A Systematic Review of the Bidirectional Relationship Between Post-traumatic Stress Disorder (PTSD) and the Development of Type 2 Diabetes
Naif Aleid, Ibrahim Enad Alenazi, Fahad Saleh Alghasham, Saud Abdulmajeed Bin Rakhis, Abdulraham Mansour A AlFawaz

TL;DR
This review explores how PTSD and type 2 diabetes influence each other, highlighting shared biological and behavioral factors and suggesting integrated care for high-risk groups.
Contribution
The paper systematically reviews the bidirectional relationship between PTSD and T2D, emphasizing mechanisms and disparities in vulnerable populations.
Findings
PTSD increases T2D risk and is linked to worse glycemic control (elevated HbA1c).
T2D populations show higher PTSD prevalence, especially among women, refugees, and veterans.
Biological pathways like HPA axis dysregulation and chronic inflammation mediate the PTSD-T2D link.
Abstract
Emerging evidence suggests a bidirectional relationship between post-traumatic stress disorder (PTSD) and type 2 diabetes (T2D), though the underlying mechanisms and population-specific risks remain unclear. This systematic review synthesizes current research on the PTSD-T2D link, focusing on biological pathways, behavioral mediators, and demographic disparities. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we conducted a comprehensive search across PubMed/Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica database (Embase), PsycINFO, and Web of Science. Eligible studies examined PTSD as a risk factor for T2D or vice versa in adults (≥18 years). Two reviewers independently screened articles, extracted data, and assessed bias using the Newcastle-Ottawa Scale (NOS) and Cochrane tools. Thirteen studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
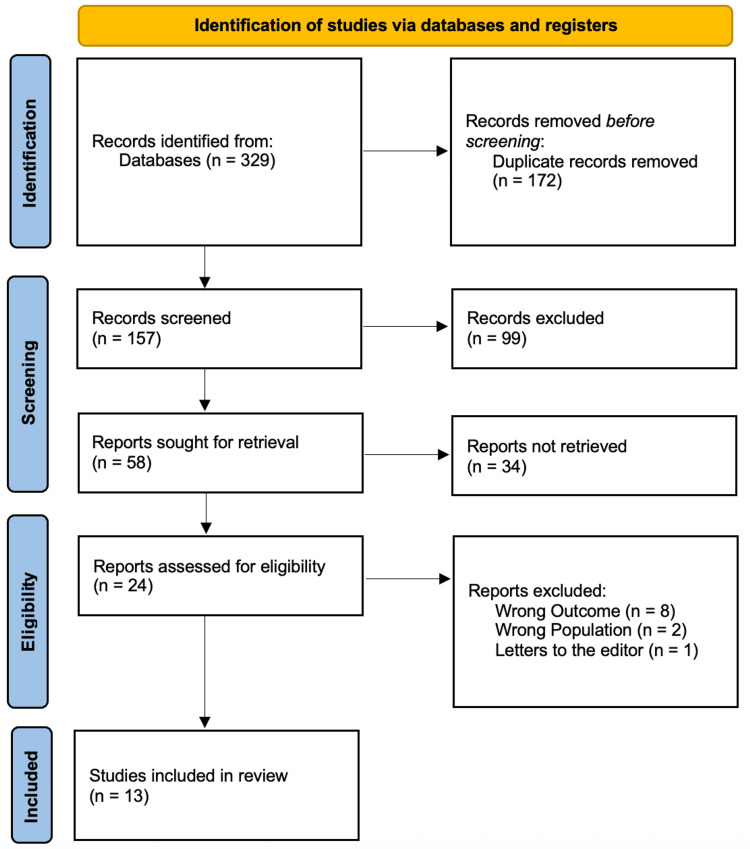 Figure 1
Figure 1| Study (Author, Year, Reference) | Country | Study Design | Sample Size | Population Characteristics | Age (Mean/%) | Gender (% Female) | Key Demographic Notes |
| Gammoh et al. (2025) [ | Jordan | Cross-sectional | 327 | Syrian refugees with HTN/T2DM | >50 years: 56.7% | 50.3% | War-displaced, high PTSD prevalence |
| Arigo et al. (2020) [ | USA | Observational | 184 | Adults with poorly controlled T2DM | NM | NM | No psychiatric history |
| Yu et al. (2024) [ | Multi-country | Mendelian randomization | NM | Genetic datasets (GWAS) | NM | NM | Focus on obesity mediation |
| Dixon et al. (2020) [ | USA | Cross-sectional | 290 | Low-income African-American women with T1D/T2D | NM | 100% | High trauma/PTSD rates |
| Hirai et al. (2022) [ | Japan | Longitudinal | NM | Fukushima disaster evacuees | NM | NM (men analyzed) | PTSD linked to incident T2D in men |
| Serhiyenko et al. (2025) [ | Ukraine | Cross-sectional | 64 (32 IDP) | T2DM patients vs. IDP with T2DM | NM | NM | Validated distress tool |
| Bergman et al. (2022) [ | Scotland | Retrospective cohort | 78,000 veterans | UK military veterans | NM | NM | PTSD-T2D comorbidity |
| Mykytyuk et al. (2024) [ | Ukraine | Cross-sectional | 91 (26 T1D, 65 T2D) | IDP/RTC in war zones | T1D: 34.7±8.79; T2D: 56.5±10.79 | NM | SF-36/HADS used |
| Venkatachalam et al. (2023) [ | Lebanon | Cross-sectional | NM | Syrian refugee women | 35–55 years | 100% (subset) | High inflammation/T2D |
