Prevalence and Risk Factors of Postoperative Spinal Infections: A Five-year Study in Northwestern Iran
Seyed Taher Mousavi, Farhad Mirzaei, Mohammad Shimia, Moslem Shakeri

TL;DR
This study found a 6% infection rate after spinal surgery in northwestern Iran and identified risk factors like diabetes and long surgery times.
Contribution
The study identifies specific risk factors for postoperative spinal infections in a regional population in Iran.
Findings
Postoperative spinal infections occurred in 6% of patients.
Staphylococcus aureus was the most common pathogen.
Diabetes and prolonged surgery duration were the strongest risk factors.
Abstract
Surgical site infections (SSIs), particularly after spinal procedures, remain a major concern despite advances in infection control. This study aimed to determine the prevalence and associated risk factors of postoperative spinal infections in northwestern Iran. A cross-sectional study was conducted on 500 adult patients (≥18 years) who underwent spinal surgery in two referral hospitals in Tabriz (Imam Reza and Shohada) between March 2019 and February 2024. Postoperative infections were confirmed by infectious disease specialists. Data on demographics and surgical variables (including surgical site, approach, duration, blood loss, and transfusion) were collected using a standardized checklist. Statistical analyses were conducted in SPSS version 23.0 using Chi-squared and independent samples t-tests. Logistic regression was performed to estimate adjusted odds ratios (ORs) with 95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
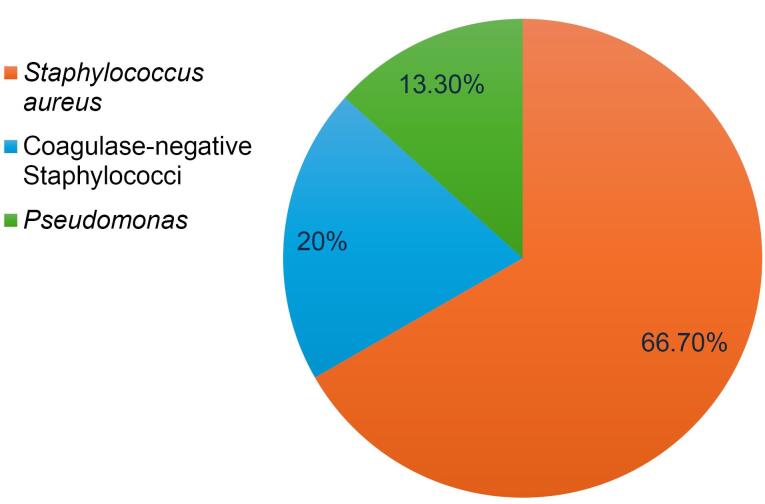 Figure 1
Figure 1|
|
|
|
| Gender | Male | 155 (31.0) |
| Female | 345 (69.0) | |
| Smoking | No | 422 (84.4) |
| Yes | 78 (15.6) | |
| History of surgery | No | 450 (90.0) |
| Yes | 50 (10.0) | |
| History of corticosteroid use | No | 414 (82.8) |
| Yes | 86 (17.2) | |
| History of hypertension | No | 376 (75.2) |
| Yes | 124 (24.8) | |
| History of diabetes | No | 430 (86.0) |
| Yes | 70 (14.0) | |
|
|
| |
| Age (years) | 42.78 (5.5) | |
| Weight (kg) | 82.18 (6.5) | |
|
|
|
|
| Surgical site | Lumbosacral | 375 (75.0) |
| Cervical | 100 (20.0) | |
| Thoracic | 25 (5.0) | |
| Approach | Posterior | 425 (85.0) |
| Anterior | 65 (13.0) | |
| Anteroposterior | 10 (2.0) | |
| Surgical method | Laminectomy | 150 (30.0) |
| Fusion and laminectomy | 225 (45.0) | |
| Laminectomy and diskectomy | 125 (25.0) | |
| Surgical duration | Less than 2 h | 150 (30.0) |
| 2‒4 h | 250 (50.0) | |
| More than 4 h | 100 (20.0) | |
| Blood loss volume | Less than 600 cc | 310 (62.0) |
| Between 600 cc and 1 liter | 125 (25.0) | |
| More than 1 liter | 65 (13.0) | |
| Blood transfusion | None | 325 (65.0) |
| 1 unit | 115 (23.0) | |
| 2 units | 60 (12.0) | |
|
|
| |
| CRP | 10.78 (2.1) | |
| ESR | 10.16 (2.5) | |
|
|
|
|
|
|
|
|
| Gender | Male | 6 | 149 | 155 | 3.87 |
|
| Female | 24 | 321 | 345 | 6.96 | ||
| Smoking | No | 12 | 410 | 422 | 2.84 | 0.230* |
| Yes | 18 | 60 | 78 | 23.08 | ||
| History of surgery | No | 13 | 437 | 450 | 2.89 | 0.390* |
| Yes | 17 | 33 | 50 | 34.00 | ||
| History of corticosteroid use | No | 7 | 407 | 414 | 1.69 |
|
| Yes | 23 | 63 | 86 | 26.74 | ||
| History of hypertension | No | 15 | 361 | 376 | 3.99 | 0.190* |
| Yes | 15 | 109 | 124 | 12.10 | ||
| History of diabetes | No | 5 | 425 | 430 | 1.16 |
|
| Yes | 25 | 45 | 70 | 35.71 | ||
|
|
|
|
| |||
| Age | 55.18 (6.8) | 34.29 (2.5) |
| |||
| Weight | 83.22 (8.2) | 78.38 (4.5) | 0.680** | |||
|
|
|
|
|
|
|
|
| Surgical site | Lumbosacral | 13 | 362 | 375 | 3.47 | 0.125* |
| Cervical | 12 | 88 | 100 | 12.0 | ||
| Thoracic | 5 | 20 | 25 | 20.0 | ||
