Early Childhood Exposure to Endocrine Disrupting and Neurotoxic Chemicals: Associations with Internalizing and Externalizing Difficulties from Childhood to Adolescence in the Rhea Cohort, Crete, Greece
Chrysi Mouatsou, Katerina Margetaki, Mariza Kampouri, Marianna Karachaliou, Antonis Myridakis, Danae Costopoulou, Leondios Leondiadis, Euripides G. Stephanou, Lida Chatzi, Manolis Kogevinas, Katerina Koutra

TL;DR
Early exposure to certain chemicals in childhood may lead to emotional and behavioral issues in girls later in life.
Contribution
This study identifies specific chemicals linked to long-term behavioral outcomes in girls from childhood to adolescence.
Findings
Exposure to HCB and DDE in early childhood was associated with increased externalizing symptoms in girls over time.
Low molecular weight phthalates were linked to internalizing, externalizing, and ADHD symptoms in girls.
Organophosphate pesticide exposure was associated with increased externalizing and ADHD symptoms.
Abstract
Many common chemicals are known or suspected to harm brain development, and children are particularly vulnerable, yet research on their long-term effects on mental health is limited. This study investigated the associations of early childhood exposure to endocrine disrupting and neurotoxic chemicals with the development of internalizing, externalizing, and attention-deficit/hyperactivity disorder (ADHD) symptoms from early childhood through adolescence in 387 children from the Rhea cohort in Crete, Greece. At age 4, serum concentrations of 3 organochlorine pesticides and 14 polychlorinated biphenyls, and urinary concentrations of 7 phthalate metabolites and 6 dialkyl phosphate metabolites were measured. Children’s symptoms were assessed via maternal reports at ages 4, 6, 11 and 15 years. Using generalized estimating equation models, the study found that early exposure to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
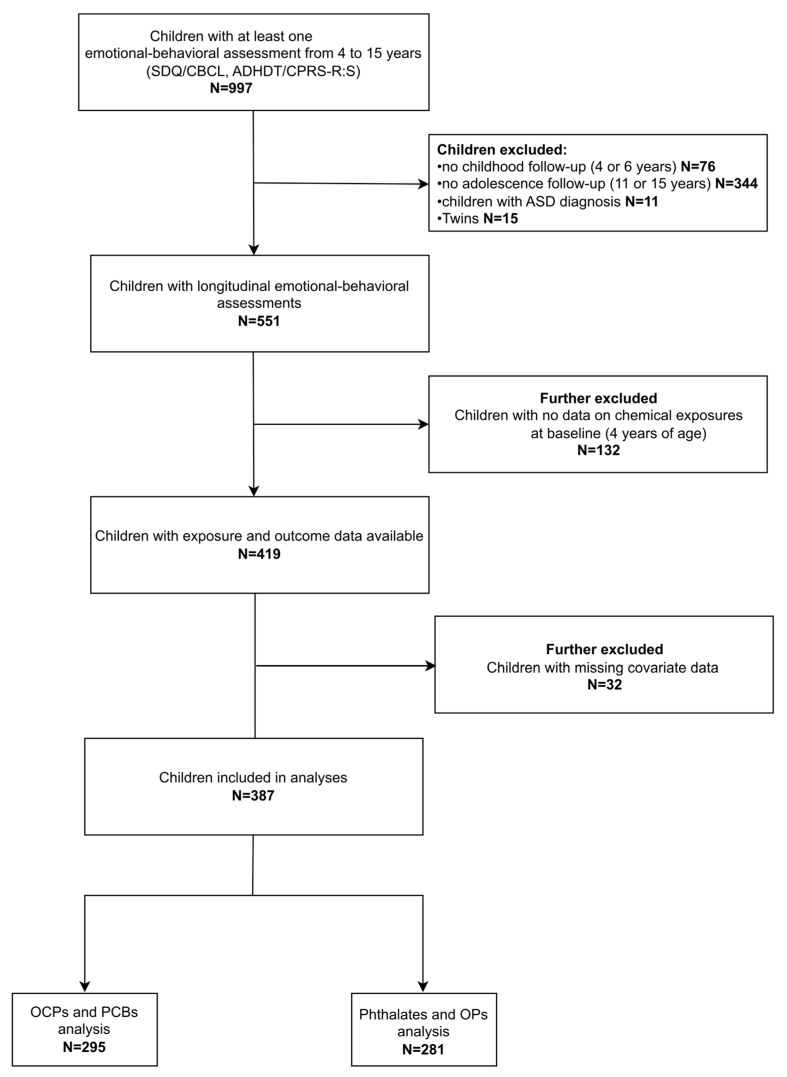 Figure 1
Figure 1- —European projects
- —Greek Ministry of Health
- —Hellenic Ministry of Health
- —General Secretariat for Research and Innovation
- —Hellenic Foundation for Research and Innovation (H.F.R.I.)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth, Environment, Cognitive Aging · Early Childhood Education and Development · Effects and risks of endocrine disrupting chemicals
1. Introduction
Emotional and behavioral disorders, as well as neurodevelopmental disorders, such as Attention-Deficit/Hyperactivity Disorder (ADHD), are prevalent among children and adolescents [1,2]. These disorders are linked to adverse outcomes, including low academic performance [3], increased risk of substance use [4], and higher unemployment rates [5]. Furthermore, experiencing elevated symptoms during childhood and adolescence is associated with an increased likelihood of these disorders continuing into adulthood [6,7].
