Gender-Associated Factors on the Occurrence and Prevalence of Zero-Dose Children in Sub-Saharan Africa: A Critical Literature Review
Godfrey Musuka, Enos Moyo, Patrick Gad Iradukunda, Pierre Gashema, Roda Madziva, Helena Herrera, Tapiwa Dhliwayo, Constantine Mutata, Noah Mataruse, Oscar Mano, Elliot Mbunge, Tafadzwa Dzinamarira

TL;DR
This paper reviews how gender-related factors affect the immunization of children in Sub-Saharan Africa, highlighting barriers like gender norms and women's empowerment.
Contribution
The study systematically identifies and categorizes gender-associated factors influencing zero-dose children in Sub-Saharan Africa.
Findings
Gender-based violence and limited women's autonomy are linked to poor immunization outcomes.
Patriarchal norms and low male involvement negatively affect vaccine uptake.
Socioeconomic barriers like poverty and geographic inaccessibility hinder immunization.
Abstract
Background: Immunisation remains one of the most effective and cost-efficient public health interventions for preventing infectious diseases in children. Despite global progress, Sub-Saharan Africa (SSA) continues to face challenges in achieving equitable immunisation coverage. Gender-related disparities, rooted in sociocultural and structural inequalities, significantly influence the prevalence of zero-dose and under-immunised children in the region. This review critically examines the gender-associated barriers to routine childhood immunisation in SSA to inform more inclusive and equitable health interventions. Methods: A critical literature review was conducted generally following some steps of the PRISMA-P and CRD guidelines. Using the Population–Concept–Context (PCC) framework, studies were selected that examined gender-related barriers to routine immunisation for children under…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
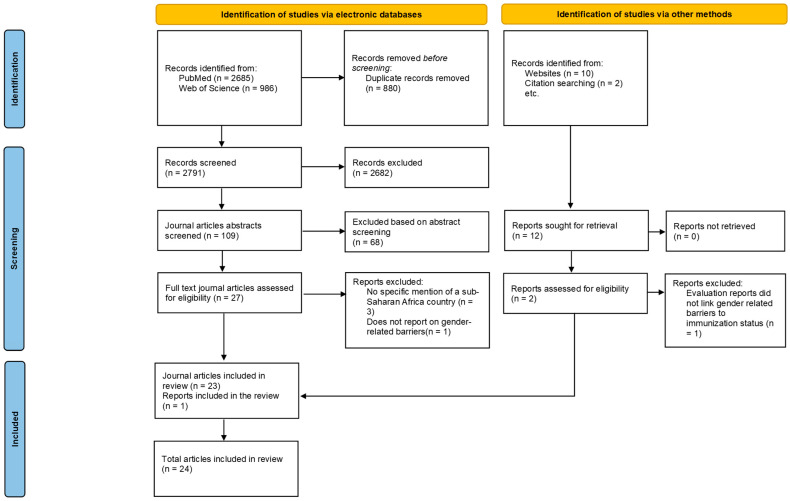 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoverty, Education, and Child Welfare · Child Nutrition and Water Access · Global Maternal and Child Health
1. Introduction
Immunisation is one of the most effective and cost-effective public health interventions for preventing infectious diseases in children [1]. Widespread immunisation coverage has significantly reduced morbidity and mortality from vaccine-preventable diseases (VPDs) globally [2]. However, despite the undeniable benefits, achieving and maintaining high levels of immunisation coverage remains a challenge in many countries, particularly for specific populations [3,4]. The Africa region has the highest prevalence of under-vaccinated and unvaccinated children. For instance, approximately 12.7 million children were under-vaccinated in 2021, and 14.5 million did not receive a single dose, also called “zero-dose” children in 2023 [5]. Among other challenges, gender-related barriers significantly contribute to inequalities in immunisation coverage and low immunisation rates. These barriers include harmful gender norms, lack of access to education, unequal power dynamics, limited mobility of women, limited decision-making among women in households and gender-based violence [6]. Gender disparities in immunisation rates persist in many parts of the world [7], including Sub-Saharan Africa. These disparities can be attributed to a complex interplay of factors, with social norms, economic inequalities, and limited access to education and information often playing a significant role [8]. Previous studies have highlighted a range of gender-related factors that influence immunisation uptake, including maternal education, autonomy in healthcare decision-making, and access to healthcare services [9,10,11]. For example, research has shown that children of mothers with limited decision-making power or restricted mobility are less likely to understand vaccination schedules [9,12]. Additionally, entrenched gender roles often result in women bearing the sole responsibility for child health without corresponding support or access to resources, further exacerbating disparities [13].
