Safety Evaluation of Tetanus, Diphtheria, and Acellular Pertussis Vaccine (Tdap) During Pregnancy Among Vietnamese Women
Hien Minh Nguyen, Nhat Thang Tran, Quoc Huy Pham, Huu Nghia Cao

TL;DR
A study in Vietnam found that the Tdap vaccine is generally safe for pregnant women, with most side effects being mild and not affecting maternal health.
Contribution
This is the first large-scale study in Vietnam evaluating the safety of Tdap vaccination during pregnancy.
Findings
Tdap vaccination during pregnancy was associated with a 49.8% rate of adverse events, primarily mild local reactions.
Co-administration of Tdap with IIV4 did not increase adverse event risk.
No adverse effects on pre-existing maternal conditions were observed.
Abstract
Background: In Vietnam, the Ministry of Health recently approved the use of Tdap vaccines—Boostrix (2022) and Adacel (2024)—for administration during pregnancy, aiming to provide passive antibody transfer to protect newborns against pertussis and tetanus from birth. However, uptake remains low, largely because Tdap is not included in the National Expanded Program on Immunization, vaccine hesitancy persists among obstetricians, and local safety data in pregnancy are limited. Methods: We conducted a prospective cohort study from September 2023 to September 2024 involving 485 pregnant women between 27 