 hours of life up to 28 days [4].
The bacteria causing neonatal sepsis vary across regions and even within hospitals. In developing countries, bacteria like Klebsiella pneumoniae, Staphylococcus aureus, and coagulase-negative *Staphylococcus *(CONS) are found as predominant microorganisms causing neonatal sepsis, often showing resistance to first-line antibiotics [5]. Neonatal sepsis cases due to gram-negative bacilli (GNB) are considered to be an increasing global burden, with the rise of multidrug resistance, which poses major challenges to effective treatment and outcomes [6]. Multidrug-resistant (MDR) bacteria show acquired resistance to a minimum of one antimicrobial agent in three or more different classes of antibiotics [7]. Globally, GNB account for nearly 60% of neonatal sepsis cases. In India, GNB are also the major culprits, with studies reporting a high frequency of multidrug resistance among isolates [8,9]. MDR Enterobacteriaceae constitute over 80% of GNB isolates, with carbapenem-resistant strains emerging as a major therapeutic challenge [10].
Antimicrobial resistance (AMR) has become a critical issue in healthcare settings that accounts for approximately 31.0% of neonatal sepsis-related deaths [11]. A comprehensive understanding of the predominant bacterial pathogens and their antibiotic susceptibility patterns is crucial for guiding effective empirical therapy [12]. The growing antibiotic resistance, coupled with the limited development of new antibiotic agents, again exacerbates the complexity of managing neonatal sepsis [13].
Neonatal sepsis predominantly affects newborns who are preterm and of low birth weight because of their underdeveloped immunity and physiological barriers [14]. This is further influenced by several risk factors such as preterm birth, prolonged rupture of membranes, maternal infections, and prolonged hospitalization. Neonates belonging to low socio-economic groups or rural backgrounds are more susceptible to septicemia because of their greater exposure to unhygienic environments [15].
This study is planned with an aim to find out the prevalence of MDR GNB strains causing neonatal sepsis, analyse the antibacterial susceptibility patterns, and evaluate the associated risk factors over a four-year study period.
Materials and methods
Operational definition
The term neonatal sepsis is characterized by a systemic inflammatory condition caused by the invasion of microbial agents into sterile body fluid compartments like blood or CSF [16]. Neonatal sepsis includes both blood culture-positive sepsis and clinical sepsis. Clinical sepsis is defined as a condition in neonates with clinical signs and symptoms of sepsis, like lethargy or irritability, poor feeding, feed intolerance, respiratory distress, thermal instability, seizure, shock, along with the presence of supportive biomarkers such as C-reactive protein (CRP) or procalcitonin (PCT). Culture-positive sepsis is confirmed by isolation of a microorganism from blood culture in neonates with the presence of clinical features of sepsis [17].
Study setting, data gathering, and study duration
This was a retrospective study conducted over four years, from January 1, 2021, to December 31, 2024, in the Department of Microbiology in association with the NICU at Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India. This hospital has a state-of-the-art NICU with a total capacity of 40 beds. The NICU has the capability of managing a substantial annual influx of neonates requiring critical care. The study was approved by the Institutional Ethics Committee, Kalinga Institute of Medical Sciences, Kalinga Institute of Industrial Technology University (approval number: KIIT/KIMS/IEC/1982/2025).
Relevant data regarding septic neonates were collected from NICU records. Blood culture data were retrieved from the Laboratory Information System (LIS) for all samples included during the study period. The variables extracted included patient age, sex, gestational age, mode of delivery, place of birth, outcome, bacterial species, year of isolation, and the antibiotic susceptibility profiles of the isolates. Neonates are classified according to gestational age as preterm (<37 weeks), term (37-42 weeks), and post-term (>42 weeks). Based on birth weight, they were further classified as LBW (1.5-2.5 kg), VLBW (1.0-1.5 kg), and ELBW (<1.0 kg) [18].To ensure data accuracy, repetitive isolates from the same patient were excluded, and only the first isolate was included in the analysis.
