A Novel Municipal-Level Approach to Uncover the Hidden Burden of Hepatitis C: A Replicable Model for National Elimination Strategies
Pietro Torre, Silvana Mirella Aliberti, Tommaso Sarcina, Mariano Festa, Chiara D’Amore, Giuseppe D’Adamo, Michele Gambardella, Antonella Santonicola, Gaetano Manzi, Mario Masarone, Mario Capunzo, Marcello Persico

TL;DR
This study introduces a new municipal-level model to identify hidden hepatitis C cases in Italy, aiming to improve national elimination efforts.
Contribution
The study presents a replicable municipal-level approach to quantify the hidden burden of HCV and address regional disparities.
Findings
Rural areas showed a higher hidden HCV burden (7 per 1000) compared to urban areas (3 per 1000).
Advanced fibrosis or cirrhosis was associated with age, male sex, urban residence, and genotype 1b.
The model highlights urban–rural disparities in underdiagnosis and late diagnosis of HCV.
Abstract
Background: Hepatitis C Virus (HCV) remains a global health challenge as WHO elimination targets are not achievable in most countries, mainly due to the high number of undiagnosed individuals. In Italy, where national elimination efforts are ongoing, regional disparities further hinder progress. This study aimed to characterize the hidden burden of chronic HCV infection across t he territory of the Province of Salerno, Southern Italy, to suggest a novel municipal-level screening approach, with implications for national strategies. Methods: We analyzed records of residents diagnosed with chronic HCV infection and linked to care between 2015 and 2022. Data included age, sex, municipality of residence, HCV genotype, and fibrosis stage. Observed prevalence was compared with expected prevalence derived from national/regional benchmarks. Municipalities were categorized as urban or rural based…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
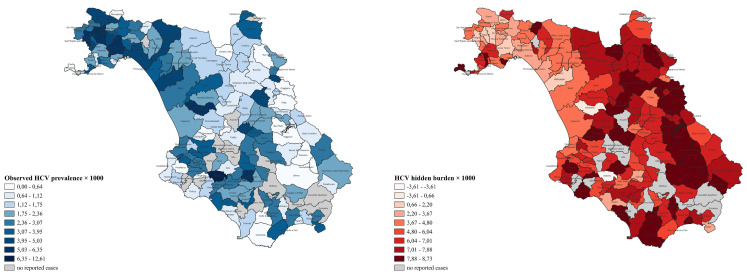 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease Diagnosis and Treatment · Hepatitis C virus research · Food Security and Health in Diverse Populations
1. Introduction
Although major advances in treatment have made the infection by hepatitis C virus (HCV) curable, it continues to pose a significant global health challenge. Nearly a decade after the World Health Organization (WHO) set the goal of eliminating viral hepatitis by 2030, including hepatitis C, only a limited number of countries are currently on track to achieve this objective, and it is estimated that 50 million individuals are still chronically infected worldwide. Key barriers to elimination include disparities in access to diagnosis and treatment, along with the significant financial and infrastructural burden associated with delivering comprehensive care services [1,2,3,4,5]. Notably, Italy, which has one of the largest populations of HCV-infected subjects in Europe [6], is also among the nations where the impact of such infection appears insufficiently managed according to the Polaris Observatory [7]. Once considered virtuous in the race toward elimination, thanks to its treatment policies and a growing number of treated patients [8,9], the country has subsequently entered a phase of stagnation. This is because the number of patients diagnosed and receiving antiviral treatment in recent years has not been deemed high enough to achieve the established targets [10]. Regional variations in the implementation of hepatitis C-related activities further hinder national progress.