and 36 weeks of gestation at two major hospitals in Ho Chi Minh City: University Medical Center and Gia Dinh People’s Hospital. Participants received either Tdap or monovalent tetanus toxoid vaccine (TT) as a comparator. Results: Among women in the Tdap group, 49.8% reported at least one…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
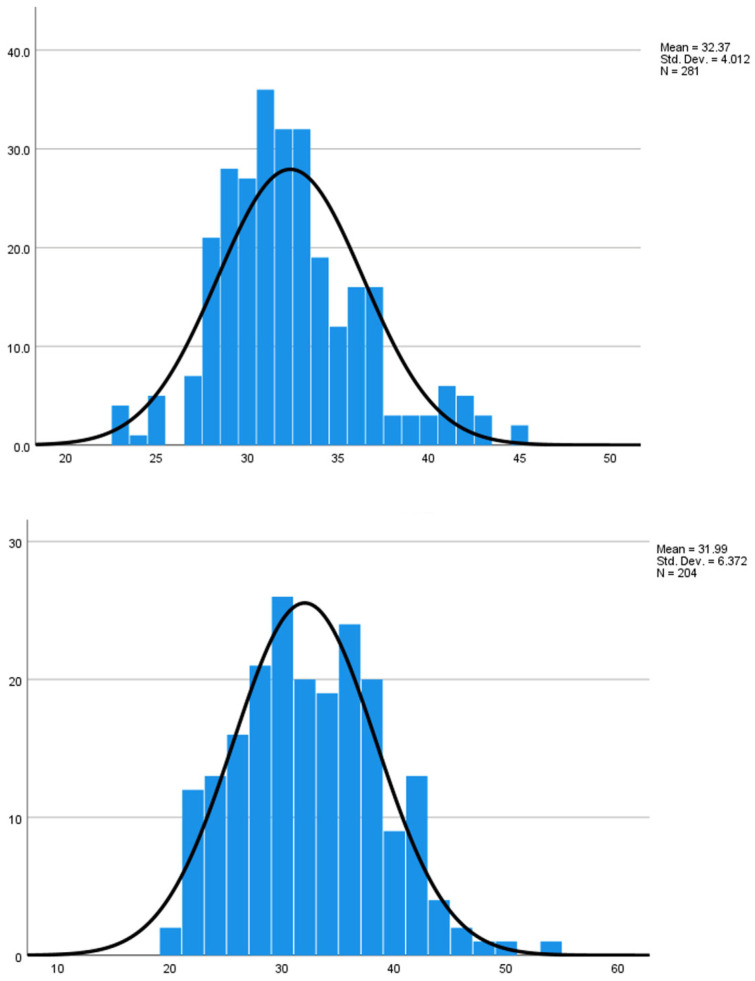 Figure 1
Figure 1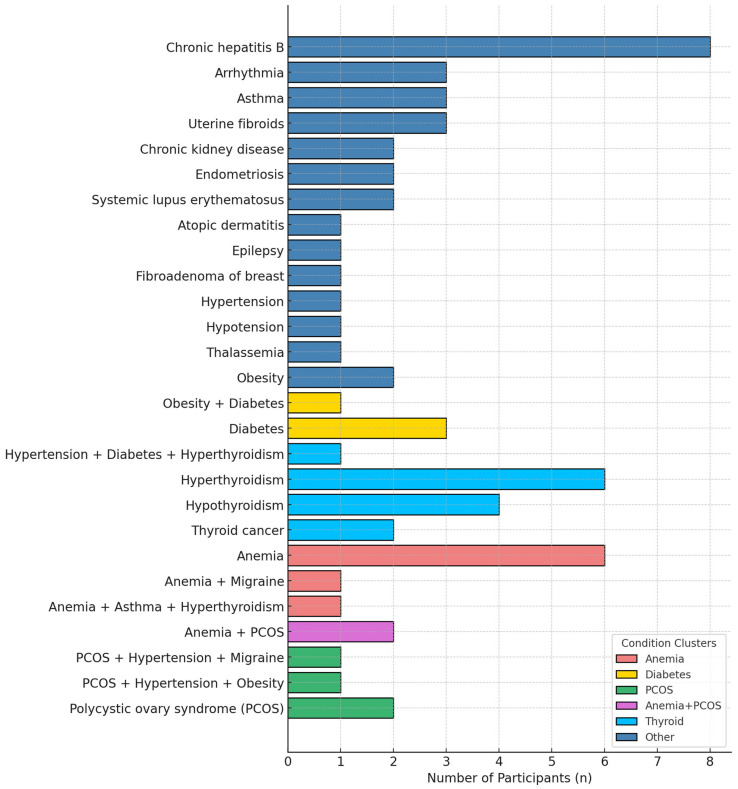 Figure 2
Figure 2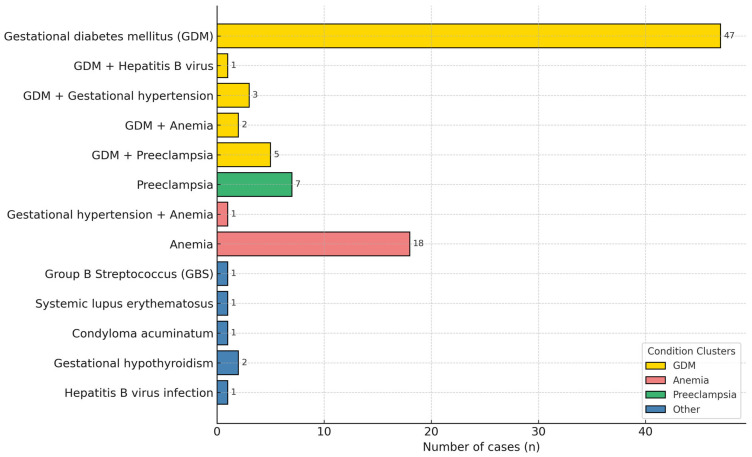 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Vaccine Coverage and Hesitancy · Influenza Virus Research Studies
1. Introduction
Pertussis, commonly known as whooping cough, has re-emerged as a significant global public health challenge. According to data from the World Health Organization (WHO), there were 158,910 reported cases of pertussis globally [1] in 2023. While the number of cases has fluctuated over the years, the recent widespread outbreaks underscore the continued threat posed by the disease. The WHO’s 2018 data indicates that pertussis was responsible for approximately 161,000 deaths worldwide [1], with the majority occurring in children under five years of age. Of particular concern is the rise in pertussis cases among infants under 3 months of age, a population especially vulnerable due to incomplete immunization [2].
