Influence of Australasian Triage Scale on time to CT for major trauma patients: a Western Australian level 1 trauma centre experience
Kyle Raubenheimer, Jeni Thomas, Gabriel Plitzko, Joseph Trimboli, Pradeep Sanjamala, Dieter G. Weber

TL;DR
The study found that higher triage urgency scores are linked to faster CT scans for major trauma patients, with males and higher urgency categories receiving quicker care.
Contribution
This study demonstrates the impact of triage urgency on CT scan timing in trauma care and identifies gender disparities in treatment delays.
Findings
Higher ATS urgency categories are associated with shorter time to CT scans for trauma patients.
Male patients received CT scans 27 minutes faster than female patients.
Time to CT was not associated with in-hospital mortality in this cohort.
Abstract
This study investigated whether higher triage urgency according to the Australasian Triage Scale (ATS) is associated with reduced time to computed tomography (CT) in major trauma patients. A retrospective analysis was conducted on 621 patients with major trauma (ISS > 12) admitted to the state adult major trauma centre in Western Australia between September 2021 and August 2022. Demographic, injury, and clinical data were extracted from the state trauma registry. Time to CT was analysed using multivariate regression to assess the influence of ATS category and other clinical variables. Median age was 50 years (range 14–103), and 75% were male. Nearly half of patients were triaged as ATS category 1. Higher urgency ATS category was independently associated with shorter time to CT: compared with ATS category 1, time to CT was delayed by 39 min in ATS 2 and 91 min in ATS 3 patients (p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
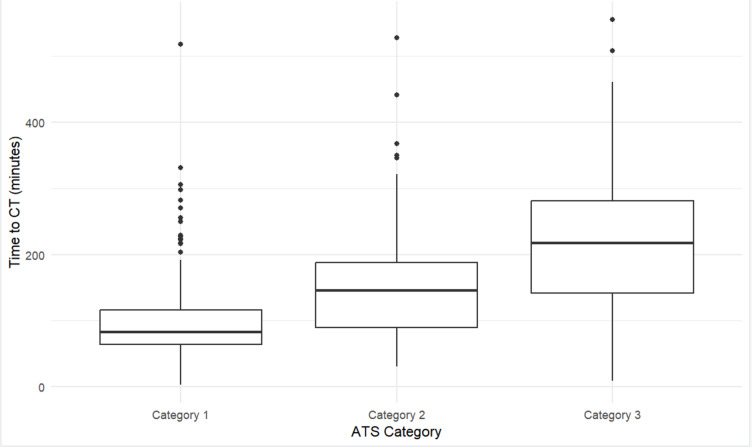 Figure 1
Figure 1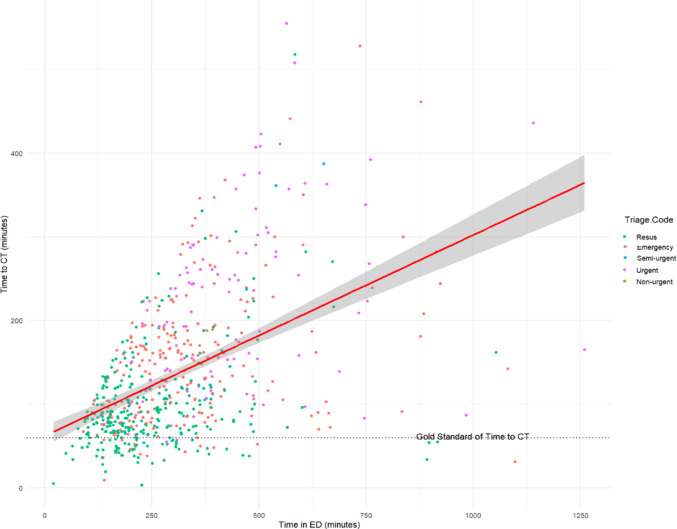 Figure 2
Figure 2- —East Metropolitan Health Service
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma and Emergency Care Studies · Abdominal Trauma and Injuries · Radiology practices and education
Introduction
Computed tomography (CT) is a critical imaging modality in modern trauma care. Expedited CT in major trauma is associated with reductions in time to diagnosis, time in the emergency department (ED), and laparotomies, as well as improvements in other metrics associated with good clinical care [1–4]. ED length of stay has been shown to be an independent predictor of mortality for trauma patients [5].
