Digital Health Intervention Combined with Personalized Healthy Breakfast Guidance Improves Breakfast Behavior Among Chinese Young Adults: A Randomized Controlled Trial
Xinru Wei, Li Huang, Zequn Fu, Qianfeng Liu, Xinyue Yu, Xinrui Zhao, Rong Luo, Feijie Wang, Jiaxin Xiao, Jiayan Xue, Fuzhi Wang, Xingzhao Tian, Shiji Qiu, Meilin Zhang, Huan Liu

TL;DR
A digital health intervention combined with personalized breakfast guidance significantly improved breakfast habits among young adults in China, with self-efficacy playing a key role.
Contribution
The study demonstrates that combining digital health tools with personalized guidance is more effective than either alone for improving breakfast behavior.
Findings
The DHI + PHBG group showed the highest adherence to healthy breakfast guidelines at 80%.
Self-efficacy and self-monitoring were key mediators of the intervention's effectiveness.
Waist-to-hip ratios decreased slightly in all intervention groups, but other body composition changes were not significant.
Abstract
Objectives: To evaluate the effects of digital health intervention (DHI) or/and personalized healthy breakfast guidance (PHBG) on the breakfast behavior and body composition of young adults in Tianjin, and to explore the underlying behavioral mechanisms using the Health Action Process Approach (HAPA) framework. Methods: In this single-blind, stratified RCT, 160 participants (n = 40/group) were randomly assigned to a control group, DHI group, PHBG group, or DHI + PHBG group. Breakfast behavior (primary outcome), HAPA constructs, and body composition were assessed at baseline and after 1 month. Group differences were analyzed using the Kruskal–Wallis test, chi-square test, and linear mixed-effects models. Mediation analysis assessed indirect effects via HAPA variables. Results: After a 1-month intervention, adherence to healthy breakfast guidelines was highest in the DHI + PHBG group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
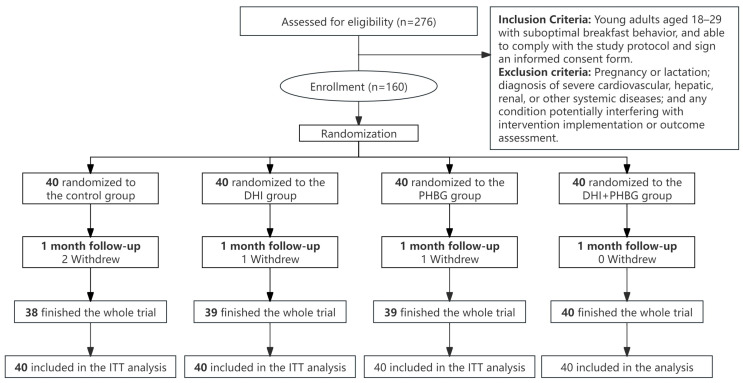 Figure 1
Figure 1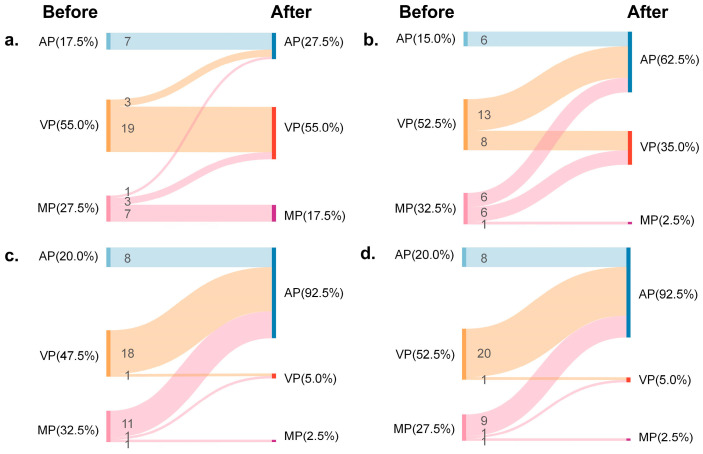 Figure 2
Figure 2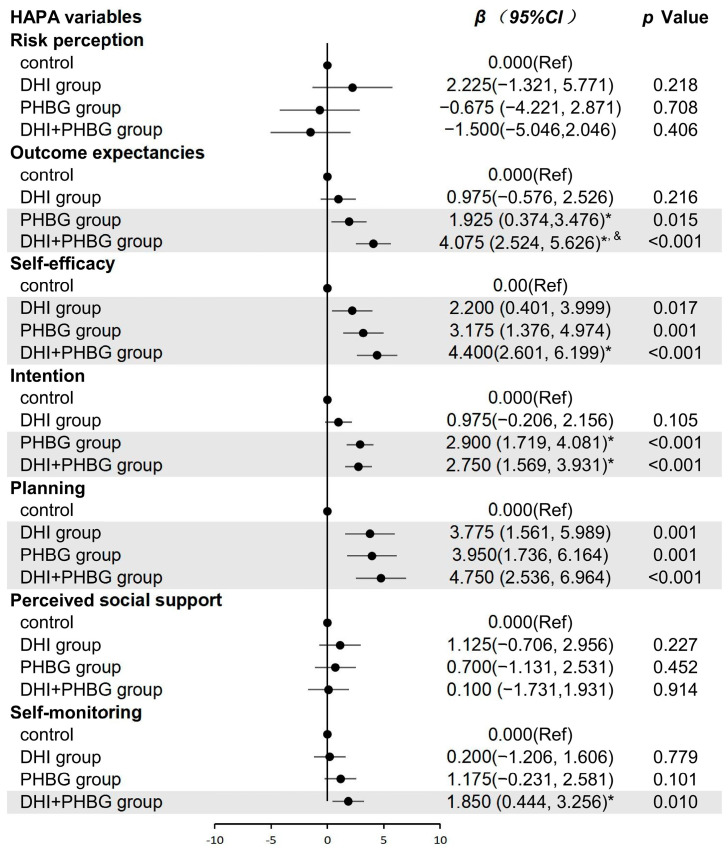 Figure 3