In Vietnam, pertussis vaccination coverage among children under 1 year of age has been consistently maintained at over 85% for many years [3,4]. As a result, the incidence of pertussis in children declined from 84.4 per 100,000 population in 1984 to only 0.46 per 100,000 in 2004 [4]. However, during the past five years (2015–2020), this rate has shown a slight upward trend, reaching 0.7–1.06 per 100,000 population [4]. The COVID-19 pandemic resulted in vaccine shortages in Vietnam from 2021 to 2023, during which the DTP3 coverage rate fell to 65% [3]. Among hospitalized pertussis cases under 5 years old, about 64% occurred in infants younger than three months [5]. Since 2020, the Vietnam Association of Preventive Medicine has recommended the administration of one dose of reduced-dose tetanus, diphtheria, and acellular pertussis vaccine (Tdap) for pregnant women between 27 and 36 weeks of gestation during each pregnancy. In 2021, the Vietnam Association of Obstetrics and Gynecology issued a similar recommendation, further emphasizing both the role and legal basis for efforts to incorporate Tdap vaccination into the national immunization program.
In Vietnam, evidence on the immunogenicity of the Tdap vaccine remains limited [6,7], and no large-scale safety studies in pregnant women have been reported to date. In line with updated global recommendations for maternal Tdap immunization and the national context, a prospective study was conducted at the University Medical Center Ho Chi Minh City and Gia Dinh People’s Hospital between September 2023 and September 2024. The primary objective was to evaluate the safety profile of Tdap vaccination during pregnancy. Specifically, the study aimed to (1) assess the clinical course of underlying maternal conditions before and after Tdap administration and (2) examine local and systemic adverse events following vaccination. We hypothesized that Tdap vaccination during pregnancy is safe and shows no difference in safety compared with tetanus toxoid (TT), which has been used in Vietnamese pregnant women for over 30 years and remains well tolerated when co-administered with the influenza vaccine.
2. Materials and Methods
2.1. Study Design
A prospective cohort study was conducted.
2.2. Study Population
Participants were pregnant women residing in Ho Chi Minh City who received the reduced-dose tetanus, diphtheria, and acellular pertussis vaccine (Tdap; Boostrix^®^, GlaxoSmithKline, Rixensart, Belgium). The comparator vaccine was monovalent tetanus toxoid (TT; adsorbed tetanus vaccine, Institute of Vaccines and Medical Biologicals IVAC, Nha Trang, Vietnam). For concomitant vaccination, the inactivated quadrivalent influenza vaccine (Influvac Tetra^®^, Abbott, Weesp, The Netherlands) was administered together with Tdap.
2.3. Study Setting and Duration
The study took place at the Vaccination Unit of the University Medical Center Ho Chi Minh City and the Obstetrics Department of Gia Dinh People’s Hospital from September 2023 to September 2024.
2.4. Inclusion Criteria
Eligible participants were pregnant women aged 18 years or older who provided written informed consent to participate in the study.
2.5. Exclusion Criteria
Participants were excluded if they failed to complete the questionnaire, had a known hypersensitivity to vaccine components, or had a history of severe adverse events following vaccination with diphtheria-, pertussis-, or tetanus-containing vaccines.
2.6. Sample Size
The required sample size was calculated using the formula for estimating a proportion:
The sample size (N) was estimated using the single-proportion formula, with Z = 1.96 (95% confidence), d = 0.05, and α = 0.05. Based on p = 23.9% from the study by Vera Lúcia Gattás [8], the minimum required sample size was N ≥ 280.
2.7. Statistical Analysis
Data entry was performed using Microsoft Excel 365, and statistical analyses were conducted with JASP software version 0.18.0.0 (JASP Team, Amsterdam, The Netherlands). A significance level of 0.05 was applied for all analyses.
2.8. Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board of the University of Medicine and Pharmacy at Ho Chi Minh City (approval No. 579/HĐĐĐ-ĐHYD, dated 22 March 2023) and the Ethics Committee of Gia Dinh People’s Hospital (approval No. 92/NDGĐ-HĐĐĐ, dated 10 August 2023).