The etiology of these disorders is considered multifactorial and research has indicated potential connections of chemical exposure with neurodevelopmental impairments, behavioral deficits, and increased risk of ADHD [8,9,10]. Children are more susceptible to the effects of environmental chemicals than adults, making them particularly vulnerable to these adverse outcomes [11]. This heightened susceptibility is attributed to several factors, including the complexity of brain development [12] and the immaturity of detoxification mechanisms [13]. Furthermore, children have a higher relative exposure to environmental chemicals as they consume more food, water, and air relative to their body weight in comparison to adults [14]. Additionally, behaviors such as hand-to-mouth activities further elevate exposure [15]. Disruption of neurodevelopment due to environmental insults during this critical period can lead to irreversible and long-lasting effects, increasing the risk for developing various pathologies across the lifespan [16,17].
Research on postnatal exposure to persistent organic pollutants, such as organochlorine pesticides (OCPs) and polychlorinated biphenyls (PCBs), is less extensive than studies on fetal exposure, with most focusing on early postnatal periods. These studies have produced inconsistent results, particularly when examining the first 12 to 24 months of life [18,19,20,21], and findings on exposure later in childhood are also mixed. Some studies suggest associations between PCB exposure and increased emotional symptoms [22,23], while others report inverse associations [24]. Research on phthalates, compounds commonly found in personal care products and plastics [25], has shown positive associations with behavioral problems [26,27], teacher-reported ADHD symptoms [28], attention problems [29], and social difficulties [30], while a study on 7-year-olds from a Polish cohort found no link between exposure at age 2 and internalizing or externalizing problems [31]. Studies on organophosphate pesticides (OPs), primarily sourced from contaminated food, also show mixed results. While some studies link OP exposure to ADHD [32,33] and internalizing symptoms [34], others report null or even inverse associations with behavioral problems [24,35].
The biological mechanisms underlying the effects of these environmental chemicals on brain development are not fully understood, but both animal and human studies suggest that these effects may be sex-specific [36,37]. Most studies evaluating postnatal exposure to persistent organic pollutants have not considered sex as a key factor [21,22], while no significant sex differences have been reported by those that have investigated it [14,18,19]. In contrast, sex-specific effects have been more extensively examined in relation to phthalate and OP exposure, though the findings remain inconsistent. These studies show that the effects can differ between boys and girls depending on the specific chemical metabolite and the neurobehavioral domain assessed [26,29,34,38], while sex differences in the concentrations and metabolism of phthalates have been previously reported in the Rhea cohort [39,40].
Given the rising prevalence of emotional, behavioral and neurodevelopmental disorders [1,2], as well as their potential links to chemical exposures, a deeper understanding of the effects of chemical pollution on mental health is needed. Existing research is limited, often focusing on specific pollutants or developmental stages, with inconsistent findings on the role of sex. In this context, our study aims to investigate childhood exposure (at age 4) to chemicals, including OCPs, PCBs, phthalates, and organophosphate pesticides, in relation to the development of internalizing, externalizing, and ADHD symptoms from early childhood through adolescence (at ages 4, 6, 11, and 15 years), while also assessing potential sex-specific effects.