The observed reduction in antiviral therapies over recent years, coupled with an estimated high number of undiagnosed individuals, the so-called “hidden burden” of infections, many of which are associated with advanced liver disease, highlights the crucial importance of screening activities [10,11,12]. Since universal screening is not currently implemented in most countries, the effectiveness of existing strategies depends heavily on the prioritization of populations with a higher expected prevalence. These, according to the “micro-elimination” model, include high-risk subjects such as people who inject drugs (PWID), prisoners, men who have sex with men (MSM), and individuals born within specific age cohorts (e.g., 1945–1965), regardless of knowledge of known risk exposures [2,10,13,14,15]. This approach has a major limitation: it overlooks the role of geographic disparities, failing to capture the healthcare inequalities that penalize hepatitis C care in remote or underserved areas, even in high-income countries. It is well known that remote communities have fewer liver specialists and HCV-related services, with distance being a barrier to accessing them, and with general practitioners (GPs) often representing the only easily accessible point of contact for healthcare. While some countries have improved access to care, for example, by allowing non-specialists to prescribe direct-acting antivirals (DAAs), this is not yet a widespread practice and is not even adopted in Italy [2,16,17,18,19]. In these cases, specific dynamics between local physicians and the community may not ensure equitable access to HCV diagnosis and treatment.
Given the lack of data on these aspects in Italy, we conducted an analysis of the geographic distribution of actively infected HCV patients who underwent antiviral therapy at hepatology centers in the Province of Salerno, as a proxy for individuals who were successfully screened, diagnosed, and linked to care. Particular attention was given to urban–rural differences within the Province, which, in its nearly 5000 km^2^, is home to over a million people, and is located in Campania (southern Italy), an area historically known for high hepatitis C prevalence [20]. By integrating local data with regional and national prevalence benchmarks, we aimed to geographically characterize the hidden burden of HCV, hypothesizing significant disparities between rural and urban areas. The gap which we intended to investigate is not just a mere epidemiological issue; it conceals cases that could progress to cirrhosis, liver decompensation, or hepatocellular carcinoma—conditions that heavily impact a person’s life and the costs of the healthcare system.
The primary objective of this study was to estimate the hidden burden of chronic HCV infection across the Province of Salerno (Campania region), Southern Italy, by applying a novel municipal-level epidemiological model. This was achieved by comparing observed and expected prevalence, derived from regional and national benchmarks, with particular attention to urban–rural disparities, and with the goal of providing population-based evidence supporting national HCV elimination initiatives through identification of priority areas for screening and linkage to care.
In parallel, secondary objectives included describing the demographic and clinical characteristics of chronically HCV-infected people residing in this territory; calculating observed HCV prevalence (diagnosed and linked-to-care cases) at both municipal and provincial levels, and stratified by age group and urban–rural status; estimating the expected prevalence by applying age-specific prevalence rates from the literature to official ISTAT population data, thereby quantifying the hidden burden by age group and geographic setting; supporting a refined classification of municipalities based on discrepancy between observed and expected cases to inform geographically targeted public health strategies.
Our model could offer a replicable framework for regional health authorities to prioritize screening and resource allocation, with potential applicability to other infectious or chronic diseases characterized by hidden prevalence. To the best of our knowledge, this is the first study in Italy to integrate municipal-level prevalence mapping with hidden burden estimates and a novel urban–rural classification system.
2. Patients and Methods
2.1. Study Design, Inclusion Criteria, and Setting
This is a multicenter, retrospective study aimed at quantifying both the observed and hidden burden of HCV infection in the Province of Salerno, Southern Italy, with the goal of supporting future screening initiatives. The study included patients who had been diagnosed with and treated for chronic hepatitis C, defined by detectable HCV-RNA in serum, and with registered residence in the Province of Salerno during the study period (March 2015–December 2022). Patients treated for hepatitis C at participating centers but living outside the province were excluded from the analysis. Additionally, five patients were excluded because their municipality of residence was unknown. All cases of active infection were included, regardless of clinical status, treatment outcome, or subsequent death. Treatment-related data (e.g., sustained virologic response, SVR) were not collected, as among the study’s objectives was not to evaluate treatment efficacy but rather to measure the cumulative diagnosed and linked-to-care HCV cases. To ensure internal validity and avoid double-counting, records were deduplicated across hospitals by cross-checking personal identifiers available at the extraction stage (name, date of birth, municipality of residence). This procedure was performed before anonymization. After deduplication, all direct identifiers were removed, and only anonymized records were retained for analysis.