2.9. Data Collection Methods
All eligible pregnant women completed a structured questionnaire and were randomly assigned to either the tetanus toxoid (TT) or Tdap group. Participant lists were verified against hospital records for accurate age selection. Enrollment was conducted after informed consent.
Data were collected from vaccination through delivery and until infants reached two months of age. Adverse events following immunization (AEFI) were monitored using passive methods (telephone calls, email questionnaires) and active methods (home or hospital visits). Infant outcomes were documented from delivery and vaccination records.
Outcomes were classified into two categories: local reactions (pain, redness, swelling/induration) and systemic reactions (fatigue, fever, anorexia, nausea/vomiting, rash, dizziness, headache). Data were obtained through self-report, direct observation, and clinical records. Redness and swelling were measured by diameter, pain was assessed by its impact on movement, and systemic events were evaluated by symptom frequency, temperature measurement, or interference with daily activities.
All adverse events were graded on a 0–3 severity scale: Grade 0 = absent; Grade 1 = mild, no impact on daily activity; Grade 2 = moderate, some limitation; Grade 3 = severe, marked limitation requiring medical care or hospitalization.
3. Results
3.1. Demographic Characteristics of Pregnant Participants
The upper panel shows the age distribution of pregnant women receiving Tdap (n = 281; mean age = 32.37 years). The lower panel shows the age distribution of pregnant women receiving tetanus toxoid (TT) (n = 204; mean age = 31.99 years), which is comparable to the Tdap group (Table 1 and Figure 1).
3.2. Maternal Comorbidities Before and During Pregnancy
3.2.1. Pre-Existing Conditions
At enrollment, 64 of 281 pregnant women (22.8%) in the Tdap group presented with underlying comorbidities. Among these 64 women, the most prevalent conditions were thyroid disorders (21.9%; including hyperthyroidism, hypothyroidism, and thyroid cancer), anemia (15.6%), and chronic hepatitis B (12.5%). Diabetes accounted for 6.3%, while polycystic ovary syndrome (PCOS), obesity, and hypertension each accounted for 4.7%. All pre-existing conditions remained clinically stable throughout pregnancy, with no evidence of worsening following vaccination (Figure 2).
3.2.2. Pregnancy-Related Conditions
Of the 281 pregnant women who received Tdap, 90 (32.0%) were diagnosed with pregnancy-related conditions, 80% of which had been identified before Tdap administration. Among these 90 women, gestational diabetes mellitus (GDM) was the most prevalent (64.4%), followed by anemia (23.3%) and preeclampsia (13.3%). These percentages reflect the overall prevalence of each condition, including both isolated and coexisting cases. No severe progression or adverse fetal outcomes were observed in association with vaccination (Figure 3).
3.3. Description of Adverse Event Following Immunization (AEFI) Following Tdap Vaccination
Among 281 pregnant women who received the Tdap vaccine, local adverse events (AEs) were the most frequently reported, with pain at the injection site observed in 43.8% of participants, followed by erythema (3.9%) and swelling (3.9%) (Table 2). The majority of pain cases were graded as mild (Grade 1, 23.5%) or moderate (Grade 2, 17.8%), while only a small proportion were severe (Grade 3, 2.5%).
Regarding systemic AEs, the most common reactions were fatigue (12.8%) and headache (3.9%), while fever (1.1%), dizziness (1.1%), and loss of appetite (2.1%) were infrequent (Table 3). All reported systemic events were self-limited and resolved without medical treatment.
A comparative analysis between women receiving Tdap and those receiving tetanus toxoid (TT) (n = 485) showed that the overall distribution of local and systemic AEs was similar between the two groups (Table 4). However, injection-site pain occurred significantly more often in the Tdap group compared to the TT group (43.8% vs. 26.8%, p = 0.008). No significant differences were observed for erythema, swelling, or systemic events such as fatigue, fever, dizziness, or headache (all p > 0.05).