| Popenko et al. (2022) [ | Ukraine | Case-control | 106 (61 ATO veterans) | Military personnel with T2DM | 30–70 years | 0% (male-only) | PTSD in 42.6% |
| Koval et al. (2023) [ | Ukraine | Cross-sectional | 56 | Civilians with HTN/T2DM in war zones | NM | NM | HADS/Spielberger scales |
| Serik et al. (2023) [ | Ukraine | Observational | 106 | Civilians with CHD/T2DM | NM | NM | PCL-5/GAD-7 used |
| Lica et al. (2021) [ | Romania | Cross-sectional | 54 (IDD adolescents) | Adolescents with IDD | 12–18 years | NM | APS-SF tool |
| Study (Author, Year, Reference) | PTSD Measure | T2D Measure | Key Findings | Mediators/Confounders |
| Gammoh et al. (2025) [ | Arabic PTSD scale | Self-reported HTN/T2DM | 69.8% had severe PTSD linked to medication lack/chronic pain | NM |
| Arigo et al. (2020) [ | Self-reported symptoms | HbA1c (9.13%) | PTSD symptoms associated with diabetes distress (R² ~3%) | Depression |
| Yu et al. (2024) [ | GWAS data | Genetic T2D risk | PTSD increased T2D risk (OR 1.036); mediated by obesity (9.51%) | Obesity, hypertension |
| Dixon et al. (2020) [ | PSS | HbA1c | PTSD associated with higher HbA1c (p=0.002) | Childhood trauma |
| Hirai et al. (2022) [ | K6/PCL-S | Incident T2D | PTSD/depression predicted T2D in men (HR sig.) | Disaster-related stress |
| Serhiyenko et al. (2025) [ | T2-DDAS | HbA1c | IDP had higher distress (hypoglycemia, healthcare access) | NM |
| Bergman et al. (2022) [ | Clinical records | T2D diagnosis | Veterans with PTSD had higher T2D (OR 1.29) | Mood disorders |
| Mykytyuk et al. (2024) [ | HADS/SF-36 | HbA1c/DBP | Warzone residents had worse mental health (p<0.05) | Anxiety/depression |
| Venkatachalam et al. (2023) [ | HTQ/HSCL-25 | Undiagnosed T2D | Women had higher PTSD/inflammation (SAA: p=0.036) | Obesity |
| Popenko et al. (2022) [ | Clinical PTSD | HbA1c (12.1 mmol/L) | ATO veterans had higher HbA1c vs. controls (7.63 mmol/L, p<0.05) | PTSD (42.6%) |
| Koval et al. (2023) [ | HADS/Spielberger | NM | 80% anxiety, 69% depression; women were more affected | HTN severity |
| Serik et al. (2023) [ | PCL-5/GAD-7 | HbA1c/lipids | CHD/T2DM patients had higher PTSD scores (p=0.037) | Visceral fat |
| Lica et al. (2021) [ | APS-SF | HbA1c (>7.6) | Girls with IDD had higher anxiety/PTSD (p<0.05) | Poor adherence |
| Study (Author, Year, Reference) | Risk of Bias Tool | Selection Bias | Comparability | Outcome/Exposure Measurement | Overall Risk |
| Gammoh et al. (2025) [ | NOS | Low (representative sample) | Moderate (adjusted for pain/medications) | High (self-reported PTSD) | Moderate |
| Arigo et al. (2020) [ | NOS | Low (defined T2D cohort) | High (no psychiatric history) | Low (validated scales) | Moderate |
| Yu et al. (2024) [ | STROBE-MR | Low (GWAS data) | Low (MR controls) | Low (robust sensitivity tests) | Low |
| Dixon et al. (2020) [ | NOS | Moderate (clinic-based) | Moderate (adjusted for trauma) | Low (PSS/BDI) | Moderate |
| Hirai et al. (2022) [ | NOS | Low (longitudinal) | Low (multivariate adjustment) | Low (K6/PCL-S) | Low |
| Serhiyenko et al. (2025) [ | NOS | Moderate (small sample) | NM | Moderate (T2-DDAS validation) | Moderate |