Sample collection and processing techniques
Blood and CSF samples (wherever required) from neonates with clinical signs and symptoms of sepsis were cultured by the automated blood culture system (BACT/ALERT® three-dimensional (3D) system; bioMérieux SA, Marcy-l'Étoile, France). A volume of 1.5 -2 mL of blood (0.5-1 mL CSF, where applicable) under aseptic conditions, prior to antibiotic administration, into BacT/ALERT PF Plus bottles (bioMérieux SA) (specific for paediatric patients). As per the available data, a single blood culture sample drawn in a sufficient volume (with 1 ml of blood as the minimum volume) can be used for the diagnosis of neonatal sepsis [19]. A sample was incubated in the automated system for up to five days in case of a negative culture result or until positive growth was detected as per the manufacturer’s guidelines. Positive blood cultures were sub-cultured onto blood agar and MacConkey agar, with petri plates incubated for 24 hours at 37°C and monitored for bacterial growth.
Cultures such as coagulase-negative Staphylococci, *Corynebacterium spp., Micrococcus spp., and Bacillus *spp., which were normal skin commensals and had no supportive clinical evidence, were excluded as contaminants from the study.
Bacteria identification and antibiotic sensitivity testing
Bacteria identification and antibiotic sensitivity testing were done by VITEK® 2 Compact automated system (bioMérieux SA). Antibiotic susceptibility results were interpreted as per Clinical and Laboratory Standards Institute (CLSI) guidelines [20]. In this study, MDR strains of bacteria were identified as the isolates exhibiting non-susceptibility to at least one antibiotic from three or more different classes of antibiotics [7]. The antibiotics on the VITEK 2 panel with their respective drug classes are as follows: ampicillin (β-lactam); amoxicillin/clavulanic acid and ticarcillin/clavulanic acid (β-lactam/β-lactamase inhibitor combinations); piperacillin/tazobactam (extended-spectrum penicillin/β-lactamase inhibitor); ceftazidime, ceftriaxone, cefepime (cephalosporins); cefoperazone/sulbactam (cephalosporins/β-lactamase inhibitor); aztreonam (monobactam); imipenem, meropenem, and ertapenem (carbapenems); amikacin and gentamicin (aminoglycosides); ciprofloxacin and levofloxacin (fluoroquinolones); minocycline (tetracycline); tigecycline (glycylcycline); and trimethoprim/sulfamethoxazole (folate pathway inhibitor).
Data analysis
The collected data were compiled using Microsoft Excel (Microsoft Corporation, Redmond, Washington, United States) and analysed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, New York, United States). Categorical variables were expressed as frequencies and percentages, while continuous variables were summarized as mean with standard deviation or median with interquartile range, as appropriate. Chi-square and Fisher’s exact tests were performed for statistical analysis, and a p-value less than 0.05 was taken to be statistically significant.
Results
A total of 2,670 neonates, admitted in the NICU of the hospital from January 2021 to December 2024, were included in the study. During this period, 2,425 samples, including blood and CSF, were collected from the neonates with clinical features of sepsis and sent to the microbiology laboratory for culture analysis. Out of this, 424 samples obtained from 424 neonates showed positive culture growth. All 424 culture samples showed a single type of microorganism growth, resulting in the isolation of a total of 424 microorganisms. Among the total 424 isolates, 186 were identified as gram-positive bacilli, 201 as GNB, and 37 as Candida spp.. Among the 201 GNB isolates obtained from 201 neonates, 192 isolates were recovered from the blood samples of 192 neonates, and nine isolates were recovered from the CSF of nine neonates. The prevalence of GNB causing neonatal sepsis was calculated to be 47.40% (201/424). Figure 2 shows the entire sample segregation process.
Flowchart showing sample segregation
Among 201 neonates, 122 (60.7%) were male and 79 (39.3%) were female, with the most being preterm neonates (n=151, 75.1%). There were 72 (35.8%) VLBW neonates, followed by 49 (24.4%) ELBW neonates, and 43 (21.4%) LBW neonates. A total of 106 (52.7%) were born through lower segment caesarean section (LSCS), with 107 (53.2%) being delivered in an outside institution, and the overall mortality rate was found to be 20.4% (41/201) (Table 1).
Among all the GNB isolates, *K. pneumoniae *was found to be the predominant bacterium with a prevalence of 26.4% (53/201), followed by Acinetobacter spp. (23.9%, 48/201) and *E. coli *(10.4%, 21/201). Other isolates included Burkholderia spp. (10.0%, 20/201), Serratia marcescens (7.5%, 15/201), Enterobacter spp. (6.5%, 13/201), Pseudomonas spp. (6.0%, 12/201), Sphingomonas spp. (5.0%, 10/201), and Elizabethkingia meningoseptica (4.0%, 8/201). Only one (0.5%) isolate of *Ralstonia pickettii *was obtained (Figure 2).
