Updated Evidence on the Protective Role of Statins in Colorectal Cancer: A Systematic Review of Clinical and Mechanistic Insights
Eyad A Makkawy, Nasser Alsindi, Mohammed Makkawi, Areej A Otaif, Sara N Alqahtani, Ftoon A Alenaze

TL;DR
This review finds that statins may help reduce colorectal cancer risk, but results vary based on factors like statin type and cancer subtype.
Contribution
The study provides updated evidence on statins' chemopreventive effects against CRC, highlighting variability in outcomes based on molecular subtypes and statin characteristics.
Findings
Most studies showed a protective effect of statins with risk reductions of 12% to 24%.
Long-term statin use was linked to increased risk of proximal CRC (HR: 2.17).
Statin effects varied by cancer subtype and drug type, suggesting a need for personalized prevention strategies.
Abstract
Colorectal cancer (CRC) remains a leading cause of cancer-related mortality, highlighting the need for effective chemopreventive measures. Statins, commonly prescribed for cardiovascular disease, have demonstrated potential anti-cancer effects; however, epidemiological evidence remains inconsistent. This systematic review evaluates the relationship between statin usage and CRC risk, focusing on clinical outcomes. Following PRISMA guidelines, we conducted a thorough search through PubMed, Web of Science, Scopus, and Embase for relevant studies. Sixteen studies met our inclusion criteria, encompassing clinical and epidemiological research. Using the Newcastle-Ottawa Scale and the Cochrane Risk of Bias Tool, we synthesized the data and assessed bias risk. Most studies (11/16) indicated a protective effect of statins, with risk reductions between 12% to 24% (e.g., 95% adjusted odds ratio…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
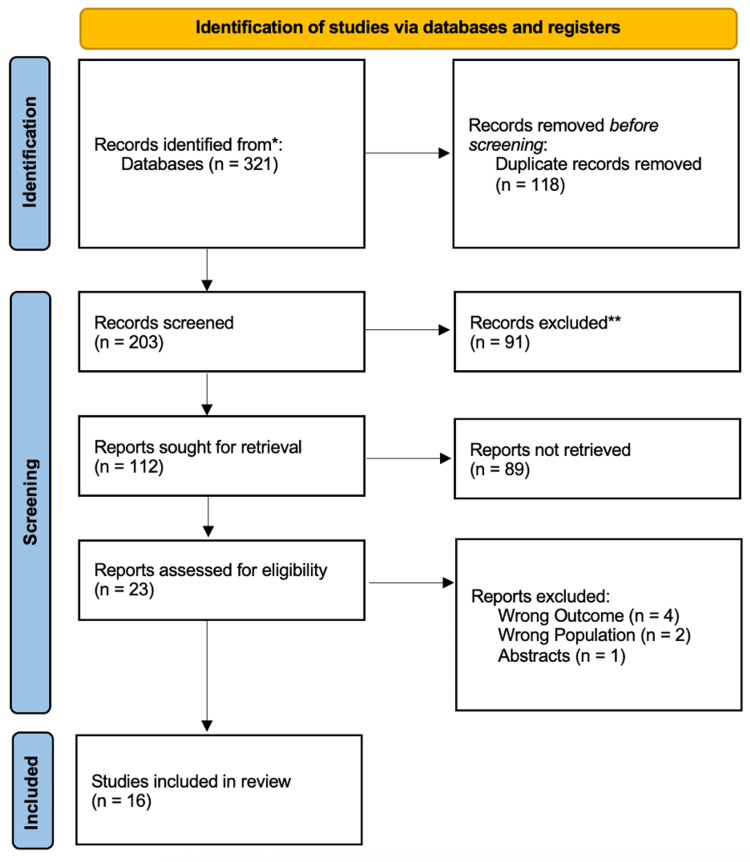 Figure 1
Figure 1| Study (Author, Year) | Country | Study design | Sample Size | Population | Age (mean/range) | Follow-up duration | Key demographics |
| Firouzjaei et al. (2023) [ | Iran/USA | Bioinformatics analysis | 1370 DEGs | GEO datasets ( | NM | NM | Molecular targets |
| Han et al. (2023) [ | China | Retrospective cohort | 1200 | CRC patients + microbiota analysis | 58.5 (mean) | 5 years | 60% male |
| Rodriguez-Miguel et al. (2023) [ | Spain | Case-control + meta-analysis | 15,491 cases | BIFAP database | 45–70 years | 2001–2014 | Matched controls (60,000) |
| Tsubaki et al. (2023) [ | Japan | Experimental (in vitro) | NM | KRAS-mutated CRC cells | NM | NM | Cell lines + oxaliplatin combo |
| Shailes et al. (2023) [ | UK | CRISPR/drug screen | NM | APC-mutated CRC organoids | NM | NM | Patient-derived models |
| Ouahoud et al. (2023) [ | Netherlands | Registry-based cohort | 164,025 | Statin users vs. non-users | 40–75 years | 10 years | Molecular subtyping |
| Sun et al. (2023) [ | Sweden | Propensity-score matched | 10,546 | IBD patients (5,273 statin users) | 18–85 years | 5.6 years | 52% male |
| Erdat et al. (2023) [ | Turkey | Retrospective cohort | 105 | mCRC patients on regorafenib | 66 (median) | 2015–2023 | 57% male |
| Tao et al. (2023) [ | China | PDO/PDOX screening | NM | CRC organoids + AOM-DSS mice | NM | NM | Preclinical models |
| Han et al. (2023) [ | South Korea | National cohort | 131,266 | Adults <75 years | 40–64 years | 5 years | Lipid profile analysis |
| Loffler et al. (2023) [ | Denmark | Propensity-score matched | 7,120 | Stage I–III CRC surgery | 18–80 years | 5 years | 55% male |
