Clinical Methods Supporting Initial Recognition of Early Post-Stroke Seizures: A Systematic Scoping Review
Clare Gordon, Hedley C. A. Emsley, Catherine Elizabeth Lightbody, Andrew Clegg, Catherine Harris, Joanna Harrison, Jasmine Wall, Catherine E. Davidson, Caroline L. Watkins

TL;DR
This review explores clinical methods for recognizing early post-stroke seizures and finds a lack of consistent evidence or guidelines.
Contribution
The study maps existing literature and highlights the need for targeted research on effective seizure recognition in acute stroke.
Findings
Only 30 papers met inclusion criteria, with limited empirical evidence on clinical methods for seizure recognition.
Current recommendations for monitoring seizures after stroke lack detail and consensus.
There is a clear need for targeted research into effective clinical identification strategies.
Abstract
Background: Stroke is a leading cause of seizures and epilepsy, both of which are linked to increased mortality, disability, and hospital readmissions. Early recognition and management of seizures in acute stroke are crucial for improving outcomes. Electroencephalogram (EEG) is not routinely used for post-stroke seizure monitoring and is typically initiated only after clinical suspicion arises, making bedside recognition essential. This scoping review aimed to map the existing literature on clinical methods used for identifying and observing early post-stroke seizures (EPSSs) at the bedside. Methods: We included literature involving adults with acute ischaemic stroke or primary intracerebral haemorrhage who were diagnosed or suspected of having inpatient EPSS. Searches were conducted in Medline, CINAHL, Embase, and the Cochrane Library for English-language publications up to April 2023.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
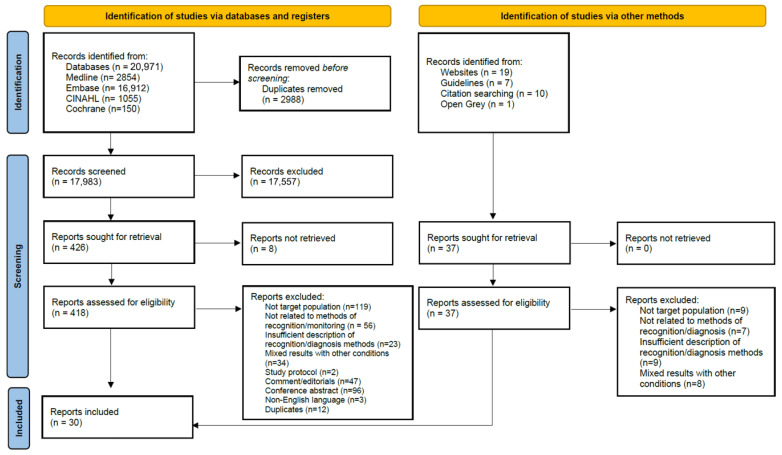 Figure 1
Figure 1| First Author, Year | Country | Study Type | Study Aim | Number of Participants | Male (%) | Ischaemic Stroke (%) | Clinical Method to Identify Seizure |
|---|---|---|---|---|---|---|---|
| France | Cohort | To evaluate whether thrombolysis is associated with an increased risk of early epileptic seizures in a cohort of consecutive patients who underwent an angiography in emergency care for cerebral ischaemia due to large-vessel occlusion | 1638 | 783 (48%) | 1638 (100%) | Clinical diagnosis. EEG used to diagnose seizures with atypical manifestation. EEG not used systematically. | |
| Italy | Cohort | To identify incidence and predictors of acute symptomatic seizures in a cohort of patients with first stroke | 714 | 399 (56%) | 609 (85%) | Direct observation by medical staff or reliable witness. Simple loss of consciousness or short episodes of confusion excluded. EEG only when indicated by medical staff. | |
| Italy | Cohort | To evaluate in a stroke unit the usefulness of a prolonged, at least 6 h, video-EEG recording (VEEG) in identifying episodes of non-convulsive status epilepticus after an acute ischemic stroke | 889 | 566 (64%) | 889 (100%) | Prolonged VEEG routinely within first 7 days of admission or immediately upon suspected seizure activity | |
| Portugal | Cohort | To compare the frequency of seizures and EEG abnormalities between stroke patients treated and not treated with thrombolysis | 151 | 89 (59%) | 151 (100%) | Continuous VEEG in first 72 h, daily for first 7 days + if neurological worsening, at discharge | |
| Portugal | Cohort | To investigate whether early EEG abnormalities are independent predictors of post-stroke epilepsy | 151 | 112 (74%) | 151 (100%) | Continuous VEEG in first 72 h, daily for first 7 days + if neurological worsening, at discharge | |
| Switzerland | Case control | To determine the incidence and risk factors of electrical seizures and other electrical epileptic activity using cEEG in patients with acute stroke | 100 | 58 (58%) | 91 (91%) | cEEG routinely on first full admission day | |
| Italy | Cohort | To evaluate the incidence of seizures and relationship between the various types of seizures and lesion location | 217 | 125 (58%) | 187 (86%) | Observation and description by either experienced departmental staff or by witness relatives of the patient | |