Distribution of gram-negative bacilli among total study isolates in percentage (N=201)
Out of a total of 201 GNB, 92 MDR strains were detected. The highest percentage of MDR strains was observed among K. pneumoniae isolates (73.6%, 39/53), followed by E. meningoseptica (62.5%, 5/8) and E. coli (61.9%, 13/21). Burkholderia spp. also exhibited a notable MDR prevalence of 55.0% (11/20) (Figure 3).
Distribution of MDR strains among total gram-negative bacilli in percentage (Sunburst) (N=201)MDR: multidrug resistant
Among GNB from the Enterobacteriaceae family, K. pneumoniae exhibited relatively low susceptibility to most of the antibiotics tested, with higher sensitivity observed for minocycline (66.67%), ticarcillin-clavulanic acid (60%), trimethoprim/sulfamethoxazole (57.64%), and gentamicin (53.13%). E. coli showed higher susceptibility to gentamicin (60%), amikacin (50%), imipenem (50%), and meropenem (50%). S. marcescens demonstrated good susceptibility to minocycline (100%), cefepime (92.86%), and ertapenem (71.43%). *Enterobacter *spp. demonstrated higher sensitivity to trimethoprim-sulfamethoxazole (90%), followed by ertapenem (80%), gentamicin (75%), and amikacin (70%). Overall, the findings highlighted varied resistance patterns among the species, underscoring the importance of regular antibiotic susceptibility testing to guide empirical treatment in neonatal sepsis (Figure 4).
Antibiotic sensitivity pattern of gram-negative bacilli from Enterobacteriaceae family (Radar Chart)
Non-fermenter GNB isolated showed the following patterns of susceptibility: Acinetobacter spp. showed the highest susceptibility to minocycline (77.42%), followed by ciprofloxacin (66.67%) and gentamicin (64.86%). Burkholderia spp. exhibited limited susceptibility to most of the antibiotics, with the highest sensitivity observed for ceftazidime (92.31%), followed by meropenem (76.47%) and minocycline (40%). Pseudomonas spp. demonstrated excellent susceptibility to ciprofloxacin, imipenem (100% each), and levofloxacin (88.89%). Sphingomonas spp. showed high sensitivity to imipenem, meropenem, and trimethoprim/sulfamethoxazole (100% each). *E. meningoseptica *exhibited maximum sensitivity to levofloxacin (100%) and minocycline (100%), but displayed significant resistance to most other antibiotics, including beta-lactams and aminoglycosides. Only one isolate of R. pickettii showed complete susceptibility to aminoglycosides, carbapenems, and fluoroquinolones (100%), while being resistant to aztreonam and some beta-lactam combinations (Figure 5).
Antibiotic sensitivity pattern of non-fermenter gram-negative bacilli (Radar Chart)
In this study, the association of various demographic parameters and outcomes with MDR GNB sepsis was evaluated. The comparison of clinical and demographic variables between MDR and non-MDR cases, like gender, gestational age, and mode of delivery, sepsis onset, birth place, or mortality, showed no statistically significant differences. However, birth weight differed significantly (p = 0.02), with the MDR group having higher proportions of LBW and VLBW neonates, while the non-MDR group had more ELBW infants. Preterm births were common in both groups, and mortality was higher in the non-MDR group, but neither of these differences was statistically significant. These findings highlight birth weight as a potential factor influencing MDR status (Table 2).
Discussion
Neonatal sepsis is a major health concern in the first month of life, causing high morbidity and mortality. Timely diagnosis and careful antibiotic administration are vital to enhance treatment outcomes in neonates with sepsis. However, the indiscriminate use of broad-spectrum antibiotics has significantly contributed to the emergence of MDR strains [21]. The United States National Healthcare Safety Network (NHSN) has documented a rising prevalence of multidrug-resistant strains among MDR GNB, comprising E. coli, K. pneumoniae, and Enterobacter spp., with above 60% of cases attributed to *Acinetobacter *spp. [22]. Similarly, the European Antimicrobial Resistance Surveillance Network (EARS-Net) identified notable resistance trends among gram-negative pathogens, with Acinetobacter spp. showing the highest resistance rates, followed by E. coli, *K. pneumoniae *[23].