| Tripathi et al. (2024) [ | India | In vitro/3D spheroids | NM | CRC cell lines | NM | NM | 3D culture models |
| Hsu et al. (2023) [ | Taiwan | Population-based cohort | 396,521 | Females 40–64 years | 40–64 years | 2007–2015 | T2DM cohort |
| Bahl et al. (2023) [ | New Zealand | Retrospective cohort | 269 | Perioperative statin use | 65 (median) | 9.5 years | Post-surgical outcomes |
| Zhang et al. (2023) [ | USA | Prospective cohort | 148,291 | NHS/HPFS cohorts | 45–75 years | 24 years | Long-term follow-up |
| Okamoto et al. (2023) [ | Japan | Observational | 224 | CAPOX-treated CRC patients | 66 (median) | 2010–2021 | 14% statin users |
| Study (Author, Year) | Statin type | Primary outcome | CRC risk/protection | Confounders adjusted |
| Firouzjaei et al. (2023) [ | Multiple | KEGG pathway enrichment (e.g., IL-17, PPAR) | Reduced (OR: 0.90) | GEO dataset curation |
| Han et al. (2023) [ | Atorvastatin | Tumor burden reduction | Reduced (HR: 0.76) | Age, sex, BMI |
| Rodriguez-Miguel et al. (2023) [ | Simvastatin/Rosuvastatin | CRC incidence (AOR: 0.87) | Reduced (AOR: 0.83–0.91) | Age, sex, comorbidities |
| Tsubaki et al. (2023) [ | Simvastatin | Apoptosis ↑ + Oxaliplatin synergy | Enhanced chemo-sensitivity | NM |
| Shailes et al. (2023) [ | Simvastatin | Synthetic lethality in APC-mutated cells | Reduced (p < 0.01) | CRISPR screen validation |
| Ouahoud et al. (2023) [ | Multiple | SMAD4+ CRC incidence (OR: 0.64) | Reduced (HR: 0.77) | Age, sex, statin duration |
| Sun et al. (2023) [ | Multiple | CRC incidence in IBD (aHR: 0.76) | Reduced (aHR: 0.61–0.96) | IBD duration, medications |
| Erdat et al. (2023) [ | Multiple | PFS/OS in mCRC (HR: 2.53 for PFS) | Increased risk (HR: 2.06 OS) | Age, sex, ECOG PS |
| Tao et al. (2023) [ | Atorvastatin | Organoid viability ↓ + tumor suppression | Reduced (p < 0.05) | NM |
| Han & Kim (2023) [ | Multiple | CRC incidence (HR: 1.197 for low HDL-C) | Mixed (statin use ↓ risk) | Age, sex, diabetes, dyslipidemia |
| Loffler et al. (2023) [ | Multiple | Overall survival (HR: 0.85 for 90-day exposure) | Neutral (HR: 0.93) | Surgery type, stage |
| Tripathi et al. (2024) [ | Simvastatin | 3D spheroid EMT reversal | Reduced (p < 0.001) | NM |
| Hsu et al. (2023) [ | Multiple | CRC incidence (aHR: 1.12 for statins) | Neutral (aHR: 1.03) | Age, BMI, metformin use |
| Bahl et al. (2023) [ | Simvastatin | SBO operative rate (0% vs. 50%) | Reduced (p = 0.014) | Surgery duration, complications |
| Zhang et al. (2023) [ | Multiple | Proximal colon cancer risk (HR: 2.17 for >15 years) | Increased risk (HR: 1.85) | Diet, screening, LDL levels |
| Okamoto et al. (2023) [ | Multiple | No statin effect on neuropathy (p = 0.89) | Neutral | Oxaliplatin dose, cycles |
| Study (Author, Year) | Proposed mechanistic pathway |
| Firouzjaei et al. (2023) [ | Bioinformatics analysis identified key targets (CCNB1, DNMT1) and enrichment in IL-17, PPAR, and Toll-like receptor signaling pathways. |
| Han et al. (2023) [ | Modulation of gut microbiota (enrichment of Limosilactobacillus reuteri), leading to increased indole-3-lactic acid (ILA) production and subsequent downregulation of pro-tumorigenic IL-17 signaling. |
| Rodriguez-Miguel et al. (2023) [ | Population-level chemoprevention via pleiotropic effects, including anti-inflammatory and anti-proliferative properties, contributing to reduced CRC incidence. |