| Bergman et al. (2022) [ | NOS | Low (national registry) | Low (matched controls) | Low (clinical records) | Low |
| Mykytyuk et al. (2024) [ | NOS | Moderate (convenience sample) | NM | Moderate (SF-36/HADS) | Moderate |
| Venkatachalam et al. (2023) [ | NOS | Moderate (refugee subset) | Moderate (adjusted for sex/age) | Low (HTQ/HSCL-25) | Moderate |
| Popenko et al. (2022) [ | NOS | High (military bias) | Moderate (case-control) | High (self-reported PTSD) | High |
| Koval et al. (2023) [ | NOS | Moderate (warzone sample) | NM | Moderate (HADS/Spielberger) | Moderate |
| Serik et al. (2023) [ | NOS | Moderate (CHD/T2DM subset) | Low (adjusted for lipids) | Low (PCL-5/GAD-7) | Moderate |
| Lica et al. (2021) [ | NOS | Low (adolescent cohort) | NM | Moderate (APS-SF) | Moderate |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPosttraumatic Stress Disorder Research · Resilience and Mental Health · Traumatic Brain Injury Research
Introduction and background
Post-traumatic stress disorder (PTSD) and type 2 diabetes (T2D) represent two major public health challenges with a growing body of evidence suggesting a bidirectional relationship between them. PTSD, a debilitating psychiatric condition triggered by exposure to traumatic events, affects approximately 3.9% of the global population, with higher prevalence rates observed in conflict-affected regions and among military veterans [1]. Concurrently, T2D has reached epidemic proportions, affecting over 537 million adults worldwide, with projections indicating a continued rise due to aging populations and lifestyle factors [2]. Emerging research indicates that individuals with PTSD are at a significantly elevated risk of developing T2D, with meta-analyses reporting a 30%-50% increased incidence compared to non-PTSD populations [3]. This association persists even after adjusting for traditional risk factors such as obesity and physical inactivity, suggesting that PTSD may exert independent metabolic effects through neuroendocrine and inflammatory pathways [4]. The biological mechanisms linking PTSD to T2D are multifaceted and involve dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, chronic low-grade inflammation, and autonomic nervous system dysfunction. Prolonged stress exposure in PTSD leads to hypercortisolism, which promotes insulin resistance and visceral fat accumulation-key drivers of T2D pathogenesis [5]. Additionally, elevated levels of pro-inflammatory cytokines (e.g., interleukin-6 (IL-6), C-reactive protein (CRP)) observed in PTSD patients contribute to β-cell dysfunction and impaired glucose metabolism [6]. Behavioral factors, including poor sleep, sedentary lifestyle, and medication non-adherence, further exacerbate this relationship, creating a vicious cycle of worsening metabolic and mental health outcomes [7]. Despite these insights, critical gaps remain in understanding how sociodemographic variables (e.g., gender, displacement status) and comorbid conditions (e.g., hypertension) modulate PTSD-T2D interactions, particularly in understudied populations such as refugees and veterans. This systematic review aims to synthesize current evidence on the bidirectional relationship between PTSD and T2D.
