Comparison between 75-g and 100-g oral glucose tolerance tests using international association of diabetes and pregnancy study group one-step diagnostic threshold to detect gestational diabetes mellitus
Li-Li Zhou, Dong Liu, Hong-Qing Song, Yuan-Bo Wu, Wei-Bing Hu, Jian-Feng Wang, Jin-Sheng Wang, Chun-Yan Qi, Sa-Sa Liu

TL;DR
This study compares 75g and 100g glucose tests for gestational diabetes and finds no significant difference in diagnostic outcomes.
Contribution
The study provides evidence that both 75g and 100g OGTTs are equally effective under IADPSG criteria for detecting gestational diabetes.
Findings
The 100g OGTT resulted in higher blood glucose levels at 1h and 2h compared to the 75g OGTT.
No significant differences in GDM detection rates or adverse outcomes were found between the two OGTT groups.
Both OGTT groups showed similar trends in the association between glucose levels and adverse outcomes.
Abstract
The oral glucose tolerance test (OGTT) is the primary screening method for gestational diabetes mellitus (GDM), but global implementation criteria remain inconsistent. This retrospective study analyzed data from 3,907 pregnant women at Tongchuan People’s Hospital, including 1,925 in the 75g OGTT group (430 with GDM) and 1,982 in the 100g OGTT group (460 with GDM). A systematic comparison was conducted between the two groups regarding: blood glucose levels at each time point (0h, 1h, 2h);diagnostic rates, positive composition ratios of gestational diabetes mellitus, and risks of adverse maternal and neonatal outcomes based on the International Association of Diabetes and Pregnancy Study Groups (IADPSG) diagnostic criteria; Correlation analysis of blood glucose levels across time points; A glucose-level-adjusted continuous analysis to evaluate the dose-response relationship between…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
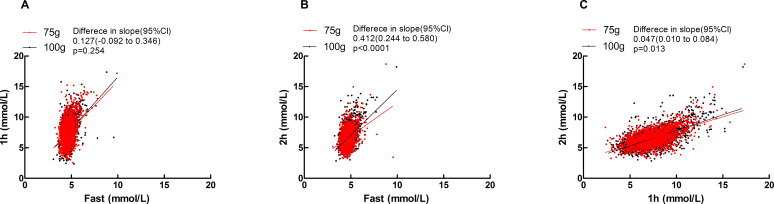 Figure 1
Figure 1| Characteristics | 75-g OGTT, mean ± SD (n = 1,925) | 100-g OGTT, mean ± SD (n = 1,982) | T/(χ2) |
|
|---|---|---|---|---|
| Maternal age (years) | 29.69 ± 4.02 | 29.55 ± 3.98 | −1.141 | 0.254 |
| Pregnancy duration at GDM screening (weeks) | 26.02 ± 1.30 | 26.03 ± 1.34 | 0.246 | 0.806 |
| BMI at GDM screening (kg/m2) | 23.37 ± 2.79 | 23.38 ± 2.81 | 0.124 | 0.902 |
| Pregnancy duration of delivery (weeks) | 39.07 ± 1.76 | 39.10 ± 2.02 | 0.525 | 0.599 |
| BMI at the time of delivery (kg/m2) | 29.20 ± 2.63 | 29.32 ± 2.56 | 1.496 | 0.135 |
| Incidence of other abnormalities* [% (n/n)] | 1.87 (36/1,925) | 2.12 (42/1,982) | 0.309 | 0.648 |
| Time point | 75-g OGTT, serum glucose mean ± SD, mmol/L (n = 1,925) | 100-g OGTT, serum glucose mean ± SD, mmol/L (n = 1,982) |
|
|
|---|---|---|---|---|
| Fasting | 4.68 ± 0.49 | 4.69 ± 0.48 | 0.811 | 0.417 |
| 1 h | 7.52 ± 1.90 | 7.72 ± 1.84 | 3.214 | 0.001 |
| 2 h | 6.58 ± 1.50 | 6.75 ± 1.38 | 3.661 | 0.000 |
| Positive modes (mmol/L) | 75-g OGTT (%) (n = 430) | 100-g OGTT (%) (n = 460) |
|
|
|---|---|---|---|---|
| Only fasting ≥5.1 | 42.33 (182/430) | 37.17 (171/460) | 2.465 | 0.131 |
| Only 1 h ≥10.0 | 11.63 (50/430) | 12.39 (57/460) | 0.122 | 0.758 |
| Only 2 h ≥ 8.5 | 11.16 (48/430) | 12.83 (59/460) | 0.581 | 0.471 |
| Fasting ≥ 5.1 and 1 h ≥ 10.0 | 7.21 (31/430) | 8.70 (40/460) | 0.669 | 0.458 |
| Fasting ≥ 5.1 and 2 h ≥ 8.5 | 5.35 (23/430) | 3.70 (17/460) | 1.415 | 0.259 |
| 1 h ≥ 10.0 and 2 h ≥ 8.5 | 8.14 (35/430) | 11.52 (53/460) | 2.853 | 0.093 |
| Fasting ≥ 5.1, 1 h ≥ 10.0, and 2 h ≥ 8.5 | 14.19 (61/430) | 13.70 (63/460) | 0.045 | 0.847 |
| Total positive rate of GDM | 22.34 (430/1,925) | 23.21 (460/1,982) | 0.421 | 0.517 |
| Maternal outcomes | Unadjusted | Adjusted※ | ||