Despite growing recognition of these challenges, much of the existing literature is fragmented or context-specific, lacking a comprehensive synthesis of evidence across Sub-Saharan Africa. This review seeks to fill that gap by critically consolidating the available evidence to better understand how gender dynamics influence immunisation access and uptake, ultimately informing gender-sensitive policies and interventions across the region. This critical literature review aims to identify and analyse significant gender-related barriers to routine immunisation service delivery for children in Sub-Saharan Africa.
2. Methods
2.1. Study Design
A critical literature review of the available literature was conducted. The review loosely adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) guidelines [14] and the Centre for Reviews and Dissemination (CRD) guidance for undertaking systematic reviews in healthcare [15].
2.2. Research Question and Study Eligibility
The population–concept–context (PCC) framework (Table 1) was employed to establish the eligibility criteria for the review question, in accordance with recommendations from the Joanna Briggs Institute [16].
This review addresses the following research question: What are gender-related barriers to routine immunisation service delivery for children in Sub-Saharan Africa?
2.3. Literature Sources
A comprehensive search was conducted on PubMed, Google Scholar, Web of Science electronic databases, and the websites of the WHO and UNICEF for articles reporting on routine immunisation service delivery. The review focused on articles published within the last 10 years to provide the most current information.
2.4. Search Strategy
A comprehensive search strategy was co-developed and pilot-tested in collaboration with a senior health science librarian. The search terms included gender, immunisation, barriers, vaccine hesitancy, decision-making, and education. Cultural practices, social norms, economic factors, health equity, and child health. The strategy was tailored for each database to ensure the retrieval of the most relevant studies. A comprehensive search strategy, along with PubMed findings, is presented in Table 2. The search strategy includes Medical Subject Headings (MeSH) and text-word searches. Grey literature was identified by consulting targeted websites for UNICEF and WHO, and by consulting contact experts within those organisations. Similar screening strategies well employed to ensure relevance.
2.5. Title, Abstract, Full-Text Screening
Two independent reviewers screened titles, abstracts, and full-text articles for eligibility. Studies identified through database searches were exported to EndNote [17]. Duplicate articles were removed. Studies were then exported from EndNote to the Covidence systematic review management platform [18]. This review was informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines; however, we did not strictly adhere to all items. Specifically, the review did not include prospective protocol registration, we broadened the inclusion criteria to include grey literature and organisational reports, and risk of bias assessments were not conducted in a standardised PRISMA format. These deviations reflect the nature of this study as a critical literature review rather than a fully systematic review, but the use of PRISMA elements still provided transparency and structure in reporting.
2.6. Data Abstraction and Analysis
A standardised data extraction form was developed specifically for this review. The form captured relevant information from the identified studies to address the research question. It extracted data that included author(s), publication year, publication type, study location, study design, population, barriers identified, other key findings and conclusion.
The extracted data was then analysed thematically. This involved identifying recurring themes and patterns related to gender-related barriers to immunisation in Sub-Saharan Africa. Notes were taken to categorise and organise the findings according to the Population, Concept, and Context (PCC) framework. This approach facilitated a comprehensive understanding of how gender intersects with various factors to create barriers to immunisation services for children in Sub-Saharan Africa.
3. Results
Our search retrieved 3683 articles. After removing duplicates, 2803 articles remained. Upon screening, 2682 articles were removed at the title screening stage, 78 at the abstract screening stage, and five at the full-text screening stage, leaving 24 for inclusion in this desk review (Figure 1).
3.1. Characteristics of Included Articles
Twenty-four articles were included [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Of these, two were reports [27,28]. The majority were cross-sectional studies, while seven employed qualitative methods [29,32,35,36,37,39,42]. More details are presented in Table 3.