Review
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [8]. A comprehensive search strategy was implemented across multiple electronic databases, including PubMed/Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica database (Embase), PsycINFO, and Web of Science over the years 2020-2025 to identify all relevant studies examining the bidirectional relationship between PTSD and T2D. The search incorporated controlled vocabulary terms (MeSH, Emtree) and free-text keywords related to PTSD, trauma-related disorders, and T2D, with search syntax adapted for each database following recommendations by Bramer et al. [9]. To minimize selection bias, two independent reviewers performed study screening, selection, data extraction, and quality assessment using standardized protocols. Discrepancies were resolved through consensus or consultation with a third reviewer when necessary. To ensure the non-redundant inclusion of data, studies originating from the same cohort or dataset were carefully examined. When overlaps were identified, the publication with the most comprehensive data or the longest follow-up period was selected for inclusion.
Eligibility Criteria
Studies were included if they (1) investigated either the risk of T2D development in PTSD populations or the risk of PTSD development in T2D populations; (2) included adult participants (≥18 years); (3) provided quantitative data on PTSD diagnosis (clinical or validated scales) and T2D outcomes (incidence, prevalence, or metabolic markers); and (4) were published in English. We excluded studies focusing exclusively on type 1 diabetes, gestational diabetes, or prediabetes; those without primary data (reviews, editorials); animal studies; and case reports with fewer than 10 participants. Both observational (cohort, case-control, and cross-sectional) and interventional studies were eligible.
Data Extraction
A piloted, standardized form was used to extract data on study design, sample characteristics (demographics, PTSD/T2D diagnostic criteria), key findings (effect sizes, adjusted odds ratios (ORs)/hazard ratios), and confounding variables. For studies reporting longitudinal outcomes, we extracted data on follow-up duration and attrition rates. Reference management software (EndNote X9, Clarivate, London, UK) and the Rayyan platform (Rayyan Systems Inc., Cambridge, MA) [10] were employed to streamline screening and eliminate duplicates. All included studies underwent full-text review, with data extraction performed independently by two researchers to ensure accuracy.
Data Synthesis Strategy
Given the heterogeneity in study designs and outcomes, a narrative synthesis was prioritized. Data were organized thematically to address (1) PTSD as a risk factor for T2D, (2) T2D as a risk factor for PTSD, and (3) mediating mechanisms (e.g., inflammation, HPA axis dysfunction). Summary tables were generated to compare effect sizes, adjustment for confounders, and population-specific findings. Where feasible, quantitative synthesis (e.g., meta-analysis of ORs) was performed for studies with comparable methodologies.
Risk of Bias Assessment
Study quality was evaluated using the Newcastle-Ottawa Scale (NOS) for observational studies [11] and the Cochrane Risk of Bias Tool for randomized trials [12]. The NOS assessed selection (representativeness, exposure/outcome ascertainment), comparability (control for confounders), and outcome/exposure assessment. For genetic studies (e.g., Mendelian randomization), we applied the Strengthening the Reporting of Observational Studies in Epidemiology using Mendelian Randomization (STROBE-MR) checklist [13]. Studies were categorized as low, moderate, or high risk based on predefined thresholds.
Results
Figure 1 presents a PRISMA flow diagram outlining the systematic study selection process. Initially, 329 records were identified through database searches, with 172 duplicates removed, leaving 157 records for screening. After title/abstract screening, 99 records were excluded, and 58 full-text articles were sought for retrieval. Of these, 34 could not be retrieved, leaving 24 reports assessed for eligibility. After full-text review, 11 reports were excluded (eight for wrong outcomes, two for wrong population, and one for being an abstract), resulting in 13 studies meeting all inclusion criteria for the final review.
PRISMA Flow Diagram of the Study Selection ProcessPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 1 summarizes demographic and study characteristics, providing a structured overview of research design, population, and sample attributes [14-26]. For instance, Gammoh et al. (2025) [14] conducted a cross-sectional study on Syrian refugees in Jordan, revealing that 69.8% of participants with hypertension or T2D exhibited severe PTSD symptoms. Similarly, Dixon et al. (2020) [17] focused on low-income African-American women with diabetes, finding that 30.4% met PTSD criteria, with trauma exposure significantly worsening glycemic control. Military and disaster-affected populations were also well-represented, such as in Hirai et al. (2022) [18], which linked PTSD to incident T2D in male Fukushima evacuees, and Bergman et al. (2022) [20], where Scottish veterans with PTSD had a 29% higher T2D risk than non-veterans.
