A Phase III Clinical Trial of Immunogenicity and Safety of Meningococcal A and C Polysaccharide Conjugate Vaccine in Infants Aged 3–5 Months
Liwei Shi, Zhe Zhang, Yuqing Liu, Maoguang Li, Weicai Lu, Yue Yang, Dan Zhao, Bin Wang, Wenjian Fang

TL;DR
A new meningococcal vaccine for infants aged 3–5 months was found to be safe and effective, with strong immune responses and no major side effects.
Contribution
The study demonstrates the non-inferiority of a new meningococcal A and C conjugate vaccine compared to a control vaccine in infants.
Findings
Seroconversion rates for meningococcal groups A and C exceeded 90% after primary immunization in pre-vaccination antibody-negative infants.
After booster immunization, antibody levels against groups A and C were significantly higher than before the booster.
Adverse reactions were mainly mild fevers with no significant difference between the experimental and control groups.
Abstract
Background/Objectives: This study aimed to evaluate the immunogenicity and safety of a Meningococcal A and C Polysaccharide Conjugate Vaccine in 3–5-month-old infants. A single-center, randomized, blinded, positive-controlled phase III clinical trial was conducted in Binyang County, Guangxi Zhuang Autonomous Region, China. Infants aged 3–5 months were randomly assigned to the experimental or control group at a 1:1 ratio. Both groups received 3 primary doses with a 1-month interval between each dose, and a booster dose administered at 18 months of age. Seroconversion rate, seropositivity rate, and GMT of bactericidal antibodies against Neisseria meningitidis groups A and C were assessed, along with adverse reactions within the full course of primary immunization and 30 days after booster immunization. Results: After primary immunization, in the experimental group’s pre-vaccination…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
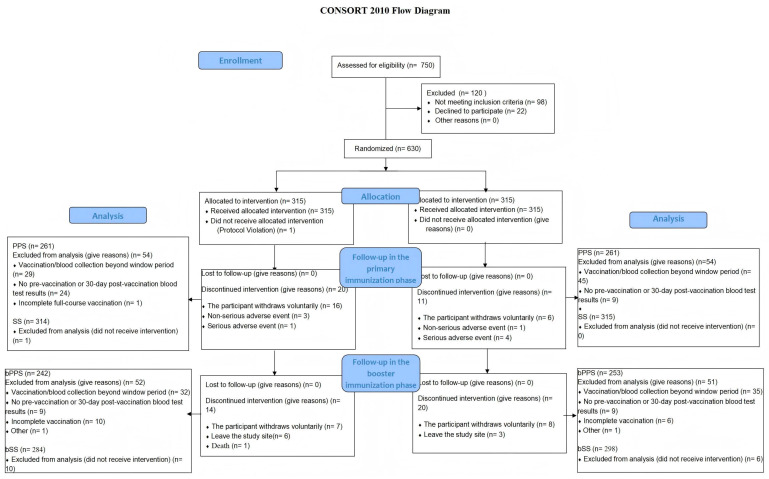 Figure 1
Figure 1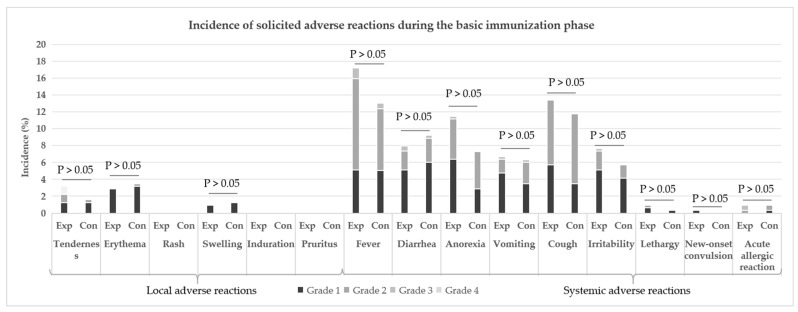 Figure 2
Figure 2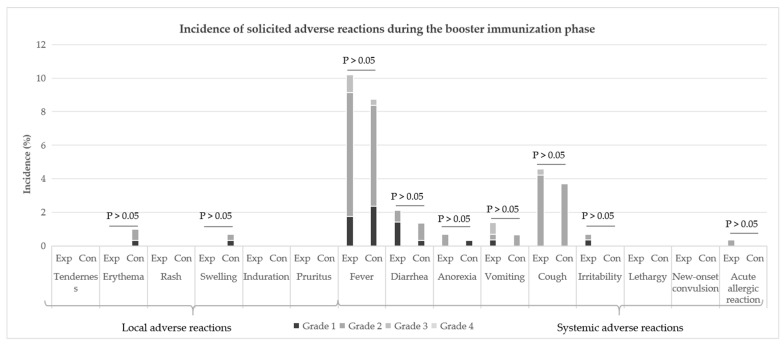 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Pneumonia and Respiratory Infections · Influenza Virus Research Studies
1. Introduction
The Gram-negative aerobic diplococcus Neisseria meningitidis (Nm) is the etiologic agent responsible for meningococcal disease. According to the different structure of the capsule, Nm has been classified into at least 12 different capsular groups, among which serogroups A, B, C, W, Y and X are the main causes of meningococcal meningitis [1,2]. Nm is the culprit behind invasive meningococcal disease (IMD), an uncommon infection characterized by rapid progression, potential lethality, and the risk of severe long-term effects in those who survive [3,4]. While IMD most commonly manifests as meningitis, septicemia, or a combination of both, it can also take other forms, including septic arthritis, pericarditis, and pneumonia [5]. IMD can