| Switzerland | Cohort | To analyse the influence of early and late epileptic seizures on the outcomes of patients with acute ischemic stroke treated with thrombolytic therapy | 805 | 438 (56%) | 805 (100%) | Symptom information from the patient, from a witness, or both | |
| South Korea | Cohort | To define clinical predictors of seizure recurrence after first post-stroke seizure in ischaemic stroke | 48 | 29 (60%) | 48 (100%) | Seizure diagnosed clinically. Standard EEG within 24–72 h of seizure onset. | |
| Poland | Cohort | To determine the prevalence and nature of changes in EEG recordings from the stroke hemisphere and contralateral hemisphere | 131 | 62 (47%) | 131 (100%) | Two EEGs in first 72 h and one before discharge | |
| Italy | Cohort | To analyse EEG patterns performed within 24 h of stroke onset | 232 | 107 (46%) | 177 (76%) | EEG within 24 h of admission | |
| Turkey | Cohort | To identify whether EEG findings could be a marker for post-stroke seizure development and survival in patients with acute ischemic or haemorrhagic stroke, who were followed up in a neurological intensive care unit | 50 | 23 (46%) | 37 (74%) | Continuous EEG in neurological intensive care unit | |
| Africa | Cohort | To assess the frequency and factors associated with post-stroke seizures by stroke types across 15 hospitals in Nigeria and Ghana | 3344 | 1870 (66%) | 2091 (62%) | Seizure diagnosed clinically. No EEG. | |
| Belgium | Cohort | To assess if epileptic activities were associated with neurological deterioration in acute ischaemic stroke | 81 | 46 (56%) | 81 (100%) | EEG | |
| Germany | Cohort | To analyse predictive factors for acute symptomatic seizures in a well-defined patient population who experienced an ischemic stroke due to large vessel occlusion and treated after mechanical recanalisation | 979 | 509 | 979(100%) | Clinically observed ictal stigmas. EEG only when indicated by medical staff. | |
| USA | Cohort | To determine whether early seizures that occur frequently after intracerebral haemorrhage led to increased brain oedema | 109 | 60 (55%) | 46 (42%) | EEG within 24 h of stroke onset and admission to intensive care | |
| USA | Cohort | To evaluate risk factors from examination, imaging, and cEEG for the development of seizures in critically ill patients with ICH | 57 | 26 (46%) | 0 (0%) | Continuous EEG at the order of the physician |
| First Author, Year | Country | Clinical Setting | Clinical Method to Identify Seizure | Duration of Method | Indications |
|---|---|---|---|---|---|
| USA | Acute ischaemic stroke | Standardised approach to recognition, assessment, and documentation of the seizure | Not reported | Monitor with EEG for change in mental status or depressed level of consciousness out of proportion to the stroke | |
| USA | Acute intracerebral haemorrhage | cEEG | At least 24 h | Depressed mental status out of proportion to the stroke | |
| USA | Inpatient | Continuous VEEG monitoring | Condition-specific | Continuous VEEG should be used to differentiate between epileptic and non-epileptic events |
- —National Institute of Health and Social Care Research Applied Research Collaboration North West Coast (NIHR ARC NWC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Intracerebral and Subarachnoid Hemorrhage Research · Epilepsy research and treatment
1. Introduction
Early post-stroke seizures (EPSSs), also termed provoked or acute symptomatic seizures, describe seizures provoked by acute brain injury due to stroke. These are different to post-stroke epilepsy that arises from long-term brain changes after stroke and seizures which are unprovoked by any other factor, such as metabolic, toxic etc. [1,2]. There is a lack of consensus in the literature on the definition and timing of what is classed as EPSS. The International League Against Epilepsy (ILAE) defines acute symptomatic seizures as occurring up to 7 days after acute stroke onset [3], whereas, in the literature, EPSS is defined as occurring between 48 h and 2 weeks after stroke [1,4].