In the present study, the prevalence of GNB was found to be 47.4% among neonatal sepsis cases. This is consistent with findings of Moftian et al., who reported GNB prevalence as 53.6% in a NICU setting in Iran [6]. However, higher prevalence rates have been observed in other studies, such as Almohammady et al. (65.3%) in Egypt [24] and Gupta et al. (71.74%) in India [25]. The predominance of GNB in neonatal sepsis could be attributed to postnatal acquisition of environmental bacterial strains from the hospital setting, both of which have been well-documented in the study done by Kurma et al. [26]. As per the literature, observed variation in GNB prevalence is influenced by several factors such as geographical differences, infection control practices, and the level of neonatal intensive care provided. Furthermore, differences in study design, sample size, and laboratory diagnostic methods can also contribute to the variability in detection rates of GNB [27].
Furthermore, the present study showed a gender disparity among septic neonates, with a higher proportion of sepsis cases in male neonates (60.7%, n=122) compared to female neonates (39.3%, n=79). This male predominance is consistent with studies by Kurma et al. [26] and Doenhardt et al. [28], where male neonates with sepsis were found to be 51.4% and 61%, respectively. The higher proportion of male neonates in our study may be attributed to a greater admission rate of male infants compared to females in our setting.
In terms of perinatal characteristics, the majority of neonates were preterm (75.1%) and VLBW (35.8%). The predominance of prematurity and low birth weight among the study population aligns with known risk factors for neonatal infections. Preterm and low birth weight neonates have underdeveloped immune systems, reduced skin and mucosal barrier integrity, and often require invasive interventions, all of which increase their vulnerability to bacterial colonization and subsequent infection [29].
In our study, the most prevalent bacteria were Klebsiella pneumoniae (26.4%), followed by Acinetobacter spp. (23.9%), and E. coli (10.4%). The predominance of K. pneumoniae is consistent with findings from a study by Pataskar et al., conducted in central India, which reported a high prevalence rate of 36.7% [30]. This high prevalence of *Acinetobacter *spp. in our study surpasses the prevalence rate of 13.7% documented by Nazir et al., which indirectly gives evidence of the frequent existence of Acinetobacter spp. in our hospital setting [31]. We found the isolation rate of E. coli as 10.4% in our study, which is comparable to the 13.84% prevalence reported by Fang et al. in China [32]. Another study conducted in China by Xiao et al. also reported E. coli as a significant pathogen in neonatal sepsis, particularly in early-onset infections [33].
In the present study, K. pneumoniae was the most prevalent MDR bacterium (73.6%). This is higher than the rate of MDR K. pneumoniae isolates (54%) reported by the investigators of the Delhi Neonatal Infection Study (DeNIS) collaboration. Similarly, MDR E. coli isolates (61.9%) in our study exceed the rate of 38% as reported in the DeNIS collaboration study [34]. Another multicentric study conducted by Jain et al. across five district hospitals in India (2019-2021) reported 84.3% MDR K. pneumoniae isolates and 84.8% MDR strains in E. coli [35]. The higher isolation of MDR bacterial isolates contributes to increased mortality, prolonged hospitalization, and limited therapeutic options [36]. The emergence of resistance to reserve group antibiotics further demands the critical need for evidence-based, targeted antimicrobial strategies in neonatal care settings.
In our study, minocycline (66.67%), ticarcillin-clavulanic acid (60%), trimethoprim/sulfamethoxazole (57.64%), and gentamicin (53.13%) emerged as the most effective antibiotics for K. pneumoniae. Cefepime (6.45%) and imipenem (20.69%) demonstrated notably reduced activity against these isolates. In contrast, a previous study by Gupta et al. reported significantly the highest susceptibility of K. pneumoniae to imipenem (91%) followed by piperacillin-tazobactam (87%), emphasizing potential regional variations in antimicrobial resistance patterns [25]. Breakpoints for ticarcillin/clavulanic acid for Klebsiella spp. are available in CLSI guidelines, and the antibiotic combination is also available commercially in India. Due to a lack of clinical evidence regarding the use of certain antibiotics like minocycline and ticarcillin/clavulanic acid in neonates, these antibiotics may not be recommended for the treatment of sepsis cases, though they are tested in the present study.