In Australia, patients presenting to the ED are triaged according to the Australasian Triage Scale (ATS) [6]. The ATS is a 5-level clinical tool predicated on a brief history and clinical assessment typically performed by trained triage nurses used to establish maximum waiting time for patients (Table 1) [6]. The ATS is applied prospectively with the aim to facilitate timely emergency care [6]. Since major trauma has been shown to impact staff workload within the ED, appropriate triaging facilitates effective management of major trauma patients, and contributes to the overall quality of care through the appropriate allocation of resources [7].
Table 1. The Australasian triage scale (ATS) [6]ATS CategoryLevel of UrgencyTime to Treatment GoalClinical Examples1 - ImmediateLife-threateningImmediate (0 min)Cardiac arrest, severe trauma, unconscious patient, massive bleeding2 - EmergencyImminent risk of deteriorationWithin 10 minSevere respiratory distress, major burns, suspected stroke, acute chest pain (possible MI)3 - UrgentPotentially seriousWithin 30 minModerate asthma, significant head injury, moderate bleeding, severe abdominal pain4 - Semi-UrgentLess serious, but requires attentionWithin 60 minMild asthma, minor fractures, stable but painful injuries5 - Non-UrgentLeast serious, can waitWithin 120 minMild cold/flu symptoms, chronic issues without acute distress, minor wounds
The Royal Australasian College of Surgeons trauma verification criteria recommends data collection on time to CT as a quality indicator for Australasian trauma systems [8, 9]. International guidelines recommend the time to CT from arrival to ED to be less than 1 h for severely injured patients [10, 11], while others have suggested more aggressive time protocols [12–14]. Previous studies in Australia have demonstrated a time to CT of between 43 min and 76 min [15, 16]. However, the potential influence of the triage category may impact the urgency in which patients in the ED receive their CT scans.
While it is intuitive that patients with higher triage priority receive expedited CT imaging, quantifying this relationship is crucial for evaluating the efficiency of trauma care delivery. Delays in CT imaging can result in prolonged diagnostic uncertainty, delayed interventions, and worse clinical outcomes in critically ill trauma patients [4, 17]. Additionally, examining the time to CT across different ATS categories can provide insights into whether triage-based prioritization aligns with actual patient needs and clinical outcomes, or whether systemic inefficiencies exist that disproportionately affect specific patient subgroups [18]. For instance, prior studies have demonstrated that workflow inefficiencies, resource limitations, and interdepartmental communication barriers can contribute to unexpected delays in imaging, even for high-acuity patients [19].
The primary aim of this study was to quantify the time to CT for major trauma patients at the state adult major trauma centre in WA over a 1-year period and to investigate the effect of ATS triage category on time to CT. Understanding this relationship is critical, as adherence to time-to-CT benchmarks has been linked to improved trauma outcomes, including reduced morbidity and mortality [20, 21]. Furthermore, this study seeks to determine the effect of time to CT on time in ED, the relationship between time to CT and mortality, and to determine other variables associated with time to CT in Western Australia.
Methods
Study population
All patients with major trauma, defined as Injury Severity Score (ISS) > 12, who were admitted to Royal Perth Hospital and recorded in the Western Australian State Trauma Registry between 01 September 2021 and 31 August 2022 were analysed. Inclusion in the registry requires definitive treatment within 7 days of trauma, hospital admission longer than 24 h, or trauma-related death. Interhospital transfers were included in the study, provided that CT scans were performed at Royal Perth Hospital.
Setting
Royal Perth Hospital is the designated adult major trauma centre for the State of Western Australia and accepts all major trauma patients within the State, over the age of 14 years. All adult major traumas within the State of Western Australia are channelled through the regional trauma network to Royal Perth Hospital for definitive care. Royal Perth Hospital employs a ‘trauma call’ system, where prehospital criteria such as mechanism of injury, physiology, and physician discretion determine ATS category designation. Computed tomography (CT) imaging is available at all times, with an in-house radiologist present 24 h a day, 7 days a week. Requesting of CT scans is performed either in person or by telephone consultation with the on-duty radiologist.
For the purpose of this study, ‘metropolitan area’ refers to the Perth Metropolitan Region as defined by the Western Australian Metropolitan Region Scheme (MRS), which covers approximately 6,400 km² and extends around 90 km north to south and 40 km inland from the coast.