|---|---|---|---|---|
| OR (95% CI) |
| aOR (95% CI) |
| |
| Abnormal fetal membranes | 0.97 (0.68–1.40) | 0.885 | 0.96 (0.67–1.40) | 0.884 |
| Abnormal stage of labor | 0.93 (0.30–2.92) | 0.906 | 0.97 (0.24–3.12) | 0.901 |
| Abnormal umbilical cord | 0.97 (0.73–1.29) | 0.828 | 0.98 (0.69–1.30) | 0.830 |
| Amniotic fluid volume abnormality | 1.11 (0.69–1.79) | 0.670 | 1.10 (0.41–1.79) | 0.528 |
| Cesarean section | 0.86 (0.66–1.12) | 0.260 | 0.89 (0.75–1.19) | 0.301 |
| Cholestatic syndrome | 1.25 (0.52–3.00) | 0.613 | 1.28 (0.48–3.01) | 0.608 |
| Dystocia | 1.24 (0.64–2.41) | 0.529 | 1.27 (0.79–2.45) | 0.595 |
| Hypoproteinemia | 1.25 (0.52–3.00) | 0.613 | 1.29 (0.68–3.02) | 0.686 |
| Perineal laceration | 1.04 (0.76–1.42) | 0.803 | 1.09 (0.69–1.48) | 0.801 |
| Pregnancy-induced hypertension | 0.96 (0.57–1.62) | 0.889 | 1.01 (0.84–1.19) | 0.885 |
| Placental abnormalities | 1.28 (0.58–2.83) | 0.535 | 1.34 (0.85–1.89) | 0.517 |
| Poor postpartum uterine rejuvenation | 1.08 (0.58–1.99) | 0.808 | 1.05 (0.62–1.94) | 0.843 |
| Postpartum hemorrhage | 1.69 (0.74–3.86) | 0.216 | 1.79 (0.91–2.95) | 0.249 |
| Postpartum infection | 1.25 (0.52–3.00) | 0.613 | 1.27 (0.48–3.01) | 0.608 |
| Other# | 1.11 (0.49–2.50) | 0.805 | 1.19 (0.71–2.57) | 0.884 |
| Neonatal outcomes | Unadjusted | Adjusted※ | ||
|---|---|---|---|---|
| OR (95% CI) |
| aOR (95% CI) |
| |
| Abnormal fetal position | 1.10 (0.80–1.51) | 0.560 | 1.11 (0.82–1.71) | 0.561 |
| Fetal distress | 1.50 (0.49–4.64) | 0.477 | 1.59 (0.21–4.75) | 0.479 |
| Fetal growth restriction | 1.28 (0.58–2.83) | 0.535 | 1.27 (0.55–2.20) | 0.553 |
| Low birth weight | 1.07 (0.39–2.98) | 0.898 | 1.05 (0.32–2.67) | 0.891 |
| Large for gestational age | 0.93 (0.39–2.27) | 0.879 | 1.00 (0.31–2.29) | 0.892 |
| Low Apgar score | 1.70 (0.56–5.10) | 0.347 | 1.81 (0.67–5.55) | 0.374 |
| Macrosomia | 1.17 (0.71–1.92) | 0.547 | 1.21 (0.74–1.93) | 0.585 |
| Neonatal cranial hematoma | 1.15 (0.68–1.92) | 0.607 | 1.14 (0.63–1.29) | 0.603 |
| Neonatal asphyxia | 1.31 (0.41–4.17) | 0.644 | 1.32 (0.84–4.21) | 0.669 |
| Neonatal hyperbilirubinemia | 0.99 (0.72–1.36) | 0.957 | 0.91 (0.65–1.01) | 0.929 |
| Neonatal hypoglycemia | 1.22 (0.53–2.82) | 0.639 | 1.29 (0.17–2.90) | 0.801 |
| Neonatal infection | 1.02 (0.73–1.43) | 0.906 | 1.05 (0.76–1.55) | 0.959 |
| Neonatal respiratory distress syndrome | 1.25 (0.43–3.64) | 0.681 | 1.16 (0.06–3.24) | 0.620 |
| Preterm delivery | 1.38 (0.81–2.33) | 0.237 | 1.41 (0.45–2.39) | 0.298 |
| Small for gestational age | 1.41 (0.39–5.02) | 0.598 | 1.61 (0.36–5.25) | 0.601 |
| Stillbirth | 1.17 (0.31–4.39) | 0.816 | 1.19 (0.35–4.41) | 0.857 |
| Outcomes | Variable | aOR (95% CI) |
|
|---|---|---|---|
| Cesarean section | groups | 0.92 (0.81-1.05) | 0.210 |
| fasting | 1.28 (1.08-1.50) | 0.003 | |
| 1hr | 1.05 (1.00-1.10) | 0.032 | |
| 2hr | 1.01 (0.96-1.08) | 0.649 | |
| Abnormal fetal membranes | groups | 1.03 (0.87-1.23) | 0.729 |
| fasting | 1.01 (0.82-1.26) | 0.904 | |
| 1hr | 0.96 (0.90-1.02) | 0.206 | |
| 2hr | 1.08 (1.00-1.17) | 0.054 | |
| Placental abnormalities | groups | 1.03 (0.73-1.45) | 0.883 |
| fasting | 0.71 (0.45-1.12) | 0.137 | |
| 1hr | 1.07 (0.95-1.21) | 0.259 | |
| 2hr | 0.95 (0.81-1.11) | 0.500 | |
| Abnormal umbilical cord | groups | 0.93 (0.81-1.06) | 0.272 |
| fasting | 1.04 (0.88-1.24) | 0.656 | |
| 1hr | 0.99 (0.95-1.04) | 0.779 | |
| 2hr | 0.98 (0.92-1.04) | 0.453 | |
| Amniotic fluid volume abnormality | groups | 0.73 (0.55-0.97) | 0.029 |
| fasting | 1.21 (0.87-1.68) | 0.256 | |
| 1hr | 1.02 (0.93-1.13) | 0.638 | |
| 2hr | 1.01 (0.89-1.14) | 0.931 | |
| Abnormal stage of labor | groups | 0.33 (0.06-1.82) | 0.204 |
| fasting | 2.44 (0.71-8.38) | 0.156 | |
