A Rare Case of Hepatocellular Carcinoma With Osteoclast-Like Giant Cells: Favorable Outcome Following Early Surgical Resection
Ryohei Aoyama, Kentaro Yasuchika, Masaki Yamada, Naoto Nakamura, Satoshi Yokoyama

TL;DR
A rare case of liver cancer with giant cells was successfully treated with early surgery, showing a good outcome.
Contribution
Reports a rare HCC case with osteoclast-like giant cells that had a favorable outcome after early surgical resection.
Findings
The patient had early-stage HCC with osteoclast-like giant cells detected during routine surveillance.
Surgical resection led to uneventful recovery and no recurrence after two years of follow-up.
Early diagnosis and treatment may improve outcomes for this rare HCC variant.
Abstract
Hepatocellular carcinoma (HCC) containing osteoclast-like giant cells (OGCs) is an exceptionally rare histological variant, with few cases reported in the literature. These tumors typically exhibit aggressive behavior and a poor prognosis, often presenting at advanced stages. We report the case of a 71-year-old male with early-stage HCC harboring OGCs, incidentally detected during routine surveillance for prior colon cancer. Imaging findings were consistent with conventional HCC, and laparoscopic partial hepatectomy was performed. Histopathological examination revealed well-differentiated HCC with scattered OGCs. The patient recovered uneventfully and has remained recurrence-free for two years postoperatively, as confirmed by routine radiological surveillance. This case highlights the potential for favorable outcomes in HCC with OGCs when diagnosed and treated at an early stage. Further…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
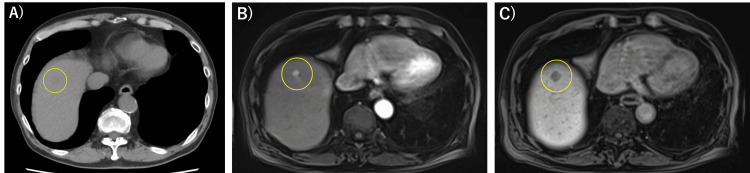 Figure 1
Figure 1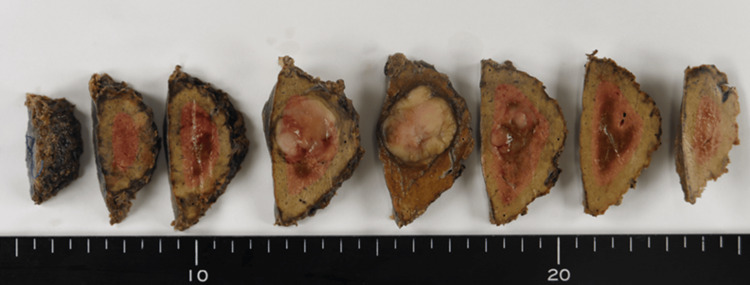 Figure 2
Figure 2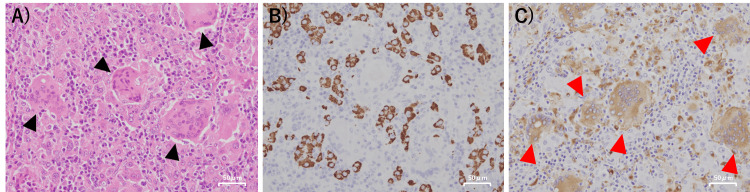 Figure 3
Figure 3| Parameter | Value | Reference Range | Unit |
| WBC | 5400 | 3300–86,000 | /μL |
| Hb | 14.7 | 13.7–16.8 | g/dL |
| PLT | 140,000 | 158,000–348,000 | /μL |
| PT% | 25.3 | 74.4–120 | % |
| PT-INR | 2.32 | ||
| APTT | 33.8 | 24.1-31.7 | sec |
| Alb | 4.1 | 4.1–5.1 | g/dL |
| AST | 30 | 13–30 | U/L |
| ALT | 39 | 10-42 | U/L |
| T-Bil | 0.4 | 0.4–1.5 | mg/dL |
| BUN | 17 | 8–20 | mg/dL |
| Cre | 1.02 | 0.65–1.07 | mg/dL |
| CRP | 0.12 | <0.14 | mg/dL |
| AFP | 4 | <10 | ng/mL |
| CEA | 10.7 | <5.0 | ng/mL |
| PIVKA-II | 28,606.7 | <40 | mAU/mL |
| No | Author, Ref. | Year | Age (Years) | Sex | Diagnosis | Tumor Size (cm) | Cirrhosis | Treatment | Prognosis |
| 1 | Kuwano et al. [ | 1984 | 54 | Male | HCC with OGC | 12 | Yes | Operation | Death (42 days) |
| 2 | Hood et al. [ | 1990 | 37 | Female | Hepatic giant cell carcinoma | - | No | Operation | Death (3 months) |
| 3 | McCluggage et al. [ | 1993 | 71 | Male | HCC with OGC | - | Yes | - | Death (1 month) |
| 4 | Sasaki et al. [ | 1997 | 42 | Male | Sarcomatoid HCC with OGC | 6 | Yes | Operation | Death (28 days) |
| 5 | Ikeda et al. [ | 2003 | 76 | Male | Sarcomatoid HCC with OGC | - | Yes | Trans-arterial embolization (TAE) + Operation | Death (5 months) |
| 6 | Tanahashi et al. [ | 2009 | 74 | Female | Combined HCC and OGC | 10 | No | Operation | Death (4 months) |