Statistical analysis indicated that pregnant women who received Tdap had more than five-fold higher odds of experiencing grade 3 adverse events compared with those who received tetanus toxoid (TT) (OR = 5.30, 95% CI: 1.19–23.56, p = 0.018). However, this odds ratio represents relative odds rather than absolute risk, and the absolute number of grade 3 events was low in both groups, indicating that the clinical significance of this finding is likely limited. Importantly, this difference was mainly attributable to mild local pain at the injection site, with no serious or unexpected events reported (Table 5).
AEFIs were generally more frequent in the Tdap + IIV4 group compared with Tdap alone, particularly for local reactions such as pain, erythema, swelling, and headache. However, no significant differences in the frequency of local or systemic adverse events were observed between women who received Tdap alone and those who received concomitant Tdap plus inactivated quadrivalent influenza vaccine (IIV4) (Table 6).
4. Discussion
In Vietnam, maternal immunization has for decades relied almost exclusively on tetanus toxoid (TT), widely administered in maternity care settings [9]. This long-standing practice has shaped both provider habits and maternal expectations, making the shift to Tdap far from straightforward. A knowledge, attitudes, and practices (KAP) survey at University Medical Center Ho Chi Minh City (UMC) showed that provider hesitation and maternal misconceptions remain major obstacles. While 71% of pregnant women expressed willingness to receive Tdap, over half held inaccurate beliefs about its potential harm to the mother or fetus [10]. Although Tdap was officially licensed for use in pregnancy in 2022, it has not yet been included in the national Expanded Program on Immunization (EPI). As a result, it is only available as a self-paid service, whereas TT remains the sole vaccine mandated for pregnant women under current regulations (Vietnam Ministry of Health Circular No. 10, 2024) [3,5,11]. In addition, many obstetricians remain hesitant to recommend Tdap over TT, citing concerns that such changes may be difficult to communicate to pregnant women, who might perceive deviations from traditional practice as potential risks to maternal and infant health. Similar barriers in the United States—limited access, provider hesitancy, and maternal safety concerns—were reported when Tdap was first introduced during pregnancy [10,12].
The first Tdap doses administered to pregnant women in Vietnam were conducted at the UMC during the COVID-19 pandemic [13]. Tdap vaccination has demonstrated a favorable safety profile within 7 days post-administration in pregnant women between 27 and 36 weeks of gestation, even when co-administered with the COVID-19 vaccine or the influenza vaccine (IIV4). In our previous small-scale study conducted at University Medical Center Ho Chi Minh City in 2021, which evaluated the co-administration of Tdap and COVID-19 vaccines in 78 pregnant women, adverse events following immunization (AEFIs) were mostly mild and self-limiting, and no serious vaccine-related events were reported [13]. Among systemic AEs, fatigue was the most frequently reported (28.2%), followed by fever (10.3%). Local AEs primarily included pain at the injection site (66.7%), with redness and/or swelling observed in 14.1% of participants and itching in 9%. These results are consistent with our subsequent observational data on concomitant Tdap and IIV4 administration, which also showed predominantly mild and self-limited AEs (Table 6). As the safety of maternal immunization is a primary concern, it is also important to address the safety of co-administration with other vaccines to build confidence and acceptance in vaccination programs. This information is essential to inform and support the development of future maternal influenza immunization policies in Vietnam. Our findings on Tdap vaccination (Table 2 and 3) are broadly consistent with studies conducted in Asian pregnant populations, which also reported predominantly mild AEFIs and no new safety concerns [14,15,16]. Our prospective cohort adds important evidence that Tdap is safe for Vietnamese pregnant women, showing an adverse event profile comparable to tetanus toxoid (Table 4). Building this local safety evidence is a crucial first step toward gaining the trust of both pregnant women and obstetricians, which is essential for broader acceptance in Vietnam. Once this confidence is established, national policy updates to replace TT with Tdap can be implemented more effectively to better protect both mothers and their infants.