Among the 158 municipalities of the province, 139 had at least one confirmed case, while in the remaining 19, no diagnosed and linked-to-care HCV cases were found. These 19 municipalities are predominantly small, all with fewer than 5000 residents, and most are located in peripheral or hilly areas of the province. For the main analysis, a cumulative approach was adopted, aggregating all diagnosed cases identified between 2015 and 2022 without stratification by year of diagnosis. This methodology was selected to estimate period-prevalence, allowing for a comprehensive assessment of the total burden of infections and for the identification of geographic and demographic gaps in case detection; in fact, the study’s objective was to estimate the overall diagnosed and hidden burden at the municipal level rather than changes over time. This strategy ensured sufficient statistical power for smaller municipalities and strengthened the robustness of municipal-level comparisons. However, we also analyzed temporal dynamics by stratifying data on observed cases, hidden burden, and patient characteristics across two 4-year periods, 2015–2018 and 2019–2022.
2.2. Data Sources
2.2.1. Clinical Data
Clinical data of HCV cases were extracted from multiple clinical sources, including electronic health records from public healthcare facilities in the Campania region. The dataset included anonymized records of patients diagnosed and linked-to-care for antiviral therapy at major provincial hospitals, which included all five adult DAAs prescribing centers active in the province during the study period: San Giovanni di Dio e Ruggi d’Aragona Hospital (Gastroenterology Unit, Infectious Disease Unit, and Internal Medicine and Hepatology Unit) in Salerno, San Luca Hospital (Infectious Disease Unit) in Vallo della Lucania, and Umberto I Hospital (General Medicine Unit) in Nocera Inferiore.
Data extraction was conducted in 2024 to ensure temporal consistency across sources. The collected variables included age at presentation for therapy, sex, municipality of residence, HCV genotype, and liver fibrosis stage, assessed before treatment with the METAVIR scoring system (F0–F4). Fibrosis was primarily evaluated via vibration-controlled transient elastography (VCTE) (FibroScan^®^, Echosens, Paris, France), with 10 kPa and 13 kPa as cutoffs for advanced fibrosis (F3) or cirrhosis (F4), respectively [21].
2.2.2. Population Data
Municipality-level and age-stratified population data for the Province of Salerno were obtained from the Italian National Institute of Statistics (ISTAT) [22], with reference date 1 January 2025. These data were used as denominators for the calculation of crude, age-specific, and geographically stratified prevalence rates. Population estimates were based on the most recent and official demographic data available at the time of analysis. Given the modest but steady annual population decline observed in the area [23], demographic shifts over the eight-year study period (2015–2022) were considered negligible for prevalence calculations and unlikely to significantly bias the results.
2.3. Age Stratification
Both diagnosed cases and the general population were stratified into four age groups, based on ISTAT categories, but adapted to reflect HCV epidemiological patterns [24,25]:
- 0–29 years: younger individuals (recent transmission routes, e.g., injection drug use).
- 30–45 years: younger adults with intermediate risk profiles.
- 46–56 years: middle-aged adults.
-
56 years: older adults, more likely exposed to historical iatrogenic sources (e.g., unscreened blood transfusions and non-sterile procedures).
2.4. Urban/Rural Classification
Municipalities were classified as urban or rural based on a threshold of 5000 inhabitants and on population density, using a cutoff of 150 inhabitants/km^2^, in line with ISTAT’s municipal classification methodology and OECD-Eurostat criteria [26,27]. Municipalities with at least 5000 inhabitants and 150 inhabitants/km^2^ were classified as urban. Conversely, municipalities with less than 5000 inhabitants and/or less than 150 inhabitants/km^2^ were classified as rural. This classification aligns with the Eurostat typology: urban areas corresponded to levels 1 and 2 (densely and intermediate populated areas), while rural areas aligned with level 3 (thinly populated areas) [26].
Urban areas (≥5000 inhabitants and ≥150 inhabitants/km^2^): characterized by higher population density, greater availability of healthcare services (e.g., hospitals, diagnostic centers), and more diversified economic activities. These included 38 municipalities, totaling 791,298 inhabitants.Rural areas (<5000 inhabitants and/or <150 inhabitants/km^2^): characterized by lower population density, economies based primarily on agriculture or tourism, and reduced access to specialist healthcare services. These comprised 101 municipalities, totaling 247,430 inhabitants.
