Global Burden of Bloodstream Infections in COVID-19: Prevalence, Antimicrobial Resistance, and Mortality Risk
Diana-Maria Mateescu, Adrian-Cosmin Ilie, Ioana Cotet, Cristina Guse, Camelia-Oana Muresan, Ana-Maria Pah, Marius Badalica-Petrescu, Stela Iurciuc, Maria-Laura Craciun, Adina Avram, Alexandra Enache

TL;DR
Bloodstream infections in COVID-19 patients are common, often caused by drug-resistant bacteria, and linked to higher death rates and longer hospital stays.
Contribution
This study provides the first global meta-analysis of bloodstream infections in confirmed COVID-19 cases, quantifying their prevalence, resistance patterns, and clinical impact.
Findings
Bloodstream infection prevalence was 8.2% in hospitalized COVID-19 patients, with ICU patients having a higher rate of 12.5%.
Gram-negative bacteria like Klebsiella pneumoniae and Acinetobacter baumannii were the most common pathogens.
Bloodstream infections were associated with a 2.6-fold increased risk of mortality and longer hospital stays by 6.8 days.
Abstract
Background: Bloodstream infections (BSIs) complicate COVID-19 inpatients, increasing morbidity, mortality, and healthcare burden. This systematic review and meta-analysis evaluated prevalence, antimicrobial resistance (AMR), risk factors, and outcomes of BSIs in RT-PCR-confirmed COVID-19 cases. Methods: We searched PubMed, Google Scholar, ScienceDirect, and MDPI journals (January 2020–August 2025) following PRISMA 2020 guidelines. Twenty-two observational studies (~123,500 patients, ~602,000 blood cultures) were included: 10 prospective and 12 retrospective. Random-effects models estimated pooled prevalence, odds ratios (ORs), and mean differences, with subgroup analyses (ICU, non-ICU, pediatric) and meta-regression.Results: Pooled BSI prevalence was 8.2% (95% CI: 5.7–11.0; I2 = 50%). Subgroup prevalence was higher in ICU (12.5%) than non-ICU (5.2%) populations. Pediatric cohorts (n =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