| 1hr | 0.70 (0.41-1.20) | 0.192 | |
| 2hr | 0.90 (0.45-1.82) | 0.774 | |
| Dystocia | groups | 0.99 (0.74-1.32) | 0.938 |
| fasting | 0.90 (0.62-1.30) | 0.565 | |
| 1hr | 0.91 (0.83-1.01) | 0.084 | |
| 2hr | 1.10 (0.96-1.25) | 0.162 | |
| Pregnancy-induced hypertension | groups | 1.65 (1.12-2.42) | 0.011 |
| fasting | 0.96 (0.58-1.59) | 0.885 | |
| 1hr | 1.00 (0.87-1.14) | 0.969 | |
| 2hr | 0.94 (0.79-1.12) | 0.486 | |
| Cholestatic syndrome | groups | 1.08 (0.57-2.06) | 0.814 |
| fasting | 0.55 (0.24-1.25) | 0.154 | |
| 1hr | 1.26 (1.02-1.57) | 0.036 | |
| 2hr | 0.99 (0.75-1.31) | 0.939 | |
| Perineal laceration | groups | 0.91 (0.78-1.06) | 0.211 |
| fasting | 0.92 (0.76-1.12) | 0.391 | |
| 1hr | 0.94 (0.89-0.99) | 0.017 | |
| 2hr | 1.04 (0.97-1.12) | 0.262 | |
| Postpartum hemorrhage | groups | 1.06 (0.45-2.51) | 0.887 |
| fasting | 0.44 (0.15-1.29) | 0.135 | |
| 1hr | 1.28 (0.97-1.70) | 0.086 | |
| 2hr | 1.02 (0.71-1.46) | 0.934 | |
| Postpartum infection | groups | 0.86 (0.37-2.01) | 0.727 |
| fasting | 1.43 (0.62-3.28) | 0.403 | |
| 1hr | 0.86 (0.64-1.15) | 0.313 | |
| 2hr | 1.25 (0.88-1.77) | 0.221 | |
| Poor postpartum uterine rejuvenation | groups | 1.14 (0.87-1.50) | 0.348 |
| fasting | 0.83 (0.58-1.19) | 0.304 | |
| 1hr | 1.07 (0.97-1.18) | 0.173 | |
| 2hr | 0.91 (0.80-1.04) | 0.151 | |
| Hypoproteinemia | groups | 0.34 (0.19-0.61) | 0.000 |
| fasting | 0.87 (0.46-1.66) | 0.673 | |
| 1hr | 0.89 (0.74-1.06) | 0.192 | |
| 2hr | 1.08 (0.85-1.37) | 0.521 |
| Outcomes | Variable | aOR (95% CI) |
|
|---|---|---|---|
| Fetal distress | groups | 0.59 (0.24-1.44) | 0.242 |
| fasting | 1.19 (0.43-3.31) | 0.735 | |
| 1hr | 1.15 (0.86-1.55) | 0.335 | |
| 2hr | 0.79 (0.53-1.17) | 0.231 | |
| Abnormal fetal position | groups | 1.84 (1.56-2.17) | 0.000 |
| fasting | 1.23 (1.01-1.51) | 0.041 | |
| 1hr | 0.92 (0.87-0.97) | 0.002 | |
| 2hr | 1.03 (0.96-1.11) | 0.372 | |
| Stillbirth | groups | 1.01 (0.52-1.99) | 0.967 |
| fasting | 0.53 (0.23-1.26) | 0.152 | |
| 1hr | 1.05 (0.83-1.33) | 0.671 | |
| 2hr | 1.20 (0.90-1.60) | 0.221 | |
| Preterm infant | groups | 0.86 (0.61-1.21) | 0.392 |
| fasting | 0.98 (0.65-1.48) | 0.929 | |
| 1hr | 1.11 (0.99-1.25) | 0.073 | |
| 2hr | 0.96 (0.82-1.12) | 0.598 | |
| Small for gestational age (SGA) | groups | 1.25 (0.27-5.72) | 0.773 |
| fasting | 1.18 (0.22-6.28) | 0.847 | |
| 1hr | 1.11 (0.66-1.88) | 0.688 | |
| 2hr | 1.04 (0.55-1.97) | 0.904 | |
| Large for gestational age (LGA) | groups | 1.32 (0.88-1.96) | 0.177 |
| fasting | 1.05 (0.64-1.70) | 0.857 | |
| 1hr | 1.11 (0.97-1.28) | 0.119 | |
| 2hr | 0.96 (0.81-1.15) | 0.661 | |
| Low birth weight infant | groups | 0.80 (0.50-1.30) | 0.375 |
| fasting | 0.81 (0.44-1.48) | 0.491 | |
| 1hr | 1.09 (0.92-1.28) | 0.334 | |
| 2hr | 0.98 (0.79-1.22) | 0.886 | |
| Macrosomia | groups | 0.83 (0.64-1.09) | 0.183 |
| fasting | 1.33 (0.98-1.81) | 0.072 | |
| 1hr | 0.99 (0.90-1.09) | 0.862 | |
| 2hr | 0.97 (0.86-1.10) | 0.641 | |
| Neonatal hypoglycemia | groups | 0.77 (0.50-1.18) | 0.230 |
| fasting | 1.05 (0.61-1.82) | 0.864 | |
| 1hr | 1.05 (0.90-1.22) | 0.551 | |
| 2hr | 0.88 (0.71-1.07) | 0.199 | |
| Neonatal hyperbilirubinemia | groups | 1.00 (0.86-1.17) | 0.976 |
| fasting | 1.08 (0.89-1.31) | 0.446 | |
| 1hr | 1.00 (0.95-1.06) | 0.968 | |
| 2hr | 0.99 (0.92-1.06) | 0.769 | |
| Neonatal asphyxia | groups | 1.23 (0.45-3.35) | 0.683 |
| fasting | 1.70 (0.68-4.26) | 0.260 | |
| 1hr | 1.21 (0.86-1.69) | 0.269 | |
| 2hr | 0.78 (0.51-1.20) | 0.254 | |
| Neonatal infection | groups | 1.09 (0.92-1.29) | 0.314 |
| fasting | 1.31 (1.07-1.61) | 0.009 | |
| 1hr | 1.00 (0.94-1.06) | 0.988 | |
| 2hr | 0.97 (0.90-1.05) | 0.401 | |
