A comparative study of online and face-to-face gatekeeper training using the suicide CARE program
Ah Rah Lee, Sung Moon Choi, Hwa-Young Lee, Soung Nam Kim, Jeungsuk Lim, Sang Min Lee, Jong-Woo Paik

TL;DR
This study compares online and in-person suicide prevention training for mental health workers in South Korea, finding both effective but with some differences in outcomes.
Contribution
The study provides evidence for the non-inferiority of online gatekeeper training compared to face-to-face delivery in suicide prevention.
Findings
Both online and face-to-face training improved knowledge, attitudes, and preparedness for suicide prevention.
Online training showed greater improvements in self-perceived knowledge and behaviors, while face-to-face improved factual knowledge more.
Hybrid models may offer the most comprehensive benefits for gatekeeper training.
Abstract
Gatekeeper training programs are essential public health strategies for suicide prevention. With the rapid digitization of health education, evaluating the effectiveness of online gatekeeper training relative to traditional face-to-face training has become increasingly important. This study compared the effectiveness of online and face-to-face formats of the standardized Suicide CARE 2.0 gatekeeper training in enhancing suicide prevention knowledge, attitudes, behaviors, and preparedness among community mental health workers in South Korea. We tested the non-inferiority of the online format in improving key outcomes. A quasi-experimental, two-group pre–post design was employed with 99 participants (51 face-to-face, 48 online) recruited from community mental health centers. Participants were randomly assigned to either the online or face-to-face gatekeeper training group using a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
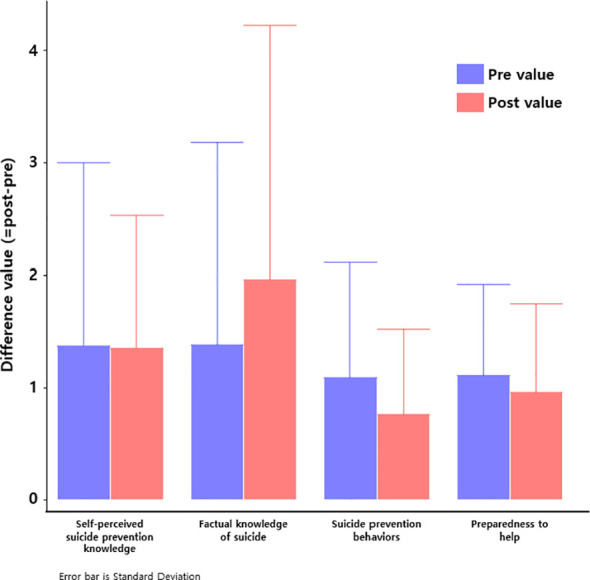 Figure 1
Figure 1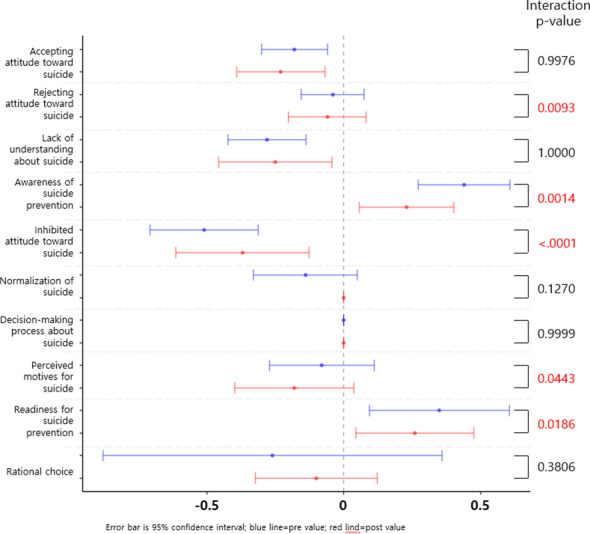 Figure 2
Figure 2| Variable | Total (n=99) | Online training | Face-to-Face training | P-value | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sex | Male | 44 | 44.4 | 28 | 58.3 | 16 | 31.4 | 0.0070 |
| Female | 55 | 55.6 | 20 | 41.7 | 35 | 68.6 | ||
| Age | Under 40 years | 47 | 47.5 | 19 | 39.6 | 28 | 54.9 | 0.1272 |
| 40 years or older | 52 | 52.5 | 29 | 60.4 | 23 | 45.1 | ||
| Educational Attainment | High School or Less | 35 | 35.4 | 15 | 35.4 | 10 | 19.6 | 0.1827 |
| College or Higher | 74 | 64.6 | 33 | 64.6 | 41 | 80.4 | ||
| Religious Affiliation | None | 53 | 53.5 | 27 | 56.3 | 26 | 51.0 | 0.5993 |
| Yes | 46 | 46.5 | 21 | 43.8 | 25 | 49.0 | ||
| Employment Type | Full-time | 65 | 66.6 | 31 | 64.6 | 34 | 66.7 | 0.3840 |
| Part-time | 9 | 9.1 | 3 | 6.3 | 6 | 11.8 | ||
| Self-employed / Employer | 6 | 6.1 | 5 | 10.4 | 1 | 2.0 | ||
| Unpaid Family Worker | 3 | 3.0 | 1 | 2.1 | 2 | 3.9 | ||
| Unemployed | 15 | 15.1 | 8 | 16.7 | 7 | 13.7 | ||
| Economic Status | Lower-middle or below | 26 | 26.3 | 14 | 29.2 | 12 | 23.5 | 0.6005 |
| Middle | 58 | 58.6 | 26 | 54.2 | 32 | 62.7 | ||
| Upper-middle or above | 14 | 14.1 | 8 | 16.7 | 6 | 11.8 | ||
| Variable | Group | Pre | Post | Difference (=post-pre)† | p-value of group†† |
|---|---|---|---|---|---|
| Self-perceived suicide prevention knowledge | Online | 2.68±1.54 | 4.05±1.36 | 1.37±1.63** | <.0001 |