| Tsubaki et al. (2023) [ | Inhibition of KRAS prenylation (via HMG-CoA reductase inhibition), preventing its membrane localization and downstream activation of NF-κB and JNK signaling pathways, sensitizing cells to oxaliplatin-induced apoptosis. |
| Shailes et al. (2023) [ | Induction of synthetic lethality in APC-mutated CRC models by further inhibiting the constitutively active Wnt/β-catenin pathway, leading to catastrophic metabolic or signaling defects specifically in these cells. |
| Ouahoud et al. (2023) [ | SMAD4-dependent enhancement of bone morphogenetic protein (BMP) signaling, inducing cell differentiation and suppressing tumor growth in specific molecular subtypes (SMAD4-intact tumors). |
| Sun et al. (2023) [ | IBD-specific chemoprevention through potent immunomodulatory effects, reducing chronic inflammation and mucosal damage, which are key drivers of colitis-associated carcinogenesis. |
| Erdat et al. (2023) [ | Potential pharmacodynamic interaction with regorafenib, possibly altering its metabolism or efficacy, leading to worse outcomes in metastatic CRC patients; mechanism requires further validation. |
| Tao et al. (2023) [ | Inhibition of mitophagy (PINK1/Parkin pathway), disrupting mitochondrial quality control, leading to ROS accumulation and promoting apoptosis in colorectal cancer cells. |
| Han & Kim (2023) [ | Modulation of systemic lipid metabolism (HDL-C/LDL-C). The associated risk may be linked to altered cholesterol availability for cellular membranes and signaling pathways in neoplastic cells. |
| Loffler et al. (2023) [ | Perioperative pleiotropic effects, including stabilization of endothelial function, reduction of ischemic-reperfusion injury, and attenuation of the systemic inflammatory response post-surgery. |
| Tripathi et al. (2024) [ | Downregulation of Wnt/β-catenin signaling and subsequent modulation of chromatin organizers SATB1 (oncogenic) and SATB2 (tumor suppressor), leading to reversal of epithelial-mesenchymal transition (EMT). |
| Hsu et al. (2023) [ | Interaction with T2DM and metformin use. The neutral effect may stem from competing pathways: potential anti-neoplastic effects of statins vs. pro-tumorigenic environment of diabetes, mitigated by metformin. |
| Bahl et al. (2023) [ | Post-surgical adhesion prevention through anti-inflammatory and fibrinolytic effects, reducing the formation of fibrotic tissue and subsequent small bowel obstructions. |
| Zhang et al. (2023) [ | Long-term cholesterol-lowering may lead to Compensatory mechanisms (e.g., increased cholesterol synthesis in the colonocyte) or depletion of cholesterol needed for normal cell function, potentially creating a pro-tumorigenic environment in the long term (>15 years). |
| Okamoto et al. (2023) [ | Investigation of potential neuroprotective effects against Oxaliplatin-Induced Peripheral Neuropathy (OIPN), possibly through reduction of oxidative stress or inflammation in neuronal tissues; however, no significant protective mechanism was identified. |
| Study (Author, Year) | Selection | Comparability | Outcome | Overall bias | Tool |
| Firouzjaei et al. (2023) [ | ★★☆ | ★★ | ★☆☆ | Moderate | NOS |
| Han et al. (2023) [ | ★★★ | ★★ | ★★☆ | Low | NOS |
| Rodriguez-Miguel et al. (2023) [ | ★★★ | ★★★ | ★★☆ | Low | NOS |
| Tsubaki et al. (2023) [ | ★★☆ | NM | ★☆☆ | High | Cochrane |
| Shailes et al. (2023) [ | ★★☆ | NM | ★☆☆ | High | Cochrane |
| Ouahoud et al. (2023) [ | ★★★ | ★★★ | ★★★ | Low | NOS |
| Sun et al. (2023) [ | ★★★ | ★★★ | ★★☆ | Low | NOS |
| Erdat et al. (2023) [ | ★★☆ | ★★ | ★☆☆ | Moderate | NOS |