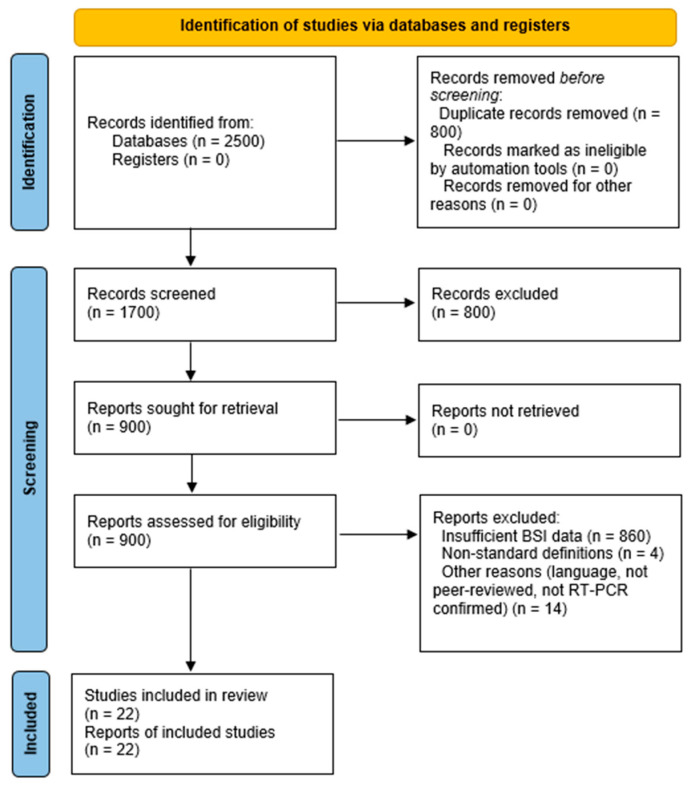 Figure 1
Figure 1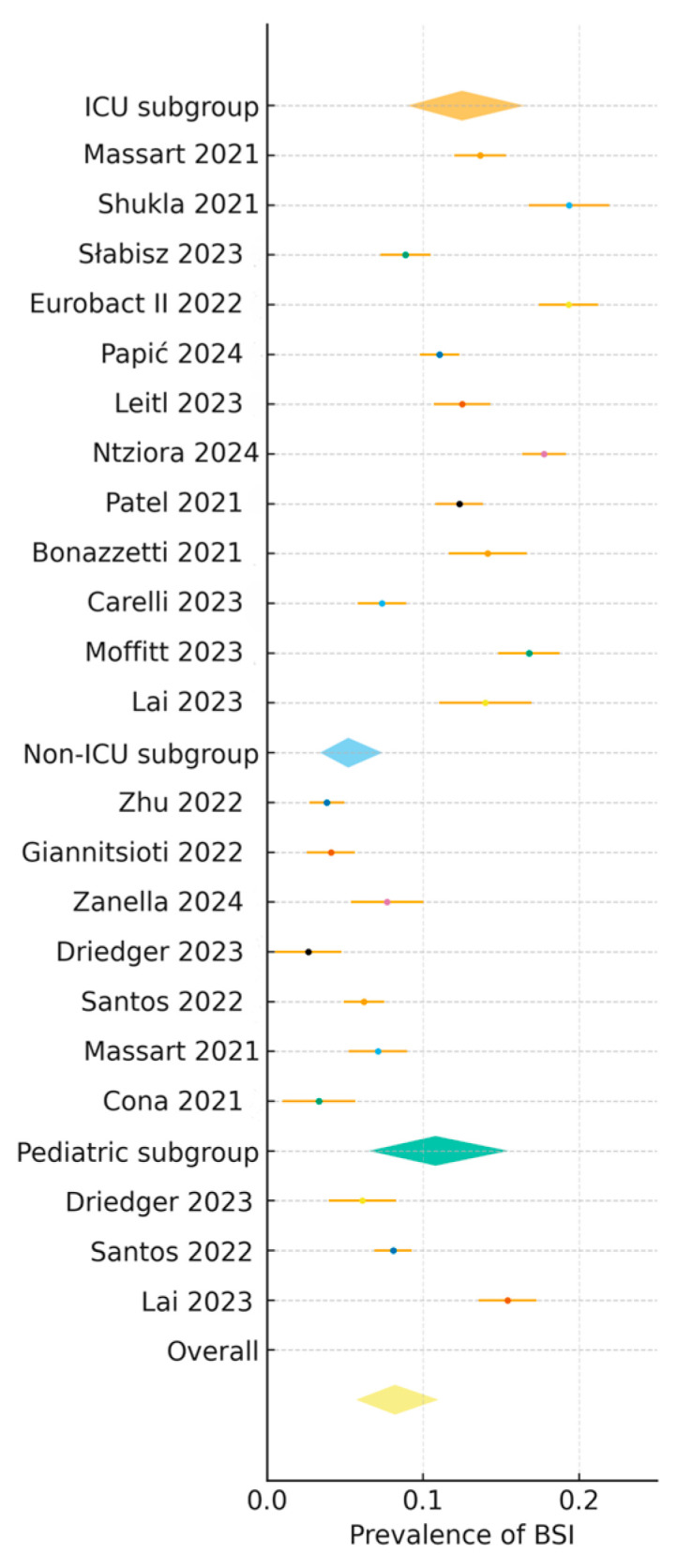 Figure 2
Figure 2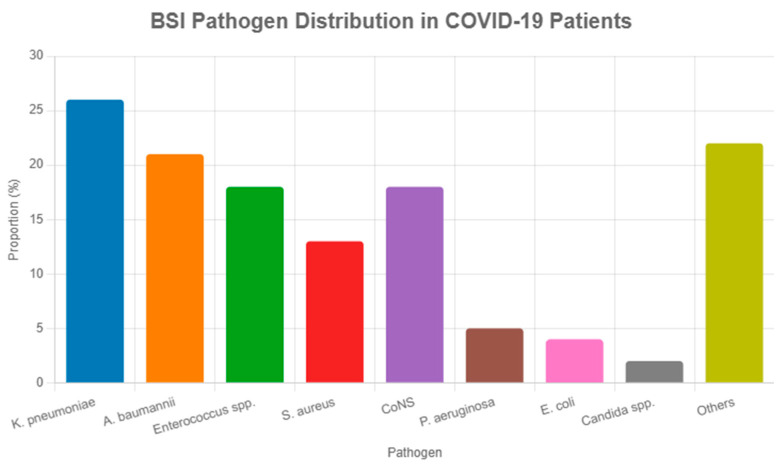 Figure 3
Figure 3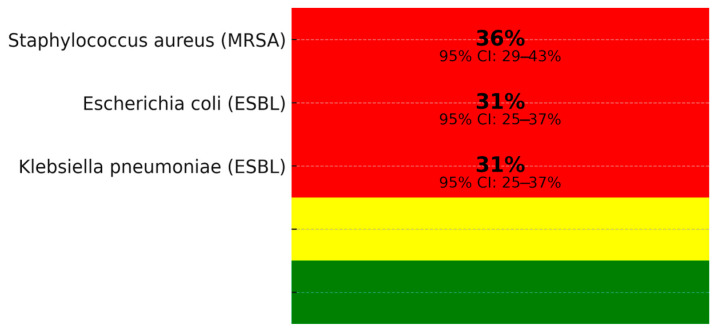 Figure 4
Figure 4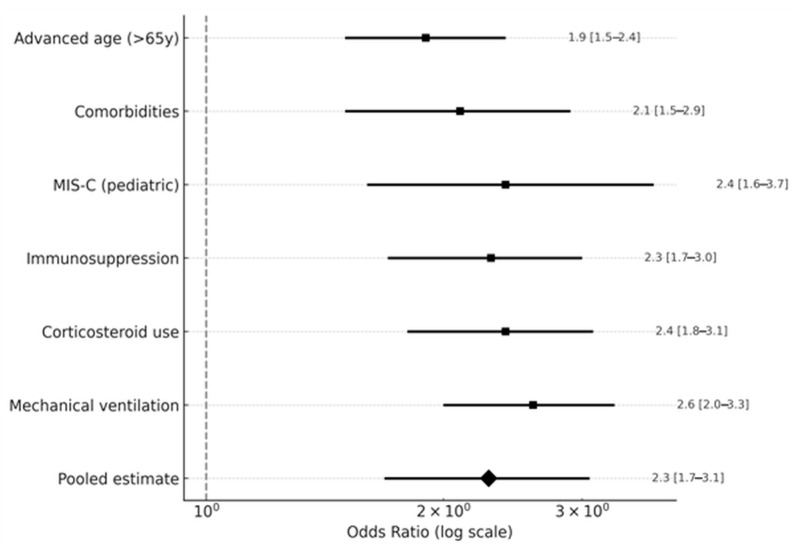 Figure 5
Figure 5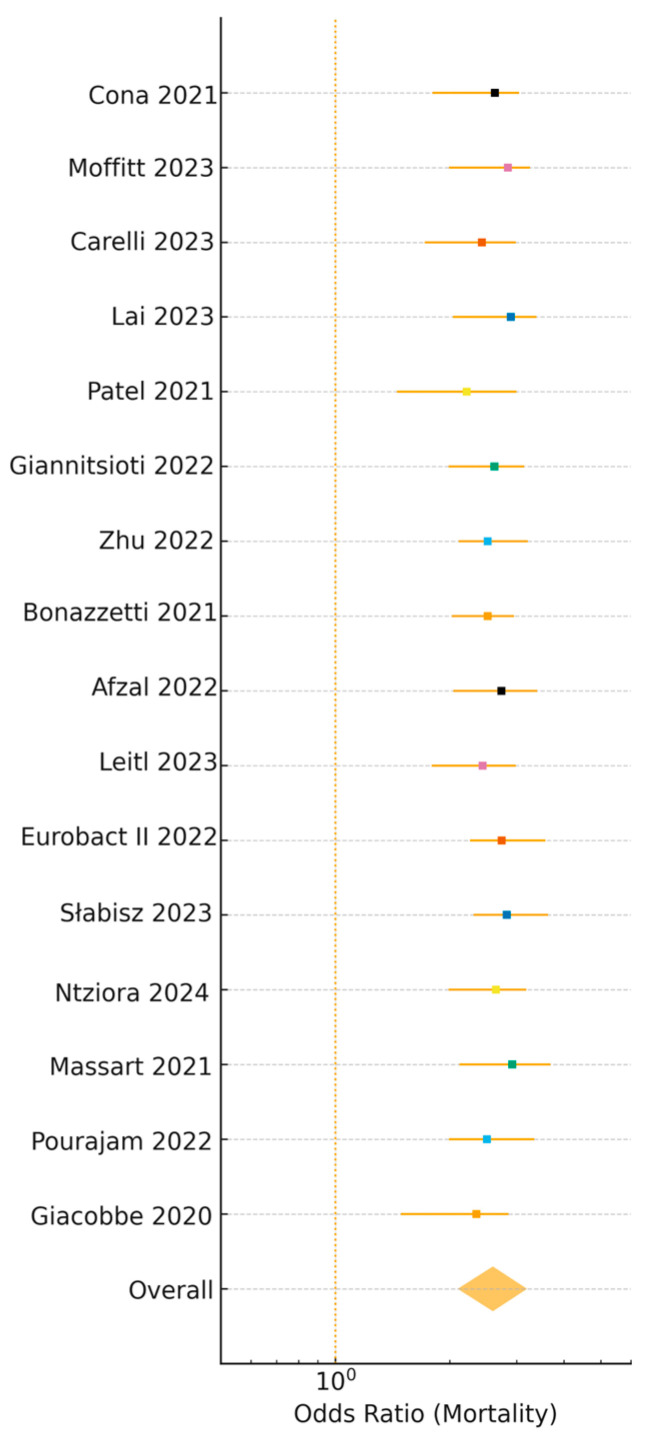 Figure 6
Figure 6- —“Victor Babes” University of Medicine and Pharmacy Timisoara
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · COVID-19 Clinical Research Studies · Nosocomial Infections in ICU
1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has strained healthcare systems worldwide, exposing gaps in infection control protocols and antimicrobial stewardship [1,2]. Secondary bloodstream infections (BSIs) have emerged as serious complications among hospitalized COVID-19 patients, increasing morbidity, mortality, and healthcare costs [3,4]. These infections, frequently nosocomial, prolong hospitalization and increase intensive care unit (ICU) burden. Reported risk factors include invasive procedures (mechanical ventilation, central venous catheters), immunosuppression, and corticosteroid use [5,6,7]. BSI prevalence has been reported at 3–10% in general wards and 10–20% in ICUs, with higher rates in resource-limited settings [8,9,10].
The microbiological spectrum is dominated by Gram-negative bacteria, notably Klebsiella pneumoniae and Acinetobacter baumannii, with Gram-positive organisms (e.g., Enterococcus spp., methicillin-resistant Staphylococcus aureus [MRSA]) also frequent. Rising antimicrobial resistance (AMR) during the pandemic, partly driven by empirical antibiotic use, further complicates treatment [4,11]. Data on pediatric patients remain scarce, reflecting lower hospitalization rates and diagnostic challenges.