| Approach | Posterior | 14 | 411 | 425 | 3.29 | 0.361* |
| Anterior | 14 | 51 | 65 | 21.54 | ||
| Anteroposterior | 2 | 8 | 10 | 20.0 | ||
| Surgical method | Laminectomy | 6 | 144 | 150 | 4.0 | 0.411* |
| Fusion and laminectomy | 12 | 213 | 225 | 5.33 | ||
| Laminectomy and diskectomy | 12 | 113 | 125 | 9.6 | ||
| Surgical duration | Less than 2 h | 5 | 145 | 150 | 3.33 |
|
| 2‒4 h | 5 | 250 | 255 | 1.96 | ||
| More than 4 h | 20 | 80 | 100 | 20.0 | ||
| Blood loss volume | Less than 600 cc | 6 | 304 | 310 | 1.94 |
|
| Between 600 cc and 1 liter | 6 | 119 | 125 | 4.8 | ||
| More than 1 liter | 18 | 47 | 65 | 27.69 | ||
| Blood transfusion | None | 5 | 320 | 325 | 1.54 |
|
| 1 unit | 7 | 108 | 115 | 6.07 | ||
| 2 units | 18 | 42 | 60 | 30.0 | ||
|
|
|
|
| |||
| CRP | 9.73 (4.1) | 10.21 (2.0) | **0.528 | |||
| ESR | 11.16 (3.5) | 10.01 (2.1) | **0.633 | |||
|
|
|
| |
|
|
| ||
| Gender | Male | 1.50 (0.70 – 3.20) | 0.30 |
| Female | Ref | Ref | |
| Smoking | Yes | 3.80 (1.60 – 8.90) | 0.003 |
| No | Ref | Ref | |
| History of surgery | Yes | 3.00 (1.20 – 7.50) | 0.020 |
| No | Ref | Ref | |
| History of corticosteroid use | Yes | 4.20 (1.70 – 10.30) | 0.002 |
| No | Ref | Ref | |
| History of hypertension | Yes | 2.10 (0.90 – 4.80) | 0.080 |
| No | Ref | Ref | |
| History of diabetes | Yes | 5.90 (2.30 – 15.20) | < 0.001 |
| No | Ref | Ref | |
| Surgical site | Cervical | 3.70 (1.40 – 9.70) | 0.008 |
| Thoracic | 6.80 (2.20 – 21.30) | 0.001 | |
| Lumbosacral | Ref | Ref | |
| Approach | Anterior | 7.40 (2.90 – 18.70) | < 0.001 |
| Anteroposterior | 6.80 (1.30 – 35.40) | 0.022 | |
| Posterior | Ref | Ref | |
| Surgical method | Fusion and laminectomy | 2.10 (0.80 – 5.70) | 0.130 |
| Laminectomy and diskectomy | 2.40 (0.90 – 6.60) | 0.086 | |
| Laminectomy | Ref | Ref | |
| Surgical duration | 2‒4 h | 0.60 (0.18 – 2.00) | 0.41 |
| > 4 h | 6.90 (2.50 – 19.00) | < 0.001 | |
| < 2 h | Ref | Ref | |
| Blood loss volume | 600 cc - 1 liter | 2.30 (0.80 – 6.80) | 0.11 |
| > 1 liter | 18.50 (7.00 – 48.80) | < 0.001 | |
| < 600 cc | Ref | Ref | |
| Blood transfusion | 1 unit | 3.90 (1.20 – 12.30) | 0.024 |
| 2 units | 25.50 (8.60 – 75.60) | < 0.001 | |
| None | Ref | Ref | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Orthopedic Infections and Treatments · Infectious Diseases and Tuberculosis
Introduction
Despite significant advances in medical care, particularly in surgical techniques, managing postoperative infectious complications remains one of the major challenges in healthcare systems.^1^ Surgical site infections (SSIs) are the most prevalent infectious complication in surgical wards and the second most frequent type of hospital-acquired infection, accounting for approximately 25% of all hospital infections.^2^ The occurrence of these infections could lead to treatment failure, prolonged hospitalization, increased healthcare costs and even mortality.^3^
Previous studies have demonstrated that numerous factors contribute to the development of SSIs, which could be broadly categorized into patient- and surgery-related factors.^4^ The first category includes host-related factors, which are often non-modifiable or difficult to control. These factors include old age, obesity, diabetes, smoking, previous surgeries or infections at the same site, previous radiation therapy, chronic skin conditions such as psoriasis, immune and nutritional status and adherence to postoperative care.^5^ In the second category, surgical factors, such as type of surgery (e.g. posterior approach), placement of metallic implants, bone graft harvesting, excessive bleeding, duration of surgery, adherence to sterile techniques, traffic in the operating room, instrument contamination and use of intraoperative fluoroscopy, are key factors that contribute to the development of infections. Moreover, the rising prevalence of resistant pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) and gram-negative bacteria has further complicated this challenge.^6^