2. Materials and Methods
2.1. Study Population
The present study utilized data from the Rhea Study, an ongoing population-based mother-child cohort in Crete, Greece. A detailed description of the cohort is available in Chatzi et al. [41]. Briefly, pregnant women were initially approached in four clinics (both public and private) in the city of Heraklion between February 2007 and February 2008. To meet the eligibility criteria, women were required to reside in the prefecture of Heraklion, be over 16 years old, and have a good understanding of the Greek language. A total of 1610 pregnant women were recruited in the Rhea Study around the 12th gestational week, and 1363 singleton pregnancies were followed through delivery. Assessments were conducted twice during pregnancy and at birth admission. Children were evaluated at multiple developmental stages: infancy (approximately 9 and 18 months), early childhood (median 4.2 years), mid-childhood (median 6.5 years), pre-adolescence (around 11 years), and adolescence (15 years).
For the purposes of this research, data from the assessments conducted at ages 4, 6, 11, and 15 years were utilized. In total, 997 children had available data on internalizing, externalizing, or ADHD symptoms for at least one of the four assessments. To capture development across both childhood and adolescence, we set the requirement that each child should have been assessed at least once at ages 4 or 6 and once at ages 11 or 15. Twins (N = 15) and children diagnosed with autism spectrum disorder (N = 11) were not included in the analyses. Data on chemical exposure at the beginning of the trajectory (4 years) were not available for 132 children. Further, 32 children (7.6%) were excluded due to missing covariate information. The final sample consisted of 387 children (Figure 1).
2.2. Exposure Assessment
Blood and urine samples were collected from children at the age of 4 years and analyzed for the following compounds. A list of the chemicals studied is shown in Table 1.
2.2.1. Organochlorine Pesticides and Polychlorinated Biphenyls
Non-fasting < 10 mL blood samples were collected in silicone gel separator vacutainers (Becton Dickinson, Cowley, Oxford, UK) and centrifuged within 2 h at 2500 rpm for 10 min. Then, serum samples were aliquoted and stored at −80 °C until assayed. The analysis was conducted in the Mass Spectrometry and Dioxin Analysis Laboratory (INRASTES, NCSR “Demokritos”) by the isotope dilution method using ^13^C labeled analogs for all compounds. The quantification of the examined compounds (HCB, DDT, DDE, and PCB 105, 114, 118, 123, 156, 157, 167, 189, 28, 52, 101, 138, 153, 180) was performed with High-Resolution Gas Chromatography-High-Resolution Mass Spectrometry (Electron-Impact) in Multiple Ion Detection mode, using previously described methods [42]. The concentrations were expressed in pg/mL serum. Concentrations below the limit of detection (LOD; 0.2 pg/mL for all monitored analytes) were substituted by the value of LOD divided by the square root of 2. OCPs were at detectable levels in every sample, while for PCBs detectability ranged from 55.3% to 100% of the samples. We calculated the total sum of all analyzed PCB congeners as well as the sum of indicator PCBs (28, 52, 101, 138, 153, 180). We adjusted for serum lipid concentrations (cholesterol and triglycerides) as continuous variables in all multivariable models to reduce potential biases from automatic lipid adjustment [43]. Analyses of serum lipid concentrations were conducted using standard enzymatic methods (Medicon Hellas S.A., Athens, Greece) on an automatic Olympus AU5400 high-volume chemistry analyzer (America, Inc., Melville, NY, USA). All chemicals were treated as continuous variables on a log_2_ scale, to account for right-skewness.