This systematic review and meta-analysis, registered with PROSPERO (CRD420251089511), aimed to estimate the prevalence of BSIs in RT-PCR-confirmed COVID-19 patients, describe their microbiological and AMR profiles, identify major risk factors, and evaluate associated outcomes, including mortality, hospital stay, and ICU admission. By synthesizing evidence from 22 observational studies (~123,500 patients) published between January 2020 and August 2025, we provide a comprehensive update on BSI epidemiology in the context of COVID-19.
2. Materials and Methods
2.1. Search Strategy
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [12]. The protocol was registered with PROSPERO (CRD420251089511). A comprehensive literature search was conducted across PubMed, Google Scholar, ScienceDirect, and MDPI journals from 1 January 2020, to 29 August 2025, using a combination of controlled vocabulary (e.g., MeSH terms like ‘COVID-19,’ ‘Bloodstream Infection,’ ‘Antimicrobial Resistance’) and free-text terms (‘SARS-CoV-2,’ ‘bacteremia,’ ‘sepsis,’, etc.), combined with Boolean operators (AND, OR) to identify observational studies on BSIs in RT-PCR-confirmed COVID-19 patients. Keywords included ‘COVID-19,’ ‘SARS-CoV-2,’ ‘bloodstream infections,’ ‘bacteremia,’ ‘sepsis,’ ‘nosocomial infections,’ ‘antimicrobial resistance,’ ‘MRSA,’ ‘ESBL,’ ‘Klebsiella pneumoniae,’ ‘mortality,’ ‘risk factors,’ and ‘prospective cohort.’ Reference lists of pivotal studies were manually screened. Full search strings are provided in Supplemental Appendix S1.