Among various types of surgeries, spinal surgeries are at higher risk for SSIs due to their complexity, prolonged operative duration and patients’ specific conditions (such as old age, chronic diseases, or use of immunosuppressive medications).^7,8^ SSIs are considered the third most prevalent complication following spinal surgeries.^9,10^ These infections result in patient readmission, adverse outcomes and substantial additional costs. In the United States, this issue results in an estimated 10 billion in direct and indirect medical costs annually and is associated with approximately 8,000 deaths per year.^11^ Additional risk factors for infection in these patients include the use of drains and catheters, hospitalization for more than 48 h, revision surgeries and the need for blood transfusions. Some studies have reported postoperative infection rates of up to 12% following spinal surgery, which is considerably higher than those observed after other types of surgical procedures.^12,13^ However, despite this broad body of literature, there is considerable variability in the methods, populations, and definitions used across studies, making comparisons and generalizations difficult.^14,15^ Additionally, many studies fail to quantify the relative impact of individual risk factors or control for confounding variables, which limits their practical applicability.^16^ These limitations highlight the need for more structured and context-specific evaluations.
In addition, most existing literature comes from high-income countries, and there is a noticeable lack of regional data from the Middle East and North Africa (MENA) region, including Iran. Despite the clinical importance of SSIs in these settings, epidemiological studies specifically focusing on spinal surgeries remain scarce, fragmented, or outdated.^17^ Moreover, previous studies often remain descriptive and do not offer critical analysis regarding the relative impact or interaction of various risk factors. This lack of analytical perspective makes it difficult to prioritize interventions or adapt global guidelines to local contexts.
Even with the implementation of preventive strategies (such as prophylactic antibiotics, strict sterilization protocols, and staff training) a substantial number of postoperative spinal infections continue to occur. In low- and middle-income countries, one major reason for this is the limited availability of reliable data regarding both the prevalence and the specific risk factors relevant to local clinical settings.^17^ Lack of accurate data regarding the prevalence and relative contribution of each risk factor seems to be among the main reasons for the insufficient control of these complications.^18^ Documenting the prevalence of postoperative spinal infections is of particular importance for several reasons, including preoperative consultation with the patient, improving the quality of services and, in some cases, addressing legal issues.^19-21^
Therefore, to address this gap in both regional epidemiology and analytical evaluation of risk factors, the present study was conducted to investigate the prevalence of postoperative infections following spinal surgeries and identify the associated risk factors in two major teaching and treatment centers in Tabriz, namely Imam Reza and Shohada hospitals, which serve as specialized and subspecialized referral centers in northwestern Iran.