3.2. Gender-Related Barriers to Routine Immunisation Service Delivery
Four themes emerged from the data analysis.
Theme 1: Women’s empowerment and autonomy
a. Decision-making power in health and household matters
Women’s ability to make autonomous decisions about their child’s health, especially immunisation, was a consistent predictor of vaccine uptake. In many households, male partners had final authority, limiting mothers’ access to services [23,25,27,36].
b. Financial resource access
Limited financial autonomy, including access to household income and decision-making around spending, was frequently cited as a barrier. Women who shared or had control over finances were more likely to vaccinate their children fully [24,31,37].
c. Influence of gender-based violence and social inequity
In contexts where women accepted or experienced gender-based violence or coercion, immunisation rates were lower [25]. Broader gender inequalities, such as restrictions on mobility or social participation, also undermined women’s health-seeking behaviours [40,42].
Theme 2: Male involvement and gender norms
a. Patriarchal decision structures and cultural norms
Deep-rooted social norms positioned men as decision-makers and excluded them from child health roles, often leading to active or passive resistance to immunisation [32,38,39].
b. Low male engagement in child health
Men were often disengaged from practical childcare tasks, such as attending health appointments. Where men participated, through providing support or transport, immunisation rates improved [26,35].
c. Stigma and gendered expectations
Women bore the burden of ensuring child health, and were blamed for missed vaccinations, even when decisions or barriers were beyond their control [36,37].
Theme 3: Socioeconomic Inequities and Structural Barriers
a. Poverty and occupational status
Economic disadvantage, particularly among single mothers, unemployed women, or those in casual work, limits access to immunisation services [19,30,32]. Feeling ashamed due to poor appearance or social status was also a deterrent [24].
b. Geographic and service accessibility
Rural women faced limited transport, long distances, and inadequate health infrastructure, further widening the urban-rural immunisation gap [19,28,40]. Similarly, mothers and children living in informal settlements encountered additional geographic and structural barriers. These communities often lacked nearby health facilities, faced overcrowding, and experienced irregular service delivery, reducing the consistency and reliability of immunisation access. Moreover, poor infrastructure, such as unpaved roads and insecure housing, created a physically and socially unstable environment that deprioritised preventive healthcare, including vaccination. Mobile populations, such as nomadic groups, faced even greater challenges. Their transient lifestyles often placed them outside the reach of static health systems, and a lack of proper identification or residence documentation further excluded them from immunisation registries and planning [28]. These geographical and structural exclusions compounded existing socioeconomic disadvantages, deepening immunisation inequities across both fixed and mobile underserved populations.
c. Maternal workload and time constraints
Heavy caregiving burdens, lack of childcare support, and household responsibilities constrained mothers’ time and energy to attend immunisation sessions [22,35].
Theme 4: Education, Awareness, and Health System Responsiveness
a. Maternal education and knowledge about vaccines
Mothers with no or low education levels were less likely to understand the benefits of immunisation and adhere to schedules [21,30,33].
b. Health Information access and media exposure
In many cases, women lacked access to information about immunisation due to limited literacy, media reach, or engagement with health extension services [26,40].
c. Gender-sensitive service design and ease of access to mothers
Several studies emphasised the lack of gender-sensitive planning in immunisation programmes. Health systems often failed to consider women’s needs, mobility restrictions, or potential for community mobilisation [35,41,42]. Further details are enclosed in Table 4.
4. Discussion
This review aimed to identify and synthesise gender-related factors influencing the access to and uptake of routine immunisation services for children in sub-Saharan Africa. The findings reveal that gender is an essential social determinant that intersects with socioeconomic, cultural, and structural barriers, shaping both the demand and supply of immunisation services. Our analysis highlights how gender norms and inequalities fundamentally influence caregivers’ ability to access and utilise these services, especially mothers.
4.1. Gendered Power Dynamics and Decision-Making Autonomy
One of the most consistent findings across studies was the role of women’s decision-making power in determining immunisation uptake [19,20,21,22,23,24,25]. Mothers with greater autonomy, especially regarding financial decisions and health-seeking behaviours, were significantly more likely to immunise their children fully. For instance, mothers who shared financial decision-making with partners had up to 8.1 times greater odds of fully vaccinating their children than those whose husbands retained sole control [21]. In contrast, male-dominated decision-making structures, which are usually shaped by patriarchal norms, often hinder timely vaccination. Even when women were willing to immunise their children, opposition or lack of support from male partners could result in missed vaccinations, illustrating how intra-household power dynamics serve as a gatekeeping mechanism that could act as barriers or facilitators to children’s health [22].