2.5. Prevalence of Infection and Hidden Burden Estimation
2.5.1. Observed Prevalence
The observed prevalence of chronic HCV infection was calculated for each municipality and for the Province of Salerno overall, using the following formula:
Prevalence was computed both at the municipal level (e.g., Ottati: 1.73 per 1000) and aggregated by urban and rural areas. Age-specific prevalence was calculated using the following formula:
where i refers to each of the four predefined age groups (0–29, 30–45, 46–56, and >56 years).
2.5.2. Expected Prevalence of Active HCV Infection
Based on published estimates of the burden of chronic HCV infection in Italy, we used age-specific prevalence rates from national and regional studies as external reference values. At the national level, the overall prevalence of active HCV infection has been estimated at 0.66% (95% CI: 0.66–0.67, as of January 2021), with higher values reported in Southern regions (0.72%) compared to Northern ones (0.54%) [12]. These data were obtained from a mathematical model incorporating variables such as new infections, migrations, and demographic factors (e.g., new births, deaths), with previously treated individuals being subtracted from the estimate. Regional analyses reported a broader range (0.1–2.4%) and demonstrated a clear age-related gradient [20,28,29,30]. From these data, we applied the following age-specific expected prevalences: 0–29 years: 0.12%; 30–45 years: 0.6%; 46–56 years: 1.2%; >56 years: 2.5%. These values, derived from prior epidemiological evidence, reflect reduced transmission in younger cohorts (due to improved medical practices, such as blood screening and single-use needles, and the introduction of DAAs) and higher prevalence in older individuals, who were more likely to have been exposed to historical iatrogenic routes of transmission. The validity of the lower prevalence for younger groups is further supported by SEIEVA surveillance data on acute HCV infections.
For geographic comparisons, expected prevalence ranges were stratified by setting to reflect contextual differences: urban areas 0.6–0.8%, characterized by greater availability of healthcare infrastructure and screening opportunities; and rural areas 0.8–1.0%, typically older in demographic profile and with fewer healthcare facilities and liver specialists, lower public awareness, and potential socioeconomic vulnerabilities [31,32,33]. These reference values were multiplied by ISTAT population estimates to calculate the expected number of HCV cases at municipal and provincial levels. The expected cases were also estimated by assuming the same prevalence (0.6–0.8%) in the two different settings.
2.5.3. Hidden Burden of HCV
The hidden burden was calculated by subtracting the number of observed cases from the expected cases:
This was performed across municipalities, urban/rural classification, and provincial levels using the expected prevalence rates described above.
2.5.4. Bayesian Prevalence
Building on the cumulative approach aggregating data from 2015 to 2022 described in Section 2.1, Bayesian smoothing was applied as an alternative method to stabilize prevalence rates in municipalities with small populations and low case counts. This approach adjusts raw municipal prevalence estimates by incorporating information from a prior rate, with the degree of shrinkage determined by the population size of each municipality. Observed HCV cases, resident population, and prior rates (7 per 1000 for urban areas, 9 per 1000 for rural areas) were used as inputs. This procedure reduces random variability, yielding more reliable estimates while preserving local differences. A stabilization parameter (τ = 10,000) was used to adjust the degree of shrinkage. Bayesian Prevalence per 1000 was calculated using the formula:
2.6. Municipality Classification Criteria
Municipalities were classified into three epidemiological categories based on Poisson test results, comparing observed to expected case counts:
- Underdiagnosed areas: Observed cases significantly below expected (p < 0.05), suggesting gaps in detection or healthcare access.
- Hotspot areas: Observed cases significantly exceeded expected values (p < 0.05), indicating possible local transmission clusters or enhanced screening programs.
- Other area: No significant difference (p ≥ 0.05) between observed and expected cases.
2.7. Statistical Analysis
Descriptive statistics summarized all demographic and clinical variables, and patients were classified according to municipality of residence (urban/rural), age group, sex, HCV genotype, and fibrosis stage. Data are represented as absolute numbers and percentages or mean ± standard deviation (SD). Chi-square test and Mann–Whitney test were used for categorical variables and continuous variables, respectively; multivariate logistic regression was used to identify predictors of F3–F4 fibrosis. The Poisson test was used to evaluate deviations from expected prevalence at the municipality level. Statistical significance was set at p < 0.05 (two-tailed). Statistical analysis was conducted using STATA v16.1 and GraphPad Prism 10.4.2.