Post-stroke seizures, occurring in the immediate aftermath of an acute stroke, can complicate diagnosis and management, and can even go unrecognised by clinicians and patients [5,6]. These seizures can present as new or unexplained reduced consciousness, persistent focal neurological deficits (e.g., due to postictal paresis), or exacerbation of existing deficits, potentially leading to inaccurate assessment of stroke severity or the attribution of symptoms to stroke recurrence. Timely recognition and treatment of seizures are essential to prevent further injury to already compromised brain tissue and to avoid the inappropriate use of stroke-specific therapies when symptoms are misattributed [7]. It is important to identify and diagnose EPSS as some studies have demonstrated associations with increased mortality, disability and recurrent hospital admissions [8,9]. Moreover, the risk of developing post-stroke epilepsy is significantly higher in patients who experience EPSS compared to those who do not [10]. Accurate detection of EPSS may also facilitate early discussions with patients regarding their long-term seizure risk.
EPSSs are more likely to occur after intracerebral haemorrhage (prevalence 10–16% across stroke populations) but are also common after ischaemic stroke (prevalence 3–15%) [1,11]. The risk of EPSS is increased in ischaemic stroke with haemorrhagic transformation, with cortical involvement and with increasing stroke severity [2,12]. Numerically, given the epidemiology of pathological stroke subtypes, early post-ischaemic stroke seizures will be more frequently encountered in the acute stroke context.
Electroencephalogram (EEG) is a helpful tool in detecting seizure activity, recognising non-convulsive status epilepticus and predicting seizure recurrence [13]. However, EEG is not 100% sensitive, nor used systematically for post-stroke seizure monitoring due to time and resource limitations, and it is usually instigated after seizures are suspected [14]. Typically, UK centres have access to up to 30 min video EEG recording, which can fail to capture seizures if they are not occurring during the recording, although a propensity towards seizure can sometimes be observed [13,15]. Therefore, interpretation of events, with or without EEG, is highly dependent upon clinical acumen and identification of clinical signs. With the lack of reference specifically on recognition and monitoring for EPSS in national guidance, this study aimed to map the breadth of evidence in relation to clinical methods used to support the identification and monitoring of EPSS. Our research question was, what is known from the existing literature about the clinical methods used for identifying and monitoring seizures in adults being treated for acute stroke?
2. Materials and Methods
The review was guided by Arksey and O’Malley’s framework, which includes the following stages: (i) identifying the research question; (ii) searching for relevant papers; (iii) selecting papers; (iv) charting the data; (v) collating, summarising, and reporting the results [16,17]. The review protocol has been registered with OSF and published online (OSF ID: bkejc) [18].
2.1. Identifying the Research Question and Eligibility Criteria
The research question was developed with input from subject experts comprising academics, clinicians, and patient advisors for the identification of relevant outcomes. We included literature published up to April 2023, encompassing all study types, including systematic reviews with meta-analysis and non-research literature such as clinical guidelines and consensus statements. We included literature on adults (≥18 years) with acute stroke (ischaemic or primary intracerebral haemorrhage) and seizures that occurred in hospital, within 2 weeks of stroke onset. We included seizures occurring at stroke onset and seizures occurring with an acute stroke intervention such as reperfusion therapies. We excluded literature reporting on seizure as a stroke mimic, patients with known epilepsy or seizures before their stroke, and patients with diagnoses of subdural and subarachnoid haemorrhages or cerebral ischaemia without arterial circulation obstruction, such as vasospasm or secondary to trauma. We excluded papers published in languages other than English. See Table 1 for the PICo criteria [19] for the review question.
2.2. Searching for Relevant Papers
MEDLINE (Ovid), CINAHL (EBSCOhost), EMBASE (Ovid), and the Cochrane Library (all databases via Wiley) were originally searched in 2021 and updated on 21 April 2023. To ensure that all relevant information was captured, we also searched a variety of grey literature sources (searched January 2023)—Grey Literature Report, OpenGrey, and Web of Science Conference Proceedings—to identify studies, case reports, and conference abstracts of relevance to this review. We also conducted a targeted search, using Google, of the grey literature, and we specifically searched national and international organisations’ websites with an interest in stroke and/or seizures, such as the Stroke Association, the Epilepsy Society, the ILAE, the British and Irish Association of Stroke Physicians, the European Stroke Organisation, and the American Stroke Association. A hand search was conducted using the reference lists of included papers to identify additional relevant papers. The search strategy was developed and piloted by an information specialist (CH) with input from the project team. The search strategies are provided in the Supplementary Materials (Supplementary Material 1) and are published online [18].