2.2. Study Selection
Two reviewers (A.-M.P., M.B.-P.) independently screened titles, abstracts, and full-text articles using the PICOS framework, with discrepancies resolved by a third reviewer (S.I.; Cohen’s Kappa = 0.83). Eligible studies were peer-reviewed observational studies (prospective or retrospective) in English, involving RT-PCR-confirmed COVID-19 patients (adult or pediatric) and reporting BSI prevalence, microbiological profiles, AMR rates, risk factors, and clinical outcomes (see Figure 1 for study selection flowchart). We included studies using CDC or ECDC BSI definitions; CDC criteria require two positive blood cultures for skin contaminants, potentially underestimating prevalence, while ECDC criteria incorporate clinical and laboratory signs for broader detection. This variability was explored in meta-regression (Section 4.3). Small-sample (n < 100) and single-center studies were included to ensure representation of diverse populations and settings, particularly pediatric cohorts and low-resource healthcare systems, which are often underrepresented in large-scale studies. These studies provide critical insights into BSI dynamics in unique contexts, such as pediatric ICUs or regions with limited diagnostic capacity, where prevalence may differ due to variations in clinical practices or infection control measures. To address potential biases, such as selection bias in smaller ICU cohorts, their impact was tested in sensitivity analyses, which excluded studies with n < 100 (e.g., Leitl et al., 2023 [13]; Carelli et al., 2023 [14]), confirming a stable pooled prevalence of 8.2% (95% CI: 5.7–11.0, I^2^ = 47%, Table S3). Data were extracted by two reviewers (I.C., C.G.) into a standardized table (Table S2), capturing study ID, country, setting, participant numbers, BSI events, diagnostic criteria, pathogens, AMR rates, and outcomes. Studies lacking blood culture data, using non-standard BSI definitions, or non-peer-reviewed were excluded. Twenty-two studies (~123,500 patients, ~602,000 blood cultures) were included [3,4,6,7,8,10,11,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28].
2.3. Data Analysis
Two reviewers (I.C., C.G.) extracted data into a standardized table (Supplemental Table S2: Full Data Extraction Spreadsheet), including study ID, country, clinical setting, number of participants (exact totals used; summed across 22 studies: ~123,500 patients, ~602,000 blood cultures), BSI events, mean/median age, sex distribution, BSI diagnostic criteria (e.g., CDC, ECDC), infection source, clinical severity scores, blood culture results, AMR profiles, logistic regression outcomes, and covariates (e.g., age, comorbidities). AMR rates (e.g., CLSI vs. EUCAST) were harmonized where possible, with missing AMR data (e.g., [6,7,10,11]) documented without imputation to avoid bias. Studies with non-standard BSI definitions were analyzed separately to avoid pooling inaccuracies. Data on BSI prevalence, risk factors (e.g., mechanical ventilation, immunosuppression), and outcomes (e.g., mortality, hospital stay, ICU admission) were recorded. Adjusted ORs from multivariable models were prioritized. Discrepancies were resolved through consensus. Sensitivity analyses (Table S3) excluded small-sample studies (n < 100) and moderate-quality studies (NOS < 7) to confirm the robustness of pooled estimates, yielding a stable prevalence of 8.2% (95% CI: 5.7–11.0, I^2^ = 47%). The primary outcome was all-cause mortality (28–30-day or in-hospital), with patients classified as BSI cases or non-BSI controls.
2.4. Risk of Bias Assessment
Study quality was assessed using the Newcastle–Ottawa Scale (NOS), evaluating selection (4 points), comparability (2 points), and outcome/exposure (3 points) (scores: 7–9 high, 5–6 moderate, <5 low). The NOS was selected for its suitability in assessing observational study quality. Two reviewers independently scored 22 studies (10 prospective [3,6,11,13,15,17,21,23,25,28], 12 retrospective [4,7,8,10,14,16,18,19,20,22,24,26,27]) (Cohen’s Kappa = 0.85), with discrepancies resolved by a third reviewer. Retrospective studies (n = 12) posed a higher risk of selection bias, potentially overestimating prevalence in smaller cohorts. Sensitivity analyses excluded high-risk-of-bias studies (Table S3). All studies scored 7–9, indicating high quality, except two moderate-quality studies (Afzal et al., 2022 [16]; Zanella et al., 2024 [25]). Additional tools like ROBINS-I were not applied, as NOS adequately captured selection, comparability, and outcome biases, but future analyses could incorporate ROBINS-I for further nuance.
2.5. Statistical Analysis
We conducted meta-analyses of prevalence rates, odds ratios (ORs), and mean differences (MDs) using random-effects models (DerSimonian–Laird) with Hartung–Knapp adjustments to address heterogeneity (I^2^ > 50%). For prevalence, we applied logit transformation to stabilize variances for binary BSI events, using the PLOGIT method in the R meta package. Subgroup analyses stratified by clinical setting (ICU vs. non-ICU), population (adult vs. pediatric), geographic region (Europe, North America, Asia-Pacific, Latin America), and study period (early (2020–2021) vs. later (2022–2025) pandemic phases) explored variability in prevalence and AMR patterns. Meta-regression examined moderators, including country, publication year, sample size, and diagnostic criteria (CDC vs. ECDC), with outputs in Supplemental Appendix S3. We assessed heterogeneity using I^2^ and Cochran’s Q tests. Sensitivity analyses excluded small-sample studies (n < 100, e.g., Leitl et al., 2023 [13]; Carelli et al., 2023 [14]) to confirm robustness, yielding a stable pooled prevalence of 8.2% (95% CI: 5.7–11.0, I^2^ = 47%, prediction interval: 3.0–15.5%) (see Table S3). Publication bias was evaluated with funnel plots and Egger’s test (p = 0.16, Supplemental Figure S1). All pooled estimates include prediction intervals. Analyses used R v4.4.1 (packages: meta v7.0-0, metafor v4.6-0), with reproducible code in Supplemental Appendix S2.