Materials and Methods
Study Design, Setting and Sampling
This cross-sectional study was conducted on the medical records of patients undergoing spinal surgeries in two specialized referral centers, Imam Reza and Shohada hospitals, in Tabriz, northwestern Iran, from March 2019 to February 2024. The minimum sample size was estimated to be 100 patients with postoperative infections using Cochran’s formula, considering α = 0.05, absolute error (d) of 0.1 and P = 0.5. However, all eligible medical records within the study period were included using a census sampling method, resulting in a total sample size of 500 patients. This approach was chosen to enhance the statistical power and generalizability of the findings. Inclusion criteria were patients over 18 years of age who had undergone spinal surgery, availability of clinical documentation, including laboratory results (CBC, ESR and CRP), pre- and postoperative radiographic images, a detailed surgical report in the medical records and documented pre- and postoperative clinical examinations. Records with missing essential data (such as laboratory results or surgical reports) were excluded from the study.
After obtaining ethical approval and access to the hospitals’ medical archives, the researcher (a trained resident) systematically reviewed and identified all spinal surgery records. Data were collected through manual review of both electronic and paper-based medical records, as the hospital archives contained a mix of structured electronic data and unstructured paper files. In the initial phase, records containing diagnoses and surgical reports were extracted. Subsequently, cases with a confirmed diagnosis of SSIs, verified by an infectious disease specialist, were identified. The diagnosis of SSIs was based on clinical signs and symptoms, supported by microbiological confirmation through laboratory cultures when available, and validated by an infectious disease specialist to ensure diagnostic accuracy. Patient data were recorded in a standard data collection checklist and later reviewed by the research team to enhance accuracy. To reduce potential information bias, data extraction was independently performed by two researchers and discrepancies were resolved through discussion and review by a third investigator.
The checklist consisted of two main sections. The first section included demographic and background information such as gender, age, history of diabetes and hypertension, body mass index (BMI), smoking status, use of immunosuppressive medications, history of previous surgeries (none, one, or multiple), history of previous SSIs, and preoperative white blood cell (WBC) count and C-reactive protein (CRP) levels.
The second section covered surgical details including the surgical site (cervical, thoracic, lumbar, or sacral), type of surgery (discectomy, decompression, fusion, osteotomy, or debridement), surgical duration (categorized as less than 2 hours, 2–4 hours, or more than 4 hours, with “longer surgery duration” defined as more than 4 hours), blood loss volume (defined as less than or more than 1 liter), and number of blood transfusion units (categorized as none, one unit, two units, or more than two units). The timing of blood transfusion was not included in the present analysis.
This observational study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist to ensure transparency and completeness in reporting.
Statistical Analysis
The data were analyzed using SPSS 23.0. The normality of quantitative variables was first assessed using Kolmogorov-Smirnov test. For the description of quantitative variables (if normally distributed), mean and standard deviation were used, while frequency and percentage were used for qualitative variables. The correlation between qualitative variables and occurrence of infection was examined using the Chi-squared test. The difference in quantitative variables between the two groups (infected and non-infected) was assessed using the independent samples t-test. Additionally, to identify independent risk factors associated with postoperative spinal infections, a multivariate logistic regression analysis was performed, reporting adjusted odds ratios (ORs) with 95% confidence intervals (CIs) and the corresponding *P *values. A *P *value of less than 0.05 was considered statistically significant.
Results
Demographic and Background Characteristics of the Study Sample
As shown in Table 1, the mean age of the patients was 42.78 years ( ± 5.5), with an approximate age range of 26 to 59 years, and their mean weight was 82.18 kg ( ± 6.5). In terms of gender, 69% were female and the remaining were male. Smoking was reported in 15.6% of the patients, history of previous surgeries in 10%, history of corticosteroid use in 17.2%, diabetes mellitus in 14% and hypertension in 24.8%.