lead to significant morbidity and mortality, and may also cause permanent sequelae, such as brain damage and the amputation of limbs or fingers [6,7]. In the era when the vaccine was not widely available, China had five pandemics of meningococcal disease, all of which were nationwide pandemics, occurring every 8–10 years and lasting about 3–4 years each time [8]. Nm serogroup A is the most common serogroup involved in meningococcal pandemics. However, between 2003 and 2004, the ST4821 strain of serogroup C emerged in Anhui Province, China, triggering a large-scale meningitis outbreak and this strain exhibits higher invasiveness, leading to severe complications and a higher case fatality rate compared to serogroup A [9]. Meningococcal Group A and C Polysaccharide Vaccines have been routinely administered nationwide since 2008.
IMD incidence in infants is 2–5 times higher than in children aged 1 to 4 years, with the rate being 10 times greater still when compared to individuals in older age groups [10]. Furthermore, the clinical manifestations of IMD in infants are mostly atypical. In the early stages, symptoms are often limited to ordinary fever or similar to those of non-specific viral infections, which easily leads to delayed diagnosis and treatment; moreover, the disease progresses rapidly, often resulting in death within a few hours, so vaccination for infants and young children has become a top priority [11]. As meningococcal polysaccharide antigen is a T cell-independent antigen and does not require T cell helper when stimulating B cells to produce antibodies, infants under 2 years of age have a weak immune response, only inducing a transient immune response and poor response to a booster dose [12,13]. Conjugate vaccines hold distinct advantages over polysaccharide vaccines: they are capable of triggering a protective immune response in children younger than 2 years old, offer protection that lasts for a longer period, and can enhance antibody levels when additional booster doses are administered [14].
Meningococcal A and C Polysaccharide Conjugate Vaccine produced by Beijing Zhifei Lvzhu Biopharmaceutical Co., Ltd. (Beijing, China) is a new generation of conjugate vaccine developed on the basis of the original liquid Meningococcal A and C Polysaccharide Conjugate Vaccine. The conjugate vaccine is a freeze-dried product without adjuvant and provides immune protection against group A and C meningococcal meningitis for people aged 3 months and above. The China former State Food and Drug Administration (SFDA) approved the clinical study of this product in the age-eligible population in September 2015 (Approval Letter for Drug Clinical Trial, Approval No.: 2015L02563). This study reports the results of a clinical trial in infants aged 3–5 months, who received primary immunization following the 0-, 1-, and 2-month schedule, with a booster dose administered at 18 months of age.