These findings underscore the importance of women’s empowerment as a critical enabler of child immunisation in issues of control over financial resources, health-related decision-making, and mobility. Where these domains are restricted, women’s capacity to prioritise or even access immunisation services is undermined. Notably, female-headed households, often considered more autonomous, had higher rates of under-immunisation, suggesting that autonomy alone is insufficient in contexts of poverty and weak health systems [25]. In addition to resource limitations, this review highlights the impact of existing attitudes and behavioural norms that may hinder vaccination uptake. This is where other factors uncovered by the critical literature review come to the fore.
4.2. Male Engagement and Gender Roles
From a delivery point of view, while much of the responsibility for child immunisation is placed on mothers, limited male engagement in child health creates a gendered burden that negatively affects immunisation uptake [20,24,35,37]. This can be due to sociocultural norms or a lack of awareness and initiative in the male parents and limited support provided to mothers, so they can access the point of delivery. Fathers were generally excluded from caregiving roles, and their involvement in vaccination was minimal. However, studies consistently show that when men are involved, vaccination rates improve significantly (AOR = 3.27, 95% CI: 1.84–5.81) [24]. Male involvement may look like providing transport, financial support for immunisation-related costs, accompanying mothers to clinics, supporting household chores, or just offering emotional and moral support besides their practical contributions. Fathers’ active support of vaccination can significantly influence the allocation of limited household resources, particularly in situations where conflicting demands may undermine preventive health initiatives.
This factor suggests that redefining caregiving from solely a woman’s responsibility to a shared parental role could improve immunisation outcomes.
Notably, male disengagement was not always passive. In some cases, opposition from fathers stemmed from misinformation, fear of vaccine side effects, or religious and cultural beliefs [36]. These findings highlight the urgent need for targeted health communication and outreach strategies that include men as partners in child health, challenge harmful gender norms, and promote shared decision-making. This is essential to empower not only women, but also men, to bring about change in this and the following generations on this critical public health intervention.
4.3. Maternal Education, Knowledge, and Age
Maternal education emerged as a robust predictor of immunisation, informed decision-making, financial independence, and social participation. Children of uneducated or illiterate mothers had significantly lower odds of being fully immunised [17,19,28,31]. Education likely functions through multiple pathways to enhance knowledge of vaccine benefits, increase health literacy, and possibly moreover empower women to make informed decisions and overcome barriers to immunisation, of which they may find fewer than those from lower cultural levels. Similarly, mothers with better knowledge about immunisation schedules were more likely to ensure complete vaccination.
Younger maternal age (especially 18–25 years) was associated with incomplete immunisation, possibly reflecting limited experience, lower autonomy, or constrained access to support systems [28]. Conversely, maternal age above 40 years was positively associated with full immunisation (AOR = 7.37, CI: 1.65–32), suggesting that older caregivers may possess greater confidence, autonomy, or social capital [24]. Further unknown factors may be influencing this group, despite similar confounders, such as financial resources and male support, to those of older women for the same outcomes.
4.4. Health System Responsiveness and Service Design
Gender-blind service delivery further perpetuated barriers. Immunisation services often failed to accommodate the unique needs of women, such as childcare responsibilities, mobility restrictions, or sociocultural expectations. This may be particularly true for younger women who have additional support needs. The health system’s limited outreach to male partners and lack of integration of gender-responsive strategies left many families navigating services within the constraints of unequal household dynamics. However, several studies noted that facility-based delivery, antenatal care (ANC) attendance, and postpartum home visits by health extension workers were associated with improved immunisation coverage. This emphasises the value of leveraging maternal health touchpoints for vaccination education and follow-up [24].
Health worker-patient gender discordance, especially in conservative settings, emerged as a barrier, with some women reluctant to access services from male providers. Moreover, poor media reach and inadequate communication channels resulted in women lacking key information about immunisation, especially in marginalised or low-literacy communities [40].