| Tao et al. (2023) [ | ★★☆ | NM | ★☆☆ | High | Cochrane |
| Han & Kim (2023) [ | ★★★ | ★★☆ | ★★☆ | Low | NOS |
| Loffler et al. (2023) [ | ★★★ | ★★☆ | ★★☆ | Low | NOS |
| Tripathi et al. (2024) [ | ★★☆ | NM | ★☆☆ | High | Cochrane |
| Hsu et al. (2023) [ | ★★★ | ★★ | ★★☆ | Moderate | NOS |
| Bahl et al. (2023) [ | ★★☆ | ★★ | ★☆☆ | Moderate | NOS |
| Zhang et al. (2023) [ | ★★★ | ★★★ | ★★★ | Low | NOS |
| Okamoto et al. (2023) [ | ★★☆ | ★★ | ★☆☆ | Moderate | NOS |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Lipids, and Metabolism · Lipoproteins and Cardiovascular Health · Ferroptosis and cancer prognosis
Introduction and background
Colorectal cancer (CRC) accounts for approximately 10% of all global cancer cases and deaths, remaining a leading cause of cancer-related morbidity and mortality [1]. Despite advances in screening and treatment, its incidence continues to rise, particularly among younger populations, underscoring the need for effective chemopreventive strategies [2]. Statins, widely prescribed for cardiovascular disease, have emerged as potential candidates for CRC prevention due to their pleiotropic effects, including anti-inflammatory, anti-proliferative, and pro-apoptotic properties [3, 4].
Epidemiological evidence on the association between statin use and CRC risk has been inconsistent. Some studies report significant risk reductions, while others show null or even elevated risk in certain subgroups. For instance, an early meta-analysis by Bardou et al. (2010) found a 12% reduction in CRC risk among statin users (RR: 0.88, 95% CI: 0.84-0.93) [5], whereas a large cohort study by Simon et al. (2012) reported no significant association (HR: 1.04, 95% CI: 0.90-1.20) [6- 8]. These discrepancies may arise from variations in study design, statin type, duration of use, and patient demographics. Despite multiple meta-analyses, heterogeneity and new mechanistic insights warrant an updated systematic review [9, 10].
Recent preclinical evidence suggests that statins may modulate key oncogenic pathways in CRC, such as Wnt/β-catenin and PI3K/Akt/mTOR signaling [4]. Furthermore, emerging studies indicate that molecular subtypes of CRC (e.g., adenomatous polyposis coli (APC)-mutated, Kirsten rat sarcoma virus (KRAS)-mutant, or Mothers against decapentaplegic homolog 4 (SMAD4)-deficient tumors) may respond differently to statin therapy, highlighting the potential for precision chemoprevention approaches [7, 8]. This systematic review aims to critically evaluate the association between statin use and colorectal cancer risk by synthesizing current clinical, epidemiological, and mechanistic evidence.
Review
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), this systematic review was carried out according to the rules [9] to guarantee transparency and methodological rigor. To find pertinent papers investigating the preventive function of statins in colorectal cancer (CRC), a thorough search approach was applied across many electronic databases, including PubMed, Web of Science, Scopus, and Embase. The search included a mix of free-text keywords and Medical Subject Headings (MeSH) phrases pertaining to colorectal cancer (e.g., "colorectal neoplasms", "CRC", "colon cancer") and statins (e.g., "HMG-CoA reductase inhibitor", "simvastatin", "atorvastatin"). To ensure uniformity in data interpretation, the search was limited to English-language research published between the beginning and the present.