| Face-to-Face | 3.73±1.27 | 5.08±1.04 | 1.35±1.18** | ||
| Knowledge of suicide | Online | 5.35±1.86 | 6.73±1.43 | 1.38±1.80*** | 0.0172 |
| Face-to-Face | 4.24±1.88 | 6.20±2.12 | 1.96±2.26*** | ||
| Suicide prevention behaviors | Online | 1.99±1.00 | 3.08±1.03 | 1.09±1.02*** | <.0001 |
| Face-to-Face | 3.10±0.95 | 3.86±0.67 | 0.76±0.76*** | ||
| Preparedness to help | Online | 2.16±0.93 | 3.27±0.92 | 1.11±0.81*** | <.0001 |
| Face-to-Face | 2.95±0.80 | 3.91±0.55 | 0.96±0.79*** |
| Variable | Group | Pre | Post | Difference (=post-pre)† | p-value of group†† |
|---|---|---|---|---|---|
| Accepting attitude toward suicide | Online | 2.92±0.59 | 2.74±0.60 | -0.18±0.44** | 0.9976 |
| Face-to-Face | 3.03±0.61 | 2.80±0.81 | -0.23±0.57** | ||
| Rejecting attitude toward suicide | Online | 3.59±0.61 | 3.55±0.70 | -0.04±0.42 | 0.0093 |
| Face-to-Face | 3.23±0.72 | 3.17±0.72 | -0.06±0.50 | ||
| Lack of understanding about suicide | Online | 3.18±0.40 | 2.90±0.51 | -0.28±0.52*** | 1.0000 |
| Face-to-Face | 3.14±0.50 | 2.89±0.74 | -0.25±0.73* | ||
| Awareness of suicide prevention | Online | 3.65±0.58 | 4.09±0.55 | 0.44±0.61*** | 0.0014 |
| Face-to-Face | 4.09±0.55 | 4.32±0.57 | 0.23±0.61* | ||
| Inhibited attitude toward suicide | Online | 2.73±0.63 | 2.22±0.69 | -0.51±0.72*** | <.0001 |
| Face-to-Face | 2.09±0.78 | 1.72±0.84 | -0.37±0.86** | ||
| Normalization of suicide | Online | 3.16±0.59 | 3.02±0.66 | -0.14±0.69 | 0.1270 |
| Face-to-Face | 3.31±0.64 | 3.31±0.82 | 0.00±0.00 | ||
| Decision-making process about suicide | Online | 2.88±0.51 | 2.88±0.54 | 0.00±0.00 | 0.9999 |
| Face-to-Face | 3.10±0.57 | 3.10±0.60 | 0.00±0.00 | ||
| Perceived motives for suicide | Online | 2.78±0.84 | 2.70±0.90 | -0.08±0.70 | 0.0443 |
| Face-to-Face | 2.48±0.67 | 2.30±0.67 | -0.18±0.77 | ||
| Readiness for suicide prevention | Online | 3.47±0.66 | 3.82±0.62 | 0.35±0.93* | 0.0186 |
| Face-to-Face | 3.81±0.62 | 4.07±0.85 | 0.26±0.76* | ||
| Rational choice | Online | 2.59±0.80 | 2.33±0.99 | -0.26±2.26 | 0.3806 |
| Face-to-Face | 2.30±0.83 | 2.20±1.06 | -0.10±0.79 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSuicide and Self-Harm Studies · Mental Health Treatment and Access · Digital Mental Health Interventions
Introduction
1
Suicide remains one of the most pressing public health concerns worldwide. South Korea continues to report the highest suicide rate among OECD countries, emphasizing the urgency of culturally relevant suicide prevention strategies (1). In response, gatekeeper training programs have been developed to train non-clinicians, such as educators, community workers, and family members, with the skills needed to recognize warning signs and refer high-risk individuals to professional help. In South Korea, the standardized gatekeeper training program known as “Suicide CARE (Careful Observation, Active Listening, Risk Evaluation and Expert Referral)” was introduced in 2011 to address cultural tendencies toward emotional suppression and to promote early suicide risk detection (2). The program has since trained over five million individuals and has evolved into multiple versions targeting specific groups such as adolescents, soldiers, teachers, and firefighters (2–4).