2.2.2. Phthalates and Organophosphate Pesticides
Urine samples from children of 4 years of age were analyzed at the Department of Chemistry of the University of Crete. Total levels of seven phthalate metabolites (mEP, mnBP, miBP, mBzP, mEHP, mEHHP, and mEOHP) and six dialkyl phosphate metabolites (DAPs: DEP, DETP, DEDTP, DMP, DMTP, DMDTP) were monitored using previously described analytical protocols [40,44]. The limits of detection (LOD) for the examined phthalate metabolites ranged from 0.01 to 0.84, and for the organophosphate metabolites ranged from 0.02 to 0.24. Measurements below LOD were replaced by the LOD divided by the square root of 2. The percentage of samples with levels above the LOD were high for all phthalate metabolites, ranging from 97.9% to 100%. Regarding organophosphate metabolites, the percentage of samples with concentration levels above the LOD was high for DEP, DETP, and DMTP (91.5–98.9%), but low for DEDTP, DMP, and DMDTP (20.6–46.6%). We calculated the molar sum of DEHP metabolites (mEHP, mEHHP, mEOHP), High Molecular Weight phthalate (mEHP, mEHHP, mEOHP, mBzP), Low Molecular Weight phthalate metabolites (mEP, mnBP, miBP), as well as diethyl phosphate metabolites (DEs: DEP, DETP, DEDTP) and dimethyl phosphate metabolites (DMs: DMP, DMTP, DMDTP) by dividing metabolite concentrations with their molecular weight and summing across. Total DAPs represent the sum of diethyl and dimethyl metabolites and are used as a biomarker of total exposure to OPs [45]. In order to account for urine dilution, metabolite concentrations were divided by urinary creatinine levels, which were determined using the OLYMPUS 2700 immunoassay system (Beckman Coulter, Brea, CA, USA). All creatinine-adjusted metabolite concentrations were log_2_ transformed, due to right-skewed distribution.
2.3. Outcome Assessment
We evaluated children’s internalizing, externalizing, and ADHD symptoms at ages 4, 6, 11, and 15 years using maternal reports.
2.3.1. Internalizing and Externalizing Symptoms
At age 4, mothers completed the Strengths and Difficulties Questionnaire (SDQ) [46], a concise tool that assesses children’s adaptive and maladaptive attributes. The SDQ consists of 25 items rated on a 3-point Likert scale. For the present analyses, two broad scales were used: (a) Internalizing difficulties, which encompasses emotional and peer problems and (b) Externalizing difficulties, which captures conduct problems and hyperactivity. The SDQ has been adapted to the Greek population [47]. In the subsequent follow-ups (ages 6, 11, 15) mothers completed the Child Behavior Checklist-Parent Report Form (CBCL) [48], a widely used instrument composed of 113 items rated on a 3-point Likert scale. For the current study, we utilized two broad-band scales: (a) Internalizing problems, which includes Anxiety/depression, Withdrawal/depression, and Somatic complaints syndrome scales and (b) Externalizing problems, which consists of Rule-breaking behavior and Aggressive behavior syndrome scales. The adaptation of the CBCL for the Greek population has been conducted by Roussos et al. [49]. In all used scales, higher scores reflect more difficulties.
2.3.2. ADHD Symptoms
At age 4, the Attention Deficit Hyperactivity Disorder Test (ADHDT) [50] was filled out by mothers. It is a 36-item psychometric tool designed to evaluate ADHD-related symptoms. The sum of all items represents a total ADHD difficulties index, which was utilized in the present analyses. The ADHDT has been translated and adapted to the Greek population [51]. In subsequent assessments (ages 6, 11, 15 years) mothers reported their children’s ADHD symptoms using the Conners’ Parent Rating Scale-Revised: Short Form (CPRS-R: S) [52]. It is a short version consisting of 27 items rated on 4-point Likert scale. An ADHD index can be derived, with possible scores ranging from 0 to 36 and this index was employed in the current study. The CPRS-R: S was translated and cross-culturally adapted by the Rhea cohort team, according to the established methodology of forward and back-translation, along with pre-testing [53]. For both indices, higher scores indicate greater and more severe ADHD symptoms.
2.4. Statistical Analysis
Descriptive statistics were used to summarize the sample characteristics, the exposures and the outcomes of the study population. Means with standard deviations (SD) and frequencies with percentages were calculated for continuous and categorical variables, respectively. Pearson correlation coefficients were calculated to examine the correlation among chemicals. Sex differences in the distributions of exposures and outcomes were evaluated with the use of Student’s t-test or Mann–Whitney U. The differences between participants and non-participants were assessed via chi-square and t-tests or Mann–Whitney U test. To account for missing data, scale scores were prorated if fewer than 25% of items were missing. Because different instruments were used for outcome assessment at age 4 compared to later timepoints, we converted prorated scale scores to z-scores (Mean = 0, SD = 1) at each timepoint to harmonize the scales. The z-scores were used in all subsequent analyses.