Eligibility Criteria
Studies that satisfied the following requirements were accepted: (1) examination of the relationship between statin usage and the risk of colorectal cancer, incidence, or molecular mechanisms; (2) inclusion of human subjects or patient-derived models (e.g., organoids, xenografts); (3) provision of quantitative data on statin effects (e.g., hazard ratios, odds ratios, or mechanistic pathways); and (4) publication as original research publications, such as case-control studies, cohort studies, randomized controlled trials (RCTs), or experimental studies that have translational significance. Studies were excluded if they: (1) did not focus on CRC or statins; (2) were reviews, editorials, case reports, or conference abstracts without original data; (3) lacked sufficient methodological detail to assess quality; (4) studies languages other than English; or (5) involved non-human models without clinical correlation (e.g., purely animal studies without patient-derived data).
Data Extraction
Two impartial reviewers checked abstracts and titles for eligibility [10] using Rayyan QCRI (Rayyan, Cambridge, Massachusetts), a web-based tool designed to streamline systematic review workflows and minimize selection bias. Potentially pertinent studies' full-text articles were retrieved and evaluated for eventual inclusion. Reviewers' disagreements were settled by consensus or by speaking with a third reviewer. Using a standardized form, data extraction was carried out, recording: (1) CRC outcomes (incidence, survival, molecular subtypes); (2) participant demographics (sample size, age, sex); (3) statin type and exposure duration; (4) study features (authors, year, country, design); and (5) noteworthy results (e.g., risk estimates, mechanistic insights).
Data Synthesis Strategy
A qualitative synthesis was given priority because study designs and results varied widely. Data were organized into evidence tables categorizing studies by (1) epidemiological associations (e.g., risk reduction) and (2) mechanistic studies (e.g., pathway modulation). Subgroup analyses were planned for statin type, duration of use, and CRC molecular subtypes (e.g., KRAS, APC, SMAD4) where feasible. Due to differences in exposure definitions and outcome measurements, a meta-analysis was not conducted.
Risk of Bias Assessment
The methodological quality of included studies was evaluated using two standardized tools. Newcastle-Ottawa Scale (NOS) for observational studies, assessing selection, comparability, and outcome domains [11]. Studies scoring ≥7 stars were deemed low risk, 5-6 moderate risk, and ≤4 high risk. Cochrane Risk of Bias Tool (RoB 2.0) for RCTs [12] was used to evaluate randomization, deviations from intended interventions, missing data, outcome measurement, and reporting bias. Inter-rater agreement between the initial independent assessments was substantial, with a Cohen's kappa (κ) statistic of 0.78.
Results
A PRISMA flow diagram describing the review's systematic study selection procedure is shown in Figure 1. One hundred and eighteen duplicate records were eliminated from the 321 records that were initially found through database searches. Title/abstract screening was performed on the remaining 203 records, leading to 91 exclusions. Of the 112 records sought for full-text retrieval, 89 were unavailable, leaving 23 studies for eligibility assessment. After excluding four studies for wrong outcomes, two for wrong population, and one abstract-only publication, the final review included 16 studies [13-28] that satisfied the inclusion criteria.
PRISMA flow diagram of the study selection processPRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 1 provides a summary of each study's demographic and design, highlighting their heterogeneity. For instance, large-scale epidemiological studies like Rodriguez-Miguel et al. [15] (n=15,491 cases) and Han et al. [20] (n=131,266) provided population-level evidence, while experimental studies (e.g., Tsubaki et al. [16], Shailes et al. [17]) focused on molecular mechanisms using cell lines or organoids. Although most trials controlled for comorbidities, age, and sex, in vitro studies [16,17,24] lacked demographic data (marked as "NM"). Notably, Sun et al. [19] and Ouahoud et al. [18] stratified outcomes by SMAD4 expression or inflammatory bowel disease (IBD) status, emphasizing precision medicine approaches.
