A post-surgical case of rib osteomyelitis and pleural abscess caused by mycobacterium abscessus after 6 years of lung cancer surgery
Yoshikazu Mutoh, Tomonori Sato, Yuko Oya, Takumi Umemura, Tatsuya Hioki, Yasuhiko Yamano, Kensuke Kataoka, Toshiaki Matsuda, Tomoki Kimura, Toshihiko Ichihara, Yasuhiro Kondoh

TL;DR
A man developed a rare infection caused by Mycobacterium abscessus six years after lung cancer surgery, which was successfully treated with a long-term antibiotic regimen.
Contribution
This case highlights a rare instance of M. abscessus causing osteomyelitis and pleural abscess, offering insights into its treatment strategy.
Findings
M. abscessus was identified as the causative agent through PCR from a bone biopsy.
A 20-month combination antibiotic therapy successfully treated the infection without surgery.
Osteomyelitis caused by M. abscessus is extremely rare and requires prolonged treatment.
Abstract
A 69-year-old man followed post lung cancer surgery for 6 years presented with back pain. His imaging revealed a pleural abscess and rib osteomyelitis along with the surgical site. Therefore, bone biopsy and culture were performed and the organism was diagnosed as Mycobacterium abscessus by PCR method. As such, the combination antibiotics therapy initiated with imipenem, amikacin, and clarithromycin, and then continued with faropenem, minocycline, clarithromycin, and moxifloxacin for 20 months, successfully surpassing the disease without additional surgery. Although the number of non-tuberculosis mycobacterial infection has been increasing, osteomyelitis caused by M. abscessus is extremely rare. This time, we describe the clinical course and current treatment strategy for M. abscessus.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
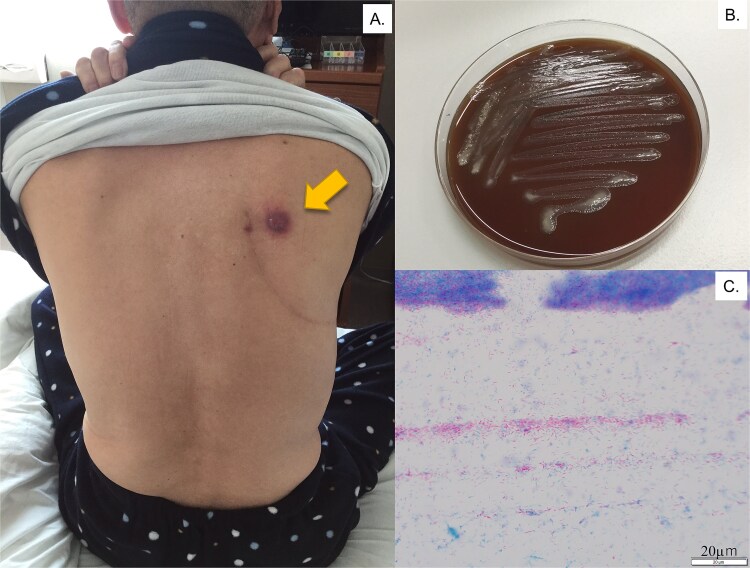 Figure 1
Figure 1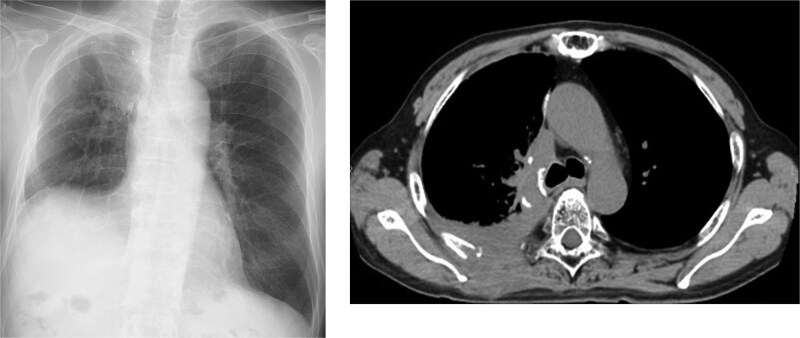 Figure 2
Figure 2| Agent | MIC(μg/mL) of our case | MIC (μg/mL) for category: | ||
|---|---|---|---|---|
| Susceptible | Intermediate | Resistant | ||
| streptomycin | 64 | |||
| ethambutol | 64 | |||
| kanamycin | 8 | |||
| rifampicin | 32 | |||
| rifabutin | 4 | |||
| levofloxacin | 8 | ≤ 1 | 2 | ≥ 4 |
| clarithromycin | > 32 | ≤ 2 | 4 | ≥ 8 |
| ethionamide | > 16 | |||
| amikacin | 8 | ≤ 16 | 32 | ≥ 64 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Tuberculosis · Diphtheria, Corynebacterium, and Tetanus
Introduction
Recently, a great deal of Non-tuberculous mycobacteria (NTM) infection has been reported globally. Among NTM species, M. abscessus complex, which classified three subspecies, is considered one of the challenging diseases from the points of diagnostic methods, selection of antibiotics, and appropriate treatment duration. Here, we reported a patient who presented with post-operative rib osteomyelitis and pleural abscess caused by M. abscessus 6 years after lung cancer surgery. Although osteomyelitis caused by this microorganism is extremely rare, aggressive long-term combination antibiotics therapy was able to suppress the infection fortunately. Robust treatment recommendations are warranted in the future.