In addition, most Vietnamese pregnant women have little or no prior experience with influenza vaccination, as influenza immunization has not been routinely recommended during pregnancy. This unfamiliarity can reinforce hesitancy when Tdap and influenza vaccines are offered together. However, our study demonstrated that co-administration of Tdap and inactivated quadrivalent influenza vaccine (IIV4) was safe, with no increase in adverse events compared with Tdap alone. This reassurance is consistent with findings from other high-income country studies [17,18]. Together, these data align with World Health Organization recommendations endorsing both Tdap and influenza vaccines during pregnancy [19,20] to enhance maternal and neonatal protection.
5. Conclusions
This study shows that Tdap vaccination is safe for Vietnamese pregnant women, including those with comorbidities or pregnancy-related conditions, with an adverse event profile comparable to tetanus toxoid (TT). Co-administration with the influenza vaccine (IIV4) was also well tolerated. These findings support our hypothesis and provide essential national evidence to guide future maternal immunization policies in Vietnam, including the integration of co-administration strategies into the Expanded Program on Immunization (EPI).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO) Pertussis—Number of Reported Cases Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/pertussis-number-of-reported-cases(accessed on 5 July 2025)
- 2Leontari K. Lianou A. Tsantes A.G. Filippatos F. Iliodromiti Z. Boutsikou T. Paliatsou S. Chaldoupis A.E. Ioannou P. Mpakosi A. Pertussis in early infancy: Diagnostic challenges, disease burden, and public health implications amidst the 2024 resurgence, with emphasis on maternal vaccination strategies Vaccines 20251327610.3390/vaccines 1303027640266155 PMC 11945951 · doi ↗ · pubmed ↗
- 3Nguyen P.N.T. Heininger U. Muloiwa R. von König C.H.W. Hozbor D. Ong-Lim A. Tan T.Q. Forsyth K. Pertussis in southeast asia: Country-level burden and recommendations from the global pertussis initiative IJID Reg.20251410055910.1016/j.ijregi.2024.10055939906191 PMC 11791295 · doi ↗ · pubmed ↗
- 4Hai D.T. Tổng quan chẩn đoán và điều trị bệnh ho gàVietnam. J. Pediatr.202141010.52724/tcnk.v 14i 1.12 · doi ↗
- 5Pham N.T. Bui Q.T. Tran D.M. Larsson M. Pham M.P. Olson L. Pertussis seasonal variation in northern vietnam: The evidence from a tertiary hospital BMC Public Health 20242428610.1186/s 12889-024-17705-938267959 PMC 10809638 · doi ↗ · pubmed ↗
- 6Hoang H.T. Leuridan E. Maertens K. Nguyen T.D. Hens N. Vu N.H. CaboréR.N. Duong H.T. Huygen K. Van Damme P. Pertussis vaccination during pregnancy in vietnam: Results of a randomized controlled trial pertussis vaccination during pregnancy Vaccine 20163415115910.1016/j.vaccine.2015.10.09826529073 · doi ↗ · pubmed ↗
- 7Maertens K. Hoang T.T. Nguyen T.D. CaboréR.N. Duong T.H. Huygen K. Hens N. Van Damme P. Dang D.A. Leuridan E. The effect of maternal pertussis immunization on infant vaccine responses to a booster pertussis-containing vaccine in vietnam Clin. Infect. Dis.201663 S 197S 20410.1093/cid/ciw 55127838673 PMC 5106623 · doi ↗ · pubmed ↗
- 8Gattás V.L. Luna E.J.A. Sato A.P.S. Fernandes E.G. Vaz-de-Lima L.R.A. Sato H.K. Castilho E.A. Adverse event occurrence following use of tetanus, diphtheria and acellular pertussis adsorbed vaccine-tdap-, são paulo, sp, brazil, 2015–2016. (Ocorrência de eventos adversos após o uso da vacina adsorvida difteria, tétano e pertussis (acelular)-d Tpa-, São Paulo, SP, 2015–2016)Epidemiol. Serv. Saude 202029 e 201928010.5123/s 1679-4974202000020002732401912 · doi ↗ · pubmed ↗