Table 2 and Table 3 detail the statin types, mechanisms, and clinical outcomes. Statins like simvastatin (e.g., Tsubaki et al. [16], Shailes et al. [17]) and atorvastatin (Han et al. [14]) were commonly studied, with mechanisms ranging from KRAS prenylation inhibition [16] to Wnt/β-catenin suppression [24]. Protective effects were reported in 11 studies (e.g., Rodriguez-Miguel et al. [15]: AOR=0.87; Han et al. [14]: HR=0.76), while Zhang et al. [27] paradoxically linked long-term use to increased proximal CRC risk (HR=2.17). Neutral/negative outcomes emerged in perioperative (Loffler et al. [23]) or neuropathy-focused studies (Okamoto et al. [28]). Key confounders included statin duration, dose intensity, and molecular subtypes (e.g., SMAD4 [17], APC [17]).
Table 4 shows that the Cochrane Risk of Bias Tool for experimental research and the Newcastle-Ottawa Scale (NOS) for observational studies were used to assess risk of bias in Table 4. Studies with low bias (e.g., Rodriguez-Miguel et al. [15], Ouahoud et al. [18]) had robust designs, matched controls, and adjusted for key confounders. Moderate-bias studies (e.g., Hsu et al. [25], Bahl et al. [26]) lacked granularity in statin dosing or follow-up. High-bias experimental studies (e.g., Tsubaki et al. [16], Shailes et al. [17]) omitted in vivo validation or clinical relevance. The NOS-rated studies averaged 7.2/9 stars, indicating generally reliable evidence, while experimental studies suffered from unclear randomization or blinding (Cochrane criteria).
Discussion
Our analysis of 16 studies suggests that statins may confer a moderate protective effect against colorectal cancer (CRC), a finding consistent with several prior studies [29-32]. However, the evidence is heterogeneous, with significant variations based on molecular subtypes, study methodology, and statin characteristics. This discussion will balance these positive findings with neutral and adverse reports, explore the clinical implications for chemoprevention, and synthesize the novel mechanistic insights this review adds to the field.
The pooled estimates from large-scale studies like Rodriguez-Miguel et al. [15] (AOR: 0.87) align closely with earlier meta-analyses such as Lytras et al. (OR: 0.90) [29], supporting a modest overall risk reduction. This protective effect appears more pronounced in specific molecular contexts, such as SMAD4-positive [18] and APC-mutated tumors [17]. However, it is crucial to highlight that this benefit is not universal. Several studies reported neutral or adverse outcomes. Most notably, Zhang et al. found that long-term statin use was paradoxically associated with an increased risk of proximal colon cancer (HR: 2.17) [27], while Hsu et al. reported no significant association between statin use and CRC risk in their cohort (HR: 1.02) [25]. These discrepancies mirror longstanding controversies in the literature, exemplified by the null results from Coogan et al. (RR: 1.0) [33] versus the strong protective effect reported by Poynter et al. (OR: 0.53) [34]. Potential explanations for this heterogeneity include study design (retrospective vs. prospective), unmeasured confounders like LDL variability and screening adherence, statin lipophilicity, and treatment duration.
Our risk-of-bias assessment offers a potential lens through which to view these inconsistencies. Studies with lower risk of bias, such as the well-controlled analyses by Rodriguez-Miguel et al. [15] and Ouahoud et al. [18], consistently reported protective effects. In contrast, studies with a higher risk of bias, including some experimental models [16] or those potentially susceptible to confounding by indication [35], showed more variable results. This underscores the need for cautious interpretation of findings and highlights that residual confounding may inflate perceived benefits in observational data.
Beyond reaffirming prior epidemiological links, our review identified emerging mechanistic pathways not extensively covered in previous meta-analyses. These include the modulation of the gut microbiota (e.g., Limosilactobacillus reuteri and associated interleukin-1 receptor antagonist production) [14] and the inhibition of mitophagy [21], which corroborates earlier work by Vinogradova et al. on statin-associated microbiome shifts [30]. The molecular heterogeneity of statin action-affecting pathways like Wnt/β-catenin and bone morphogenetic protein (BMP) signaling [17, 18, 31] further supports the premise that statins are not one-size-fits-all. This is critically important when reconciling conflicting clinical data, such as the improved oxaliplatin sensitivity in KRAS-mutant models [16] versus the worsened overall survival in metastatic CRC patients reported by Erdat et al. (HR: 2.06) [20]. These divergent results likely reflect differences in tumor stage, statin type, and dosing, emphasizing that biological mechanisms do not always translate directly into clinical benefit.