With the increasing integration of digital technologies into public health education, numerous studies have examined whether online gatekeeper training can achieve outcomes comparable to traditional face-to-face formats (5–7). While evidence suggests that both modalities are effective in improving suicide-related knowledge, attitudes, and self-efficacy (6), there remain concerns regarding the quality of learner engagement, long-term knowledge retention, and the affective depth of learning, especially in online formats (7). These concerns are particularly relevant because online programs often lack interpersonal interaction, emotional resonance, and experiential learning activities, like role-playing or group discussions, which are considered critical in suicide prevention training (7, 8). Furthermore, even in countries with mandated suicide prevention education, insufficient funding and poor quality control have led to superficial, checklist-based implementation, undermining the impact of such programs (9).
Against this background, this study evaluates whether an online delivery of the Suicide CARE program produces non-inferior outcomes when compared to face-to-face education. The core hypothesis is that, when the training content and instructional quality are held constant, online gatekeeper education can lead to equivalent gains in suicide prevention knowledge, attitudes, and behaviors. Establishing non-inferiority would support the scalability of online formats, particularly in resource-limited contexts or during public health emergencies, such as the COVID-19 pandemic.This study aimed to test whether online training is non-inferior to face-to-face training in improving suicide prevention knowledge, self-efficacy, and attitudes among community mental health workers.
Methods
2
Participants
2.1
Between July and December 2020, mental health professionals were recruited from community mental health centers and online platforms. Eligibility required current employment in the field and no gatekeeper training within the past year. Of 109 initial respondents, 99 completed both pre- and post-training assessments (face-to-face: n = 51; online: n = 48) and were included in the analysis. Participants were randomly assigned to either the online or face-to-face gatekeeper training group using a computerized randomization tool (www.randomizer.org). Baseline demographics (e.g., gender, age, education, religion, employment status, perceived economic status) were collected; only gender differed significantly between groups (p = 0.007). An a priori power analysis using G*Power 3.1, based on a medium effect size (Cohen’s d ≈ 0.50), indicated a minimum of 34 participants per group (α = 0.05, power = 0.80). The final sample exceeded this threshold, ensuring sufficient statistical power. All procedures adhered to the Declaration of Helsinki.
Study design and procedure
2.2
This study employed a single-session, pre-post design to compare the effectiveness of face-to-face versus online gatekeeper training using Suicide CARE Version 2.0, South Korea’s national suicide prevention curriculum (3, 4). Participants in both groups completed pre-training assessments (30 minutes), received a standardized 60-minute training session, and then completed post-training assessments (30 minutes). All training was conducted by the same certified instructor to control for instructor effects.
Intervention: suicide CARE version 2.0
2.3
The intervention was based on Suicide CARE Version 2.0, an evidence-based update of the national standard program (3, 4). This version includes three core modules: “Careful Observation,” which focuses on recognizing behavioral and verbal warning signs; “Active Listening,” which promotes empathetic dialogue with individuals at risk; and “Risk Evaluation and Expert Referral,” which teaches how to assess suicide risk and refer individuals to appropriate mental health services. The same content and instructor were used across both formats to ensure internal validity.