Data collection
Data for this study were obtained from the Western Australian State Trauma Registry. Variables extracted included time to CT, ATS category, time of patient triage, time first seen by a member of the medical team, and time of first recorded CT image. In addition, patient demographics (age and sex), mechanism of injury, injury severity score (ISS), and hospital admission details (including time in ED, ED disposition destination, hospital length of stay [LOS], and final discharge destination), as well as in-hospital mortality, were collected from the registry.
Time to CT was defined as time from emergency department triage to time of first images recorded on the hospital imaging system (IMPAX, Agfa-Gevaert Group, Mortsel, Belgium). For time of first image recorded, time of first scouting image is recorded as an automated process. Where a first scouting image is not loaded onto the hospital imaging system, the manually recorded time on the first image on the hospital system was recorded.
Study approval
Approval from the hospital Clinical Safety and Quality Unit was obtained prior to commencement of this study (GEKO Approval #49617). Study was conducted according to the STROBE guidelines [22].
Statistical analysis
Initial exploratory data analysis was performed and outliers were removed from the dataset. A threshold of 8 standard deviations was used to remove outliers (11 outliers were removed from the 632 original study patients).
QQ-plots and Kolmogorov-Smirnov test was utilized to assess the normal distribution of the data. Normally distributed data were compared using a two-tailed unpaired t-test, whereas non-normally distributed and ordinal-scaled data were compared using the Mann-Whitney U test. Differences between nominal data were analyzed with the χ² (chi-squared) test. If the event count was below five, Fisher’s exact test was applied.
For time to CT and mortality, univariate regression was used to identify significant variables to include in separate multivariate regression models. Hospital length of stay, ED disposition, and outcome were included in exploratory analyses but were not primary predictors of time to CT, as they occur post-imaging. Statistical significance was set at p < 0.05. Statistical analyses and data visualisations were completed using R Statistical Package (R Foundation for Statistical Computing, Vienna, Austria) [23].
Results
Demographics
Between 01 September 2021 and 31 August 2022, 621 major trauma patients underwent CT imaging. The median age was 50 years (range 14–103), and most patients were male (n = 464, 75%). The most common mechanisms of injury were falls (n = 188, 30%), motor vehicle crashes (n = 144, 23%), motorbike crashes (n = 96, 15%), being struck by objects (n = 45, 7%), and pedal cyclist incidents (n = 34, 5%). A total of 457 patients (74%) sustained their injuries in the metropolitan area. Nearly half of the cohort were triaged as ATS category 1 (n = 302, 49%). Between ATS categories, there were statistical differences in biological sex, rurality, time to CT, time in ED, ED disposition, and final discharge destination. Patients with higher urgency ATS category had a greater proportion from metropolitan areas, were more often admitted to the ICU, and were less frequently discharged directly home. Overall, the most common discharge destination was home (n = 361, 58%), followed by rehabilitation facilities (n = 100, 16%). The median Injury Severity Score (ISS) was 19 and the median hospital length of stay (LOS) was 9 days (Table 2).
Table 2. Descriptive statistics of the study populationVariableCategory/MeasurementTotalATS 1ATS 2ATS 3ATS 4/5p value^†^n = 621n = 302n = 210n = 104n = 5SexMale464 (75%)226 (75%)165 (79%)70 (67%)3 (60%)< 0.001Female157 (25%)76 (25%)45 (21%)34 (33%)2 (40%)AgeMedian, years (IQR)50 (32–67)46 (29–61)51 (35–67)63 (44–77)73 (71–86)0.064Range14–10314–9515–9915–10371–87RuralityMetropolitan457 (74%)209 (69%)155 (74%)88 (85%)5 (100%)< 0.001Rural/Remote164 (26%)93 (31%)55 (26%)16 (15%)0 (0%)Clinical VariablesGCS, median score (IQR)15 (14–15)15 (13–15)15 (14–15)15 (15–15)15 (15–15)0.42HR, median BePM (IQR)85 (73–100)89 (74–105)84 (74–98)77 (66–92)72 (64–76)0.817SBP, median mmHg (IQR)130 (117–148)123 (106–140)136 (125–151)138 (124–153)144 (109–147)0.667ISSMedian, score (IQR)19 (16–26)24 (17–30)17 (14–24)17 (14–21)16 (14–17)0.998Range13–7513–7513–7513–4314–22Time to CTMedian, minutes (IQR)108 (75–174)83 (64–116)146 (90–188)218 (142–281)237 (148–361)0.002Range3–5553–51831–5289–555118–368Time in EDMedian, minutes (IQR)282 (192–386)209 (158–306)312 (228–398)394 (308–504)505 (437–568)0.03Range105–157821–105391–1098140–1260333–651ED DispositionOperating Theatres46 (7%)34 (11%)11 (5%)1 (< 1%)0< 0.001ICU103 (17%)90 (30%)13 (6%)00SMTU High Acuity111 (18%)67 (22%)33 (16%)10 (10%)1 (20%)SMTU Low Acuity260 (42%)98 (32%)107 (51%)54 (52%)1 (20%)Other Wards101 (16%)13 (5%)46 (22%)39 (38%)3 (60%)Discharge DestinationHome361 (58%)151 (50%)136 (65%)71 (68%)3 (60%)< 0.001Rehabilitation Facility100 (16%)77 (25%)21 (10%)2 (2%)0Hospital Transfer60 (10%)21 (7%)24 (11%)15 (14%)0Death48 (8%)27 (9%)13 (6%)8 (8%)0Discharge at own risk23 (4%)14 (5%)8 (4%)1 (1%)0Residential Care Facility11 (2%)2 (< 1%)1 (< 1%)6 (6%)2 (40%)Other18 (3%)10 (3%)7 (4%)1 (1%)0LOSMedian, days (IQR)9 (4–18)12 (6–25)7 (3–14)4 (3–9)7 (5–9)0.995Range0–1450–1450–1301–431–15^†**^ Statistical analysis only conducted for ATS categories 1–3 due to low numbers in ATS categories 4–5ATS* Australasian Triage Scale, IQR Interquartile Range, GCS Glasgow Coma Scale, HR Heart Rate, BeBPM Beats Per Minute, SBP Systolic Blood Pressure, DBP Diastolic Blood Pressure, RR Respiratory Rate, BrBPM Breaths Per Minute, *ISS * Injury Severity Score, ED Emergency Department, LOS Length of Stay
Influence of triage category on time to CT
Comparisons of the demographics between different triage categories are described in Table 2. Higher urgency ATS category was associated with a faster time to CT (Fig. 1). Using ATS category 1 as a reference point, patients who were triaged as ATS category 2 received a CT scan 39 min later, whilst patients triaged as ATS category 3 received CT scans 91 min later. Due to low numbers, patients in ATS category 4 and 5 were not included in the analysis. Notably, inclusion of outliers did not change statistical significance of main analysis.
Fig. 1. Boxplots of Time to CT by Australasian Triage Category
Time to CT and time in ED
Increases in time to CT were associated with increased time in ED (Fig. 2). In both the univariate and multivariate modelling, time to CT was correlated with time in ED (Tables 3 and 4). Multivariate regression analysis determined that for every 1-minute increase in time in ED, there is an increased time to CT of 9 s (Table 4). The intercept for the multivariate model was 51 min for time to CT.
Fig. 2. Scatterplot of Time to CT vs. Time in ED by Australasian Triage Category Score
Table 3. Univariate analysis of variables associated with time to CTVariableβ_1_Adjusted R^2^ Valuep valueISS−1.9810.046< 0.001Age0.6350.021< 0.001Gender (ref: Female)0.019< 0.001*** Male−28.672< 0.001TBI Category (ref: Mild)0.044< 0.001 Moderate−25.9660.073 Severe−70.075< 0.001Arrival Temperature−0.133−0.0020.801Arrival HR−0.3280.0040.058Arrival SBP0.5130.023< 0.001Arrival DBP0.3060.0010.174Arrival RR−1.1690.0030.116Rurality (ref: Country)0.0020.12 Metropolitan12.4240.12ATS Category (ref: Category 1)0.277< 0.001*** Category 2 55.079< 0.001*** Category 3 126.917< 0.001Mechanism125.4290.0150.073Time in ED0.2350.221< 0.001ED Disposition (ref: SMTU Low Acuity)0.093< 0.001*** ICU −67.001< 0.001*** Operating Theatres −52.983< 0.001*** SMTU High Acuity −36.574< 0.001*** Other Wards 5.8080.556Length of Stay−0.7790.02< 0.001Outcome (ref: Death)0.06< 0.001 Home 34.8930.008** Hospital Transfer 51.0920.002** Non-Hospital Transfer −14.2320.681 Own Risk 8.6250.691 Rehabilitation Facility −10.2150.497 Residential Care Facility 68.4030.027* Other −1.4860.962*ISS * Injury Severity Score, TBI Traumatic Brain Injury, HR Heart Rate, SBP Systolic Blood Pressure, DBP Diastolic Blood Pressure, RR Respiratory Rate, ATS Australasian Triage Scale, ED Emergency Department, SMTU State Major Trauma Unit, ICU Intensive Care Unit
Table 4. Multivariate regression model of variables associated with time to CTVariableEstimateStandard Errorp valueISS−0.109−0.2810.778Age0.1000.5750.565Gender (ref: Female) Male −26.998 −3.885 < 0.001TBI Category (ref: Mild) Severe −16.799 −1.114 0.266Arrival SBP0.1881.5290.127ATS Category (ref: Category 1) Category 2 39.080 5.325 < 0.001 Category 3 91.238 9.281 < 0.001Time in ED0.1558.312< 0.001ED Disposition (ref: SMTU Low Acuity) ICU −4.972 −0.383 0.702 Operating Theatres −8.670 −0.692 0.489 SMTU High Acuity −11.971 −1.403 0.161Length of Stay0.2420.9870.324Outcome (ref: Death) Home 9.94 0.671 0.502 Hospital Transfer 11.081 0.66 0.51 Residential Care Facility 0.991 0.035 0.972*ISS * Injury Severity Score, TBI Traumatic Brain Injury, SBP Systolic Blood Pressure, ATS Australasian Triage Scale, ED Emergency Department, SMTU State Major Trauma Unit