Figure 3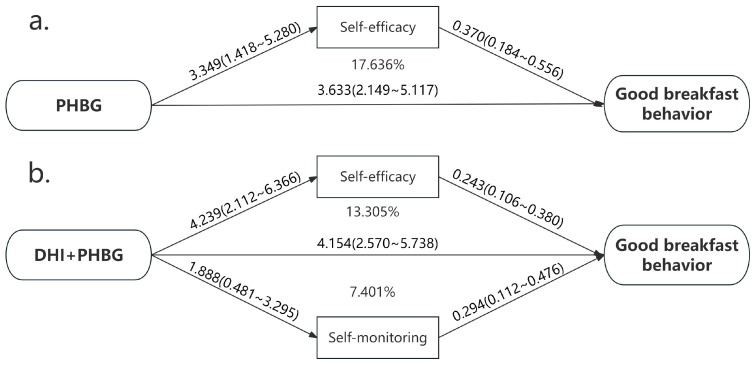 Figure 4
Figure 4- —Chinese Nutrition Society-Healthy Diet Special Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMobile Health and mHealth Applications · Dietary Effects on Health · Nutritional Studies and Diet
1. Introduction
Breakfast is a critical meal for nutrient intake and health outcomes [1]. According to the Chinese Dietary Guidelines (2022), a high-quality breakfast should include at least three of four food groups—cereals/tubers, vegetables/fruits, meat/eggs, and dairy/legumes/nuts. Increased breakfast frequency and quality are linked to improved cognitive performance [2,3,4,5], lower risks of diabetes [6] and cardiovascular disease [7], reduced abdominal obesity [8,9], and better muscle mass maintenance [10]. Despite these benefits, national surveys reveal that most Chinese adults, particularly those aged 18–29, consume unbalanced breakfasts, primarily consisting of cereals and tubers, with over half (55%) eating fewer than three food categories. As young adulthood is a crucial period for establishing long-term dietary habits, effective strategies to improve breakfast quality in this population are urgently needed.
Conventional dietary interventions, such as health education programs, balanced dietary pattern intervention [11], and personalized nutritional guidance [12,13], are increasingly complemented by digital health interventions (DHIs), which leverage digital technologies to improve accessibility, cost-effectiveness, and user engagement [14,15]. Given the widespread smartphone and social media use among young adults, DHIs represent a feasible approach for promoting breakfast improvements [16,17,18,19,20]. Meanwhile, precision nutrition and personalized healthy diet guidance have shown effectiveness in chronic disease management and dietary improvement among middle-aged and elderly populations [21,22,23,24], yet their role in shaping breakfast habits of young Chinese adults remains unclear. No study has examined the separate or combined effects of DHI and personalized healthy breakfast guidance (PHBG) in this population.