| 7 | Lee [ | 2014 | 64 | Male | Sarcomatoid HCC with OGC | 6 | Yes | Operation | Recurrence (2 months) |
| 8 | Dioscoridi et al. [ | 2015 | 74 | Female | HCC with OGC | 10 | No | Operation | Death (4 months) |
| 9 | Dahm [ | 2015 | 68 | Male | Sarcomatoid HCC with OGC | 6 | No | Operation | Recurrence (3 months) |
| 10 | Tsukimoto et al. [ | 2022 | 70 | Male | Recurrent HCC with OGC | 2.1 | Yes | Operation | No recurrence (a year and a half) |
| 11 | Frittoli et al. [ | 2024 | 77 | Male | HCC with OGC | 3.8 | Yes | Operation | Recurrence (6 months) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Cancer-related Molecular Pathways · Bone health and treatments
Introduction
Tumors containing osteoclast-like giant cells (OGCs) are rare entities that have been reported in various non-osseous organs, including the ovary, pancreas, urinary tract, thyroid gland, and liver [1]. These multinucleated giant cells resemble osteoclasts morphologically, but their histogenesis remains unclear, with possibilities including reactive transformation or neoplastic origin [2].
In the liver, hepatocellular carcinoma (HCC) is the most prevalent primary malignancy, accounting for approximately 75-85% of all liver cancers globally [3]. HCC is typically suspected based on imaging findings such as arterial phase hyperenhancement and portal venous washout, elevated tumor markers, and underlying risk factors such as chronic liver disease or viral hepatitis. Conventional HCC is the most common histologic subtype and is classified into well, moderately, and poorly differentiated forms based on the degree of cellular differentiation. However, HCC with OGCs is extremely rare, and only a limited number of cases have been reported. This variant may also occur in cirrhotic liver but is typically associated with aggressive behavior, rapid progression, and poor prognosis, often presenting at advanced stages [1,4]. The imaging findings of HCC with OGCs are nonspecific and resemble those of conventional HCC [4]. Due to its rarity, the clinical characteristics, optimal management strategies, and prognostic implications of HCC with OGCs remain poorly defined. Surgical resection is considered one of the treatment options for HCC, but its role in OGC-containing variants has not been well established.
Here, we present a case of HCC with OGCs that was successfully treated with laparoscopic resection, resulting in long-term survival. To our knowledge, this represents only the second documented case of extended survival following surgical intervention for this rare variant, highlighting its potential for curative treatment.
Case presentation
A 71-year-old Japanese man was admitted to our hospital for evaluation and treatment of a liver tumor. He had undergone right hemicolectomy for ascending colon cancer (tub2, pT2N0M0, pStage I) at the age of 69. During routine postoperative surveillance, plain computed tomography (CT) showed a low-density mass in the right hepatic lobe, suggestive of a metastatic lesion from the prior colon cancer (Figure 1A). Contrast-enhanced CT was not performed due to the patient’s known allergy to CT contrast agents.