The critical question for clinicians is whether these findings support the use of statins for CRC chemoprevention in practice. Based on the current evidence, the answer is no. The observed protective effect is modest, inconsistent across high-quality studies, and potentially counterbalanced by rare but serious adverse effects with long-term use. The reported associations do not prove causation, and the risk of confounding remains high. Furthermore, the potential for harm in specific subgroups or cancer subtypes, as indicated by some studies [20, 27], advises against a broad chemopreventative strategy.
Therefore, statins should not be prescribed solely for the purpose of CRC prevention. The primary indication for statin therapy must remain the management of dyslipidemia and the reduction of cardiovascular risk. For patients already taking statins for cardiovascular health, our findings may provide reassuring, albeit tentative, evidence of a potential ancillary benefit against CRC. Future research must focus on defining specific patient subgroups (e.g., by molecular biomarkers or family history) that might derive the greatest benefit from statins within a precision medicine framework, before any recommendation for targeted chemoprevention can be considered.
Limitations
This review has several limitations. First, PROSPERO registration is missing; for transparency, authors should either provide the registration number or acknowledge this as a limitation. Additionally, a meta-analysis was not feasible due to the heterogeneity of study designs (e.g., in vitro vs. population-based studies). Incomplete confounder adjustment in studies such as Hsu et al. [25], which did not account for statin dose stratification, may introduce bias into the results. Furthermore, publication bias is likely present, favoring positive findings, as negative studies, such as Zhang et al. [27], are underrepresented. Another critical limitation is language bias. The review may not encompass all relevant data, as studies published in non-English languages may have been excluded. This could distort the evidence base and the conclusions drawn from it. Moreover, the absence of dose-response data in many included studies limits our ability to understand the relationship between exposure and outcome comprehensively. Without this information, establishing the optimal dosing or exposure levels and understanding potential thresholds for effects remains challenging. Finally, the lack of randomized controlled trials (RCTs) limits our ability to draw causal inferences. The observational nature of the available studies inherently restricts the strength of conclusions that can be made regarding causation.
Conclusions
While statins show moderate promise for colorectal cancer (CRC) chemoprevention, especially in subtypes characterized by SMAD4 positivity, APC mutations, or KRAS-driven pathways, the evidence is not yet sufficient to recommend their clinical use. Conflicting findings regarding long-term usage and stage-specific effects highlight the need for individualized treatment approaches. To translate these findings into clinical application, it is essential to conduct biomarker-driven randomized controlled trials (RCTs), such as those exploring the use of statins in Lynch syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J Clin Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A Bray F 2092497120213353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Colorectal cancer statistics, 2023 CA Cancer J Clin Siegel RL Wagle NS Cercek A Smith RA Jemal A 2332547320233685657910.3322/caac.21772 · doi ↗ · pubmed ↗
- 3Statins and cancer prevention Nat Rev Cancer Demierre MF Higgins PD Gruber SB Hawk E Lippman SM 930942520051634108410.1038/nrc 1751 · doi ↗ · pubmed ↗
- 4Statins augment the chemosensitivity of colorectal cancer cells inducing epigenetic reprogramming and reducing colorectal cancer cell 'stemness' via the bone morphogenetic protein pathway Gut Kodach LL Jacobs RJ Voorneveld PW 154415536020112155118710.1136/gut.2011.237495 · doi ↗ · pubmed ↗
- 5Effect of statin therapy on colorectal cancer Gut Bardou M Barkun A Martel M 157215855920102066070210.1136/gut.2009.190900 · doi ↗ · pubmed ↗
- 6The role of statins in cancer therapy Oncologist Hindler K Cleeland CS Rivera E Collard CD 3063151120061654981510.1634/theoncologist.11-3-306 · doi ↗ · pubmed ↗
- 7Statin as a therapeutic agent in gastroenterological cancer World J Gastrointest Oncol Uemura N Hayashi H Baba H 1101231420223511610610.4251/wjgo.v 14.i 1.110PMC 8790423 · doi ↗ · pubmed ↗
- 8Recent advances and challenges in colorectal cancer: from molecular research to treatment World J Gastroenterol Qi GX Zhao RX Gao C Ma ZY Wang S Xu J 1069643120254053851610.3748/wjg.v 31.i 21.106964 PMC 12175868 · doi ↗ · pubmed ↗