4.5. Socioeconomic and Structural Inequities
Gender-related barriers to immunisation were shown to be strongly influenced by structural determinants of health such as poverty, education, and geographic location. Economic disadvantage, particularly among women in low-income households, single mothers, or those engaged in informal work, limits access to services [17,28,29,30]. Some mothers expressed shame related to poverty, for example, being unable to dress appropriately for clinic visits, which further discouraged service utilisation [22]. Wealth disparities, combined with gendered financial dependency, meant that poorer women often lacked the resources to prioritise immunisation even when they were motivated to do so.
Geographic inequalities further complicated access. Women in rural areas faced long travel distances, limited transport options, and inadequate health infrastructure [17,26]. These barriers were particularly acute for mothers with childcare and domestic burdens, highlighting how the intersection of gender roles and spatial marginalisation creates compounding disadvantages. While improvements in rural coverage have been observed, the urban-rural gap remains a significant challenge in achieving equitable immunisation.
4.6. Cultural and Social Norms
Traditional gender norms were found to be pervasive, for instance, expectations that women alone are responsible for child health delivery [38,39,40] but not necessarily for broader decision-making with regard to prioritising and resourcing how and if healthcare should be delivered. These norms simultaneously placed the burden of immunisation on mothers while restricting their ability to fulfil it. Mothers were often blamed when children fell ill due to missed vaccinations, even when underlying causes included poverty, lack of partner support, or systemic barriers that were outside her control. Religious and cultural beliefs also played a role, with some communities using these ideologies to justify restrictions on women’s mobility or decision-making power within a culture of victim blaming, as women often suffer the consequences of poor child health.
Fear of vaccine side effects, especially among mothers who lacked spousal support, contributed to vaccine hesitancy [36,37]. When children experienced adverse reactions, women feared blame or violence, further reinforcing avoidance. These findings reveal a climate in which social expectations, emotional pressure, and limited autonomy converge to produce inequitable immunisation outcomes. Supporting these women in educating the next generation of children so that women can feel empowered and male carers understand the need for an equitable role can have a substantial impact on changing prevalent cultural and social norms.
5. Recommendations
Improving immunisation coverage in sub-Saharan Africa requires a gender-responsive approach that tackles the barriers faced by women, promotes shared responsibility for child health, and includes tailored education.
First, women’s decision-making empowerment must be addressed comprehensively, with a priority on maternal education. Education is a vital enabler of self-confidence and informed decision-making, fostering financial literacy and autonomy, which in turn leads to greater access to accurate health information. This will collectively enable more mothers to seek and complete immunisation for their children. This should be expanded beyond health education to encompass aspects that support the breaking of obstructive social norms, such as the fear of discrimination by healthcare providers or blame for adverse vaccination events. Programmes should support women through transport subsidies, flexible clinic hours, and integration of immunisation with maternal health services such as ANC and facility deliveries. They also show how the financial impact of vaccination can prevent the disease from posing a further burden on the family’s resources.
Second, male engagement is essential. Immunisation should be reframed as a shared parental responsibility. Involving men through targeted outreach, couple-based education, and community dialogues can reduce opposition and improve support for mothers. This could also widen their perceived responsibility concerning the day-to-day provision of healthcare to their family.
Third, health systems must recognise and respond to the realities of gender roles, with a focus on rural areas where religious and cultural norms have a stronger hold that limits the effectiveness of empowerment interventions. This includes addressing heavy maternal workloads, lack of male partner support, and religious and cultural restrictions on women’s mobility and autonomy. Gender-sensitive service delivery, outreach in hard-to-reach areas, and respectful interactions with providers are key. This should be particularly sensitive to vulnerable groups, such as single mothers or those with previous negative experiences when engaging with healthcare services.
Finally, policies and programmes must be informed by gender analysis and data. Collecting and using sex-disaggregated data, monitoring gender-related disparities, and designing interventions with a gender lens will help ensure equity and reach for all children, especially the zero-dose and under-immunised. This will be done while building a robust evidence base that can be used to rationalise resources and maximise the outcomes of investments in healthcare interventions.