2.3. Selection of Sources of Evidence and Charting the Data
Following the searches, duplicate records were removed in EndNote before results were uploaded into Rayyan© online collaborative systematic review software [20] for record management and title and abstract screening. A two-part screening process against the inclusion criteria was used: (a) a title and abstract review, and (b) a full text review.
Title and abstract screening were conducted mainly by one reviewer, with 1000 citations independently screened by two reviewers (C.G. & J.W.) with 91.5% agreement between reviewers. Full text papers were assessed against the inclusion criteria; reasons for exclusion were recorded and are reported in the results by one reviewer. Any disagreements that arose were resolved through discussion with the wider project team. The results of the search selection are reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (flow diagram in Figure 1) [21]. The completed PRISMA-ScR checklist is available in the Supplementary Material (Table S1).
2.4. Data Charting Process
We developed and piloted our data charting form with evidence synthesis experts (J.H. & A.C.) based on scoping review methodology [16]. The piloting process included data charting of three papers independently, with comparison of accuracy and comprehension after completion. The charting of the data was divided between the three reviewers (C.G., J.W., C.E.D.). Where results of the same study were reported in more than one publication, we collated the results and used the publication with the most data relevant to our research question as the primary reference. Data charted included type of paper (e.g., primary research, conference proceedings, clinical guideline), study aims, methods, clinical assessment method, participants, study location, study setting, type of stroke, type of seizure, and key results relevant to our research question (e.g., sensitivity and specificity of tool). Due to inconsistencies in EEG terminology across studies, we systematically charted the terminology used by authors, along with reported technical parameters and recording durations. Where there was no reference to video data in the methods or results, we assumed video was not incorporated. Finally, a scoping review does not typically involve a quality assessment and therefore we did not appraise the quality of evidence [17].
3. Results
3.1. Selection of Sources of Evidence
We included 30 papers, 26 from database searches and four retrieved from alternative sources and citation searching. The selection process is outlined in the PRISMA diagram (Figure 1). Dates of publication ranged from 1996 to 2023. The definition of EPSS ranged from 24 h to 1 month after stroke onset. Papers originated from 13 different countries, 18 (60%) from Europe (Belgium (2), France (1), Germany (1), Italy (4), Poland (1), Portugal (2), Sweden (2), Switzerland (2), Turkey (3)), nine (30%) from the United States of America (USA), two (7%) from Asia (China (1), South Korea (1)) and one (3%) from Africa. A summary of the key characteristics are in Table 2.
For reporting the results, we tabulated the papers according to the traditional hierarchy of evidence [22] (see Table 3, Table 4 and Table 5). Table 3 summarises the characteristics of 10 included papers consisting of expert opinions and case reports that are considered low-quality evidence in the hierarchy of evidence [22]. Apart from Green et al.’s clinical guidelines [23] (Table 5), these 10 papers provided the most detail on the nursing contribution to seizure observation and supporting bedside EEG monitoring in critical care settings.
Seventeen primary research papers were identified (Table 4). All were observational design and eight used retrospective data collection [31,33,34,35,36,37,38,39]. Most patients were recruited from centres providing stroke specialist services. Three studies recruited patients from intensive care [31,39,40]. Two studies did not describe the type of specialist stroke service provision [36,41]. Sample sizes ranged from 48 to 3344. Eleven papers (64.7%) had <500 participants, four papers (23.5%) had 500–1000 participants, and two papers (11.8%) had >1000 participants (Table 2). Ethnicity was not consistently reported. Of the participants recruited, 83.7% (n = 8111) had a diagnosis of ischaemic stroke and 54.7% (n = 5302) were male.
Three clinical guidelines were identified (Table 5). Two papers were American Heart Association scientific statements [23,40]. Green et al. [23] provided guidance on observation for seizures within their nursing care scientific statement. Both Green et al. [23] and Hemphill et al. [40] outlined indications for EEG monitoring in acute stroke. A third guideline, jointly published by the International League Against Epilepsy and the International Federation of Clinical Neurophysiology, provided guidance on inpatient long-term VEEG monitoring for differentiation between epileptic and non-epileptic events. It did not provide any guidance specifically for stroke [50].