Surgical and Therapeutic Characteristics of the Study Sample
In this study, the mean (standard deviation) levels of preoperative inflammatory markers, including CRP and ESR, were reported at 10.78 ( ± 2.1) and 10.16 ( ± 2.5), respectively. The lumbosacral region (75%) was the most common surgical site, and the posterior approach (85%) was the most frequently applied approach. A combination of fusion and laminectomy (45%) was the predominant surgical method among the participants. Surgical duration lasted 2‒4 h in half of the patients (50%). Blood loss was less than 600 mL in more than half of the patients (62%). Additionally, 65% of the patients did not require blood transfusions. Further details on surgical and therapeutic characteristics are presented in Table 2.
Prevalence of Infections Following Spinal Surgeries in the Study Sample
Overall, 30 patients (6% of the total sample) developed SSIs following spinal surgeries. Staphylococcus aureus was the most common infectious agent among the participants, followed by coagulase-negative staphylococci and Pseudomonas (Figure 1).
**
Comparison of Demographic and Background Variables Between the Two Patient Groups
Table 3 compares the demographic and background variables between infected and non-infected groups. The infection rate among females was 6.96%, compared to 3.87% among males (P = 0.021). Patients with a history of corticosteroid use had an infection rate of 26.74%, versus 1.69% in those without (P = 0.042). Similarly, the infection rate was 35.71% among diabetics compared to 1.16% in non-diabetics (P = 0.002). No significant differences were observed regarding weight, smoking status, history of previous surgeries, or hypertension (P > 0.05).
Comparison of Surgical and Therapeutic Variables Between the Two Patient Groups
Table 4 presents the comparison of the surgical and therapeutic variables between patients with and without postoperative infections. As shown in the table, a surgical duration of more than 4 hours (with 20.0% infection rate in this group, P = 0.022), blood loss volume exceeding 1 liter (27.69% infection rate, P = 0.009), and receiving two units of blood transfusion (30.0% infection rate, P = 0.040) were significantly associated with the occurrence of SSIs. However, no significant correlation was found between postoperative infections and preoperative CRP and ESR levels, surgical site, surgical approach, or surgical method (P > 0.05).
Table 5 presents the results of the multivariate logistic regression analysis evaluating independent risk factors associated with postoperative spinal infections. Adjusted ORs with their corresponding 95% CIs and P-values are reported for each category of the studied variables, with the reference groups clearly indicated. The analysis revealed that smoking significantly increases the risk of infection, with an adjusted OR of 3.80 (95% CI: 1.60 to 8.90, P = 0.003). A history of previous surgery and corticosteroid use were also significant risk factors, with adjusted ORs of 3.00 (95% CI: 1.20 to 7.50, P = 0.020) and 4.20 (95% CI: 1.70 to 10.30, P = 0.002), respectively. Diabetes mellitus demonstrated the strongest association with postoperative infection, with an adjusted OR of 5.90 (95% CI: 2.30 to 15.20, P < 0.001). Surgical site played an important role as well, with surgeries performed in the cervical and thoracic regions associated with higher infection risks compared to the lumbosacral region (adjusted ORs 3.70 and 6.80, respectively). Furthermore, surgical duration exceeding four hours and blood loss greater than one liter were strongly linked to increased infection risk, with adjusted ORs of 6.90 (P < 0.001) and 18.50 (P < 0.001), respectively. Blood transfusion was also a significant factor, with receiving one or two units increasing the infection risk (adjusted ORs of 3.90 and 25.50, respectively). Other variables such as male gender, history of hypertension, and surgical methods showed elevated ORs but did not reach statistical significance. These findings emphasize the importance of managing comorbidities like diabetes and corticosteroid use, along with optimizing surgical factors such as minimizing operative time and blood loss, to reduce the likelihood of postoperative spinal infections.
Discussion
The present study was conducted to investigate the prevalence of postoperative infections following spinal surgeries and the contributing factors. The results indicated postoperative infections occurred in 30 cases (6%). These findings were consistent with those of numerous similar national and international studies, suggesting that the prevalence of SSIs following spinal surgeries is similar across different countries and healthcare centers, despite some differences in infection rates and pathogen types. For example, Zarei et al reported a relatively low infection rate (6.8% in the case group and 4.5% in the control group) from Al-Zahra Hospital in Isfahan.^22^ In the study by Nota et al on 5,761 patients, the incidence of postoperative infections within 90 days was reported at 6%.^23^ These alignments suggest homogeneity in the factors contributing to infection rates. However, some studies have reported differing results, which may be attributed to factors such as type of surgeries, geographical location, sample size and patient inclusion criteria. For example, in the study by Al-Gamdi et al in Saudi Arabia, the infection rate was 4%.^24^ In the studies by Liu et al in the United States^25^ and Abolfotouh et al in Africa,^17^ the infection rates were 2.4% and 4.2%, respectively. These observed differences underscore the heterogeneity across healthcare systems, which may reflect variations in surgical infrastructure, ICU admission policies, antibiotic stewardship, and infection control protocols. Without accounting for these contextual differences, direct comparisons between settings may be limited in interpretability.