Identifying the mechanisms of behavior change is critical for ensuring that newly adopted healthy behaviors are sustained [25,26]. The health action process approach (HAPA), which combines stage and continuity theory [27], provides a framework for understanding the processes of generating and maintaining behavior; specifically, the transition from intention to action. Simultaneously, this model serves as an assessment tool capable of evaluating whether interventions enhance self-efficacy for healthy behaviors, thereby predicting their long-term maintenance. HAPA has been successfully applied to physical activity [28,29], internet use [30], oral health [31], and fruit and vegetable intake [32], making it a valuable tool for elucidating the underlying mechanisms of breakfast behavior change and predicting the long-term effects of behavior intervention approaches in young adults.
Therefore, this study aimed to evaluate the effects of DHI or/and PHBG on breakfast behavior and body composition in young adults aged 18–29 years in Tianjin. Using the HAPA framework, we further sought to identify the mechanisms underlying behavioral change and provide evidence for tailored intervention models to improve breakfast quality and health outcomes in this population.
2. Methods
2.1. Study Design
The study was a single-blind, stratified, randomized controlled trial conducted for 1 month among young adults from Tianjin in China. Participants were randomly assigned to one of four groups: the digital health intervention (DHI) group, the personalized healthy breakfast guidance (PHBG) group, the combined intervention (DHI + PHBG) group, or the control group. This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the ethics committee. The trial was registered at the Chinese Clinical Trial Registry (ChiCTR2400084398) on 15 May 2024.
2.2. Sample Size and Participants
According to the sample size calculation formula for randomized controlled trial measures, based on reported evidence [33], the anticipated increases in good breakfast behavior after DHI (p1 = 0.35) and in the control group (p2 = 0.1), and accounting for a 10% dropout rate, 40 participants were required per group. Prior to enrollment, all participants provided informed consent.
The participants were recruited from May to June in 2024. Initially, 276 individuals were screened for eligibility. Using 1:1 propensity score matching (PSM) based on sex, age (±1 year), education level, and baseline breakfast frequency, 160 participants were selected and included in the trial. These participants, stratified by their baseline HAPA phases, were randomly allocated into four groups: including a control group, a DHI group, a PHBG group, and a DHI + PHBG group (40 participants/group). An independent researcher assigned subjects to groups using randomization codes. The study subjects were not aware of the grouping throughout the process. Personnel responsible for intervention delivery and outcome data collection were unblinded due to the nature of the intervention (i.e., researchers needed to provide guidance). However, outcome assessors responsible for evaluating primary outcomes (such as body composition measurements) were blinded to minimize measurement bias.
According to the Chinese Dietary Guidelines (2022), good breakfast behavior is defined as consuming a nutritious breakfast which contains 4 food categories (cereals/root and tuber crops, meat/eggs, vegetables/fruits, and milk/beans) and the regular consumption of breakfast (≥3 times a week).
The inclusion criteria were young adults (i) aged 18–29 years, (ii) able to comply with the study protocol and sign an informed consent form, (iii) with suboptimal breakfast behavior. Participants meeting all three criteria were included in this study.
The exclusion criteria were (i) pregnancy or lactation, (ii) diagnosis of severe cardiovascular, hepatic, renal, or other systemic diseases, and (iii) any condition potentially interfering with intervention implementation or outcome assessment.
Eligible participants were stratified by baseline HAPA stage and then randomly allocated to one of the four groups by an independent researcher using computer-generated randomization codes. During the one-month intervention, 4 participants dropped out: 2 (5%) from the control group, 1 (2.5%) each from the DHI and PHBG groups, and none from the combined DHI + PHBG group. All participants were included in the intention-to-treat (ITT) analysis. Multiple imputations were performed for missing data after the intervention. The flow diagram of enrollment, randomization, and follow-up is shown in Figure 1.
2.3. Intervention
The intervention lasted for one month. Breakfast energy intake was targeted to account for 25–30% of total daily energy intake. For adults aged 18–29, the recommended breakfast energy range was 425–900 kcal for males and 430–740 kcal for females. Participants were also instructed to maintain their usual dietary structure and energy intake for lunch and dinner. All participants attended weekly “Healthy Breakfast” educational lectures to reinforce awareness of good breakfast practices.
Participants in the control group were asked to keep breakfast records (with photographs) via WeChat but received no personalized guidance or feedback.