Case report
A 69-year-old man was referred to the hospital with progressing right back pain and subcutaneous abscess persistent for 4 weeks (Fig. 1). The patient had also reported productive cough beginning a few days prior to consultation. Six years prior, he had a history of squamous cell carcinoma of his right upper lung with the stage of IIIA (cT3N1M0), then he subsequently received four cycles of chemotherapy with carboplatin and paclitaxel, along with concurrent radiation therapy (40 Gy). Thereafter, a right upper lobectomy via the 4th intercostal space, upper mediastinal lymph node dissection, and pulmonary angioplasty were performed. There has been no history of trauma or immunosuppressive therapy since the surgery. On examination, his vital signs were normal, and blood test showed a white blood cell count of 6800/μL and a C-reactive protein level of 3.5 mg/dL. His T-SPOT.TB test was negative and the tumor markers were within normal range. He reported no fever and no loss of body weight. Exudates were observed from subcutaneous nodules with erythema and induration on his back (Fig. 1A). A chest X-ray revealed pleural abscess in the right lung and infiltration behind his heart. A chest computed tomography (CT) image revealed an osteolytic lesion in the right fifth/sixth rib and an abscess involving latissimus dorsi muscle and subcutaneous tissue (Fig. 2). Three days after of transbronchial lung and bone biopsy and abscess culture from his back, acid-fast bacilli was found using Ziehl–Neelsen stain (Fig. 1B and C). The isolated bacteria were identified as M. abscessus (M. abscessus) complex using a DNA–DNA hybridization, and subsequently classified as M. abscessus subsp. abscessus or M. abscessus subsp. Bolletii, using a multiplex polymerase chain reaction assay detecting presence of erm (41) gene [1]. The minimal inhibitory concentration was evaluated by brothMIC NTM method, and the results (day3) was showed in Table 1. As such, the patient was hospitalized, then a 4-week course of intravenous imipenem, amikacin, and oral clarithromycin combination therapy was administered based on the guidelines [2]. Surgery was not performed because substantial postoperative adhesions were identified. Therefore, faropenem, minocycline, and clarithromycin, along with intravenous amikacin, were initiated and then replaced with moxifloxacin. Finally, 20 months of oral combination antibiotic treatment completed and as of 24 months after treatment completion, his symptom was completely resolved, and laboratory data showed no findings suggestive of recurrence.
Cutaneous lesion at presentation. (A) Exudates coming out from a nodule surrounded by erythema and swelling on the patient’s back (arrow). (B) Rough and dry morphologic colonies on chocolate agar, incubating for 48 h with CO2. (C) Acid-fast bacilli were observed on Ziehl-Neelsen stain.
Chest X-ray and computed tomography (CT) at the initiation of treatment. CT scan reveals an osteolytic lesion and an abscess extending into the subcutaneous tissue.
Discussion
We experienced a successful treated case of osteomyelitis and pleural abscess caused by M. abscessus, one of the species of rapidly growing mycobacterium (RGM), usually generate colonies on solid culture media within 7–14 days [3]. In a previous article reporting RGM surgical wound infection, all sixteen cases developed symptoms and had pathogens isolated within 3 weeks after surgery [4]. Additionally, the most probable causes of surgical site infection due to NTM are exposure to contaminated equipment or water during surgery. In contrast, our case presented clinical progression and yielded M. abscessus from the surgical site after 6 years of lung surgery. Surgical site infection caused by NTM should be considered in the differential diagnosis of patients suspected of cancer recurrence, even several years after surgery.