| Low Apgar score | groups | 0.93 (0.41-2.14) | 0.872 |
| fasting | 0.98 (0.38-2.52) | 0.969 | |
| 1hr | 1.19 (0.90-1.57) | 0.232 | |
| 2hr | 1.00 (0.70-1.42) | 0.989 | |
| Neonatal cephalohematoma | groups | 1.09 (0.84-1.43) | 0.519 |
| fasting | 0.73 (0.52-1.04) | 0.080 | |
| 1hr | 0.99 (0.91-1.09) | 0.904 | |
| 2hr | 1.12 (0.99-1.26) | 0.073 | |
| Fetal growth restriction (FGR) | groups | 1.64 (0.59-4.54) | 0.340 |
| fasting | 0.98 (0.27-3.56) | 0.969 | |
| 1hr | 0.88 (0.62-1.25) | 0.466 | |
| 2hr | 1.14 (0.73-1.79) | 0.571 | |
| Neonatal respiratory distress syndrome (NRDS) | groups | 0.59 (0.24-1.44) | 0.242 |
| fasting | 1.19 (0.43-3.31) | 0.735 | |
| 1hr | 1.15 (0.86-1.55) | 0.335 | |
| 2hr | 0.79 (0.53-1.17) | 0.231 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Birth, Development, and Health · Pregnancy and preeclampsia studies
Introduction
1
Gestational diabetes mellitus (GDM) is a metabolic disease characterized by impaired glucose metabolism and is first detected or diagnosed during pregnancy. Its incidence increases with lifestyle and dietary changes. The prevalence of GDM is estimated at 9.3–25.5% worldwide (1, 2) and 9.3–18.9% in China (3, 4). Studies (5–7) have shown that GDM is associated with an increased risk of multiple adverse outcomes for both mother and baby, including cesarean section, neonatal hypoglycemia, and neonatal hyperbilirubinemia.
GDM is mainly diagnosed using the oral glucose tolerance test (OGTT), for which there is still a lack of consensus (8–10). There are two main strategies recommended internationally: the one-step strategy (2-h 75-g OGTT), which is recommended by the International Association of Diabetes and Pregnancy Study Group (IADPSG) (11), and the two-step strategy (50-g glucose loading test and 3-h 100-g OGTT), which is recommended by the American College of Obstetricians and Gynecologists(ACOG) (12). In addition to the two methods mentioned, other screening strategies are being used in some countries and regions (13–17). In mainland China, the IADPSG one-step 2-h 75-g OGTT was recommended to diagnose GDM by the Obstetrics Association of the Chinese Medical Association in 2014 (18). However, the latest version of the “National Guide to Clinical Laboratory Procedures, 4th edition (2014)” (19) was recommended by the National Health Commission of the People’s Republic of China later in 2014. The procedure suggested a 100-g glucose dose to perform OGTT for pregnant women, but the blood collection time point and diagnostic threshold were not clear. As a result, some laboratories in mainland China, including Tongchuan People’s Hospital, used the IADPSG one-step approach and the corresponding diagnostic threshold value to screen GDM for pregnant women, and the glucose load was 100 g. Although international recommendations for OGTT methods are inconsistent and lack the support or recognition of authoritative guidelines, the application of OGTT still exists objectively today. Evaluating these methods may play a positive role in the improvement of GDM screening strategies.
This study employed a multidimensional analytical approach to systematically evaluate the following key metrics of 75g versus 100g OGTT: 1) Blood glucose levels at fasting (0h), 1h, and 2h post-load timepoints; 2) GDM screening performance based on IADPSG criteria, including diagnostic positivity rate, clinical characteristics of GDM population, and differential risks of adverse maternal-neonatal outcomes; 3) Correlation patterns of glucose values across different timepoints (0h, 1h, 2h); 4) Dose-effect relationship between dynamic glucose variations and adverse maternal-neonatal outcomes in the overall study population.