6. Strengths and Limitations of the Review
The key strength of our study is the rigorous systematic methodology, as evidenced by the inclusion of diverse studies from across sub-Saharan Africa, focusing on an under-researched topic: the gendered dimension of immunisation.
The reviewed studies revealed several methodological limitations that may have influenced our findings. A significant issue was the reliance on convenience sampling, which often led to unrepresentative study populations, a lack of standard error measures, and selection bias. An additional limitation is that only articles published in English were considered, which might have introduced a language bias. Some of the studies included in this review were retrospective, which may have led to some findings being affected by recall bias. The inclusion of cross-sectional studies means that causality cannot be established with certainty.
Other limitations of our study include the limited availability of sex-disaggregated and zero-dose-specific data in some studies, the absence of critical appraisal of included studies, the lack of quantitative synthesis, and limited homogeneity in study designs, review quality, and comparability.
Additionally, the review process is susceptible to a potential selective reporting bias, as it relies heavily on the authors’ interpretations. Nonetheless, the findings provide insights critical to immunisation programmes in the region.
7. Conclusions
The review has highlighted the critical role of gender in shaping access to and uptake of childhood immunisation in sub-Saharan Africa. The persistence of zero-dose and under-immunised children is closely linked to gendered barriers ranging from limited maternal autonomy and male disengagement to poverty, poor service design, and restrictive social norms. Strategies to address these issues should not only involve those that seek to empower women but also engage men, reform health systems, and apply an intersectional gender lens to policy and programming. A more equitable and inclusive approach is essential to reach all children, particularly those who have been historically excluded, such as those residing in rural areas, from life-saving immunisation services.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rémy V. Zöllner Y. Heckmann U. Vaccination: The cornerstone of an efficient healthcare system J. Mark. Access Health Policy 201532704110.3402/jmahp.v 3.27041 PMC 480270327123189 · doi ↗ · pubmed ↗
- 2Brenzel L. Wolfson L.J. Fox-Rushby J. Miller M. Halsey N.A. Vaccine-preventable diseases Disease Control Priorities in Developing Countries Oxford University Press New York, NY, USA 2006 Volume 2389412
- 3Lindstrand A. Cherian T. Chang-Blanc D. Feikin D. O’Brien K.L. The world of immunization: Achievements, challenges, and strategic vision for the next decade J. Infect. Dis.2021224 S 452S 46710.1093/infdis/jiab 28434590130 PMC 8482029 · doi ↗ · pubmed ↗
- 4Duclos P. Okwo-Bele J.-M. Gacic-Dobo M. Cherian T. Global immunization: Status, progress, challenges and future BMC Int. Health Hum. Rights 20099 S 210.1186/1472-698X-9-S 1-S 219828060 PMC 2762311 · doi ↗ · pubmed ↗
- 5WHO Global Childhood Immunization Levels Stalled in 2023, Leaving Many Without Life-Saving Protection Available online: https://www.who.int/news/item/15-07-2024-global-childhood-immunization-levels-stalled-in-2023-leaving-many-without-life-saving-protection(accessed on 26 September 2025)
- 6Nyasulu B.J. Heidari S. Manna M. Bahl J. Goodman T. Gender analysis of the World Health Organization online learning program on Immunization Agenda 2030 Front. Glob. Womens Health 20234123010910.3389/fgwh.2023.123010938152380 PMC 10751919 · doi ↗ · pubmed ↗
- 7Ali H.A. Hartner A.-M. Echeverria-Londono S. Roth J. Li X. Abbas K. Portnoy A. Vynnycky E. Woodruff K. Ferguson N.M. Vaccine equity in low and middle income countries: A systematic review and meta-analysis Int. J. Equity Health 2022218210.1186/s 12939-022-01678-535701823 PMC 9194352 · doi ↗ · pubmed ↗
- 8Fekadu H. Mekonnen W. Adugna A. Kloos H. Haile Mariam D. Inequities and trends of polio immunisation among children aged 12–23 months in Ethiopia: A multilevel analysis of Ethiopian demographic and health survey BMJ Open 202414 e 07957010.1136/bmjopen-2023-079570 PMC 1095297238503420 · doi ↗ · pubmed ↗