Table 2 synthesizes key findings, emphasizing PTSD measurement tools, T2D outcomes, and mediating factors. Studies like Yu et al. (2024) [16] used Mendelian randomization to demonstrate that PTSD increases T2D risk (OR 1.036), with obesity mediating 9.51% of this effect. Clinical studies, such as Arigo et al. (2020) [15], highlighted that PTSD symptoms in adults with poorly controlled T2D were associated with elevated diabetes distress (R² ~3%), independent of depression. War-related studies, including Venkatachalam et al. (2023) [22] and Popenko et al. (2022) [23], identified higher PTSD prevalence in conflict zones, correlating with worse metabolic outcomes (e.g., HbA1c 12.1 mmol/L in Ukrainian veterans). Gender disparities were notable, with women refugees showing higher PTSD-related inflammation [22] and civilians in war zones exhibiting severe anxiety-depression comorbidity [24].
Table 3 shows that most studies demonstrated low-to-moderate risk, with Mendelian randomization [16] and registry-based designs [20] having the lowest bias due to robust methodologies. Cross-sectional studies [14, 19, 21-22] faced a moderate risk from self-reported outcomes or convenience sampling. Military studies [20, 23] had higher bias due to selection (e.g., veterans only) or unmeasured confounders (e.g., combat exposure severity). Tools like the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (PCL-5) [25] and Harvard Trauma Questionnaire (HTQ) [22] improved reliability in PTSD measurement, whereas self-reported glycated hemoglobin A1c (HbA1c) [14, 23] introduced variability. Overall, longitudinal designs [18] and genetic analyses [16] were most rigorous, while warzone studies [21, 24-25] struggled with uncontrolled environmental stressors.
Discussion
This review synthesizes evidence on the complex relationship between PTSD and T2D, corroborating and expanding upon existing literature that highlights a significant association between the two conditions. Our analysis underscores critical nuances involving risk factors, mediating mechanisms, and population-specific vulnerabilities.
The aggregated findings indicate a robust association between PTSD and an increased risk for T2D, with obesity and hypertension emerging as key mediating factors [16, 27]. For instance, genetic evidence from a Mendelian randomization study by Yu et al. (2024) supports a potential causal pathway, demonstrating that genetic liability to PTSD is associated with a higher risk of T2D, with obesity mediating a significant portion of this effect [16]. This aligns with longitudinal data, such as from the Nurses’ Health Study II, which reported a 1.5- to two-fold increased incidence of T2D in women with PTSD [28]. Beyond behavioral mediators, our review identified chronic stress and inflammation as exacerbating factors. This is consistent with research in veteran populations, where inflammatory markers like CRP and IL-6 have been shown to mediate the PTSD-T2D relationship [29].
The context of trauma and demographic factors appear to be pivotal modifiers of risk. Disparities are particularly evident by gender. While one study of disaster survivors found PTSD was predictive of T2D only in men [18], other research involving refugees and trauma-exposed civilians has documented a disproportionately high PTSD prevalence and worse glycemic control among women [17, 22]. This observation aligns with meta-analytic data suggesting women with PTSD may face a greater T2D risk than men, possibly due to sex-specific hormonal interactions [30, 31]. Military and conflict-affected populations also exhibit unique vulnerabilities. Studies consistently show that veterans with PTSD have a higher incidence of T2D compared to their civilian counterparts [20, 32]. Furthermore, research in war zones, such as studies on Ukrainian veterans and internally displaced persons (IDPs), highlights the compounding effects of chronic stress, with these groups displaying significantly higher diabetes distress and worse metabolic outcomes [19, 21, 23].
The pathophysiological pathways linking PTSD to T2D likely involve dysregulation of the HPA axis, leading to increased cortisol secretion and subsequent insulin resistance, as reflected in studies showing elevated fasting glucose in individuals with PTSD [17, 25, 33, 34]. Concurrently, PTSD-associated pro-inflammatory cytokines (e.g., tumor necrosis factor-alpha (TNF-α), IL-6) may further impair β-cell function [22, 29]. These biological mechanisms are often compounded by behavioral sequelae of PTSD, such as physical inactivity, poor diet, and medication non-adherence, which collectively worsen metabolic health [23, 26].