Measures
2.4
We assessed suicide prevention-related knowledge, attitudes, and behavioral intentions using a combination of validated and adapted instruments. Cronbach’s α values were calculated using the current study sample to assess internal consistency; the assessment tool comprised five subscales derived from validated instruments. Assessments were conducted immediately before and after the training session using structured self-report questionnaires. The Institutional Review Board approved the study protocol.
Self-perceived suicide prevention knowledge
2.4.1
Participants’ subjective understanding of suicide risk factors and intervention strategies was assessed using a 9-item scale adapted from Wyman et al. (10) and translated into Korean by Ryu (11). Items were rated on a 7-point Likert scale (1 = “Not at all” to 7 = “Very much”), with higher scores indicating greater self-perceived knowledge. This scale has demonstrated strong internal consistency and cross-cultural applicability. In the current study, Cronbach’s α was 0.88, indicating high reliability.
Factual knowledge about suicide
2.4.2
Objective suicide prevention knowledge was measured using 10 multiple-choice questions derived from the standardized “See, Listen, Speak” framework of the Korean Ministry of Health and Welfare (2). Each item was scored dichotomously (0 = incorrect, 1 = correct), with total scores ranging from 0 to 10. Higher scores reflected greater factual knowledge. The internal consistency of this scale in the current study was high (Cronbach’s α = 0.89).
Preparedness to help
2.4.3
Participants’ perceived readiness to assist individuals at risk of suicide was measured using a 4-item scale developed by Baber and Bean and translated by Kim H (12). Items were rated on a 5-point Likert scale (1 = “Strongly disagree” to 5 = “Strongly agree”), with higher scores reflecting greater preparedness. The scale demonstrated excellent reliability in this study (Cronbach’s α = 0.91).
Attitudes toward suicide
2.4.4
Attitudes were assessed using the Attitudes Toward Suicide Scale (ATTS), initially developed by Renberg and Jacobsson (13) and culturally adapted for Korea. The Korean version comprises 37 items across 10 subdomains (e.g., tabooing, preventability, normalization, autonomy), rated on a 5-point Likert scale. Higher scores in different subdomains indicate either stronger preventive attitudes or more permissive views, depending on item framing. In the present sample, subdomain reliabilities were acceptable.
Suicide prevention behaviors
2.4.5
Gatekeeper behavioral intentions were assessed using an 8-item measure developed by Kim J (14). based on the framework by Wyman et al. (10). Items reflect the likelihood of performing specific behaviors such as asking about suicide or referring someone to professional help. Responses were recorded on a 5-point Likert scale (1 = “Very unlikely” to 5 = “Very likely”). The scale showed strong internal consistency in this study (Cronbach’s α = 0.87).
Statistical analysis
2.5
Data were analyzed using IBM SPSS Statistics 26.0. Paired t-tests were used to evaluate within-group pre-post changes. Between-group differences were tested using ANCOVA, controlling for baseline scores. Effect sizes were reported as Cohen’s d (within-group) and partial η² (between-group), along with 95% confidence intervals. Statistical significance was set at p <.05.
Results
3
Participant characteristics
3.1
Of the 99 participants included in the final analysis, 51 were allocated to the face-to-face training group (51.5%) and 48 to the online group (48.5%). A significant gender imbalance was noted, with a higher proportion of females in the face-to-face group and males in the online group (χ² = 7.279, p = 0.007). No significant differences were observed between groups in age, education level, employment status, religious affiliation, or perceived economic status (Table 1).
Knowledge and preparedness
3.2.1
Both training modalities led to statistically significant improvements in all key domains: self-perceived knowledge, objective factual knowledge, preparedness to help, and behavioral intention (p < 0.001 for all measures). Effect sizes were medium to large (Cohen’s d = 0.58–0.94), indicating meaningful psychological and educational change.
The online group demonstrated greater gains in self-perceived knowledge (d = 0.74, 95% CI [0.47, 1.01]) and preparedness (d = 0.73, 95% CI [0.46, 0.99]), with significant group × time interactions (partial η² = 0.09 and 0.11, respectively), suggesting enhanced self-efficacy and confidence to intervene. These outcomes are practically substantial, as they reflect readiness to apply learned skills in real-world scenarios, an essential goal of gatekeeper training.
Conversely, the face-to-face group showed greater gains in objective knowledge (d = 0.94, 95% CI [0.68, 1.19]; partial η² = 0.07), suggesting that in-person formats may be more effective for delivering dense factual or technical content. These findings underscore the strengths of each modality, depending on the intended learning objectives (Table 2, Figure 1).