2. Materials and Methods
2.1. Participants and Recruitment
This study is a single-center, randomized, blinded, positive-controlled phase III clinical study. Infants aged 3–5 months are being recruited in Binyang County, Guangxi Zhuang Autonomous Region, People’s Republic of China. The eligibility criteria included the following: full-term infants (born between 37 and 42 weeks of gestation) with a birth weight ranging from 2500 g to 4000 g; axillary body temperature < 37.5 °C; written informed consent forms signed by their legal guardians; families capable of complying with the requirements of the clinical trial protocol; no history of vaccination with Meningococcal A and C Polysaccharide Conjugate Vaccine; no history of receiving other live attenuated vaccines within 14 days prior to the vaccination; and no history of receiving other inactivated vaccines within 7 days prior to the vaccination. This study was conducted after being reviewed and approved by the Ethics Committee of Guangxi Zhuang Autonomous Region (Approval Letter No.: GXIRB2020-0067; Date: 29 December 2020) and has been registered at ClinicalTrials.gov (NCT06314659). All procedures and results of the study were reported in compliance with the Consolidated Standards of Reporting Trials (CONSORT 2025).
2.2. Vaccines and Immunization Procedure
The study vaccine was Meningococcal A and C Polysaccharide Conjugate Vaccine (lyophilized form, 20 μg/vial, batch number: Y20200701) produced by Beijing Zhifei Lvzhu Biopharmaceutical Co., Ltd. The control vaccine in the basic immunization phase (control vaccine 1) was Meningococcal A and C Polysaccharide Conjugate Vaccine (lyophilized form, 20 μg/vial, batch number: C202008009) manufactured by Yuxi Walvax Biotechnology Co., Ltd. (Kunming, China). The control vaccine in the booster immunization phase (control vaccine 2) was Meningococcal A and C Polysaccharide Conjugate Vaccine manufactured by Chengdu Olymvax Biopharmaceuticals Inc. (Chengdu, China). All three investigational vaccines contain 10 μg each of Nm group A and group C polysaccharides (conjugated to tetanus toxoid) per 0.5 mL dose. And all are administered by intramuscular injection in the deltoid muscle on the lateral upper arm. A 3-dose primary immunization is given following the 0, 1, and 2-month schedule, and a booster dose is administered at 18 months of age.
2.3. Immunogenicity
All subjects underwent blood collection before the first immunization, 30 days after the primary immunization, before the booster immunization at 18 months of age, and 30 days after the booster immunization. Serum antibody assay was conducted by the National Institutes for Food and Drug Control (NIFDC). The serum bactericidal assay (SBA) was performed using rabbit complement via the triphenyltetrazolium chloride (TTC) method to measure the antibodies against Nm serogroups A and C in the subjects’ serum. Antibody levels of the subjects were evaluated at 30 days after primary immunization. The evaluation indicators included following items: (1) antibody seroconversion rate, which refers to the proportion of subjects with a pre-immunization antibody titer against Nm serogroup A or C of <1:8 who achieved a post-immunization antibody titer of ≥1:8; (2) post-immunization antibody geometric mean titer (GMT); (3) the antibody seropositivity rate (antibody titer ≥1:8 and ≥1:128). Meanwhile, the antibody levels of the subjects were investigated before booster immunization and 30 days after the booster immunization.
2.4. Safety
All subjects were followed up through a combination of regular follow-up visits and active reporting after each vaccine dose, with all vaccine-related adverse reactions (ARs) collected within 0–30 days post each dose. ARs occurring after vaccination were graded for severity in accordance with the Guidelines for Grading Standards of ARs in Clinical Trials of Vaccines for Preventive Use issued by China SFDA, which are categorized as Grade 1 (mild), Grade 2 (moderate), Grade 3 (severe), and Grade 4 (potentially life-threatening). All subjects were monitored for the occurrence of serious adverse events (SAE) until 6 months after the primary immunization and 1 month after the booster immunization.