The associations between each chemical exposure and internalizing, externalizing and ADHD symptom z-scores from ages 4 to 15 years were examined using Generalized Estimating Equation (GEE) models with an unstructured correlation matrix. Effect estimates are reported as beta coefficients with 95% confidence intervals (CIs). Various maternal and child characteristics, known or suspected to be linked to environmental exposures and children’s internalizing, externalizing, or ADHD symptoms, were considered potential confounding variables. Our models were adjusted for child sex (male, female), exact child age at outcome assessment (years), maternal age at childbirth (years), maternal education (low: up to 9 years of compulsory schooling, medium: post-secondary education, high: attained a university or technical/college degree), parity (nulliparous, multiparous), log-equivalized disposable household income in tertiles [54], child Body Mass Index (BMI; kg/m^2^) at 4 years, passive smoking at 4 years (never, ever), breastfeeding duration (months) and place of residence (urban, rural). Models for OCPs and PCBs were additionally adjusted for child serum lipids (cholesterol and triglycerides). To evaluate effect modification by child sex, we introduced in each model a multiplicative interaction term between each exposure and sex and then, using these models, we calculated the respective effect estimates for each sex.
Secondary analyses examined potential age-varying effects by including an interaction term between each exposure variable and the child’s age at outcome assessment (4, 6, 11 and 15 years) in the models. Effect estimates for each timepoint and the corresponding p-value for the age interaction were obtained from these models. In a subset of participants, maternal levels of chemicals were available. To evaluate the independent role of postnatal exposure, we adjusted GEE models for maternal levels of chemicals. Specifically, models for child exposure to OCPs and PCBs were adjusted for maternal levels of HCB, DDE, PCBs 118, 138, 153, 156, 170 and 180, and models for child phthalate exposure were adjusted for maternal levels of phthalates (HMW and LMW). Finally, we conducted sensitivity analyses: (a) Excluding children with a diagnosis of learning disability or ADHD (N = 29), and (b) Excluding preterm born children (<37 gestational weeks, N = 48).
The significance level was set at p < 0.05, and for all tests a two-sided alternative hypothesis was used. Statistical analyses were performed with Stata software, version 16.0 (Stata Corp, College Station, TX, USA).
3. Results
3.1. Descriptive Characteristics of the Study Population
The sample characteristics (N = 387) are presented in Table 2. Participating mothers were on average 30.2 years old (±4.7) at the time of childbirth, and the vast majority were Greek (96.1%). Approximately half of the mothers had acquired medium educational level (52.2%), while 38.0% had high level of education. A slightly higher percentage of mothers were multiparous (54.0%) compared to nulliparous (46.0%) mothers. Regarding child characteristics, 55.0% of the children were male and 45.0% were female. The average birthweight was 3204.3 g (±443.9), and the mean gestational age was 38.2 weeks (±1.6). Forty-eight children (12.4%) were born preterm. The median breastfeeding duration was 3 months. Most children (72.9%) lived in urban areas at the age of 4 and 43.4% were exposed to passive smoking. By the age of 15, twenty children (5.2%) had been diagnosed with learning disabilities and nine children (2.3%) with ADHD. No sex differences were observed in socio-demographic characteristics, except for birthweight which was higher among boys (p < 0.001).
Mothers in our sample were more likely to have higher education and household income than non-participating mothers. Children who participated had slightly higher birthweights, were breastfed for longer periods, and were more likely to have attended nursery before age 2. Regarding exposures, children in our sample were exposed to higher levels of DDE and HMW phthalates than non-participants (Table S1).
The concentrations of the examined biomarkers are shown in Table 3. For each chemical class, the highest concentrations were observed for DDE among OCPs, PCB153 among PCBs, mEP among phthalate metabolites, and DMTP among OPs. No significant sex differences were detected in exposure levels, except for miBP, which was found at higher concentrations in females (p = 0.022). Correlations among biomarker concentrations are presented in heatmap form in Figure S1. In brief, significant positive correlations were observed within the same chemical groups, as well as among phthalates and OPs.
With respect to outcome distribution (Table 4), girls exhibited significantly lower levels of emotional symptoms at age 4, but higher levels at age 15 compared to boys. As expected, boys demonstrated higher externalizing symptoms at ages 4, 6, and 11 years, as well as elevated ADHD symptoms across all follow-up assessments.