The patient had achieved a sustained virological response for chronic hepatitis C and was receiving warfarin therapy for atrial fibrillation. He was hemodynamically stable on admission. Laboratory data are summarized in Table 1. Notably, the serum carcinoembryonic antigen (CEA) level was elevated at 10.7 ng/mL (reference < 5.0 ng/mL), and des-γ-carboxy prothrombin (DCP) was markedly elevated at 28,606.7 mAU/mL (reference < 40 mAU/mL). These elevations were suspected to be influenced by the patient’s active smoking status and concurrent warfarin therapy.
Gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging (Gd-EOB-DTPA MRI) revealed a 2 cm lesion in segment 8 of the liver, demonstrating arterial phase hyperenhancement and hepatobiliary phase hypointensity, consistent with typical imaging features of HCC (Figure 1B,C). Based on these imaging findings and his history of HCV infection, the lesion was considered more consistent with a newly developed HCC rather than a hepatic metastasis from previously resected ascending colon adenocarcinoma. Due to the risk of tumor cell seeding associated with needle biopsy, we did not perform a biopsy. Instead, we proceeded with a laparoscopic partial liver resection of segment 8.
Plain CT and Gd-EOB-DTPA-Enhanced MRI Images(A) Plain CT image: a low-density mass was found in the right lobe of the liver (yellow circle). (B) Gd-EOB-DTPA-enhanced MRI (arterial phase) showing a 2-cm hyperenhancing lesion in segment 8 of the liver (yellow circle). (C) Hepatobiliary phase image demonstrating hypointensity of the same lesion (yellow circle).Gd-EOB-DTPA MRI: gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging.
The resected specimen demonstrated a solid and well-defined tumor measuring 2.2 × 2.0 × 1.8 cm (Figure 2). Histopathologically, it was diagnosed as well-differentiated HCC. In addition, OGCs were observed in the background (Figure 3A). Immunohistochemical staining demonstrated diffuse HepPar1 positivity in HCC cells and strong CD68 expression in OGCs (Figure 3B,C). Based on these findings, we diagnosed the tumor as a newly developed HCC with OGCs, rather than a metachronous metastasis from the previously resected ascending colon adenocarcinoma. No vascular or bile duct invasion was observed, and surgical margins were negative.
Macroscopic Findings of the Resected SpecimenA solid and well-defined tumor 2.2 × 2.0 × 1.8 cm in size was observed.
Microscopic Findings of the Resected Specimen(A) Hematoxylin and eosin (H.E) staining (×200) showing trabecular proliferation of HCC cells with numerous OGCs in the background (black arrows). (B) Immunohistochemical staining for HepPar1 demonstrating diffuse positivity in HCC cells (×200). (C) Immunohistochemical staining for CD68 showing positivity in OGCs (×200). Red arrows indicate representative CD68-positive giant cells.HCC: hepatocellular carcinoma, OGC: osteoclast-like giant cell, H.E.: hematoxylin and eosin, HepPar-1: hepatocyte paraffin 1, CD68: cluster of differentiation 68.
The patient was discharged on postoperative day 9 and has remained recurrence-free for two years, as confirmed by routine radiological surveillance.
Discussion
HCC is the most common primary liver malignancy, but HCC with OGCs is an extremely rare variant. This tumor type was first reported by Kuwano et al. in 1984 [5].
The imaging findings of HCC with OGCs are not specific and generally show the same radiological features as conventional HCC [4], making radiological differentiation challenging. In the present case, the Gd-EOB-DTPA MRI findings were also suggestive of typical HCC. Therefore, histopathological evaluation remains indispensable for establishing a definitive diagnosis. Although HCC is commonly associated with underlying liver disease, several cases of HCC with OGCs have been reported in patients without prior hepatopathies [6-9], further complicating the diagnostic process.
The treatment approach for this tumor is similar to that of conventional HCC, and surgical resection is an option. However, HCC with OGCs typically exhibits highly aggressive clinical and biological characteristics, leading to a poor prognosis even after surgical resection [1].