Digital Health Intervention (DHI) Group: Participants used the Xiao’an Nutritionist WeChat mini program to record their daily breakfast intake. The WeChat mini program provided automated feedback, including a breakfast quality score and detailed nutrient analysis, based on its built-in dietary tracking and assessment algorithms.
Personalized Healthy Breakfast Guidance (PHBG) Group: This group received customized breakfast plans tailored to their dietary preferences, while adhering to the nutritional principles of the Chinese Dietary Guidelines (2022). These plans emphasized four essential breakfast components (grains, meat/eggs, vegetables/fruits, and milk/beans) and met the breakfast energy needs of healthy adults aged 18–29 years. Participants submitted daily breakfast records (including photographs) via WeChat and received researcher feedback comprising: (i) quality assessments, (ii) food combination suggestions, and (iii) encouragement for maintaining good breakfast habits.
DHI + PHBG Group: Participants received both interventions described above, namely using the Xiao’an Nutritionist WeChat mini program and receiving personalized weekly guidance and feedback from researchers.
Data Collection: At baseline (T0), data were collected on sociodemographic variables, anthropometry, body composition, breakfast behavior assessment, stages, and the social-cognitive variables outlined in the HAPA model. All assessments (except sociodemographic variables) were repeated at the end of the 1-month intervention (T1).
2.4. Study Variables
Primary (breakfast behavior) and secondary outcomes (HAPA constructs, anthropometric indices, and body composition) were evaluated at baseline (T0) and post intervention (T1). Sociodemographic data were obtained through interviews using a form developed by the researchers. The questions covered age, sex, education level, and living expenses.
2.4.1. Breakfast Behavior Assessment
The primary outcome was the proportion of participants with good breakfast behavior. Breakfast behavior was assessed using a structured questionnaire. Participants reported the types of foods usually consumed at breakfast, categorized as: (1) cereals/potatoes, (2) vegetables/fruits, (3) meat/eggs, and (4) milk/beans/nuts. They also reported breakfast frequency by answering, “How many times do you have breakfast per week?” These data were used to determine the number of food categories consumed per day and to evaluate overall breakfast behavior. The 24 h dietary recall was used to control the average daily energy intake of the participants at lunch and dinner to remain unchanged from that before the intervention.
2.4.2. Anthropometric and Body Composition Assessment
The participants underwent the following anthropometric measurements: weight and height. Weight was measured using a portable electronic scale with a capacity of up to 150 kg and an accuracy of 100 g, with participants wearing light clothing and no shoes. Height was measured in a standing position using a portable stadiometer, with a range of 200 cm and a variation of 0.1 cm. These values were used to calculate BMI.
For body composition analysis, participants underwent bioelectrical impedance analysis using a tetrapolar device. The following conditions were included in the testing protocol: no pacemaker, water and food fasting (8–12 h), no smoking for at least two hours prior to testing, empty bladder, and no exercise for at least 12 h prior to testing.
2.4.3. HAPA Assessment
Social-cognitive constructs from the HAPA model—including risk perception, outcome expectancies, self-efficacy, intention, planning, perceived social support, and self-monitoring—were evaluated using a validated structured questionnaire. Each construct was measured using multiple items rated on Likert-type scales, with higher scores indicating stronger levels of each psychological factor.
2.5. Statistical Analysis
Baseline participant characteristics were described using medians with interquartile ranges (25–75%) for skewed continuous variables and numbers with percentages (%) for categorical variables. The Kruskal–Wallis test and chi-square test were used to compare continuous and categorical variables, respectively. Linear mixed models with repeated measures were used to assess the effects of different intervention patterns, with β coefficients and 95% confidence intervals (95% CIs) calculated after adjusting for age, sex, education level, and living expenses. Spearman’s rank correlation and conditional logistic regression, adjusted for the same covariates, analyzed associations between HAPA constructs and breakfast quality. Mediation effects of HAPA constructs on breakfast quality were evaluated using SPSS 24.0.
The variables were subjected to the intent-to-treat method, where missing data were imputed using the complete database to obtain postintervention (T1) values from the baseline values of the participants.
All analyses were conducted in SPSS 24.0 with a p-value < 0.05 was considered statistically significant.
3. Results
3.1. Demographics Characteristics of Participants
The baseline demographic and clinical characteristics of participants are summarized in Table 1. No statistically significant differences were observed among the four groups in any baseline variables (all p values > 0.05), indicating that the groups were homogeneous and comparable.