Materials and methods
2
Participant sources
2.1
OGTT data for GDM screening were available for 3,907 of 10,228 primiparas who gave birth in two districts of Tongchuan People’s Hospital. This retrospective study covers the period from January 1, 2017, to September 30, 2022. The timeframe was selected based on comprehensive considerations including data availability, quality, consistency in clinical practice, and group sample size balance, with the aim of enhancing the scientific rigor and result reliability of the study. All primiparas who gave birth at the hospital during this period were enrolled, and their data were retrospectively analyzed using electronic medical records. Data extraction took place from April 16 to April 23, 2023.According to the actual screening strategy adopted, participants were divided into the 75-g and 100-g OGTT groups. Among these, the 75-g glucose dose recommended by the IADPSG was used in OGTT between October 1, 2019, and September 30, 2022, in the central southern campus, and between September 18, 2018, and September 30, 2022, in the northern campus. The 100-g glucose dose recommended in the guidelines was used in the OGTT experiments on the southern campus area from January 1, 2017, to September 30, 2019, and on the northern campus from January 1, 2017, to September 17, 2018. Women with maternal diabetes mellitus before pregnancy, multiple births, chronic kidney disease, and related endocrine diseases, such as hyperpituitarism, hyperthyroidism, and adrenal hyperfunction, were excluded from the study. The electronic medical records in this study have clearly identified individuals who experienced vomiting, and we have verified and excluded all data from subjects who experienced vomiting through electronic medical record review.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study design was approved by the Ethics Committee of Tongchuan People’s Hospital (approval number: TCSRMYY2022-01-03-005). The requirement for written informed consent was waived owing to the retrospective nature of the study. This retrospective study was conducted according to the STrengthening the Reporting of OBservational studies in Epidemiology guidelines. When we obtained the data, we obtained the patients’ identifying information, including name, address, identification number, telephone number, clinical diagnosis and treatment information, various examination results, etc.; however, only age, sex, outcome, and treatment interventions are disclosed in the manuscript.
Main observation index
2.2
We obtained patient data from electronic medical records such as age, pregnancy duration at GDM screening and delivery, BMI at GDM screening and delivery and status of serum glucose management and treatment of GDM. Serum glucose levels at 0, 1 h, and 2 h time points during the 75-g and 100-g OGTT were analyzed. The correlations and regression lines for glucose levels (fasting vs. 1 h, fasting vs. 2 h, and 1 h vs. 2 h) were compared between the two groups. The GDM diagnosis rate and positive composition characteristics of the two groups were assessed using the IADPSG one-step diagnostic threshold. Further, 15 adverse maternal and 16 neonatal outcomes were evaluated. The 15 adverse maternal outcomes included abnormal fetal membranes, abnormal stage of labor, abnormal umbilical cord, abnormal amniotic fluid volume, placental abnormalities, cesarean section, cholestatic syndrome, dystocia, hypoproteinemia, perineal laceration, pregnancy-induced hypertension, poor uterine rejuvenation after childbirth, postpartum hemorrhage, and postpartum infection, as well as amniotic/chorionic abnormalities, induction of labor, postpartum fever, and postpartum anemia. The 16 adverse neonatal outcomes included abnormal fetal position, fetal distress, fetal growth restriction, low birth weight, large for gestational age, low Apgar score, macrosomia, neonatal cranial hematoma, neonatal asphyxia, neonatal hyperbilirubinemia, neonatal hypoglycemia, neonatal infection, neonatal respiratory distress syndrome, preterm delivery, small for gestational age, and stillbirth. These adverse outcomes are defined in Supplementary Methods 1.
GDM screening approach
2.3
GDM screening approaches were similar in the northern and southern regions of the hospital. Pregnant women maintained normal physical activity, a normal diet, and daily carbohydrate consumption of at least 150 g for 3 days before the test. Pregnant women fasted for 10–12 h on the day before OGTT (which was conducted no later than 9 am). During examination, the participants did not drink tea, drink coffee, smoke, or engage in strenuous exercise. OGTT was performed 2 h after ingesting a standard 75-g or 100-g glucose load.
Determination of serum glucose levels
2.4
Venous blood was collected in a procoagulant negative pressure tube, allowed to stand for 20 min, and centrifuged (3,000 rpm) for 5 min to separate the serum. The serum glucose level was detected using a Hitachi 008AS automatic biochemical analyzer (Toranomon, Minato-ku, Tokyo, Japan) in the south campus and a Hitachi 7,600 automatic analyzer (Toranomon) in the north campus. All procedures were completed within 2 h of blood collection. Hexokinase glucose detection reagents were produced by Ningbo Meikang Co., Zhejiang, China. The internal quality control data were controlled during the testing period. The external quality assessment data from the Shaanxi Provincial Clinical Laboratory Center and the Clinical Laboratory Center of the National Health Commission of China were qualified.
Diagnosis, management, and treatment of GDM
2.5
The diagnostic criteria for GDM in both groups were based on the 2010 IADPSG one-step screening method (11). Pregnant women were diagnosed with GDM if any of the following glucose thresholds were met: 0 h ≥5.1 mmol/L; 1 h ≥10.0 mmol/L; and 2 h ≥8.5 mmol/L. Pregnant women with GDM should undergo diet, exercise, and drug treatment according to the “Diagnosis and therapy guideline of pregnancy with diabetes mellitus (2014)” (20) (see Supplementary Methods 2 for details).
Statistical analyses
2.6
Data analysis was performed using SPSS Statistics 20.0 (IBM Corp., Armonk, NY, USA) for statistical computations and GraphPad Prism 8.0 (GraphPad Software Inc., La Jolla, CA, USA) for scatter plot generation. Continuous variables were assessed for normality via the Shapiro-Wilk test, with normally distributed data presented as mean ± standard deviation (mean ± SD) and compared using independent samples t-tests. Categorical variables were expressed as frequency (percentage), analyzed by chi-square tests. For OGTT glucose levels across timepoints (0h, 1h, 2h), intergroup comparisons were supplemented with Pearson correlation analyses and scatter plots.Employing a stratified analytical approach, we systematically evaluated 15 maternal and 16 neonatal adverse outcomes. In the GDM-positive cohort: 1) Potential determinants were screened through univariate analysis; 2) Multivariable unconditional logistic regression adjusted for baseline characteristics (age, pre-pregnancy BMI, gestational weight gain) to quantify outcome risk differences; 3) Log-linear modeling examined outcome interactions, with variance inflation factors (VIF <5) confirming absence of multicollinearity. For the full cohort, binary logistic regression modeled OGTT glucose levels (continuous) against adverse outcomes (dichotomous) to characterize dose-response relationships, adjusting for identical covariates. All analyses rigorously accounted for GDM diagnostic criteria and confounders—particularly excessive gestational weight gain per National Academy of Medicine standards (21, 22). Effects are reported as odds ratios (ORs) and adjusted odds ratios (aORs) with 95% confidence intervals. Statistical significance for primary outcomes was defined as p < 0.05 (two-tailed α=0.05). (Detailed protocols: Supplementary Methods 3).