In the present study, among the common microbial factors, S. aureus, coagulase-negative staphylococci and Pseudomonas were identified as the most common pathogens associated with infections, respectively. In contrast, the study by Fakour et al in Razi hospital in Ahvaz reported Pseudomonas as the most common causative agent of infection, likely due to differences in settings and types of surgeries performed.^26^ Durkin et al found that the most common pathogens included S. aureus, coagulase-negative staphylococci and Escherichia coli.^27^ These differences may be attributed to variations in environmental conditions, study designs, populations studied and care practices at different centers, all of which could influence the final results. Such microbial variations could be also influenced by local antimicrobial policies, availability of infection surveillance systems, and differences in surgical asepsis standards, which were not consistently reported across studies.
Importantly, this study went beyond descriptive statistics by presenting adjusted ORs for several independent risk factors. Among patient-related variables, diabetes mellitus emerged as the strongest risk factor for postoperative spinal infections (adjusted OR = 5.90; 95% CI: 2.30–15.20; P < 0.001). Corticosteroid use was also significantly associated with infection (adjusted OR = 4.20; 95% CI: 1.70–10.30; P = 0.002), as was smoking (adjusted OR = 3.80; 95% CI: 1.60–8.90; P = 0.003), and prior surgery (adjusted OR = 3.00; 95% CI: 1.20–7.50; P = 0.020). In terms of surgical factors, longer surgical duration ( > 4 hours) showed a strong association with infection (adjusted OR = 6.90; P < 0.001), as did blood loss exceeding 1 liter (adjusted OR = 18.50; P < 0.001). Blood transfusion further increased the risk significantly, especially in patients receiving two units (adjusted OR = 25.50; P < 0.001). Surgical site was another determinant: surgeries in the thoracic (adjusted OR = 6.80) and cervical (adjusted OR = 3.70) regions had higher risks compared to the lumbosacral region. The strength of these associations highlights the importance of risk stratification, but also points to the need for further studies that control for setting-specific practices, such as surgical team experience, infection prevention protocols, and postoperative ICU care.
Consistent with our findings, Najafizadeh et al identified advanced age and a history of chemotherapy or radiotherapy as factors contributing to the occurrence of infection.^28^ However, in contrast to our results, no significant correlation was observed between infection and variables such as gender, smoking and diabetes. Furthermore, our findings were in line with other research that has confirmed the role of diabetes as a contributing factor to infections. Karamouzian et al identified diabetes as the most important risk factor for deep wound infections.^29^ Also, Soroush et al reported factors such as surgical duration, presence of drains, steroid use and low hemoglobin levels as independent predictors of infection.^30^ Mosleh et al reported a higher prevalence of infection among male patients and those under 35 years of age, particularly in emergency surgeries.^31^ Hojjat et al found a significant correlation between surgical wound infection and factors such as type of fracture, smoking, surgical duration, type of surgery and length of hospital stay.^32^ Additionally, Al-Gamdi et al showed that factors such as hypertension, prolonged hospital stay, prolonged surgical duration and use of multiple blood units play a significant role in increasing the risk of infection.^24^ Furthermore, Abolfotouh et al identified factors such as diabetes, smoking, reconstructive surgery and prolonged hospital stay as significant contributors to the occurrence of postoperative infections.^17^ Dong et al reported advanced age, prolonged surgical duration, blood loss exceeding 1,000 mL and history of diabetes as factors associated with an increased risk of SSIs.^33^ Similarly, Liu et al identified factors such as diabetes, low albumin and calcium levels, prolonged surgical duration, increased blood loss and decreased hemoglobin as major predictors of SSIs.^25^ These comparative findings, while valuable, should be interpreted cautiously due to likely heterogeneity in patient case-mix, surgical subspecialties, and hospital-level infection monitoring protocols that may not have been standardized across studies.