3.2. Effect of the DHI or/and PHBG on Breakfast Behavior
More than 92% of the participants in both the DHI and DHI + PHBG groups used the Xiao’an Nutritionist WeChat mini program daily. Following the 1-month intervention, all intervention groups demonstrated significant improvements in breakfast behavior. The proportion of participants adhering to good breakfast behavior increased significantly in the DHI (50.0%, p < 0.001), PHBG (72.5%, p < 0.001), and DHI + PHBG (80.0%, p < 0.001) groups compared to baseline. All intervention groups showed significantly higher adherence rates than the control group (χ^2^ = 51.127, p < 0.001). The number of daily breakfast food categories also increased significantly in all intervention groups (p < 0.001). Furthermore, the combined DHI + PHBG intervention led to a significantly greater improvement in good breakfast behavior than the DHI alone group (χ^2^ = 7.912, p < 0.05). Detailed results are presented in Table 2.
After 1 month, no significant phase shifts were observed in the control group (p > 0.05). In the DHI group, participants in the action phase increased (from 15.0% to 62.5%, p < 0.001), while participants in the motivation phase significantly decreased (from 32.5% to 2.5%, p < 0.001). No significant change occurred in the volition phase (p > 0.05). In the PHBG group, participants in both the motivation (from 32.5% to 2.5%, p < 0.001) and volition phases (from 47.5% to 5.0%, p < 0.001) decreased, accompanied by a marked increase in the action phase (from 20.0% to 92.5%, p < 0.001). Similarly, in the DHI + PHBG group, the motivation (from 27.5% to 2.5%, p < 0.05) and volition phases (from 52.5% to 5.0%, p < 0.001) declined, while the action phase rose sharply (from 20.0% to 92.5%, p < 0.001). Detailed results are shown in Figure 2.
The Kruskal–Wallis test confirmed that the interventions significantly promoted progression across the HAPA stages (H = 34.678, p < 0.001).
3.3. Effect of DHI or/and PHBG on HAPA Constructs
Following the 1-month intervention, significant between-group differences were observed in several HAPA constructs. Compared with the control group, the DHI group showed significant improvements in self-efficacy (β = 2.200, 95% CI: 0.401, 3.999) and planning (β = 3.775, 95% CI: 1.561, 5.989). The PHBG group demonstrated significant increases in outcome expectancies (β = 1.925, 95% CI: 0.374, 3.476), self-efficacy (β = 3.175, 95% CI: 1.376, 4.974), intention (β = 2.900, 95% CI: 1.719, 4.081), and planning (β = 3.950, 95% CI: 1.736, 6.164). The combined DHI + PHBG intervention resulted in significant improvements in outcome expectancies (β = 4.075, 95% CI: 2.524, 5.626), self-efficacy (β = 4.400, 95% CI: 2.601, 6.199), intention (β = 2.750, 95% CI: 1.569, 3.931), planning (β = 4.750, 95% CI: 2.536, 6.964), and self-monitoring (β = 1.850, 95% CI: 0.444, 3.256). Detailed results are presented in Figure 3.
3.4. Association of the HAPA Constructs and Good Breakfast Behavior
As shown in Table 3, after adjusting covariates, higher self-efficacy (OR:1.443, 95% CI: 1.230, 1.692) and higher self-monitoring (OR:1.225, 95% CI: 1.051, 1.427) were associated with improved breakfast behavior (p < 0.05). Furthermore, Spearman’s rank correlation analyses indicated that outcome expectancies, self-efficacy, intention, planning, perceived social support, and self-monitoring were positively related with good breakfast behavior (p < 0.05).
3.5. Mediation Analysis of HAPA Constructs on the Intervention–Behavior Association
Mediation analysis was performed to examine the potential mediating effects of HAPA constructs on the relationship between the interventions and good breakfast behavior. As illustrated in Figure 4, self-efficacy significantly mediated the effect of the PHBG intervention on breakfast behavior, accounting for 17.636% of the total effect. For the combined DHI + PHBG intervention, both self-efficacy and self-monitoring served as significant mediators, with mediation proportions of 13.305% and 7.401%, respectively.
3.6. Effect of the DHI or/and PHBG on Body Composition
Body composition was analyzed under the intent-to-treat principles. A small but statistically significant reduction in waist-to-hip ratio (WHR) was observed in the DHI (β = −0.014, 95% CI: −0.020, −0.000), PHBG (β = −0.013, 95% CI: −0.023, −0.005), and DHI + PHBG groups (β = −0.015, 95% CI: −0.024, −0.005). No other body composition indicators showed significant changes in response to the interventions (BMI, PBF, BMR, SLM, FFM, and SMM, all p > 0.05), although all displayed a slight downward trend (Table 4).