M. abscessus is classified into three distinct subspecies: M. abscessus subsp. abscessus,M. abscessus subsp. massiliense, and M. abscessus subsp. bolletii [5]. M. abscessus subsp. bolletii is considered to be responsible for less than 5% of M. abscessus complex infections [6]. In our case, osteomyelitis caused by M. abscessus, especially by M. abscessus subsp. abscessus or M. abscessus subsp. bolletii, is extremely rare.
The treatment of M. abscessus infection is not well established. The current guidelines for NTM pulmonary disease recommend more than one month of initial treatment including at least three active drugs (including azithromycin), followed by at least two to three active drugs, typically consisting of inhaled amikacin, azithromycin or clarithromycin, and oral antibiotics (such as clofazimine, linezolid, minocycline, moxifloxacin, and co-trimoxazole), as guided by antimicrobial susceptibility during continuation therapy [1, 7]. In our case, susceptibility testing was outsourced; therefore, we were not able to evaluate clarithromycin susceptibility after 14 days of incubation. However, the result at 3 days of incubation showed resistance.
In this case, although the microorganism was resistant to clarithromycin, intravenous amikacin, imipenem, and clarithromycin were initially selected in accordance with guidelines. Subsequently, we chose faropenem, minocycline and moxifloxacin. Faropenem, one of the oral β-lactam agent, has been expected to show efficacy against Mycobacterium tuberculosis, and previous reports have shown favorable outcome in the patient with M. abscessus pulmonary infection [8]. In addition, although minocycline, a tetracycline agent, has recently been reported to be inactive and lacking synergic effects with other antibiotics against M. abscessus [9], we selected it because this had been considered a potential oral treatment option in previous guidelines. As a result, we achieved sputum culture conversion, and the treatment was completed.
In conclusion, we experienced a case of rib osteomyelitis and pleural abscess caused by M. abscessus. Even several years after surgery, the pathogen may be isolated and misdiagnosed as recurrence of lung cancer. Moreover, since the treatment of M. abscessus remains controversial, the development of robust treatment recommendations is warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nakanaga K, Sekizuka T, Fukano H. et al. Discrimination of mycobacterium abscessus subsp. massiliense from mycobacterium abscessus subsp. abscessus in clinical isolates by multiplex PCR. J Clin Microbiol 2014;52:251–9.24197885 10.1128/JCM.01327-13PMC 3911466 · doi ↗ · pubmed ↗
- 2Haworth CS, Banks J, Capstick T. et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017;72:ii 1–ii 64. 10.1136/thoraxjnl-2017-21092929054853 · doi ↗ · pubmed ↗
- 3Pfyffer GE, Wittwer F. Incubation time of mycobacterial cultures: how long is long enough to issue a final negative report to the clinician? J Clin Microbiol 2012;50:4188–9. 10.1128/JCM.02283-1223052304 PMC 3502948 · doi ↗ · pubmed ↗
- 4Shah AK, Gambhir RP, Hazra N. et al. Non tuberculous mycobacteria in surgical wounds- a rising cause of concern? Indian J Surg 2010;72:206–10. 10.1007/s 12262-010-0057-923133248 PMC 3452638 · doi ↗ · pubmed ↗
- 5Bryant JM, Grogono DM, Greaves D. et al. Whole-genome sequencing to identify transmission of mycobacterium abscessus between patients with cystic fibrosis: a retrospective cohort study. Lancet. 2013;381:1551–60. 10.1016/S 0140-6736(13)60632-723541540 PMC 3664974 · doi ↗ · pubmed ↗
- 6Zelazny AM, Root JM, Shea YR. et al. Cohort study of molecular identification and typing of mycobacterium abscessus, Mycobacterium massiliense, and mycobacterium bolletii. J Clin Microbiol 2009;47:1985–95. 10.1128/JCM.01688-0819420162 PMC 2708513 · doi ↗ · pubmed ↗
- 7Daley CL, Iaccarino JM, Lange C. et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J 2020;56:2000535. 10.1183/13993003.00535-202032636299 PMC 8375621 · doi ↗ · pubmed ↗
- 8Tanaka E, Kimoto T, Tsuyuguchi K. et al. Successful treatment with faropenem and clarithromycin of pulmonary mycobacterium abscessus infection. J Infect Chemother 2002;8:252–5. 10.1007/s 10156-002-0176-812373490 · doi ↗ · pubmed ↗