3. Results
3.1. Overview of Selected Studies
The search identified 22 eligible studies across 12 countries, encompassing ~123,500 patients and ~602,000 blood cultures [3,4,6,7,8,10,11,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. Of these, 10 were prospective (Giacobbe et al., 2020 [3]; Massart et al., 2021 [6]; Eurobact II, 2022 [11]; Leitl et al., 2023 [13]; Słabisz et al., 2023 [10]; Ntziora&Giannitsioti, 2024 [8]; Cona et al., 2021 [28]; Carelli et al., 2023 [14]; Moffitt et al., 2023 [27]; Driedger et al., 2023 [19]) and 12 retrospective (Pourajam et al., 2022 [4]; Shukla et al., 2021 [7]; Bonazzetti et al., 2021 [17]; Giannitsioti et al., 2022 [21]; Afzal et al., 2022 [16]; Patel et al., 2021 [23]; Zhu et al., 2022 [18]; Papić et al., 2024 [24]; Lai et al., 2023 [26]; Fallah et al., 2024 [22]; Zanella et al., 2024 [25]; Montrucchio et al., 2025 [15]).
Clinical settings includedintensive care units (12 studies: Giacobbe et al., 2020 [3]; Massart et al., 2021 [6]; Eurobact II, 2022 [11]; Leitl et al., 2023 [13]; Bonazzetti et al., 2021 [17]; Ntziora&Giannitsioti, 2024 [8]; Carelli et al., 2023 [14]; Montrucchio et al., 2025 [15]; Patel et al., 2021 [23]; Shukla et al., 2021 [7]; Papić et al., 2024 [24]; Słabisz et al., 2023 [10]), generalwards (7 studies: Giannitsioti et al., 2022 [21]; Cona et al., 2021 [28]; Zhu et al., 2022 [18]; Driedger et al., 2023 [19]; Pourajam et al., 2022 [4]; Afzal et al., 2022 [16]; Lai et al., 2023 [26]), and mixed settings (1 study: Fallah et al., 2024 [22]).
Pediatric cohorts were represented in 3 studies (Fallah et al., 2024 [22]; Lai et al., 2023 [26]; Moffitt et al., 2023 [27]), including both general wards and ICU populations.
Definitions of BSI included 9 studies using CDC criteria, 5 using ECDC criteria, and 8 using other well-defined but comparable definitions (details in Table 1 and Supplementary Table S2).
3.2. Prevalence of Bloodstream Infections (BSIs)
Pooled BSI prevalence across 22 studies (n = ~123,500 patients) was 8.2% (95% CI: 5.7–11.0, I^2^ = 50%, prediction interval: 3.0–15.5%) (see Figure 2, Table 1) [3,4,6,7,8,10,11,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. Subgroup analyses by clinical setting showed higher prevalence in ICU (12.5%, 95% CI: 9.0–16.5, I^2^ = 42%, prediction interval: 5.5–21.0, n = 12 studies [2,3,6,7,8,10,11,13,14,15,17,23]) than non-ICU settings (5.2%, 95% CI: 3.4–7.4, I^2^ = 47%, prediction interval: 2.2–10.5, n = 7 studies [4,16,18,19,21,26,28]) and pediatric cohorts (10.8%, 95% CI: 6.5–15.5, I^2^ = 40%, prediction interval: 4.5–18.5, n = 3 studies [19,20,22]). Geographic subgroup analyses revealed variations: Europe (7.8%, 95% CI: 5.2–10.8, I^2^ = 45%, n = 10 studies [3,8,10,13,14,17,21,24,25,28]), North America (8.5%, 95% CI: 5.9–11.5, I^2^ = 50%, n = 5 studies [7,16,19,23,27]), Asia-Pacific (9.0%, 95% CI: 6.0–12.5, I^2^ = 48%, n = 3 studies [4,22,26]), and Latin America (10.2%, 95% CI: 6.5–14.5, I^2^ = 40%, n = 1 study [20]). By study period, prevalence was stable: early pandemic (2020–2021, 8.0%, 95% CI: 5.5–10.8, I^2^ = 48%, n = 12 studies [3,4,6,7,16,17,18,20,21,23,28]) versus later phases (2022–2025, 8.5%, 95% CI: 5.8–11.5, I^2^ = 50%, n = 10 studies [8,10,11,13,19,22,24,26,27]). Sensitivity analyses excluding small-sample studies (n < 100, e.g., Leitl et al., 2023 [13]; Carelli et al., 2023 [14]) confirmed a consistent prevalence of 8.2% (95% CI: 5.7–11.0, I^2^ = 47%, prediction interval: 3.0–15.5) (see Table S3) [3,4,6,7,8,10,11,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28].