Time to CT and mortality
Multivariate analysis did not show any significant difference in time to CT on mortality (p = 0.410). When time to CT was included in a multivariate model, factors associated with mortality included ISS (p < 0.001), age (p < 0.001), moderate or severe TBI (p < 0.001), systolic blood pressure (p = 0.014), diastolic blood pressure (p = 0.025), ATS category 3 (p = 0.014), length of stay (p = 0.014), and ED disposition to the ICU (p = 0.022).
Variables associated with time to CT
Univariate modelling determined that ISS, age, sex, severe TBI, arrival SBP, ATS category, time in ED, length of stay, ED disposition, and outcome were statistically significant variables associated with time to CT (Table 3). Statistically significant variables of the univariate analysis were used for the multivariate model. Statistically significant variables associated with reductions in time to CT included male gender (p < 0.001), moderate TBI (p = 0.032), and ED disposition to other wards (p = 0.003). Variables that reached statistical significance and were associated with increased time to CT included ATS categories 2 and 3 (p < 0.001) and time in ED (p < 0.001) (Table 4).
Discussion
This series demonstrates a clear association between a higher urgency ATS triage category with a reduction in the time to CT. To our knowledge, this is the first time the relationship between time to CT and triage category has been defined. Other notable observations include a description of the demographics of WA major trauma patients receiving CT scans, lack of evidence on an effect of time to CT and mortality, and the variables associated with time to CT at our centre.
The result of reduced time in ED associated with reductions in time to CT is in keeping with the current literature. Time to CT has been shown to reduce time in ED within New Zealand, and elsewhere [24, 25]. Since CT scanning provides the basis for many diagnoses, expedited CT scanning leads to faster time to diagnosis and thus expedited disposition from the ED [17]. Whilst studies have investigated the time to the CT itself, fewer studies have commented on the time to CT report – a crucial step that many non-radiological clinicians rely on prior to deciding on an appropriate disposition for non-critical injuries. In-house emergency radiologists have been shown to reduce report turnaround significantly [25]. Future studies may consider incorporating the temporal variable of report turnaround time to gain a better understanding of factors related to time to CT, time in ED and clinical outcomes.
The present study did not find a statistically significant effect of time to CT on mortality for major trauma patients. This observation is in keeping with the Australian literature and the only multicentre, randomised controlled trial for time to CT [15, 16]. However, recent studies have postulated that faster time to CT may be associated with reductions in mortality, with times less than 30 min shown to have reduced mortality [13, 17, 26]. Furthermore, certain injuries are more likely to benefit from an expedited time to CT than others [26], suggesting patient selection and optimisation of in-hospital trauma systems may be important. Time to CT of less than 26 min was associated with lower mortality in blunt traumatic injury, whilst reduced time to angioembolization (which typically proceeds following a positive CT at our centre), has been shown to reduce mortality in pelvic trauma patients [26, 27]. In contrast, despite time to craniectomy having been shown to improve mortality in a military cohort, time to CT head does not seem to influence mortality in TBI [22, 24, 28, 29]. The absence of an observed effect of time to CT on mortality in this study is likely explained by sample size, cohort heterogeneity, and the overall low mortality rate in the WA trauma system. Moreover, our analysis included all CT scans across major trauma presentations, whereas certain subgroups (e.g. blunt aortic injury or pelvic trauma) may derive greater benefit from expedited imaging [26]. Organisational and infrastructural factors of trauma centres may also influence time to CT [29]. Future studies should stratify patients by specific injury patterns to better determine which cohorts benefit most from reduced imaging delays.