3.2. Childhood Exposure to Chemicals and Mental Health Symptoms from Childhood to Adolescence
The associations between chemical exposures at 4 years of age and internalizing, externalizing, and ADHD symptoms from early childhood to adolescence, estimated by GEE models, are presented in Table 5. No significant associations were observed when analyzing the overall sample. However, the sex-specific analysis revealed significant results. Specifically, within the class of organochlorines, exposure to HCB and DDE was associated with increased behavioral symptoms across ages in females [beta (95% CI): 0.20 (0.04, 0.37), p-interaction = 0.013 and 0.11 (0.01, 0.21), p-interaction = 0.001, respectively]. Moreover, a significant interaction with sex (p = 0.018) suggested that HCB exposure had opposite effects on ADHD symptoms in boys and girls. However, the effect estimates for each sex did not reach statistical significance. HCB exposure was also associated with decreased internalizing symptoms among boys [beta (95% CI): −0.13 (−0.25, −0.01)], though the interaction with sex was non-significant (p = 0.368). No significant associations were found for PCBs.
Among phthalate metabolites, exposure to LMW phthalates was associated with higher internalizing symptoms in girls [beta (95% CI): 0.15 (0.04, 0.26)], although the interaction with sex was not statistically significant (p = 0.054). Furthermore, LMW phthalate exposure was linked to increased externalizing and ADHD-related difficulties in girls [beta (95% CI): 0.13 (0.01, 0.25) and 0.13 (0.02, 0.24), respectively; p-interaction = 0.030 and 0.008]. For boys, the corresponding effect estimates were close to null for internalizing symptoms and negative, though not significant, for externalizing and ADHD symptoms.
Significant interactions with sex were also observed for OPs in relation to externalizing and ADHD symptoms. In girls, higher concentrations of diethyl (DE), dimethyl (DM), and dialkyl phosphate (DAP) metabolites were associated with elevated behavioral symptoms [beta (95% CI): 0.10 (0.02, 0.17), 0.08 (0.01, 0.16), and 0.13 (0.04, 0.22), respectively; p-interaction = 0.004, 0.019, and 0.003], and increased ADHD-related symptoms [beta (95% CI): 0.08 (0.01, 0.15), 0.09 (0.01, 0.16), and 0.12 (0.04, 0.20), respectively; p-interaction = 0.009, 0.014, and 0.003]. In boys, the corresponding effect estimates were in the opposite direction but did not reach statistical significance.
3.3. Secondary and Sensitivity Analyses
Furthermore, we investigated the age-specific associations between chemical exposures and child symptoms, identifying some time patterns (Table S2). Specifically, significant interactions of PCB exposure with age indicated that the exposure effect on ADHD symptoms was more pronounced at 6 years of age. Conversely, the association between OP exposure and internalizing symptoms was particularly evident at 15 years of age, although age interactions did not reach statistical significance.
In models further adjusted for prenatal exposure (Table S3), analysis of the overall sample showed that HCB exposure was linked to reduced internalizing symptoms [beta (95% CI): −0.10 (−0.19, −0.00)], while DEHP metabolites were related to elevated externalizing difficulties [beta (95% CI): 0.13 (0.01, 0.25)]. In models with sex interaction, no meaningful changes were observed for OCPs. For LMW phthalate exposure, effect estimates were slightly magnified, and significant inverse associations emerged for boys. However, these changes can be attributed to the significant reduction in sample size (approximately 75%) in this analysis.
Sensitivity analyses (Table S4) excluding children diagnosed with learning disabilities or ADHD and prematurely born children did not substantially change our results.
4. Discussion
In this longitudinal study, we explored the association of childhood exposure to a wide range of endocrine disrupting and neurotoxic chemicals with the developmental trajectories of internalizing, externalizing, and ADHD symptoms up to adolescence. Overall, our results revealed sex-specific associations, with the adverse effects of HCB, DDE, phthalates, and OPs on emotional and behavioral development being particularly observed in girls.