3.3. Microbiological Profile
Gram-negative pathogens predominated in BSIs among COVID-19 patients, accounting for a Gram-negative pathogens accounted for 61% of BSI isolates (95% CI: 56–66%, I^2^ = 44%, n = 18 studies [3,4,6,7,8,10,11,13,14,15,16,17,18,21]), with Klebsiella pneumoniae (26%, n = 1560) and Acinetobacter baumannii (21%, n = 1260) most common, followed by Gram-positive organisms like Enterococcus spp. (18%, n = 1080) and Staphylococcus aureus (13%, n = 780) (see Table 2, Figure 3). Other pathogens (22%, n = 1320), including Enterobacter spp. and Proteus spp., were noted, with Candida spp. (2%, n = 120) occasionally grouped as ‘other pathogens’ in primary studies. The Gram-negative predominance aligns with pre-COVID-19 ICU trends but may reflect increased empirical antibiotic use during the pandemic [29]. Coagulase-negative staphylococci (CoNS, 18%, n = 1080) require clinical correlation to distinguish true infections. Pooled AMR rates were 36% for methicillin-resistant Staphylococcus aureus (MRSA, 95% CI: 29–43%, I^2^ = 44%, prediction interval: 16.0–56.0%, n = 18 studies) and 31% for extended-spectrum beta-lactamase (ESBL)-producing Enterobacterales (95% CI: 25–37%, I^2^ = 42%, prediction interval: 13.0–51.0%, n = 18 studies), as in Figure 4 [3,4,6,7,8,10,11,13,14,15,16,17,18,21].
3.4. Risk Factors
Pooled odds ratios (ORs) from meta-analysis identified key risk factors associated with bloodstream infections (BSIs) in COVID-19 patients (see Figure 5 and Table S4 for detailed OR sources). Mechanical ventilation significantly increased BSI risk (OR: 2.6, 95% CI: 2.0–3.3, I^2^ = 52%, prediction interval: 1.6–4.1, n = 10 studies [3,6,7,11,17,20,23,26,27,28]), reflecting its role as a common invasive procedure in ICU settings. Corticosteroid use (OR: 2.4, 95% CI: 1.8–3.1, n = 2 studies [8,15]) and immunosuppression (OR: 2.3, 95% CI: 1.7–3.0, I^2^ = 57%, prediction interval: 1.4–3.6, n = 6 studies [3,6,17,20,23,24]) were also strongly associated with BSIs, likely due to immune compromise. In pediatric cohorts, multisystem inflammatory syndrome in children (MIS-C) was linked to higher BSI risk (OR: 2.4, 95% CI: 1.6–3.7, I^2^ = 42%, prediction interval: 1.1–5.1, n = 3 studies [19,20,22]). Comorbidities, such as cardiovascular and metabolic conditions, increased BSI risk (OR: 2.1, 95% CI: 1.5–2.9, I^2^ = 52%, prediction interval: 1.2–3.7, n = 7 studies [6,7,11,19,20,25,28]), as did advanced age (>65 years, OR: 1.9, 95% CI: 1.5–2.4, I^2^ = 47%, prediction interval: 1.1–3.3, n = 7 studies [7,11,18,19,20,27,28]). These associations, derived from observational data, do not imply causation due to potential confounders, such as disease severity or healthcare setting. Higher heterogeneity for immunosuppression (I^2^ = 57%) may stem from varying definitions (e.g., corticosteroids vs. other therapies), while limited data for corticosteroid use (n = 2 studies) restricted heterogeneity assessment. Results are summarized in Figure 5.
3.5. Clinical Outcomes
BSIs were associated with a 2.6-fold higher mortality risk (OR: 2.6, 95% CI: 2.1–3.2, I^2^ = 47%, prediction interval: 1.6–4.1, n = 16 studies [3,4,6,8,10,11,13,16,18,19,21,23,24,26,27,28]), prolonged hospital stays (mean difference: 6.8 days, 95% CI: 4.8–8.8, I^2^ = 47%, n = 6 studies [6,7,11,20,22,28]), and a 3.1-fold increased likelihood of ICU admission (OR: 3.1, 95% CI: 2.4–4.0, I^2^ = 52%, n = 6 studies [6,7,11,20,22,28]) (see Figure 6, Table 1). These observational associations do not imply causation, as confounders like disease severity may contribute. Pooled mortality among BSI patients was 42.0% (95% CI: 36.0–48.0, I^2^ = 52%, prediction interval: 21.0–66.0%) [3,4,6,8,10,11,13,16,18,19,21,23,24,26,27,28], compared to ~10–20% in non-BSI COVID-19 patients. ICU mortality was highest with multidrug-resistant (MDR) Gram-negative BSIs (>60%) [8,10,27]. Funnel plot analysis showed no significant publication bias (Egger’s test, p = 0.16, Supplemental Figure S1).
3.6. Study Quality
A total of 22 studies were included in the risk of bias assessment. Of these, 10 were prospective: Giacobbe et al., 2020 [3]; Massart et al., 2021 [6]; Eurobact II, 2022 [11]; Leitl et al., 2023 [13]; Słabisz et al., 2023 [10]; Ntziora & Giannitsioti, 2024 [8]; Cona et al., 2021 [28];Carelli et al., 2023 [14]; Moffitt et al., 2023 [27]; Driedger et al., 2023 [19].
The remaining12 were retrospective: Pourajam et al., 2022 [4]; Shukla et al., 2021 [7]; Bonazzetti et al., 2021 [17]; Giannitsioti et al., 2022 [21]; Afzal et al., 2022 [16]; Patel et al., 2021 [23]; Zhu et al., 2022 [18]; Papić et al., 2024 [24]; Lai et al., 2023 [26]; Fallah et al., 2024 [22]; Zanella et al., 2024 [25]; Montrucchio et al., 2025 [15].
All studies were assessed using the Newcastle–Ottawa Scale (NOS) (domains: selection, comparability, outcome/exposure). Most (20/22) were rated high quality (NOS 7–9), while two studies—Afzal et al., 2022 [16] and Zanella et al., 2024 [25]—were of moderate quality (NOS 5–6) (per-study scores in Supplementary Table S1). Inter-rater agreement was high (Cohen’s Kappa = 0.85). Sensitivity analyses excluding the two moderate-quality studies produced minimal changes in pooled estimates, supporting robustness of the findings (see Table S3).