Results
3
Baseline characteristics of the study population
3.1
After applying the exclusion criteria, this study included 1,925 pregnant women (430 with GDM) in the 75-g OGTT group and 1,982 pregnant women (460 with GDM) in the 100-g OGTT group. Maternal age, pregnancy duration at GDM, body mass index (BMI), and incidences of other abnormalities were calculated (Table 1). No significant difference was noted in these characteristics between the groups (p > 0.05). Similarly, pregnancy duration and BMI at the time of delivery showed no significant differences (p > 0.05; Table 1). There was no significant difference in serum glucose control among GDM-positive people between the groups (p > 0.05; Supplementary Table 1).
Comparison of serum glucose levels between the groups
3.2
There was no significant difference in fasting glucose levels between the two groups (p > 0.05). The serum glucose levels at 1 h and 2 h after oral glucose were significantly lower in the 75-g group than in the 100-g group (p < 0.05), as shown in Table 2.
Comparison of GDM diagnostic rates, positive composition ratio, and adverse outcomes between groups
3.3
Using IADPSG one-step criteria, no significant differences were observed in GDM diagnostic rates or positive case characteristics between groups (p > 0.05; Table 3). Similarly, maternal and neonatal adverse outcomes showed no significant differences (p > 0.05; Tables 4, 5). Given potential confounding by age, gestational age, BMI trajectory, and post-diagnosis interventions, we performed full covariate adjustment (Supplementary Table 2). Logistic regression analysis using the 75g group as reference demonstrated that the 100g group’s risk profile for adverse outcomes (expressed as aORs) remained stable before versus after adjustment (p > 0.05; Tables 4, 5). In the GDM-negative population, there were no significant differences in the risks of adverse outcomes between the 75g and 100g oral glucose tolerance tests, except for the “other” outcomes category (p > 0.05). Among those screened and diagnosed with GDM who received corresponding management, the risks of adverse pregnancy outcomes showed no significant difference compared to the GDM-negative group, except for cesarean delivery (p > 0.05). In contrast, the screened group demonstrated a statistically significant reduction in the risk of major adverse pregnancy outcomes compared to the unscreened group (p < 0.05); for detailed results, please refer to Supplementary Table 3.
Intergroup analysis of glycemic correlations
3.4
Significant positive correlations were observed between fasting vs. 1h, fasting vs. 2 h, and 1 h vs. 2 h blood glucose levels in two groups (see Supplementary Table 4). The effects of different glucose loads (75-g vs. 100-g) on glycemic kinetics demonstrated distinct phase-specific variations: During the fasting-to-1h phase, the rate of glucose elevation (slope) showed no statistically significant difference between the two groups [Difference in slope (95% CI): 0.127 (-0.092 to 0.346), p=0.254]; in the fasting-to-2 h phase, the 100-g group exhibited a significantly higher glucose elevation rate than the 75-g group [Difference in slope (95% CI): 0.412 (0.244 to 0.580), p<0.0001]; during the 1h-to-2 h phase, glucose decline occurred significantly more slowly in the 100-g group [Difference in slope (95% CI): 0.047 (0.010 to 0.084), p=0.013], see Figure 1.
Scatters of fast Vs 1h, fast Vs 2h, 1h Vs 2h in two groups. (A)fast Vs 1h; (B) fast Vs 2h; (C) 1h Vs 2h. Solid lines represent regression fits for each group (red: 75 g group; black: 100 g group). Difference in slope was defined as the slope of the 100 g group minus that of the 75 g group.
Analysis of the continuous dose-response relationship between blood glucose levels and adverse outcomes in two groups
3.5
After adjusting for potential confounders, no significant differences were observed in the incidence of any adverse outcomes between the two groups (all *p >*0.05; Tables 6, 7). The effects of glucose levels varied by timepoints.For example, for cesarean delivery risk, each 1 mmol/L increase in fasting glucose was associated with a 27.5% significantly higher risk (aOR=1.275, 95%CI:1.084-1.501, *p=*0.003), while 1-h postprandial glucose showed a 5.1% increased risk per 1 mmol/L (aOR=1.051, 95%CI:1.004-1.100, *p=*0.032), with no significant effect of 2-h glucose (p = 0.649); for macrosomia risk, although neither fasting (aOR=1.33, 95%CI:0.98-1.81, *p=*0.072), 1-h (aOR=0.99) nor 2-h glucose (aOR=0.97) reached statistical significance, the effect size and upper 95%CI limit of fasting glucose suggested potential clinical relevance. Detailed results for other adverse outcomes are shown in Tables 6 and Table 7.