2.5. Statistical Analysis
During the study, data collection was conducted using an Electronic Data Capture (EDC) system, with original data also preserved in paper documents. All statistical analyses were performed using Statistical Analysis System (SAS) 9.4 or later versions. When the post-vaccination seroconversion rates for both Nm serogroups A and C are expected to be 90%, it has been calculated that 252 evaluable participants per group are required. With the Bonferroni method applied for correction, this sample size enables the test to achieve a 95% power under the conditions of a one-sided significance level (α) of 0.025 and a clinical non-inferiority margin of −10%. For Serogroup A and C antibodies, post-vaccination seroconversion rates and antibody seropositivity rates were calculated for the experimental and control groups respectively. Their two-sided 95% confidence intervals (CIs) were computed via the Clopper-Pearson method, while the Miettinen-Nurminen method was used to calculate the rate difference (experimental-control group) and its two-sided 95% CI; inter-group differences were tested with the chi-square or Fisher’s exact test. For antibody GMT, data were first log-transformed, then a covariance analysis model was fitted to calculate the adjusted inter-group GMT ratio; meanwhile, log-transformed independent samples t-test was used to test inter-group GMT differences. For adverse reactions, we calculated the number of cases and incidence, and used Fisher’s exact test to compare differences between groups.
3. Results
3.1. Basic Information of Subjects
A total of 630 participants were enrolled in this trial, including 315 participants in the experimental group and 315 participants in the control group. There were 53.21% males and 46.79% females in the experimental group and 56.19% males and 43.81% females in the control group. The average age was 4.35 months in the experimental group and 4.32 months in the control group. There were no significant differences in gender or average age. See Figure 1 for details of participant screening, enrollment and completion of the clinical trial.
3.2. Immunogenicity Results
3.2.1. Primary Immunization Phase
Antibody seroconversion rate in pre-vaccination antibody-negative population
Among the pre-vaccination antibody-negative participants, the post-vaccination antibody seroconversion rates for serogroup A were 99.21% in the experimental group and 94.74% in the control group, respectively. For serogroup C, the post-vaccination antibody seroconversion rates were 91.54% in the experimental group and 89.96% in the control group, respectively. The antibody seroconversion rates for both serogroup A and serogroup C in the experimental group were non-inferior to those in the control group (with a non-inferiority margin of −10%) (Table 1).
Post-vaccination antibody GMT in pre-vaccination antibody-negative population
Among pre-vaccination antibody-negative participants, the post-vaccination GMTs of serogroup A antibody were 222.5 in the experimental group and 105.8 in the control group, respectively. Compared with the pre-vaccination levels, the fold increases in their GMT values were 219.5 and 105.2, respectively. For serogroup C antibody, the post-vaccination GMTs were 91.5 in the experimental group and 70.7 in the control group, while the fold increases relative to pre-vaccination GMT levels were 91.0 and 70.1, respectively. The adjusted post-vaccination antibody GMT ratio for both serogroup A and serogroup C in the experimental group were non-inferior to those in the control group (with a non-inferiority margin of 0.67) (Table 2).
Rate of post-vaccination antibody titer ≥1:128 in populations with pre-vaccination antibody negativity
In the pre-vaccination antibody-negative population, the rates of post-vaccination antibody titer ≥1:128 in the experimental group and the control group were 81.35% and 59.11% for serogroup A, and 64.62% and 53.67% for serogroup C, respectively. For both serogroup A and serogroup C, the seropositivity rates in the experimental group were significantly higher than those in the control group (p < 0.05) (Table 3).
3.2.2. Booster Immunization Phase
Seropositivity Rate in the Total Population
Before booster immunization, the total population of the experimental and control groups showed the following serogroup A antibody titer rates: 73.14% vs. 66.01% for titers ≥1:8, and 19.83% vs. 14.23% for titers ≥1:128. At 30 days post-booster immunization, the rate of serogroup A antibody titer ≥1:8 reached 100% in both groups, while the rate of titers ≥1:128 was 96.69% in the experimental group and 96.44% in the control group. No statistically significant differences in antibody seropositivity rates were observed between the two groups for serogroup A (p > 0.05).