Pre-post differences in suicide prevention competencies across four domains. Bar graph displays mean changes from baseline to post-intervention in (1) self-perceived suicide prevention knowledge, (2) factual knowledge of suicide, (3) suicide prevention behaviors (behavioral intention), and (4) preparedness to help. Blue bars represent pre-intervention values; red bars represent post-intervention values. Error bars indicate standard deviations. All domains showed significant improvements from pre- to post- intervention (p<0.001), with the largest gains observed in factual knowledge and self-perceived preparedness.
Gatekeeper behavior
3.2.2
Both groups showed significant increases in their intention to engage in suicide prevention behaviors (p < 0.001). The online group exhibited a significantly larger change compared to the face-to-face group (d = 0.81, 95% CI [0.53, 1.09]; partial η² = 0.08, p < 0.0001). Given that behavioral change is the ultimate objective of gatekeeper education, this finding has strong practical relevance, supporting the utility of online formats for scalable implementation in resource-limited or remote settings.
Changes in attitudes toward suicide
3.3
Among the 10 subdomains assessed by the ATTS, both groups demonstrated improvements in accepting attitudes, prevention awareness, and readiness to intervene (d = 0.40–0.73; p < 0.01). The online group showed significantly greater reductions in inhibited attitudes (partial η² = 0.19, p < 0.0001), lack of understanding (η² = 0.08), and perceived motives for suicide (η² = 0.05), indicating its effectiveness in reshaping negative or stigmatizing beliefs.
While no significant group × time interactions were found for decision-making autonomy, normalization of suicide, or rational choice, modest within-group improvements were observed in both formats. These findings demonstrate that online education can influence not only knowledge and behavior but also complex affective and cognitive dimensions related to suicide prevention (Table 3, Figure 2). All relevant statistics, including means, standard deviations, t-test results, effect sizes, 95% confidence intervals, and interaction p-values are presented in Tables 2 and Table 3. Effect plots are visualized in Figures 1 and 2.
Pre-Post Evaluation of Attitudes Toward Suicide in the Online and Face-to-Face Gatekeeper Training Groups. Pre- (blue) and post-intervention (red) means with 95% confidence intervals are shown for each attitude subdomain. The x-axis indicates the change direction and magnitude. Interaction p-values reflect group x time effects (ANCOVA, adjusted for baseline). Significant between-group differences were observed in rejecting attitude, awareness, inhibited attitude, perceived motives, and readiness for prevention. See Table 3 for detailed statistics.
Discussion
4
The present study demonstrates that both face-to-face and online formats of the Suicide CARE 2.0 gatekeeper training significantly enhanced suicide-related knowledge, attitudes, and behavioral intentions among mental health professionals. These findings align with previous studies reporting comparable efficacy between online and traditional gatekeeper training (6, 7). Our findings also contribute to the growing literature supporting the scalability of e-health interventions for suicide prevention (15, 16).
Importantly, gatekeeper training programs, particularly those designed for non-clinicians such as educators and community workers, have consistently been shown to improve proximal outcomes such as increased suicide-related knowledge, preparedness, and willingness to intervene (8–10). These outcomes are especially critical in community and non-medical settings, where early detection can prevent suicidal crises from escalating.
In the Korean context, the Suicide CARE program has been culturally tailored and widely implemented, showing long-term efficacy and adaptability to various populations, including adolescents and frontline workers (3–5). Our results further validate the program’s effectiveness even when delivered digitally, suggesting promising implications for broader dissemination, especially in remote or underserved regions (11, 12).
While several studies support the long-term impact of gatekeeper interventions on attitudes and behavioral intentions, findings regarding sustained change are mixed (9, 10). This highlights the need for booster training and periodic reinforcement, particularly for attitudinal components such as reducing suicide stigma and increasing empathy toward high-risk individuals. Institutional-level factors such as administrative support, organizational readiness, and policy mandates have also been identified as critical to the success and sustainability of suicide prevention programs (17, 18). Integrating gatekeeper training into institutional structures, such as schools, hospitals, and community centers, may improve long-term sustainability and alignment with national mental health strategies (20).
Despite its strengths, the online delivery format may face challenges related to learner engagement, emotional immersion, and real-time interaction. Future research should explore hybrid or augmented models that combine the scalability of digital platforms with the interpersonal depth of face-to-face learning (15, 16, 20). Technological enhancements, such as video-based narratives, peer-led discussion, and AI-assisted feedback mechanisms, may further improve engagement and knowledge retention.