Discussion
4
The international controversy regarding the standardization of GDM screening persists, primarily manifested in three aspects: First, fundamental discrepancies exist in international guidelines—the IADPSG recommends the one-step 75g approach, while the ACOG advocates the two-step 50g+100g method, with significant differences in key parameters including glucose load, blood sampling timepoints, and diagnostic thresholds (13, 23, 24). Second, global implementation standards demonstrate regional variations: some countries rely solely on 2h glucose values while others incorporate both 1h and 2h measurements (14); within the United States alone, cutoff values for the 50g screening test vary between 7.2, 7.5, and 7.8 mmol/L across different states (23); and mainland China, while adopting the NDDG standard framework, employs IADPSG diagnostic cutoffs (13). Third, screening strategy selection is further influenced by multiple factors including regional epidemiological characteristics, healthcare resource allocation, and cultural acceptance (13, 14, 23). This global inconsistency in standards not only fuels diagnostic controversies regarding over- or under-diagnosis of GDM, but also severely compromises the comparability of epidemiological data, underscoring the urgent need for establishing internationally unified screening criteria. Against this backdrop, this study focuses specifically on evaluating differences between 75g and 100g glucose loads in OGTT-based GDM screening, aiming to provide evidence-based support for developing standardized protocols.
This study systematically evaluated the diagnostic performance of the 100g 2h OGTT for GDM screening and pregnancy outcome prediction, using the one-step 75g 2h OGTT recommended by the IADPSG as the reference standard. The results demonstrated that although the 100g group showed significantly higher postprandial glucose levels at 1h and 2h timepoints compared to the 75g group (p < 0.05, Table 2), no statistically significant differences were observed between the two groups in fasting glucose levels, GDM diagnosis rates, or clinical characteristics of GDM-positive individuals (p>0.05, Table 3). These findings likely reflect the physiological mechanisms of glucose homeostasis maintained through multi-organ coordination, including hepatic glucose metabolism regulation, compensatory insulin secretion, and peripheral tissue glucose uptake (24, 25). This suggests that the difference in glucose loads between 75-100g may not exceed the threshold required to disrupt the body’s compensatory balance, thereby failing to induce significant metabolic disturbances. These results provide important physiological evidence for selecting appropriate OGTT glucose loads in clinical practice.
Current evidence demonstrates that clinical management of GDM exerts greater influence on pregnancy outcomes than screening method selection (26, 27). Our study revealed consistent clinical interventions between the two GDM groups, with potential confounders controlled through restriction to primiparous women and adjustment for covariates including BMI trajectory. Notably, GDM and excessive gestational weight gain exhibited significant interaction effects on both cesarean delivery rate and gestational hypertension incidence (p < 0.05; Supplementary Table 2). After comprehensive adjustment, both groups showed comparable risks of adverse outcomes (p>0.05, Tables 4, 5). In the GDM-negative population, no statistically significant differences were observed in the risks of adverse outcomes between the 75g and 100g oral glucose tolerance tests, except for the “other” outcomes category (Supplementary Table 3). This indicates that under the IADPSG criteria, the two OGTT loads have comparable predictive value. The observed difference within the “other” category may be due to the limited sample size, and further validation in larger studies is warranted.
Under a unified diagnostic criterion—that is, using identical glucose thresholds and cut-off values—the volume of the OGTT glucose load (75g versus 100g) does not significantly impact the diagnostic efficacy for GDM or alter the risks associated with adverse pregnancy outcomes. This result aligns with existing literature emphasizing the central importance of diagnostic thresholds (reference 14). Moreover, among those diagnosed with GDM through screening and subsequently managed, the risks for most adverse outcomes did not differ significantly from those in the GDM-negative population (Supplementary Table 3), highlighting the effectiveness of systematic GDM management. However, the higher rate of cesarean delivery observed in the GDM-positive group suggests that GDM may itself be an independent risk factor for cesarean section. The elevated risk of adverse outcomes in the unscreened group (Supplementary Table 3) further underscores the clinical importance of implementing OGTT screening and appropriate GDM management.
Dynamic glycemic correlation analysis revealed significant yet modest time-dependent correlations (fasting→1h→2h) within both 75g and 100g glucose load groups (all R²=0.138-0.413, p<0.0001; Supplementary Table 4). These findings indicate that: (1) Fasting glucose levels, serving as metabolic baselines, partially predict subsequent glycemic responses but explain limited variation (≤24.0%); (2) The fasting vs. 2h glucose association was stronger under 100g loading (75g R²=0.138 vs. 100g R²=0.240), suggesting high-dose amplification of inter-individual baseline variations with potential implications for diabetes risk stratification; (3) Collinear effects between fasting and dynamic glucose levels (e.g., each 1 mmol/L fasting increase caused 0.412 mmol/L additional 2h glucose elevation specifically in 100g group) underscore the necessity of baseline adjustment in clinical trials, which could otherwise mask true intervention effects.
Figure 1 demonstrated comparable fasting-to-1h glucose elevation rates between 75g and 100g glucose loads (no dose-dependent difference in early-phase response). The 100g group exhibited significantly accelerated glucose rise during fasting-to-2h phase (indicating dose-amplified late-phase hyperglycemia) and attenuated glucose decline at 1h-to-2h phase. Collectively, 100g loading altered glucose metabolism through enhanced late-phase glycemic surge and prolonged hyperglycemia, whereas 75g loading better maintained glucose homeostasis. These differential responses reflected more stable/efficient physiological regulation of 75g glucose.
Given the absence of statistically significant differences in outcome risks among women diagnosed with GDM based on diagnostic cutoff values, we conducted an in-depth analysis using binary logistic regression models. In these models, the occurrence of adverse outcomes served as the dichotomous dependent variable, while glucose levels at each time point were included as continuous independent variables. The analysis incorporated adjustments for potential confounding factors, including interactions between glucose levels at different time points, to systematically evaluate the risk of adverse outcomes in the entire study population across both groups. The results demonstrated that although glucose levels at various time points showed correlations with most adverse outcomes, with varying degrees of association for different outcomes, none of the adverse outcome rates exhibited statistically significant differences between the two groups (all p > 0.05; Tables 6, 7). These findings provide robust evidence that the glucose load is not a primary determinant influencing the occurrence of adverse outcomes.