For serogroup C, before booster immunization, the rate of antibody titer ≥1:8 in the total population was 31.40% in the experimental group and 17.39% in the control group—with the experimental group showing a significantly higher rate (p = 0.0003). However, there was no statistically significant difference in the rate of serogroup C antibody titer ≥1:128 between the two groups (1.24% vs. 0.40%, p > 0.05). At 30 days post-booster immunization, the rate of serogroup C antibody titer ≥1:8 was 93.39% in the experimental group and 90.12% in the control group, and the rate of titers ≥1:128 was 61.16% vs. 52.57%, respectively; there was no statistically significant differences in antibody seropositivity rates were noted between the experimental and control groups (p > 0.05) (Table 4).
GMT in the Total Population
Before booster immunization, the GMT of serogroup A antibody in the total population was 18.0 for the experimental group and 11.1 for the control group, with the experimental group showing a slightly higher value (p = 0.0051). At 30 days after booster immunization, the serogroup A antibody GMTs were 463.2 (experimental group) and 514.8 (control group), respectively, with no statistically significant difference between the two groups. However, compared with the pre-booster period, the GMTs increased by 25.7-fold in the experimental group and 46.3-fold in the control group, and the increase multiple in the experimental group was lower than that in the control group (p = 0.0003).
Prior to booster immunization, the serogroup C antibody GMT in the total population was 2.9 for the experimental group and 2.2 for the control group, where the experimental group had a higher GMT (p = 0.0362). At 30 days post-booster immunization, the serogroup C antibody GMTs were 98.1 (experimental group) and 77.7 (control group). Compared with the pre-booster period, the GMTs increased by 34.4-fold and 35.0-fold in the two groups, respectively. No statistically significant differences were observed between the experimental group and the control group in terms of either GMT value or increase multiple (p > 0.05) (Table 5).
3.3. Safety Results
3.3.1. Incidence of ARs
During the primary immunization phase, ARs in both the experimental group and the control group were mainly solicited ARs, with systemic ARs being the most common. In terms of symptom analysis, fever was the predominant systemic AR, with incidence rates of 16.56% in the experimental group and 12.38% in the control group; this was followed by symptoms such as cough, anorexia, and diarrhea. For local adverse reactions, erythema was the most frequent, with incidence rates of 2.87% (experimental group) and 3.49% (control group), respectively, and tenderness and swelling were the next most common symptoms (Figure 2). There were no statistically significant differences in the incidence rates of ARs for each symptom between the two groups (p > 0.05).
Similar to the primary immunization phase, the booster immunization phase was dominated by solicited systemic ARs. In terms of symptom analysis, fever was the primary systemic AR in both the experimental group and the control group, with incidence rates of 10.21% and 8.72%, respectively; this was followed by symptoms such as cough, diarrhea, and vomiting. No local ARs occurred in the experimental group, while the control group had 4 cases, specifically including 2 cases of erythema, 1 case of swelling, and 1 case of erythema accompanied by swelling (Figure 3). There were no statistically significant differences in the incidence rates of ARs for each symptom between the two groups (p > 0.05).
3.3.2. Severity of ARs
During the primary immunization phase, the incidences of grade 1, 2, 3, and 4 ARs in the experimental group were 27.71%, 26.75%, 2.23%, and 0%, respectively, while those in the control group were 22.22%, 23.17%, 1.27%, and 0.32%, respectively; the severity of ARs in both groups was mainly grade 1 and grade 2, with no statistically significant difference between the two groups (see Table 6). Specifically, 7 cases (2.23%) of grade 3 ARs occurred in the experimental group and 4 cases (1.27%) in the control group, primarily presenting as fever; no grade 4 or above ARs were observed in the experimental group, whereas 1 case of grade 4 serious AR (SAR) occurred in the control group, which was immune thrombocytopenia, and no SARs were reported in the experimental group (Figure 2 and Table 7).
During the booster immunization phase, the incidences of grade 1, 2, 3 and 4 ARs in the experimental group were 3.52%, 11.27%, 1.76% and 0%, respectively, while those in the control group were 3.36%, 12.08%, 0.34% and 0%, respectively. The severity of ARs was mainly grade 2. There was no statistical difference between the two groups (Table 7). The incidence of grade 3 and above ARs was low. There were 6 cases of grade 3 ARs in 5 patients in the experimental group, including 2 cases of fever, 2 cases of vomiting, and 1 case of fever and cough, respectively. There was 1 case of grade 3 fever in the control group. None of the patients had grade 4 and above ARs (Figure 3). No SARs occurred in either group (Table 7).