2.8. Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and Italian data regulations. All patient data were anonymized and analyzed in aggregate form. Due to the retrospective design, the exclusive use of anonymized records, and publicly available data, formal ethical approval was not required.
3. Results
3.1. Study Population and Demographics
Between 2015 and 2022, a total of 3528 confirmed and linked-to-care chronic active HCV cases were identified across 139 municipalities in the Province of Salerno, covering 98.5% of the provincial population (1,038,728) (Table 1). Urban areas comprised 38 municipalities (791,298 inhabitants), accounting for 86.9% (3067) of cases, while rural areas included 101 municipalities (247,430 inhabitants), with 13.1% (461) of cases. All 19 municipalities with no identified cases were rural, comprising a total population of 16,038 inhabitants.
The age distribution of cases showed a marked predominance in older adults, with the mean age being approximately 63 years. Individuals aged >56 years represented 65.5% of all cases (2310/3528), followed by those aged 46–56 (21.7%), 30–45 (11.7%), and 0–29 (1.1%). A slight male predominance was observed (54.7%), and fibrosis staging revealed that 50.2% of patients were diagnosed at advanced stages (F3–F4), suggesting a significant delay in diagnosis and treatment initiation, meaning, in turn, that many patients were identified only when their risk of serious outcomes was greater. Genotype 1b was the most prevalent (38.6%), followed by genotype 2 (31.3%), genotype 3 (13.3%), genotype 1a (12.0%), genotype 4 (4.6%), and other genotypes (0.3%).
Overall, observed HCV prevalence was 0.34% (3.40 per 1000 population; 95% CI: 0.33–0.35), while the total expected number of HCV cases (using an estimated prevalence of 0.72%) was about 7479, indicating a hidden burden of 3951 undiagnosed cases.
Despite having a smaller estimated total of undiagnosed cases, in rural areas the prevalence of the hidden burden per 1000 inhabitants was more than double compared to urban ones (3.12 in urban vs. 7.14 in rural areas, and slightly higher if we also include the 19 rural municipalities with no detected cases); by using the same expected prevalence of cases (of 0.6–0.8%) in the two settings, rural areas still had a higher prevalence of undiagnosed cases (5.14 per 1000 inhabitants). In particular, urban areas, comprising 791,298 inhabitants, demonstrated a greater number of diagnosed, linked-to-care cases. Nevertheless, a substantial hidden burden of undiagnosed infection persists. Applying an expected prevalence range of 0.6–0.8%, the estimated number of HCV cases in urban areas was 4748–6330, compared to 3067 observed cases. This corresponds to an estimated hidden burden of 1681–3263 undiagnosed individuals. In contrast, rural areas (247,430 inhabitants) exhibited a lower number of cases and observed prevalence of 1.86 per 1000 (461/247,430), compared to urban areas (3.88 per 1000; 3067/791,298; p < 0.001 for urban vs. rural prevalence). By using a higher expected prevalence of 0.8–1.0% in this context, the estimated number of cases in rural areas corresponded to 1979–2474, yielding a hidden burden of 1518–2013 undiagnosed cases. These results are summarized in Table 2.
3.2. Municipal-Level Analysis and Geographic Classification
Municipal prevalence varied substantially, ranging from 0.03% (0.27 per 1000 in Positano) to 1.26% (12.61 per 1000 in Salento). Table 3 summarizes the classification of municipalities based on the results of the Poisson test:
- Underdiagnosed (UD): Municipalities with significantly fewer observed cases than expected, p < 0.05 (observed < expected), indicating high hidden burden (e.g., Acerno, Agropoli, and others).
- Hotspots (HS): Municipalities with significantly more observed cases than expected, p < 0.05 (observed > expected), suggesting effective screening or localized outbreaks (e.g., Salento).
- Other (OTH): Municipalities with no significant difference between observed and expected cases, p ≥ 0.05. (e.g., Albanella, Atrani, and others).
The application of Bayesian smoothing refined prevalence estimates by stabilizing values through the incorporation of a prior rate. Bayesian prevalence ranged from 0.22 per 1000 (Positano) to 8.02 per 1000 (Salento), mirroring the previously described range. Estimates showed little deviation from observed prevalences in the most populated municipalities, while in municipalities with smaller populations and fewer cases, the values were more pronouncedly smoothed.