The incidence of adverse outcomes in this study differed from those in other studies; for example, the incidences of hypoproteinemia in the 75-g and 100-g OGTT groups in our study were 2.09% (9/430) and 2.61% (12/460), respectively. Yuen et al. (28) reported that the incidence of hypoproteinemia was 4.6%. However, the incidence of macrosomia between the two groups in our study was 6.98% (30/430) and 8.04% (37/460), respectively. Moreover, Niroomand et al. (29) reported the incidence of macrosomia as 4.5%. These differences may be due to the occurrence of GDM influenced by region, socioeconomic status, and nutritional status (1–4), not related to the OGTT glucose dose.
All data in this study were collected from two campuses in Tongchuan People’s Hospital. The total number of primiparas in this region from 2017 to 2022 was 20,042 (http://www.tongchuan.gov.cn/), of whom 6,427 were at Tongchuan People’s Hospital. Ultimately, a total of 3,907 primiparas (19.49%) were included in this study. Therefore, this research provides a good representation of this region. Moreover, the total numbers of adverse outcomes of pregnant women and newborns in this study were 15 and 16, respectively, more than those included in many other similar studies (27, 29).
This study has several limitations. Ideally, both the IADPSG and C&C criteria should have been applied for cross-analysis of the two groups. However, due to the retrospective design, the historical 100g OGTT tests did not include the 3-hour glucose measurement. Moreover, the 100g OGTT was intended to be performed only after a positive 50g GCT preliminary screening—a test not routinely conducted at our institution—making related data unavailable. Similarly, applying the C&C criteria was not feasible for the 75g OGTT group due to the lack of 3-hour glucose values. Given considerations of data accessibility and reliability, the IADPSG criteria (i.e., the 75g OGTT and its diagnostic thresholds) were uniformly used in this analysis. Additionally, information on the management and treatment of gestational diabetes mellitus (GDM) could only be obtained through retrospective medical record review, and statistical methods were employed to minimize inaccuracies. Nonetheless, lifestyle factors such as alcohol consumption, dietary quality, physical activity level, as well as socioeconomic indicators beyond education, were generally not systematically documented in medical records. This may have resulted in residual confounding and might have influenced the outcomes. Furthermore, since December 2019, the COVID-19 pandemic has affected both GDM screening and post-diagnosis management (30). This factor was not assessed in the present study and may also represent a potential source of interference.
In summary, under the IADPSG criteria, our study found no significant differences in GDM detection rates or adverse pregnancy outcomes between the 75-g and 100-g OGTT protocols. These results suggest that the two loads have comparable diagnostic and prognostic performance; however, a formal equivalence or non-inferiority trial is ultimately required to confirm true equivalence. To enhance clinical consistency and comparability across practices, we recommend that countries or regions move toward adopting a unified OGTT glucose load. The development of such a standardized screening strategy should be informed by multidisciplinary expertise, encompassing clinical, laboratory, health economic, and sociological perspectives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allehdan SS Basha AS Asali FF Tayyem RF. Dietary and exercise interventions and glycemic control and maternal and newborn outcomes in women diagnosed with gestational diabetes: systematic review. Diabetes Metab Syndr. (2019) 13:2775–84. doi: 10.1016/j.dsx.2019.07.040, PMID: 31405707 · doi ↗ · pubmed ↗
- 2Zhu Y Zhang C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: a global perspective. Curr Diabetes Rep. (2016) 16:7. doi: 10.1007/s 11892-015-0699-x, PMID: 26742932 PMC 6675405 · doi ↗ · pubmed ↗
- 3Leng J Shao P Zhang C Tian H Zhang F Zhang S. Prevalence of gestational diabetes mellitus and its risk factors in Chinese pregnant women: a prospective population-based study in Tianjin, China. Plo S One. (2015) 10:e 0121029. doi: 10.1371/journal.pone.0121029, PMID: 25799433 PMC 4370728 · doi ↗ · pubmed ↗
- 4Ye W Luo C Huang J Li C Liu Z Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. (2022) 377:e 067946. doi: 10.1136/bmj-2021-067946, PMID: 35613728 PMC 9131781 · doi ↗ · pubmed ↗
- 5Zheng Y Shen Y Jiang S Ma X Hu J Li C. Maternal glycemic parameters and adverse pregnancy outcomes among high-risk pregnant women. BMJ Open Diabetes Res Care. (2019) 7:e 000774. doi: 10.1136/bmjdrc-2019-000774, PMID: 31798901 PMC 6861069 · doi ↗ · pubmed ↗
- 6Ejaz Z Azhar Khan A Sebghat Ullah S Aamir Hayat M Maqbool MA Amin Baig A. The effects of gestational diabetes on fetus: a surveillance study. Cureus. (2023) 15:e 35103. doi: 10.7759/cureus.35103, PMID: 36938248 PMC 10023128 · doi ↗ · pubmed ↗
- 7Metzger BE Coustan DR Trimble ER. Hyperglycemia and adverse pregnancy outcomes. Clin Chem. (2019) 65:937–8. doi: 10.1373/clinchem.2019.303990, PMID: 30996054 · doi ↗ · pubmed ↗
- 8Egan AM Dunne FP. Diagnosis of gestational diabetes mellitus: the debate continues. Nat Rev Endocrinol. (2022) 18:723–4. doi: 10.1038/s 41574-022-00761-9, PMID: 36266574 · doi ↗ · pubmed ↗