4. Discussion
Since the inclusion of group A meningitis polysaccharide vaccine in the routine immunization program in 1984, the cases of group A-related meningococcal meningitis have decreased significantly in China. In 2008, the inclusion of Meningococcal A and C Polysaccharide Vaccine in the Expanded Immunization Program in China further reduced the national incidence of IMD [15]. A systematic review and meta-analysis of IMD in China from 2010 to 2020 indicated that the epidemiology of IMD in China over this decade exhibited distinct serogroup distribution characteristics: among Nms strains associated with IMD, NmC (serogroup C Nm) accounted for the highest proportion (49.7%, 95%CI: 35.8–63.5%), followed by NmB (serogroup B Nm) at 30.2% (95%CI: 17.3–43.0%) and NmW (serogroup W Nm) at 23.8% (95%CI: 7.0–40.7%) [16]. Compared with people of other age groups, infants are a vulnerable population, and multiple factors collectively increase their risk of IMD—the immature immune system is a key reason for their high susceptibility to infections, while general IMD risk factors such as close contact with infected individuals, overcrowded living conditions, exposure to smoke, or concurrent viral infections also elevate their disease risk, so there is an urgent need to develop effective prevention and control strategies to protect infants from IMD [17].
A single-center, randomized, blinded, positive-controlled Phase III clinical trial was conducted in this study, targeting infants aged 3–5 months. The immunogenicity results of the primary immunization phase showed that, in the population with negative pre-immunization antibodies, both the post-immunization seroconversion rate and GMT of the experimental group were non-inferior to those of the control group. Furthermore, in this same pre-immunization antibody-negative population, the experimental group exhibited higher values than the control group in terms of the post-immunization seroconversion rate and GMT of serogroup A antibodies, and the rate of serogroup A and C antibody titer reaching ≥1:128 (p < 0.05). Overall, the vaccine in the experimental group demonstrated favorable immunogenicity outcomes.
Before booster immunization at 18 months of age, the rate of serogroup A and C antibody titer ≥ 1: 8 and GMT in the experimental group were higher than those in the control group, but they were significantly lower than those 30 days after primary immunization, especially when the seropositivity rate of serogroup C antibody was reduced to less than 30%, suggesting that booster immunization should be carried out timely. 30 days after booster vaccination, the antibody seropositivity rate and GMT of the whole population in the experimental group and the control group were similar. The serogroup A and serogroup C antibody levels after booster vaccination in the experimental group and control group were significantly increased compared with those before booster vaccination. The serogroup A antibody GMT was higher than the level on the 30th day after basic immunization, and the serogroup C antibody GMT was close to the level on the 30th day after basic immunization, indicating the necessity and rationality of one dose of booster vaccination at the age of 18 months for infants after basic immunization. In this trial, the control group underwent sequential vaccination with vaccines produced by different manufacturers during the booster immunization phase, and the results indicated favorable immunogenicity.
The safety results showed that during the primary immunization phase, both the experimental group and the control group were mainly affected by solicited systemic ARs. Fever was the most common among these reactions, with no statistically significant difference observed between the two groups and this is consistent with the most common ARs reported after vaccination with similar vaccines—most of these fevers were mild and transient [18], followed by other systemic reactions such as cough, anorexia, and diarrhea. For local ARs, erythema was the primary one, followed by tenderness and swelling. Regarding the incidence of all types of ARs in the experimental group and the control group, there were no statistically significant differences between the two groups. During the booster immunization phase, the most common AR in both the trial group and the control group was also fever, followed by cough, diarrhea, and vomiting and no local adverse reactions occurred in the trial group after booster immunization. In addition, the severity of adverse reactions during the primary immunization phase was mainly grade 1–2, and during the booster immunization phase was mainly grade 2. The incidence of grade 3 adverse reactions was low, and only 1 case of grade 4 SAR occurred in the control group, while no SAR occurred in the experimental group, reflecting the safety of the study vaccine.