Figure 1 depicts the observed HCV prevalence and hidden burden in the different municipalities.
3.3. Age-Specific Prevalence and Diagnostic Gaps
Age-stratified analysis (Table 4) revealed increasing prevalence and hidden burden with age (with the highest values in the >56 age group, in which ~25% of the cases have been diagnosed), and with significant underdiagnosis across all groups (p < 0.001):
3.4. Multivariate Predictors of Advanced Liver Disease (F3–F4 Fibrosis)
A multivariable logistic regression model was applied to the full patient cohort (n = 3528) to identify independent predictors of F3–F4 fibrosis, adjusting for age, sex, residential context (urban vs. rural), and HCV genotype. Full results are reported in Table 5.
Age emerged as the strongest predictor of F3–F4 fibrosis, with a stepwise increase in risk:
- Patients aged ≥56 years had more than fourfold increased odds compared to those aged 0–29 years, OR = 4.50; 95% CI: 2.14–10.6; p <0.001.
- Those aged 46–56 years had an OR of 2.93 (95% CI: 1.38–6.95; p = 0.008).
- Those aged 30–45 years had an OR of 1.28 (95% CI: 0.590–3.07; p = 0.56).
Notably, urban residence was associated with higher likelihood of being diagnosed with advanced fibrosis or cirrhosis compared to rural areas (OR = 1.29; 95% CI: 1.05–1.58; p = 0.01), as well as infection by genotype 1b (OR = 1.56; 95% CI: 1.35–1.80; p < 0.001) and male sex (OR = 1.63; 95% CI: 1.42–1.89; p < 0.001).
3.5. Temporal Analysis
The temporal analysis (Table 6) documented a reduction in the number of observed and linked-to-care cases between the two periods considered, in line with regional and national reports, with a lower reduction in the burden in the 2019–2022 period compared to 2015–2018 (of 24.6% and 30.0% respectively). In parallel, there was a change in patient characteristics, with a decrease in the mean age and in the percentage of patients presenting for treatment with F3–F4 fibrosis, likely due to the expansion of treatment criteria. Conversely, there was no significant difference in the percentage of patients from the two different settings (urban vs. rural) across the two time periods.
4. Discussion
Despite the widespread availability of the DAAs, HCV infection continues to represent a silent yet persistent public health challenge in Italy and worldwide. A substantial proportion of the disease burden remains unseen due to the significant number of undiagnosed individuals, particularly among older adults and residents of geographically or socioeconomically marginalized communities. Against this backdrop, the present study aimed to offer a novel epidemiological analysis, trying to characterize the hidden burden of HCV infection, through the integration of the evaluation of observed and expected prevalence, official demographic data, and a new urban–rural classification system. This was applied to the vast territory of the province of Salerno, in Campania (Southern Italy), a region consistently affected by hepatitis C based on historical data. This framework could provide regional health authorities with a replicable, data-driven tool to guide the strategic allocation of screening and treatment resources, prioritizing specific risk areas, also in other regions. While previous Italian studies have examined national or regional prevalence and associated risk factors [20,28,34,35], none have achieved the level of spatial and demographic resolution or examined the hidden burden and differences between urban and rural areas. We also calculated Bayesian prevalence to improve estimate accuracy, especially by smoothing values in municipalities with small populations and low case counts.