A notable strength of this study is the use of validated measures to ensure reliable outcome assessment across multiple domains. Additionally, having the same experienced instructor deliver training across both groups minimized variability in content delivery and controlled for instructor-related bias. The high response rates for both pre- and post-intervention surveys further indicate good participant adherence and internal validity, even amid the constraints of the COVID-19 pandemic.
Nonetheless, several limitations should be acknowledged. First, the sample consisted of highly motivated volunteers, which may limit the generalizability of findings to broader or less-engaged populations. Second, the study did not include measures of subjective satisfaction, engagement levels, or learner preferences, factors that could inform future digital content optimization and instructional design. Third, the short-term follow-up precluded evaluation of long-term skill retention or translation into real-world gatekeeping behaviors. Lastly, while the sample size was adequate to detect main effects, the power may have been insufficient for subgroup analyses, particularly for more nuanced attitudinal shifts.
From a policy perspective, our findings support the incorporation of gatekeeper training into national suicide prevention strategies. Online delivery, in particular, presents a scalable, cost-effective modality well suited for resource-limited settings, rural regions, and public health emergencies, including the COVID-19 pandemic (19). To ensure quality and sustainability, digital dissemination should be supported by standardized curricula, instructor certification programs, and continuous fidelity monitoring. Learning management systems and mobile-based reinforcement tools may further enhance engagement and long-term retention. Additionally, implementing national tracking systems for trained gatekeepers could improve post-training support and reduce attrition in suicide prevention competencies over time (8).
In conclusion, this study adds to the growing evidence base for the effectiveness and scalability of online gatekeeper training in suicide prevention. While face-to-face instruction continues to offer distinct cognitive and interpersonal benefits, digital formats are emerging as equally effective and more flexible alternatives, mainly when based on structured, theory-driven models such as Suicide CARE.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organisation for Economic Co-operation and Development (OECD). Suicide rates (indicator) (2024). Available online at: https://data.oecd.org/healthstat/suicide-rates.htm (Accessed August 31, 2025).
- 2Korean Suicide Prevention Association, Central Suicide Prevention Center. See, listen, speak: standardized korean suicide prevention program. Seoul: Ministry of Health and Welfare (2013).
- 3Lim SW Lee SH Park JI Lee SM Oh KS Paik JW. Suicide CARE (Standardized suicide prevention program for gatekeeper intervention in korea): an update. Psychiatry Investig. (2020) 17:911–24. doi: 10.30773/pi.2020.0166, PMID: 32933238 PMC 7538250 · doi ↗ · pubmed ↗
- 4Lee SM Park JI Hwang JW Oh KS Paik JW. Development of a standardized suicide prevention program for gatekeeper intervention in korea (Suicide CARE version 2.0) to prevent adolescent suicide: version for teachers. Psychiatry Investig. (2024) 21:860–9. doi: 10.30773/pi.2024.0081, PMID: 39111745 PMC 11321880 · doi ↗ · pubmed ↗
- 5Seol J Lee HY Lee SM Ki SW Cho SJ Oh KS. Evaluating the longitudinal efficacy of Suicide CARE in a general community sample: a randomized controlled trial. Psychiatry Investig. (2024) 21:1329–37. doi: 10.30773/pi.2024.0231, PMID: 39757812 PMC 11704805 · doi ↗ · pubmed ↗
- 6Liu H Zheng C Cao Y Zeng F Chen H Gao W. Gatekeeper training for suicide prevention: a systematic review and meta-analysis of randomized controlled trials. BMC Public Health. (2025) 25:1206. doi: 10.1186/s 12889-025-01206-5, PMID: 40165179 PMC 11956478 · doi ↗ · pubmed ↗
- 7Holmes G Clacy A Hermens DF Naismith SL Hickie IB Lagopoulos J. Online versus in-person gatekeeper suicide prevention training: a comparative study. J Ment Health. (2024) 33:100–8. doi: 10.1080/09638237.2023.2242102 38602188 · doi ↗ · pubmed ↗
- 8Holmes G Clacy A Hermens DF Naismith SL Hickie IB Lagopoulos J. Effectiveness of suicide prevention gatekeeper training: 12-month follow-up outcomes of Safe TALK training. Health Promot J Aust. (2023) 34:14–22. doi: 10.1002/hpja.753, PMID: 37824290 · doi ↗