From a clinical perspective, these findings underscore the necessity for integrated screening and management strategies that address both PTSD and T2D, particularly in high-risk groups such as refugees, veterans, and survivors of chronic trauma. The validation of targeted tools, like the Ukrainian Type 2 Diabetes Distress Assessment System (T2-DDAS) for diabetes distress, demonstrates their utility in identifying at-risk individuals within specific populations [19]. Moreover, the evidence supporting the mediating role of obesity suggests that weight management and metabolic health interventions could be valuable components of a comprehensive treatment approach for individuals with PTSD [16].
Limitations
This review has several limitations that should be considered when interpreting the findings. First, the significant heterogeneity in how the key variables were measured poses a challenge for direct comparison across studies. PTSD was assessed using a range of tools, from clinical interviews and standardized scales like the PCL-5 to simpler self-report measures [14, 23]. Similarly, T2D was defined inconsistently, using criteria from HbA1c levels to International Classification of Diseases (ICD)-coded clinical diagnoses [17, 20]. Second, the overreliance on cross-sectional data, particularly in studies of conflict-affected populations [21, 24, 25], prevents the determination of temporal sequence and the establishment of causal inferences between PTSD and T2D. A further critical limitation is the imbalance in the evidence base. Many studies, especially those conducted in warzone settings, had small sample sizes (e.g., <100 participants), yet their findings are often reported with weights comparable to large-scale registry or genetic studies; this may inadvertently overstate preliminary or weak evidence. Additionally, the generalizability of the findings is constrained by demographic and geographic biases. For instance, the genetic evidence from Mendelian randomization studies is primarily based on European genome-wide association study (GWAS) data, limiting its applicability to diverse, non-European populations [16]. Furthermore, research focused on military and veteran cohorts [20, 23] often lacks adequate representation of female participants, which may obscure important sex-specific mechanisms and risk profiles.
Conclusions
PTSD elevates T2D risk through biological (inflammation, HPA dysfunction) and behavioral pathways, with heightened vulnerability in women, refugees, and veterans. Clinicians should prioritize trauma-informed diabetes care, including routine PTSD screening in T2D populations and vice versa. Future research must employ longitudinal designs in diverse cohorts to clarify causal mechanisms and evaluate targeted interventions (e.g., anti-inflammatory therapies, stress-reduction programs).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Posttraumatic stress disorder in the World Mental Health Surveys Psychol Med Koenen KC Ratanatharathorn A Ng L 226022744720172838516510.1017/S 0033291717000708 PMC 6034513 · doi ↗ · pubmed ↗
- 2IDF Diabetes Atlas, 10th Edition Brussels: International Diabetes Federation Magliano DJ Boyko EJ IDF Diabetes Atlas 10th edition scientificcommittee Brussels International Diabetes Federation 2021 https://www.ncbi.nlm.nih.gov/books/NBK 581934/
- 3Posttraumatic stress disorder and cardiovascular disease Prog Cardiovasc Dis Edmondson D Cohen BE 5485565520132362196410.1016/j.pcad.2013.03.004PMC 3639489 · doi ↗ · pubmed ↗
- 4Post-traumatic stress disorder symptoms and risk of hypertension over 22 years in a large cohort of younger and middle-aged women Psychol Med Sumner JA Kubzansky LD Roberts AL 310531164620162753480210.1017/S 0033291716001914 PMC 5093068 · doi ↗ · pubmed ↗
- 5Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress J Psychosom Res Tsigos C Chrousos GP 8658715320021237729510.1016/s 0022-3999(02)00429-4 · doi ↗ · pubmed ↗
- 6Association between traumatic brain injury and risk of posttraumatic stress disorder in active-duty Marines JAMA Psychiatry Yurgil KA Barkauskas DA Vasterling JJ 1491577120142433753010.1001/jamapsychiatry.2013.3080 · doi ↗ · pubmed ↗
- 7The short and long-term effects of aerobic, strength, or mixed exercise programs on schizophrenia symptomatology Sci Rep García-Garcés L Sánchez-López MI Cano SL 243001120213493411510.1038/s 41598-021-03761-3PMC 8692409 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 03722021 https://www.bmj.com/content/372/bmj.n 71.short 10.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