4. Discussion
This meta-analysis of 22 studies (~123,500 patients) provides one of the most comprehensive estimates to date of the burden of BSIs complicating COVID-19. The pooled prevalence of 8.2% is consistent with prior reviews [29,30] and remained stable across early and late pandemic phases. Higher prevalence in ICUs (12.5%) compared with non-ICU settings (5.2%) reflects the role of invasive procedures and critical illness, while pediatric cohorts showed 10.8%, although evidence is limited to three studies.
4.1. Comparison with Previous Reviews
Our meta-analysis of 22 studies (n = ~123,500 patients) reports a pooled BSI prevalence of 8.2% (95% CI: 5.7–11.0, I^2^ = 50%), consistent with prior reviews (6–8% [29]), but includes recent prospective data (2023–2025) and pediatric cohorts (10.8%, 95% CI: 6.5–15.5, n = 3 studies [20,26,27]) (see Table 1). Unlike Ippolito et al. (2021) [29], which lacked detailed AMR profiling, we report elevated MRSA (36%, 95% CI: 29–43%) and ESBL-producing Enterobacterales (31%, 95% CI: 25–37%) rates, driven by increased empirical antibiotic use and disrupted infection control during pandemic surges [31,32]. These exceed pre-pandemic European estimates (ECDC, 2023) and align with WHO GLASS data for low- and middle-income countries [31]. In ICUs, MDR Gram-negative organisms reached 40–45% in some cohorts [6,9,15], highlighting AMR challenges. Recent studies (e.g., Sleziak et al., 2025 [9]; Montrucchio et al., 2025 [15]) provide post-Omicron insights, supporting antimicrobial stewardship needs.
4.2. Context of Antimicrobial Resistance
The elevated MRSA (36% vs. 25% pre-pandemic [33]) and ESBL (31%) rates likely reflect increased empirical antibiotic use and disrupted infection control during pandemic surges, consistent with WHO GLASS data for low- and middle-income countries (LMICs) [31]. These rates exceed pre-pandemic European estimates (ECDC, 2023 [33]). In ICUs, multidrug-resistant (MDR) Gram-negative organisms reached 40–45% in some cohorts [6,9,14], amplifying AMR challenges. However, retrospective designs in 12/22 studies may overestimate AMR due to selective sampling in sicker patients, while the predominance of high-income country studies (e.g., USA, Italy [3,7,16,17]) may underestimate AMR compared to LMICs, where resistance is typically higher due to variable infection control practices [31,34]. The predominance of Gram-negative pathogens (Klebsiella pneumoniae 26%, Acinetobacter baumannii 21%) aligns with pre-COVID-19 ICU BSI trends but underscores the pandemic’s exacerbation of resistance [33]. Geographical variations, particularly for Acinetobacter baumannii, showed higher resistance in Asia-Pacific and Latin America [4,20,22] compared to North America and Europe [3,7,16,17], reflecting regional prescribing patterns. For Pseudomonas aeruginosa, regional differences in resistance across Chinese provinces suggest local practices influence patterns [35]. Fungal BSIs, such as Candida spp., may be underreported (grouped under ‘other pathogens,’ 22%), with recent evidence suggesting increased candidemia in severe COVID-19 patients, warranting further investigation [35].
4.3. Heterogeneity in BSI Prevalence
Moderate heterogeneity (I^2^ = 50%) in BSI prevalence likely stems from differences in diagnostic criteria, with CDC’s stricter requirement of two positive blood cultures for contaminants potentially underestimating prevalence compared to ECDC’s broader clinical and laboratory criteria (meta-regression, p = 0.05). This variability particularly affects classification of coagulase-negative staphylococci (CoNS), where clinical correlation is essential. Subgroup analyses by geographic region showed slight variations: Europe (7.8%), North America (8.5%), Asia-Pacific (9.0%), and Latin America (10.2%) (see Section 3.2), possibly due to regional AMR and infection control differences [34]. Prevalence was stable across early (2020–2021, 8.0%) and later (2022–2025, 8.5%) pandemic phases, suggesting persistent infection prevention challenges. Sensitivity analyses excluding non-standard definitions confirmed robust estimates (see Table S3). Future studies should adopt ECDC criteria for greater sensitivity and report CoNS validation to enhance comparability.
4.4. Risk Factors and Clinical Implications
Factors associated with BSIs include mechanical ventilation (OR: 2.6), immunosuppression (OR: 2.3), and corticosteroid use (OR: 2.4), suggesting invasive procedures and immune compromise increase risk [3,6,17,20,23,24]. Pediatric MIS-C was linked to higher BSI risk (OR: 2.4, n = 3 studies [19,20,22]). These observational associations do not confirm causation due to potential confounders like disease severity. Clinicians should prioritize infection prevention, early BSI detection, and targeted antimicrobials (e.g., vancomycin for MRSA, carbapenems for ESBL) based on local resistance profiles.
4.5. Strengths and Limitations
This meta-analysis has several strengths, including a large sample size (~123,500 patients, ~602,000 blood cultures) across 22 studies from 12 countries [3,4,6,7,8,10,11,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28], inclusion of prospective and retrospective designs, and adherence to PRISMA 2020 guidelines [12]. Moderate heterogeneity (I^2^ = 50%) reflects diverse populations and settings, enhancing generalizability. However, limitations include moderate heterogeneity due to differences in CDC and ECDC diagnostic criteria (meta-regression, p = 0.05), which may affect prevalence estimates. Retrospective designs in 12/22 studies may introduce selection bias, particularly from selective blood culture sampling in critically ill patients. Pediatric data are limited to three studies [20,26,27], precluding firm conclusions about MIS-C and BSI risk. Most studies originated from high-income countries (e.g., USA, Italy [3,7,16,17]), potentially underestimating AMR in LMICs, where resistance is typically higher due to resource constraints and variable infection control practices [31]. For instance, WHO GLASS data report elevated ESBL rates in LMICs [31], suggesting our AMR estimates (e.g., 31% ESBL) may not fully capture the burden in these settings. The absence of a formal GRADE assessmentlimits confidence in pooled estimates. Future studies should incorporate GRADE, prioritize LMIC representation, and use harmonized ECDC criteria to enhance comparability.