The study results of other similar vaccines showed that the incidence of local, systemic and gastrointestinal reactions after vaccination with Meningococcal A and C Polysaccharide Conjugate Vaccine was low, mild and short-lasting, mainly redness, itching, pain, fever and vomiting [19]. Another clinical study of the similar vaccine products showed that the incidence of ARs occurring 30 days after vaccination from high to low were fever, diarrhea, injection site redness, irritability, injection site tenderness, lethargy, cough, nausea and vomiting, lactation or eating disorders, etc. [18]. The ARs in this trial were approximately the same as those of the like products, but the incidence of cough was slightly higher. Considering that the occurrence time of cough related to the study vaccine was in winter and spring, which was the season of high incidence of respiratory diseases, which affected the incidence of cough to a certain extent, and the incidence of cough was similar between the experimental group and the control group.
5. Conclusions
In this study, infants aged 3–5 months were given 3 doses of basic immunization according to the schedule of 0, 1, and 2 months, and 1 dose of booster immunization at 18 months of age. Results derived from this study demonstrated favorable immunogenicity and safety of the experimental vaccine. In the control group, vaccines from different manufacturers were used in the booster immunization phase, which also showed good immunogenicity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harrison O.B. Claus H. Jiang Y. Bennett J.S. Bratcher H.B. Jolley K.A. Corton C. Care R. Poolman J.T. Zollinger W.D. Description and nomenclature of Neisseria meningitidis capsule locus Emerg. Infect. Dis.20131956657310.3201/eid 1904.11179923628376 PMC 3647402 · doi ↗ · pubmed ↗
- 2Whittaker R. Dias J.G. Ramliden M. Ködmön C. Economopoulou A. Beer N. Pastore Celentano L. ECDC Network Members for Invasive Meningococcal Disease The epidemiology of invasive meningococcal disease in EU/EEA countries, 2004–2014 Vaccine 2017352034204110.1016/j.vaccine.2017.03.00728314560 · doi ↗ · pubmed ↗
- 3Aye A.M.M. Bai X. Borrow R. Bory S. Carlos J. Caugant D.A. Chiou C.S. Dai V.T.T. Dinleyici E.C. Ghimire P. Meningococcal disease surveillance in the Asia-Pacific region (2020): The global meningococcal initiative J. Infect.20208169871110.1016/j.jinf.2020.07.02532730999 · doi ↗ · pubmed ↗
- 4Booy R. Gentile A. Nissen M. Whelan J. Abitbol V. Recent changes in the epidemiology of Neisseria meningitidis serogroup W across the world, current vaccination policy choices and possible future strategies Hum. Vaccin. Immunother.20191547048010.1080/21645515.2018.153224830296197 PMC 6505668 · doi ↗ · pubmed ↗
- 5Pace D. Pollard A.J. Meningococcal disease: Clinical presentation and sequelae Vaccine 201230 B 3B 910.1016/j.vaccine.2011.12.06222607896 · doi ↗ · pubmed ↗
- 6Brooks R. Woods C.W. Benjamin D.K.Jr. Rosenstein N.E. Increased case-fatality rate associated with outbreaks of Neisseria meningitidis infection, compared with sporadic meningococcal disease, in the United States, 1994–2002 Clin. Infect. Dis.200643495410.1086/50480416758417 · doi ↗ · pubmed ↗
- 7Dinleyici E.C. Ciftci E. Somer A. Yilmaz D. Tezer H. A new quadrivalent meningococcal tetanus toxoid conjugate vaccine: Menquadfi® (MENACWY-TT)Hum. Vaccin. Immunother.202521251694910.1080/21645515.2025.251694940493501 PMC 12153384 · doi ↗ · pubmed ↗
- 8Xu M. Liang Z. Xu Y. Wang J. Chinese vaccine products go global: Vaccine development and quality control Expert Rev. Vaccines 20151476377310.1586/14760584.2015.101250325697690 · doi ↗ · pubmed ↗