*E. coli *isolates from neonatal sepsis cases showed moderate susceptibility to aminoglycosides such as gentamicin (60%) and amikacin (50%), as well as to imipenem (50%) and meropenem (50%). These findings are in contrast to a study from China (Xiao et al. 2023), which reported higher susceptibility rates to amikacin (98%) and gentamicin (70%) among *E. coli *isolates [33]. Similarly, a study done by Dalal et al. in India (2021) documented sensitivity rates of 70% to amikacin and 64% to gentamicin in neonates with sepsis [37]. The observed differences may be influenced by underlying genetic mechanisms, such as the presence of antibiotic resistance genes due to mutations or by horizontal gene transfer from closely related strains, as well as variations in neonatal ICU infection control practices and antibiotic prophylaxis policies [38].
Enterobacter spp. in our study demonstrated the highest susceptibility, particularly to trimethoprim-sulfamethoxazole (90%), ertapenem (80%), gentamicin (75%), and amikacin (70%). These findings are partially aligned with those of Almohammady et al. (2023), who reported 67% susceptibility to amikacin, whereas 100% susceptibility was seen to levofloxacin [24]. However, our results diverge from those of Siddiqui et al., who found complete susceptibility to carbapenems (100%) and widespread resistance in other antibiotic classes [39]. Our results revealed the sensitivity of S. marcescens to minocycline as 100% and higher sensitivities to cefepime (92.86%) and ertapenem (71.43%).
In the present study, Acinetobacter spp. showed the highest susceptibility to minocycline (77.42%), followed by ciprofloxacin (66.67%) and gentamicin (64.86%). These findings contrast sharply with the results reported by the study conducted by Nazir et al. in northern India, who observed much lower susceptibility rates for minocycline (30.6%), ciprofloxacin (4.08%), and gentamicin (4.08%) [31]. *Acinetobacter *spp. are rapidly spreading, with rising resistance even to newer antimicrobials. Their ability to quickly acquire resistance and persist in hospital environments makes them potent causes of nosocomial outbreaks. The global rise of MDR Acinetobacter baumanii limits treatment options, highlighting the need for novel therapies.
Burkholderia spp. demonstrated high susceptibility to ceftazidime (92.31%) and meropenem (76.47%), findings that are consistent with those reported by Kar et al., who observed ceftazidime susceptibility of 87% among clinical isolates [40]. In our findings, Pseudomonas spp. showed higher sensitivity to ciprofloxacin (100%), imipenem(100%), meropenem (81.82%), and piperacillin-tazobactam (60%). In contrast, Dalal et al. reported higher susceptibility to meropenem (96%) and piperacillin-tazobactam (93%) but lower susceptibility to ciprofloxacin (47%) [37].
The susceptibility profile of Sphingomonas spp. revealed complete sensitivity to imipenem, meropenem, and trimethoprim/sulfamethoxazole. Another emerging bacteria, E. meningoseptica, was susceptible only to levofloxacin (100%) and minocycline (100%), consistent with findings by Anil et al., who reported that E. meningoseptica was susceptible to minocycline and levofloxacin while showing resistance to all other antibiotics tested [41].
MDR infections were significantly more common in neonates with low birth weight, particularly in the VLBW and ELBW groups (p = 0.02). MDR (58.7%) was more prevalent in outborn neonates, while higher mortality occurred in the non-MDR group (24.8%). Although variables such as gender, gestational age, mode of delivery, onset of sepsis, and mortality showed no significant association, these findings are consistent with those of Miranda et al. [42], who identified low birth weight and outborn status as risk factors, but differ from Zou et al. [43], who reported higher mortality with MDR infections, a discrepancy that may reflect differences in care quality and treatment practices. The higher MDR rate in LBW neonates may be explained by their immature immune systems, prolonged hospitalization, and increased use of invasive procedures, whereas the higher mortality in the non-MDR group could be due to severe underlying conditions or early-onset sepsis, where rapid disease progression leads to poor outcomes despite pathogen susceptibility.
Limitations
The present study has certain limitations. The retrospective study design may introduce selection and information biases. Due to a smaller number of CSF samples, the patients with CSF culture-positive cases were considered together with blood culture-positive neonates for analysis of antibiotic sensitivity and prevalence of MDR strains. Moreover, the lack of molecular characterization limits the ability to elucidate the specific mechanisms underlying antimicrobial resistance. Finally, the absence of long-term follow-up data restricts the assessment of the extended clinical impact of multidrug-resistant infections in neonates.