Several variables were associated with time to CT when in the multivariate regression modelling. Male gender, moderate TBI and disposition from the ED to inpatient wards other than the State Major Trauma Unit ward resulted in reduced time to CT. The negative association with admission to the State Major Trauma Unit ward is likely a marker of sicker patients, with a higher multi-system involvement of their traumatic injuries. Conversely, longer time in the ED and lower urgency ATS category were associated with longer times to CT. The biological sex discrepancy may be partially explained by delays in obtaining pregnancy test results prior to CT scans for potentially pregnant patients. However, this alone may not fully account for the discrepancy, as major trauma activations typically prioritize urgent imaging when clinically indicated. Other factors, such as differences in injury patterns, triage decisions, or implicit biases in clinical workflows, may warrant further investigation. Moderate, but not severe TBI, was associated with decreased time to CT as compared to mild TBIs. This may be the result of the interventions required for severe TBI, particularly as a GCS less than 8 typically warrants intubation. Time to sedation for patients following RSI has been shown to be between 12 and 55 min, which may account for the lack of statistical significance in the multivariate regression model for severe TBIs [30]. The decision for expeditious imaging in unwell patients should be balanced against the time requirement for interventions. In patients with a high degree of suspicion of severe TBI, expeditious imaging may facilitate timely transfer to the operating theatre for urgent cranial decompression. If the intervention is not lifesaving, it may be prudent to obtain imaging to facilitate faster diagnosis and subsequent interventions that may improve outcomes. ED disposition to other wards may indicate the opposite, as less complex traumatic injuries may not require as comprehensive scanning strategies, resulting in faster CT scans and subsequent dispositions to specialty wards.
We acknowledge several limitations in this study. This retrospective case-series was performed at a single centre. Whilst data for the trauma registry is collected prospectively, the research question is retrospective and prone to bias associated biases and methodological limitations. As data was only collected from a single centre, external validity of the study to other centres with other environments, hospital policies and procedures. We acknowledge that certain variables have low sample sizes, potentially resulting in exaggerated statistical significance without concurrent clinical significance. Finally, we note that trauma team activations (TTAs), time-to-provider, and ATS category are not independent variables but overlapping components of the same urgency framework. At Royal Perth Hospital, a two-tiered TTA system operates in parallel with ATS assignment, with higher urgency ATS categories frequently triggering a Tier 1 activation. Similarly, the time from arrival to first medical assessment is directly determined by ATS thresholds. For this reason, ATS was selected as the primary measure in our analysis, as it is a standardised, externally validated triage system applied universally across emergency presentations, whereas TTA criteria and time-to-provider are centre-specific and inherently coupled to ATS urgency. While this overlap limits the ability to isolate the independent contribution of TTA or time-to-provider, our approach ensures comparability and generalisability of findings to other trauma systems that also apply ATS or similar validated triage scales.
Conclusion
Higher urgency ATS triage category is associated with shorter time to CT for major trauma patients. Shorter time to CT was also associated with reduced time spent in the emergency department. Female patients experienced longer delays to CT compared with male patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Royal Australasian College of Surgeons. Australian and Aotearoa New Zealand Trauma Verification Program: Model Resource Criteria For Trauma Services [Internet]. 2022 Apr. Report No.: 2.0. Available from: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/trauma-verification/model-resource-criteria.pdf?rev=71ad 3d 4faf 9049 dcb 542a 38a 18dd 2e 7e&hash=6757 B 62EFA 5715 EC 752B 85E 35EC 3FB 45
- 2Recommendations | Head injury: assessment and early management | Guidance | NICE [Internet]. NICE. 2023 [cited 2023 Nov 5]. Available from: https://www.nice.org.uk/guidance/ng 232/chapter/recommendations