Finally, it should be noted that the observed differences in findings may be attributed to several factors, including geographical location, sample size, type of surgeries, patients’ demographic characteristics, and differences in inclusion and exclusion criteria across studies. These differences could account for the discrepancy between our results and those of other studies.
The results of this study, along with previous evidence, emphasize the importance of identifying high-risk patients before the surgery, closely monitoring patients during the procedure and ensuring the control of patient safety conditions. Using infection control protocols, reducing surgical duration and optimizing patient conditions before the surgery could help reduce the incidence of infections. Despite its significance, the present study has several limitations. First, its retrospective and cross-sectional design only allows for identification of associations, limiting causal inference and introducing potential biases inherent to retrospective data collection. Second, the study was conducted in a single region in northwestern Iran, which may affect the generalizability of the findings to other geographical areas or populations. Third, the microbial resistance profiles of isolated pathogens were not assessed, which could have provided important insights into treatment challenges. Finally, clinical outcomes related to postoperative infections, such as length of hospital stay or functional recovery, were not reported. Future research should aim to include multi-center data from diverse healthcare systems and explicitly examine how structural variations (such as ICU protocols, preoperative optimization strategies, and antibiotic stewardship) may affect infection rates. Prospective longitudinal design, broader geographic coverage, and inclusion of antimicrobial resistance and clinical outcomes are recommended.
Conclusion
In this study, the prevalence of postoperative spinal infections was reported at 6%. The most common microbial factors associated with infections were S. aureus, coagulase-negative staphylococci and Pseudomonas, in decreasing order of frequency. Data analysis revealed that certain variables, such as female gender, history of corticosteroid use, diabetes mellitus, surgical duration exceeding 2 hours, blood loss greater than 1 liter and receiving at least 2 units of blood transfusion, were significantly associated with an increased risk of postoperative infections. Additionally, the mean age of patients with infections was significantly higher than that of patients without infections. However, no significant correlation was found between the occurrence of infection and other variables, including weight, smoking, surgical history, hypertension, CRP, ESR, surgical site, type of approach or surgical method. Conducting further studies in other regions of the country could help identify factors influencing postoperative infections, develop preventive strategies and improve the quality of healthcare services in this field.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Järbrink K Ni G Sönnergren H Schmidtchen A Pang C Bajpai R Prevalence and incidence of chronic wounds and related complications: a protocol for a systematic review Syst Rev 20165115210.1186/s 13643-016-0329-y 27609108 PMC 5017042 · doi ↗ · pubmed ↗
- 2Woo K Song J Adams V Block LJ Currie LM Shang J Exploring prevalence of wound infections and related patient characteristics in homecare using natural language processing Int Wound J 20221912112110.1111/iwj.1362334105873 PMC 8684883 · doi ↗ · pubmed ↗
- 3Reddy M Gill SS Wu W Kalkar SR Rochon PA Does this patient have an infection of a chronic wound?JAMA 201230766051110.1001/jama.2012.9822318282 · doi ↗ · pubmed ↗
- 4Schimmel JJ Horsting PP de Kleuver M Wonders G van Limbeek J Risk factors for deep surgical site infections after spinal fusion Eur Spine J 201019101711910.1007/s 00586-010-1421-y 20445999 PMC 2989231 · doi ↗ · pubmed ↗
- 5Martinengo L Olsson M Bajpai R Soljak M Upton Z Schmidtchen A Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies Ann Epidemiol 20192981510.1016/j.annepidem.2018.10.00530497932 · doi ↗ · pubmed ↗
- 6Nampiaparampil DE Prevalence of chronic pain after traumatic brain injury: a systematic review JAMA 20083006711910.1001/jama.300.6.71118698069 · doi ↗ · pubmed ↗
- 7Schuster JM Rechtine G Norvell DC Dettori JR The influence of perioperative risk factors and therapeutic interventions on infection rates after spine surgery: a systematic review Spine (Phila Pa 1976)2010359 Suppl S 1253710.1097/BRS.0b 013e 3181 d 8342 c 20407344 · doi ↗ · pubmed ↗
- 8Weinstein MA Mc Cabe JP Cammisa FP Jr Postoperative spinal wound infection: a review of 2,391 consecutive index procedures J Spinal Disord 2000135422610.1097/00002517-200010000-0000911052352 · doi ↗ · pubmed ↗