3.2. Clinical Methods for the Identification and Observation of Seizures
Our aim for this review was to map the available literature on methods used in the identification and observation of EPSS in inpatient settings. We identified one research paper evaluating the usefulness of EEG monitoring on a stroke unit [43]. No papers were identified that evaluated the accuracy of different clinical methods for identifying EPSS. Five types of clinical methods used in the identification and observation of EPSS were reported in the literature: (i) cEEG, (ii) periodic EEG, (iii) VEEG, (iv) clinical observation, and (v) family witness. There were inconsistencies in the terminology and definitions for EEG type and therefore we have used the same terminology used by the authors. cEEG (reported with or without concurrent video recording) received the most attention in the literature, including eight research studies evaluating EEG changes in EPSS [13,37,40,43,44,45,48] (Table 6). Indications for performing EEG also varied and are summarised in Table 7. Routine EEG at prescribed timepoints was mostly implemented in research papers. Case studies, expert opinion, and clinical guidance literature relied on clinical changes in neurological status to justify EEG investigation (Table 7). Only two papers reported using methods of seizure activation such as hyperventilation [44,46].
Table 5 provides a summary of the key information for each clinical method.
(i)cEEG. Seventeen papers, including eight research studies, referred to cEEG for EPSS detection and monitoring. Technical parameters for EEG were reported in nine papers with varying detail and no standardisation. cEEG was typically initiated at the earliest opportunity after suspected seizure or stroke onset. Duration of monitoring ranged from >6 h to 7 days; one intensive care study monitored for up to 38 days. Three papers described bedside cEEG visible to nursing staff [25,31,45], and two highlighted the need for nursing and physician competency in recognising electrographic seizure patterns [25,31]. Bautista [25] specified essential bedside EEG interpretation skills, including waveform frequency, amplitude, morphology, and symmetry. Two papers reported retrospective cEEG review by either trained physicians or electroencephalographers [31,45]. Several papers highlighted the utility of cEEG in detecting non-convulsive seizures and periodic discharges (associated with increased seizure risk) [2,28,31,32].(ii)Periodic EEG. Eleven papers referred to periodic EEG, reported as 20 to 30 min in duration (Table 6). One paper [28] initiated an emergency EEG performed soon after stroke presentation due to fluctuant confusion, followed by cEEG. Two research papers used periodic EEG systematically on all acute stroke patients [46,47]. They were also the only papers reporting on technical parameters, both using the International 10–20 system with 14 [47] or 21 [46] electrodes. In one study, serial EEGs over several days were indicated if the first EEG showed abnormal epileptiform activity [47].(iii)VEEG. Concurrent video recording with EEG is considered best practice, supplementing clinical assessments and linking electrographic seizures with clinical changes [2]. Tatum et al. [50] recommend a single camera setup and provide guidance on EEG and video synchronisation and digital memory requirements. Video use was reported in one out 11 papers using periodic EEG and in 10 out of 19 cEEG papers (Table 6). Mader’s case report [30] described a 28 s clonic seizure observed on video but obscured on EEG due to movement artefact. This case drew attention to the narrow time window for observing seizures if relying on human observation as well as the value of concurrent video recording with EEG.(iv)Clinician observation. Nine papers, six research papers, addressed clinical observation in EPSS. In five papers, seizures were diagnosed clinically without details on observation procedures or staff training [34,35,38,41,42]. Among papers reporting criteria, seizure definitions and thresholds were varied [24,35,36]. The International League Against Epilepsy definitions were used in three papers [36,38,41]. Green et al. [23] recommended a standardised nursing observation approach for post-stroke complications, including seizures, but did not specify a method. Bautista [50] recommended a systematic assessment covering onset and duration, level of consciousness, eye deviation, gaze, pupil size, urinary incontinence, body movements, and motor function, with periodic assessments until baseline recovery [50].(v)Family witness. Four research papers [34,35,41,42] and case report [30] referred to a family witness description contributing to the diagnosis of seizure at stroke onset or on hospitalisation. No papers referred to supplemental video information recorded on smart phones provided as part of the witness account.
4. Discussion
This scoping review has identified clinical and electrophysiological methods used in the identification and monitoring of EPSS. While we found no studies evaluating the effectiveness of these methods, we included papers that described seizure identification and monitoring methods within their research designs or practice recommendations. Many studies on seizure prevalence and characteristics in acute stroke were excluded because they lacked detail on how seizures were identified. Our review highlights a notable gap in the literature, particularly in nursing research, regarding the most effective and accurate methods for seizure monitoring in acute stroke patients.