4.6. Implications for Practice and Research
The convergence of COVID-19 and AMR highlights the urgency of strengthening infection prevention and control (IPC) programs, particularly in ICUs. Rapid diagnostics (e.g., next-generation sequencing) and antimicrobial stewardship, aligned with WHO’s AMR action plan [32,36], are critical to mitigate BSIs. Global health policies should integrate AMR surveillance with standardized BSI definitions to enhance data comparability. Prospective, multicenter studies with harmonized criteria and a focus on pediatric populations are essential to address data gaps and guide future pandemics.
5. Conclusions
This systematic review and meta-analysis of 22 studies (~123,500 patients, ~602,000 blood cultures) confirms that bloodstream infections (BSIs) are a frequent and severe complication of COVID-19. The pooled prevalence was 8.2%, with higher rates in ICU settings (12.5%) compared to non-ICU populations (5.2%). Pediatric cohorts (Fallah et al., 2024 [22]; Lai et al., 2023 [26]; Moffitt et al., 2023 [27]) showed a prevalence of 10.8%, though limited evidence precludes firm conclusions. While MIS-C appeared associated with an increased risk of BSI, evidence is limited to three studies. Therefore, pediatric-specific findings should be interpreted with caution until validated by larger, multicenter cohorts.
BSIs were associated with a 2.6-fold increased risk of mortality, prolonged hospital stays (+6.8 days), and higher ICU admissions (OR: 3.1). Multidrug-resistant organisms—including MRSA (36%), ESBL-producing Enterobacterales (31%), and carbapenem-resistant Gram-negative pathogens—dominated the microbiological profile.
Limitations of the present review include moderate heterogeneity (CDC vs. ECDC diagnostic criteria), the predominance of retrospective designs (12/22 studies), and limited pediatric evidence. Certainty assessment (GRADE) was not performed, which may limit confidence in pooled estimates.
Strengthened infection prevention, antimicrobial stewardship, and harmonized diagnostic definitions are urgently needed. Future research should prioritize multicenter, prospective studies, particularly in low- and middle-income countries, and dedicated pediatric cohorts to address current knowledge gaps.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chu H. Chan J.F.-W. Yuen T.T.-T. Shuai H. Yuan S. Wang Y. Hu B. Yip C.C. Tsang J.O. Huang X. Comparative tropism, replication kinetics, and cell damage profiling of SARS-Co V-2 and SARS-Co V with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: An observational study Lancet Microbe 20201 e 14e 2310.1016/S 2666-5247(20)30004-532835326 PMC 7173822 · doi ↗ · pubmed ↗
- 2Wu Z. Mc Googan J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention JAMA 20203231239124210.1001/jama.2020.264832091533 · doi ↗ · pubmed ↗
- 3Giacobbe D.R. Battaglini D. Ball L. Brunetti I. Bruzzone B. Codda G. Crea F. De Maria A. Dentone C. Di Biagio A. Bloodstream Infections in Critically Ill Patients with COVID-19Eur. J. Clin. Investig.202050 e 1331910.1111/eci.1331932535894 PMC 7323143 · doi ↗ · pubmed ↗
- 4Pourajam S. Kalantari E. Talebzadeh H. Mellali H. Sami R. Soltaninejad F. Amra B. Sajadi M. Alenaseri M. Kalantari F. Secondary Bacterial Infection in COVID-19 Patients Front. Cell. Infect. Microbiol.20221278413010.3389/fcimb.2022.78413035281440 PMC 8904895 · doi ↗ · pubmed ↗
- 5Russell C.D. Fairfield C.J. Drake T.M. Turtle L. Seaton R.A. Wootton D.G. Sigfrid L. Harrison E.M. Docherty A.B. de Silva T.I. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study Lancet Microbe 20212 e 354e 36510.1016/S 2666-5247(21)00090-234100002 PMC 8172149 · doi ↗ · pubmed ↗
- 6Massart N. Maxime V. Fillatre P. Razazi K. FerréA. Moine P. Legay F. Voiriot G. Amara M. Santi F. Characteristics and Prognosis of Bloodstream Infection in Patients with COVID-19 Admitted in the ICU: An Ancillary Study of the COVIDICU Study Ann. Intensive Care 20211118310.1186/s 13613-021-00971-w 34952960 PMC 8708508 · doi ↗ · pubmed ↗
- 7Shukla B.S. Warde P.R. Knott E. Arenas S. Pronty D. Ramirez R. Rego A. Jimenez G.S. Larson E.L. Pereira M.R. Bloodstream Infection Risk, Incidence, and Deaths for Adults Hospitalized with COVID-19Emerg. Infect. Dis.2021272551255810.3201/eid 2710.21053834352195 PMC 8462325 · doi ↗ · pubmed ↗
- 8Ntziora F. Giannitsioti E. Bloodstream infections in the era of the COVID-19 pandemic: Changing epidemiology of antimicrobial resistance in the intensive care unit J. Intensive Med.2024426928010.1016/j.jointm.2023.12.00439035613 PMC 11258508 · doi ↗ · pubmed ↗