4.1. Organochlorine Pesticides
Our findings indicate that exposure to HCB and DDE is associated with increased behavioral symptoms among girls from early childhood through adolescence. A systematic investigation of OCPs revealed that children in the Rhea cohort were exposed to DDT/DDE in utero and through breastfeeding and diet during their early years, with exposure levels found to be higher compared to other countries [14]. Studies on childhood exposure to organochlorines are limited to those estimating exposure using pharmacokinetic models for the first two years of life [18,19,20] producing inconclusive results. In this context, sex differences are seldom explored, and the underlying mechanisms are not completely understood. However, animal studies have reported that DDE can act as antagonist on the androgen receptors [55]. In addition, endosulfan, an organochlorine insecticide similar to DDT, has been reported to decrease dopamine levels in the striatum of males and increase them in females [56]. Alterations in dopaminergic activity are implicated in ADHD [57], while disruption of brain monoamines by organochlorines may contribute to the observed sex-specific behavioral effects [58]. For example, one animal study reported that HCB exposure led to changes in norepinephrine, serotonin and dopamine concentrations, with effects varying by sex, dose, and specific brain region [59].
4.2. Phthalates
Moreover, higher concentrations of LMW phthalate metabolites in urine samples at age 4 years were associated with elevated internalizing, externalizing, and ADHD-related symptoms across development in girls. This finding is consistent with results from a longitudinal study in Cincinnati, USA, which identified more prominent associations between childhood exposure to mEP, a LMW phthalate, and internalizing and externalizing problems in girls [26]. Similarly, a cross-sectional Korean study reported that higher urine concentrations of mnBP were linked to increased thought and attention problems in females, although no sex differences were detected in total scores [29]. Furthermore, Daniel et al. [38] demonstrated that the adverse effects of phthalates differ between boys and girls, depending on the specific metabolite and behavioral aspect, providing further support to the sex-specific nature of these associations. The potential mechanisms through which phthalates exert their effects include the disruption of hormonal homeostasis, particularly of gonadal hormones, which are essential for brain function and sex-specific neurodevelopment [36]. Several phthalates have been shown to exhibit anti-androgenic properties [60] by interfering with aromatase activity, thereby affecting the sexual differentiation of the brain [61]. In addition, phthalates can interfere with thyroid function, with evidence suggesting that this effect is more pronounced in females [62,63]. This mechanism might also explain the sex differences in the behavioral effects of phthalates. However, further research is warranted to better understand the biological pathways underlying the effects of phthalates.
4.3. Organophosphate Pesticides
Finally, our analysis revealed another sex-specific association, with child exposure to OPs being linked to elevated externalizing and ADHD symptoms only among girls. Contaminated food has been identified as the primary source of OP exposure among children in the Rhea cohort [40]. Evidence on the behavioral effects of child pesticide exposure remains inconsistent. While some studies have demonstrated associations with ADHD-related behaviors [32,33] and emotional problems [34], others have found null or inverse associations [24,35]. However, it must be noted that direct comparisons with these studies cannot be made, due to differences in research design (e.g., cross-sectional studies), variations in the timing of exposure and outcome assessment, and in some cases the lack of biomarker-based exposure measurements. Evidence about sex differences is largely inconclusive. The effects of OPs are primarily attributed to acetylcholinesterase inhibition [64], which leads to the synaptic accumulation of acetylcholine, a neurotransmitter with significant role in cell proliferation, migration, and synapse formation [65,66]. Additional biological effects have also been proposed, including impaired glucose homeostasis, altered expression and function of transcription factors involved in cell differentiation and apoptosis, and epigenetic changes [67,68]. These mechanisms, along with the potential disruptions in sex and adrenal hormones caused by pesticides [69], may contribute to the varying effects observed between males and females.
4.4. Strengths and Limitations
This study has several strengths. First, it was conducted within the prospective mother-child Rhea cohort, allowing us to examine the effects of childhood exposure to a wide range of environmental chemicals on developmental trajectories across four timepoints, from early childhood to adolescence. Second, we used biomarkers for exposure assessment, providing a direct and reliable measure of exposure to all investigated chemicals, including organochlorine pesticides, polychlorinated biphenyls, phthalates, and organophosphate pesticides. Third, we focused on three composite scores for common childhood and adolescent difficulties—internalizing, externalizing, and ADHD symptoms—derived from valid and reliable psychometric instruments.