This scoping review was undertaken to highlight knowledge gaps and areas requiring further research in relation to diagnostic approaches, in light of the lack of consensus on key definitions of EPSS in the literature. We aimed to include a wide range of literature, using a systematic search process in extensive databases and within grey literature, but it is possible that we have missed some relevant literature. We did not undertake a formal quality assessment, but we did chart data on methodological information that informed our interpretation of the evidence. We did exclude papers that had mixed early- and late-seizure onset participants or where onset of seizure after stroke was not clear.
We found significant heterogeneity in seizure identification and monitoring practices across research, clinical settings, and guidelines. Although consensus classifications such as the ILAE exist, they are not fully utilised in acute stroke care. This leads to variability in how clinical signs are interpreted and managed. We found EEG monitoring also lacked standardisation—indications for its use, technical parameters, duration and interpretation varied widely. This inconsistency hampers accurate estimation of EPSS prevalence and affects diagnostic accuracy, and, ultimately, patient outcomes.
A further layer of complexity is distinguishing seizure activity from the acute stroke itself, especially in the first hours post-stroke when seizure signs may be misattributed to stroke progression [39]. Several studies assumed that post-stroke seizures are readily recognised by clinicians, triggering EEG investigation. However, other papers challenge this assumption as short-duration focal seizures are more likely to go unnoticed by staff. Systematic EEG monitoring can reveal electrographic seizures with no clinical manifestations, non-convulsive status epilepticus, and specific patterns indicating heightened seizure risk [39,43,46,47]. This review identified justification for EEG in acute stroke, and further prospective research is needed into patient selection, type, and duration of EEG monitoring and its impact on treatment.
5. Conclusions
Research on the prevalence, diagnosis, and management of EPSS relies on effective recognition and observation of post-stroke patients for seizures. This scoping review highlights a significant gap in the literature on validated methods for identification and observation of seizures in acute stroke care. The absent of consistent methods may contribute to the underestimation of its prevalence, delayed diagnosis and treatment, and, ultimately, poorer outcomes. Greater attention to EPSS in both research and clinical practice is warranted. Our findings highlight a need for further clinical research to determine which methods, or combination of methods, can improve recognition rates of suspected seizure activity and ultimately improve diagnostic accuracy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Holtkamp M. Beghi E. Benninger F. Kälviäinen R. Rocamora R. Christensen H. European Stroke Organisation guidelines for the management of post-stroke seizures and epilepsy Eur. Stroke J.2017210311510.1177/239698731770553631008306 PMC 6453212 · doi ↗ · pubmed ↗
- 2Zelano J. Holtkamp M. Agarwal N. Lattanzi S. Trinka E. Brigo F. How to diagnose and treat post-stroke seizures and epilepsy Epileptic Disord.20202225226310.1684/epd.2020.115932597766 · doi ↗ · pubmed ↗
- 3Fisher R.S. Cross J.H. French J.A. Higurashi N. Hirsch E. Jansen F.E. Lagae L. MoshéS.L. Peltola J. Roulet Perez E. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology Epilepsia 20175852253010.1111/epi.1367028276060 · doi ↗ · pubmed ↗
- 4Beghi E. Carpio A. Forsgren L. Hesdorffer D. Malmgren K. Sander J. Tomson T. Hauser A.W. Recommendation for a definition of acute symptomatic seizure Epilepsia 20105167167510.1111/j.1528-1167.2009.02285.x 19732133 · doi ↗ · pubmed ↗
- 5Chung J.M. Seizures in the acute stroke setting Neurol. Res.20143640340610.1179/1743132814 Y.000000035224641717 · doi ↗ · pubmed ↗
- 6Blum D.E. Eskola J. Bortz J.J. Fisher R.S. Patient awareness of seizures Neurology 19964726026410.1212/WNL.47.1.2608710091 · doi ↗ · pubmed ↗
- 7Brigo F. Lattanzi S. Poststroke seizures as stroke mimics: Clinical assessment and management Epilepsy Behav.202010410629710.1016/j.yebeh.2019.04.05031303444 · doi ↗ · pubmed ↗
- 8Stefanidou M. Das R.R. Beiser A.S. Sundar B. Kelly-Hayes M. Kase C.S. Devinsky O. Seshadri S. Friedman D. Incidence of seizures following initial ischemic stroke in a community-based cohort: The Framingham Heart Study Seizure 20174710511010.1016/j.seizure.2017.03.00928364691 · doi ↗ · pubmed ↗