The origin of OGCs remains uncertain. Previous reports have proposed that OGCs represent reactive histiocytic cells rather than true malignant components, based on their immunohistochemical profile. Specifically, OGCs consistently express the histiocytic marker CD68 and show a low Ki-67 proliferation index, suggesting limited proliferative activity and a non-neoplastic nature [2,7]. Additionally, OGCs in the liver demonstrate an expression pattern similar to osteoclasts in bone, including markers such as CD68, receptor activator of nuclear factor-kappa B (RANK), and RANK ligand (RANKL). These findings suggest that the histogenesis of OGC formation in liver cancer may follow mechanisms similar to those of bone osteoclastogenesis [2]. To the best of our knowledge, only 11 cases of HCC with OGCs have been reported in the English literature (Table 2) [1,2,4-12].
Among the patients, eight were male and three were female, with ages ranging from 37 to 77 years (median age, 70 years). Seven patients had underlying hepatopathies, while four did not. The tumors measured between 2.1 and 12 cm in diameter. Sarcomatous transformation of HCC was observed in four cases. Sarcomatous transformation is considered a form of tumor dedifferentiation, and OGCs are occasionally observed in poorly differentiated areas, suggesting a possible association. Surgical resection was performed in 10 patients. However, the prognosis of previous cases was very poor, with 10 patients experiencing recurrence or death within six months after treatment. Only one case has been reported to achieve long-term survival, with a tumor size of 2.1 cm, which was relatively small. Similarly, in our case, the tumor size was also small. These findings suggest that tumor size may be a prognostic factor, underscoring the importance of early detection and timely intervention.
While the presence of OGCs in HCC has been documented in rare cases, their biological and clinical significance remains unclear. This report is limited by the rarity of this histological subtype and the lack of statistically supported data. In our case, the presence of OGCs may represent an incidental histological finding without a clear impact on tumor behavior or prognosis.
Conclusions
HCC with OGCs is an uncommon histological subtype typically associated with aggressive behavior and poor prognosis. However, this case suggests that early detection and timely surgical intervention can lead to favorable long-term outcomes, highlighting the importance of routine surveillance in at-risk individuals.
Continued documentation and analysis of similar cases are essential to better characterize the clinicopathological features of this variant and to inform future diagnostic and therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Recurrent hepatocellular carcinoma with osteoclast-like giant cells: a case report J Med Case Rep Tsukimoto M Sugimoto K Shigefuku R Sugimoto R Yuasa H Uchida K Yamamoto N 1421620223536127610.1186/s 13256-022-03355-1PMC 8974057 · doi ↗ · pubmed ↗
- 2Hepatocellular carcinoma with osteoclast-like giant cells: possibility of osteoclastogenesis by hepatocyte-derived cells Pathol Int Ikeda T Seki S Maki M 4504565320031282861010.1046/j.1440-1827.2003.01503.x · doi ↗ · pubmed ↗
- 3Hepatocellular carcinoma: a comprehensive review Diseases Amin N Anwar J Sulaiman A Naumova NN Anwar N 13202510.3390/diseases 13070207 PMC 1229380940709997 · doi ↗ · pubmed ↗
- 4A unique case of lymphoepithelioma-like HCC with osteoclast-like giant cells: CT imaging features with pathologic correlations Clin J Gastroenterol Frittoli B Castaldo A Santarsiere M 1121171720243786465510.1007/s 12328-023-01871-1PMC 10830663 · doi ↗ · pubmed ↗
- 5Hepatocellular carcinoma with osteoclast-like giant cells Cancer Kuwano H Sonoda T Hashimoto H Enjoji M 837842541984633162910.1002/1097-0142(19840901)54:5<837::aid-cncr 2820540513>3.0.co;2-8 · doi ↗ · pubmed ↗
- 6Hepatic giant cell carcinoma. An ultrastructural and immunohistochemical study Am J Clin Pathol Hood DL Bauer TW Leibel SA Mc Mahon JT 111116931990215300110.1093/ajcp/93.1.111 · doi ↗ · pubmed ↗
- 7Combined hepatocellular carcinoma and osteoclast-like giant cell tumor of the liver: possible clue to histogenesis Pathol Int Tanahashi C Nagae H Nukaya T Hasegawa M Yatabe Y 8138165920091988343310.1111/j.1440-1827.2009.02450.x · doi ↗ · pubmed ↗
- 8Hepatocellular carcinoma with osteoclast-like giant cells: report of the seventh case in the literature Case Rep Surg Dioscoridi L Bisogni D Freschi G 836105201520152579313910.1155/2015/836105 PMC 4352421 · doi ↗ · pubmed ↗