However, there are several limitations to consider. Although we did not observe major differences between participants included in our analysis and those excluded due to non-available data on both exposure and outcome, using a sub-sample of the initial population might have introduced selection bias in our analyses. Furthermore, the use of different instruments for outcome assessment may lead to inconsistencies in measurement, potentially affecting the accuracy of association estimates. However, evidence suggests that SDQ and CBCL are correlated and assess similar constructs [70,71], and data harmonization was performed using z-scores to minimize potential discrepancies. Another concern is that child symptoms were reported by mothers, which might have influenced the outcome assessment. Moreover, we acknowledge as a limitation of the study the lack of biomarkers of neurotoxicity or endocrine disruption (e.g., hormone levels, thyroid function, cytokines). Future studies integrating biological measurements of such indicators could offer valuable insights into the observed behavioral outcomes and help clarify the sex-specific effects identified in our analyses. In addition, further evidence on how environmental chemicals disrupt hormonal balance, especially estrogenic and androgenic pathways, can be critical for understanding their differential effects in boys and girls. Finally, although our models were adjusted for important confounding variables, the possibility of residual confounding remains.
5. Conclusions
Our study reveals that exposure to environmental chemicals at age 4 can have lasting adverse effects from early childhood through adolescence, particularly in girls. The robust sex-specific associations underscore the importance of considering sex as a key factor in environmental health research. Additionally, these findings highlight the need for further investigation into the biological mechanisms driving the differential effects of chemicals between males and females. Understanding these mechanisms is crucial for developing evidence-based policies and strategies aimed at minimizing children’s exposure to toxic chemicals, thereby protecting this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sacco R. Camilleri N. Eberhardt J. Umla-Runge K. Newbury-Birch D. A Systematic Review and Meta-Analysis on the Prevalence of Mental Disorders among Children and Adolescents in Europe Eur. Child. Adolesc. Psychiatry 2022332877289410.1007/s 00787-022-02131-236581685 PMC 9800241 · doi ↗ · pubmed ↗
- 2Sayal K. Prasad V. Daley D. Ford T. Coghill D. ADHD in Children and Young People: Prevalence, Care Pathways, and Service Provision Lancet Psychiatry 2018517518610.1016/S 2215-0366(17)30167-029033005 · doi ↗ · pubmed ↗
- 3Deighton J. Humphrey N. Belsky J. Boehnke J. Vostanis P. Patalay P. Longitudinal Pathways between Mental Health Difficulties and Academic Performance during Middle Childhood and Early Adolescence Br. J. Dev. Psychol.20183611012610.1111/bjdp.1221829150840 · doi ↗ · pubmed ↗
- 4Colder C.R. Scalco M. Trucco E.M. Read J.P. Lengua L.J. Wieczorek W.F. Hawk L.W. Prospective Associations of Internalizing and Externalizing Problems and Their Co-Occurrence with Early Adolescent Substance Use J. Abnorm. Child. Psychol.20134166767710.1007/s 10802-012-9701-023242624 PMC 3640685 · doi ↗ · pubmed ↗
- 5Mousteri V. Daly M. Delaney L. Tynelius P. Rasmussen F. Adolescent Mental Health and Unemployment over the Lifespan: Population Evidence from Sweden Soc. Sci. Med.201922230531410.1016/j.socscimed.2018.12.03030677644 · doi ↗ · pubmed ↗
- 6Kim-Cohen J. Caspi A. Moffitt T.E. Harrington H. Milne B.J. Poulton R. Prior Juvenile Diagnoses in Adults With Mental Disorder: Developmental Follow-Back of a Prospective-Longitudinal Cohort Arch. Gen. Psychiatry 20036070971710.1001/archpsyc.60.7.70912860775 · doi ↗ · pubmed ↗
- 7Mulraney M. Coghill D. Bishop C. Mehmed Y. Sciberras E. Sawyer M. Efron D. Hiscock H. A Systematic Review of the Persistence of Childhood Mental Health Problems into Adulthood Neurosci. Biobehav. Rev.202112918220510.1016/j.neubiorev.2021.07.03034363845 · doi ↗ · pubmed ↗
- 8Grandjean P. Landrigan P. Developmental Neurotoxicity of Industrial Chemicals Lancet 20063682167217810.1016/S 0140-6736(06)69665-717174709 · doi ↗ · pubmed ↗