Our results highlight a significant hidden burden of active HCV infection in the territory of Salerno (approximately 4000 people), with a complex relationship between urban and rural areas: urban areas show a higher number of cases and hidden burden in absolute terms, explained by the higher number of residents, despite a lower prevalence of estimated undiagnosed cases compared to rural areas. Our urban–rural classification system allowed quantification of such disparities that were previously invisible in aggregated regional data. This disparity is likely attributable to factors such as a lack of healthcare infrastructure, less frequent use of diagnostic tools, and longer travel distances to services in rural areas. It could also be due to a different distribution of risk factors in the two different settings, such as a historically greater injecting drug use (IDU) in urban areas. In addition to the comparison of undiagnosed/untreated cases, this subdivision reveals other relevant aspects. For instance, our data indicate that individuals in urban areas were more frequently diagnosed with more advanced liver disease (F3–F4 fibrosis). This may reflect greater disease awareness and access to diagnostic services, resulting in greater detection of advanced disease compared to rural areas, potentially, on the other hand, at greater risk of diagnostic delays. Alternatively, the influence of favorable environmental and sociocultural factors that delay clinical manifestation could intervene, linking the increased burden of more severe liver disease also to environmental stressors, known to adversely affect hepatic and immune functions. In fact, it is known that longevity in Cilento, a large area in the central–southern part of the Province of Salerno, is associated with favorable environmental factors [36,37,38], which could contribute to improved immune-metabolic resilience and lower systemic and liver inflammation. This could translate into a lower prevalence of metabolic dysfunction-associated steatotic liver disease (MASLD) and its associated cardiometabolic risk factors (like obesity and diabetes) in some areas of this region, thereby potentially slowing or reducing HCV-related fibrogenesis [39,40]. The different prevalence of MASLD between rural/urban contexts due to different lifestyles, contributing to a different manifestation of HCV-related disease and translating into fewer cases of advanced fibrosis or cirrhosis in the rural areas of Cilento, remains a hypothesis to be confirmed in further studies. However, this interpretation is coherent with prior research in longevity zones like Cilento, where protective environmental factors (including lifestyle) may delay the progression or expression of chronic diseases [41,42]. While speculative, this perspective aligns with our findings, and it cannot be excluded that both biological protection and diagnostic vulnerability coexist, though further research is needed to substantiate these claims.
Regarding age, beyond documenting more HCV-infected, linked-to-care individuals in older age groups, our study additionally highlights an age-dependent rise in hidden hepatitis C infections. When considered alongside recent projects from northern and southern Italy, these results underscore the imperative to broaden free HCV screening eligibility to older people, coupled with greater involvement of GPs and non-liver specialists (e.g., through opportunistic screening), a measure that aligns with appeals from the Italian hepatological community to the government [11,29,43,44,45]. By limiting it to the 1969–1989 birth cohort (the age group in which free screening is currently provided in Italy in the general population setting), we are currently missing crucial opportunities for early detection and intervention. In fact, older age is generally associated with a longer disease duration, which is linked to a higher risk of advanced fibrosis. This is well-documented in the literature and further corroborated by the association we found in our cohort among older age, genotype 1b (the most common genotype in the general population in Italy), and more severe liver disease [11].
Data analysis between two distinct timeframes, 2015–2018 and 2019–2022, enabled an examination of temporal trends in the number of patients and their characteristics. The reduction in the number of observed, linked-to-care cases between the two periods aligns with the declining trend registered both in Italy and globally [3,46], and is associated with a smaller decline in hidden burden in the later period. Concurrently, the reduction in the mean age and the proportion of patients presenting for treatment with F3–F4 fibrosis can be linked to the broadening of treatment eligibility criteria. This latter finding is consistent with nationwide trends; however, over the years following the expansion of the criteria (introduced in 2017), there was not a significant decline in late diagnoses and treatment start, which again underscores the need for sustained interventions [11,47].
Taken together, our results demonstrate the potential of a municipality-level approach to generate precision public health insights. By integrating epidemiological modeling with demographic and spatial data, our study highlights both the determinants of underdiagnosis and the ecological contexts in which they occur, potentially providing a replicable and policy-relevant model to support precision public health strategies. These could involve establishing new prescribing centers in underserved areas or empowering local GPs or non-liver specialists to manage hepatitis C, guided by liver specialists (task-sharing), as is already the case in some countries on track for elimination. This guidance could potentially be provided through telemedicine (like the Extension for Community Healthcare Outcomes, ECHO, model). Alternatively, time-limited screening campaigns, also utilizing temporary facilities or mobile units—like efforts previously conducted in Egypt—could expand our capacity to identify and treat patients [2,48,49].