4. Discussion
This study demonstrated that DHI or/and PHBG interventions improved breakfast behavior by increased adherence to recommended breakfast patterns and greater dietary variety. These interventions also led to notable improvements in key social-cognitive constructs outlined by the HAPA model, including outcome expectations, self-efficacy, intention, planning, and self-monitoring. These findings suggest that PHBG and DHI + PHBG improve breakfast behavior by facilitating transitions across HAPA phases. Furthermore, the DHI or/and PHBG interventions for breakfast reduced the waist-to-hip ratio in young adults.
Digital health tools are increasingly applied to monitor health status and support behavior change [34,35,36]. Mobile health interventions, particularly smartphone applications, provide convenient platforms for self-monitoring, dynamic data collection, and real-time feedback outside clinical settings [37,38]. In this study, the loss-to-follow-up rate in the DHI group was lower than in previous behavioral interventions [39,40], indicating strong acceptability and effectiveness of the breakfast-focused DHI strategy.
Personalized healthy breakfast guidance (PHBG) tailored dietary recommendations and remains resource-intensive yet effective. When combined with digital health intervention (DHI), the integrated approach achieved greater improvements in dietary variety and behavioral stage transitions than either modality alone. Notably, DHI + PHBG outperformed DHI, though no significant difference was observed compared with PHBG. Participants preferred practical, personalized plans tailored to energy needs and preferences, highlighting the irreplaceable role of nutrition professionals. While DHI supports decision-making by providing information and incentives [37], its limited effect may stem from reliance on general feedback without the individualized guidance offered by PHBG.
The HAPA model is widely applied to evaluate health behavior change in areas such as physical activity [32], oral hygiene [41], and diet [42]. Our findings further support its utility in explaining the effect of breakfast interventions. DHI or/and PHBG improved self-efficacy and planning, while PHBG and DHI + PHBG also improved outcome expectations and intentions. DHI + PHBG uniquely enhanced self-monitoring, suggesting stronger potential for long-term behavioral maintenance. Self-efficacy and self-monitoring were the key mediators. DHI + PHBG strengthened confidence and behavioral regulation strategies, helping participants overcome setbacks and sustain healthy habits. In contrast, PHBG primarily enhanced confidence and guided choices through personalized meal plans. Thus, PHBG and DHI + PHBG were effective across motivational and action stages, whereas DHI mainly supported short- and long-term planning but showed weaker sustainability. This limitation may reflect simplified program design and insufficient integration of health behavior theory in app development [43,44]. Future studies should improve engagement by incorporating dynamic updates, personalized reminders [37], and integrating wearable devices [39].
The DHI and/or PHBG interventions also reduced WHR, with trends toward lower BMI, BMR, SLM, and FFM. These findings are consistent with evidence linking high-fiber breakfast patterns, such as fruit, cereal, nuts, and yogurt, to reduced WHR and abdominal obesity [8,45,46,47,48,49]. While participants in the DHI, PHBG, and DHI + PHBG groups experienced a significant reduction in waist-to-hip ratio, the change was minimal (0.01), making it difficult to conclude that the intervention had a meaningful effect on body composition. Body composition is influenced by multiple factors, including diet, exercise, and genetics. Although breakfast behavior improved, changes in diet alone may not be sufficient to cause significant changes in other body composition indicators in the short term. The intervention period in this study was one month, which may be short to induce significant changes in more complex body composition metrics, such as body fat percentage and lean body mass. Future studies with longer intervention durations, potentially incorporating physical activity, are needed to assess the long-term impact of lifestyle interventions on health outcomes.
This study has several strengths. First, by integrating digital health interventions and personalized guidance, it compares the effects of single and combined interventions on dietary behavior, providing a novel, population-tailored nutrition intervention model and laying the foundation for exploring the effects of interventions targeting other meals (such as lunch, dinner, and snacks). This approach could be extended to other meals in future studies. Second, the use of the HAPA model to explain the intervention mechanisms and validate its mediating effects establishes a strong theoretical foundation for broader application of this model in future nutrition research. Third, this study is among the first to explore the impact of breakfast interventions on body composition, contributing to a deeper understanding of the health effects of breakfast behavior.