Conclusions
GNB in neonatal sepsis has become a major concern, particularly in developing countries, because of the rising prevalence of MDR strains. This study highlights the burden of GNB in neonatal sepsis with the distribution of MDR strains among different species of GNB in a tertiary care health setting. The most predominant bacteria isolated were *K. pneumoniae, *followed by Acinetobacter spp., and E. coli. The maximum number of MDR strains was observed among K. pneumoniae isolates, followed by E. meningoseptica and E. coli. Species-specific susceptibility patterns were noted as *K. pneumoniae showed higher sensitivity to trimethoprim/sulfamethoxazole and gentamicin; E. coli to gentamicin and imipenem; Enterobacter *spp. to trimethoprim-sulfamethoxazole and ertapenem; Acinetobacter spp. to minocycline and ciprofloxacin; Pseudomonas spp. to ciprofloxacin, imipenem, and cefoperazone-sulbactam; Burkholderia spp. to ceftazidime and meropenem. LBW and VLBW neonates were significantly associated with sepsis caused by MDR GNB compared to ELBW neonates. These findings emphasize the importance of species-specific antimicrobial strategies and sustained resistance surveillance to guide effective management in NICUs through implementing appropriate antibiotic stewardship.
These findings highlight the urgent need for species-directed antimicrobial stewardship, routine resistance surveillance in neonatal intensive care units, and implementation of appropriate Infection Prevention and Control (IPC) practices. Appropriate empirical therapy based on local susceptibility trends is essential to improve clinical outcomes and reduce the burden of multidrug-resistant infections in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical and bacteriological profile of neonatal sepsis: a prospective hospital-based study Int J Pediatr Jatsho J Nishizawa Y Pelzom D Sharma R 1835945202020203295257410.1155/2020/1835945 PMC 7481930 · doi ↗ · pubmed ↗
- 2Neonatal sepsis Stat Pearls [Internet] Singh M Alsaleem M Gray CP Treasure Island (FL)Stat Pearls Publishing 2022 https://www.ncbi.nlm.nih.gov/books/NBK 531478/30285373 · pubmed ↗
- 3A decade of neonatal sepsis caused by gram-negative bacilli-a retrospective matched cohort study Eur J Clin Microbiol Infect Dis Nordberg V Iversen A Tidell A Ininbergs K Giske CG Navér L 180318134020213376102010.1007/s 10096-021-04211-8PMC 8346411 · doi ↗ · pubmed ↗
- 4Diagnosis and management of neonatal bacterial sepsis: current challenges and future perspectives Trop Med Infect Dis De Rose DU Ronchetti MP Martini L Rechichi J Iannetta M Dotta A Auriti C 199920243933088810.3390/tropicalmed 9090199 PMC 11435811 · doi ↗ · pubmed ↗
- 5Neonatal sepsis, antibiotic susceptibility pattern, and treatment outcomes among neonates treated in two tertiary care hospitals of Yangon, Myanmar from 2017 to 2019 Trop Med Infect Dis Oo NA Edwards JK Pyakurel P Thekkur P Maung TM Aye NS Nwe HM 62620213392474610.3390/tropicalmed 6020062 PMC 8167801 · doi ↗ · pubmed ↗
- 6Prevalence of gram-negative bacteria and their antibiotic resistance in neonatal sepsis in Iran: a systematic review and meta-analysis BMC Infect Dis Moftian N Rezaei-Hachesu P Arab-Zozani M Samad-Soltani T Esfandiari A Tabib MS Mirnia K 5342320233758272610.1186/s 12879-023-08508-1PMC 10426195 · doi ↗ · pubmed ↗
- 7Multidrug resistant, extensively drug resistant and pan drug resistant gram negative bacteria at a tertiary care centre in Bhubaneswar Int J Community Med Public Health Pattnaik D Panda SS Singh N Sahoo S Mohapatra I Jena J 56757262019
- 8Gram-negative neonatal sepsis in low- and lower-middle-income countries and WHO empirical antibiotic recommendations: a systematic review and meta-analysis P Lo S Med Wen SC Ezure Y Rolley L 018202110.1371/journal.pmed.1003787 PMC 847817534582466 · doi ↗ · pubmed ↗