This study has several limitations. The analysis focuses on patients diagnosed and treated at specialized centers in the province of Salerno, reflecting linked-to-care cases rather than the full prevalence of active infection, which, aligns with our aim to estimate the hidden burden, however. Moreover, the expected prevalence used to calculate this burden (approximately 4000 subjects) is itself an estimate and therefore inherently uncertain. The municipal-level analysis provides population-level insights, and while it is ecological in nature, caution is advised when applying findings to individual risks. The cumulative approach, combining eight years of data, was a necessary methodological choice to ensure statistical stability and reliable estimates at the municipal level, particularly for small populations. The addition of a temporal analysis comparing two periods (2015–2018 vs. 2019–2022) partially mitigates this by revealing trends in burden and patient characteristics, such as changes in age and disease stage at presentation. However, this temporal assessment is constrained by its broad time intervals, which may obscure shorter-term fluctuations or local variations, limiting its ability to capture dynamic changes fully. Further refinements, such as hierarchical Poisson regression or geostatistical models, could enhance the integration of temporal trends, improve uncertainty quantification, and integrate contextual covariates like socioeconomic indicators or healthcare accessibility, offering a more nuanced understanding of the hidden burden. Lastly, our study does not directly account for high-risk populations such as PWID, MSM, incarcerated individuals, and homeless people, whose distribution is uneven and likely concentrated in urban areas. Due to the absence of reliable, municipal-level epidemiological data for these groups in Italy, our estimates were based primarily on age structure and urban–rural classification. Future adaptations of the model could benefit from integrating data from addiction centers, prisons, or other at-risk contexts, thereby refining its capacity to guide precision public health interventions in both urban and rural settings.
5. Conclusions
In conclusion, we observed differences in HCV care and estimated hidden burden across the vast territory of the province of Salerno, with a complex relationship between rural and urban contexts. Through the model we applied, and that can be replicated in other areas and for other diseases, we documented a more than double prevalence of HCV hidden burden in rural areas compared to urban ones, with the latter, conversely, being characterized by a greater probability of diagnosis of advanced fibrosis or cirrhosis. By prioritizing municipalities with the highest diagnostic gaps and adapting interventions to local contexts based on our approach, a transition from broad, non-targeted strategies to precision public health can be implemented. From a policy perspective, we recommend prioritizing underdiagnosed municipalities for immediate, targeted interventions, which may include increased GP-led opportunistic testing, task-sharing models supported by specialist oversight (also based on telemedicine), the involvement of mobile screening units, and time-limited outreach campaigns. These should occur alongside improved data linkages to addiction, correctional, and harm-reduction services. These measures, coupled with periodic reassessment using the proposed framework, could increase case-finding efficiency and accelerate progress toward national and WHO elimination targets.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Hepatitis C-Fact Sheets Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c(accessed on 29 August 2024)
- 2Torre P. Festa M. Sarcina T. Masarone M. Persico M. Elimination of HCV Infection: Recent Epidemiological Findings, Barriers, and Strategies for the Coming Years Viruses 202416179210.3390/v 1611179239599906 PMC 11598908 · doi ↗ · pubmed ↗
- 3Blach S. Terrault N.A. Tacke F. Gamkrelidze I. Craxi A. Tanaka J. Waked I. Dore G.J. Abbas Z. Abdallah A.R. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: A modelling study Lancet Gastroenterol. Hepatol.2022739641510.1016/S 2468-1253(21)00472-635180382 · doi ↗ · pubmed ↗
- 4Heath K. Hill A. WHO hepatitis C elimination targets: The global equity challenge Lancet Gastroenterol. Hepatol.2024928628810.1016/S 2468-1253(23)00408-938367625 · doi ↗ · pubmed ↗
- 5WHO Global health sector strategy on viral hepatitis 2016–2021 Towards Ending Viral Hepatitis World Health Organization Geneva, Switzerland 2016
- 6Thomadakis C. Gountas I. Duffell E. Gountas K. Bluemel B. Seyler T. Pericoli F.M. Kászoni-Rückerl I. El-Khatib Z. Busch M. Prevalence of chronic HCV infection in EU/EEA countries in 2019 using multiparameter evidence synthesis Lancet Reg. Health–Eur.20243610079210.1016/j.lanepe.2023.10079238188273 PMC 10769889 · doi ↗ · pubmed ↗
- 7The CDA Foundation Hepatitis C Available online: https://cdafound.org/polaris/elimination-maps/(accessed on 19 September 2025)
- 8Ridefinizione dei Criteri di Trattamento Per la Terapia Dell’Epatite C Cronica Available online: https://www.aifa.gov.it/sites/default/files/Determina_n._500-2017_Epatite-C.pdf(accessed on 12 May 2023)