However, there are several limitations. First, the online recruitment method may lead to a relatively homogeneous sample. Second, supported by previous research, we employed a one-month intervention to assess the primary outcome (behavioral change), which limited the evaluation of the effect of intervention on secondary outcomes (body composition). Third, although total energy intake at lunch and dinner was controlled, the study did not examine the specific dietary patterns during these meals and their potential influence on breakfast behavior and body composition. Finally, given that the participants were young adults rather than a clinical population, although it may have limitations in precision compared to DEXA, the use of bioelectrical impedance analysis (BIA) could a be practical method to measure the body composition in a population study.
Future research should focus on more diverse and larger populations to assess the effectiveness of interventions across different age groups and health conditions. Additionally, this study provides a solid framework for subsequent investigations targeting other meals. Longer-term studies are also needed to evaluate the sustainability of these interventions. To improve control over confounding variables, future research should incorporate more comprehensive dietary monitoring to account for the impact of food or energy intake from other meals on breakfast behavior and body composition. Moreover, more precise methodologies are essential for accurately assessing the impact of interventions on health outcomes.
5. Conclusions
DHI or/and PHBG could effectively improve the breakfast behaviors among young people, with the combined intervention of DHI and PHBG superior to DHI alone. Self-efficacy is a key social cognitive factor influencing the behavioral changes in PHBG alone or in combination with digital health intervention. However, the effect of these interventions on body composition remains uncertain. These findings underscore the potential for integrating DHI and PHBG into public health nutrition policies to improve dietary behaviors at a population level. Public health programs should consider adopting multifaceted approaches that combine digital tools with personalized advice to promote sustained, healthy eating habits and improve overall health outcomes in young adults.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stratton M.T. Holden S.L. Davis R. Massengale A.T. The Impact of Breakfast Consumption or Omission on Exercise Performance and Adaptations: A Narrative Review Nutrients 20251730010.3390/nu 1702030039861430 PMC 11767684 · doi ↗ · pubmed ↗
- 2Sámano R. Hernández-Chávez C. Chico-Barba G. Córdova-Barrios A. Morales-del-Olmo M. Sordo-Figuero H. Hernández M. Merino-Palacios C. Cervantes-Zamora L. Martínez-Rojano H. Breakfast Nutritional Quality and Cognitive Interference in University Students from Mexico City Int. J. Environ. Res. Public Health 201916267110.3390/ijerph 1615267131357381 PMC 6695580 · doi ↗ · pubmed ↗
- 3Liu J. Wu L. Um P. Wang J. Kral T.V.E. Hanlon A. Shi Z. Breakfast Consumption Habits at Age 6 and Cognitive Ability at Age 12: A Longitudinal Cohort Study Nutrients 202113208010.3390/nu 1306208034204553 PMC 8234310 · doi ↗ · pubmed ↗
- 4Bell L. Dodd G.F. Jeavons M. Fisher D.R. Whyte A.R. Shukitt-Hale B. Williams C.M. The impact of a walnut-rich breakfast on cognitive performance and brain activity throughout the day in healthy young adults: A crossover intervention trial Food Funct.2025161696170710.1039/D 4FO 04832 F 39924976 · doi ↗ · pubmed ↗
- 5Kawabata M. Lee K. Choo H. Burns S.F. Breakfast and Exercise Improve Academic and Cognitive Performance in Adolescents Nutrients 202113127810.3390/nu 1304127833924598 PMC 8068805 · doi ↗ · pubmed ↗
- 6Xiao K. Furutani A. Sasaki H. Takahashi M. Shibata S. Effect of a High Protein Diet at Breakfast on Postprandial Glucose Level at Dinner Time in Healthy Adults Nutrients 2022158510.3390/nu 1501008536615743 PMC 9824806 · doi ↗ · pubmed ↗
- 7Santos H.O. Genario R. Macedo R.C.O. Pareek M. Tinsley G.M. Association of breakfast skipping with cardiovascular outcomes and cardiometabolic risk factors: An updated review of clinical evidence Crit. Rev. Food Sci. Nutr.20226246647410.1080/10408398.2020.181976832935557 · doi ↗ · pubmed ↗
- 8Gwin J.A. Leidy H.J. A Review of the Evidence Surrounding the Effects of Breakfast Consumption on Mechanisms of Weight Management Adv. Nutr.2018971772510.1093/advances/nmy 04730204837 PMC 6247188 · doi ↗ · pubmed ↗