Improving Good Practices for Patient Safety in an Emergency Department Based on Multidisciplinary Training Using Simulation Techniques
Francisco Javier Redondo Calvo, Victor Baladrón González, María Ángeles Tebar Betegón, Alejandro Martínez Arce, Gema Verdugo Moreno, Juan Fernando Padin, Laura Muñoz de Morales-Romero, Alberto Bermejo-Cantarero, Natalia Bejarano Ramírez

TL;DR
This paper describes how simulation-based training improved patient safety practices in an emergency department through multidisciplinary teamwork and resource management.
Contribution
The novel contribution is the implementation of simulation techniques and critical resource management training to identify and address patient safety issues in emergency departments.
Findings
Simulation workshops identified areas for improvement and led to the development of local protocols for patient safety.
Cognitive aids and visual tools were incorporated to standardize processes in crisis situations.
Debriefing with experienced instructors after simulation scenarios helped contextualize and analyze safety recommendations.
Abstract
Background: We present a multidisciplinary training experience based on simulation techniques and critical resource management implemented in the emergency department. Methods: Simulation courses/workshops were conducted with a multidisciplinary team from the Hospital Emergency Department. The timeline for their development includes a preliminary analysis of needs, objectives, and scenario design, development of the simulation course, and finally, areas of implementation. In this last phase, the teaching team prepares a document and/or report/summary of the activity in which, among other things, the aspects with the greatest capacity for improvement or the areas for implementation of safety measures are determined. A total of 112 healthcare professionals (doctors, nurses, and care assistants) participated in this training program. Its design consisted of the following stages: a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1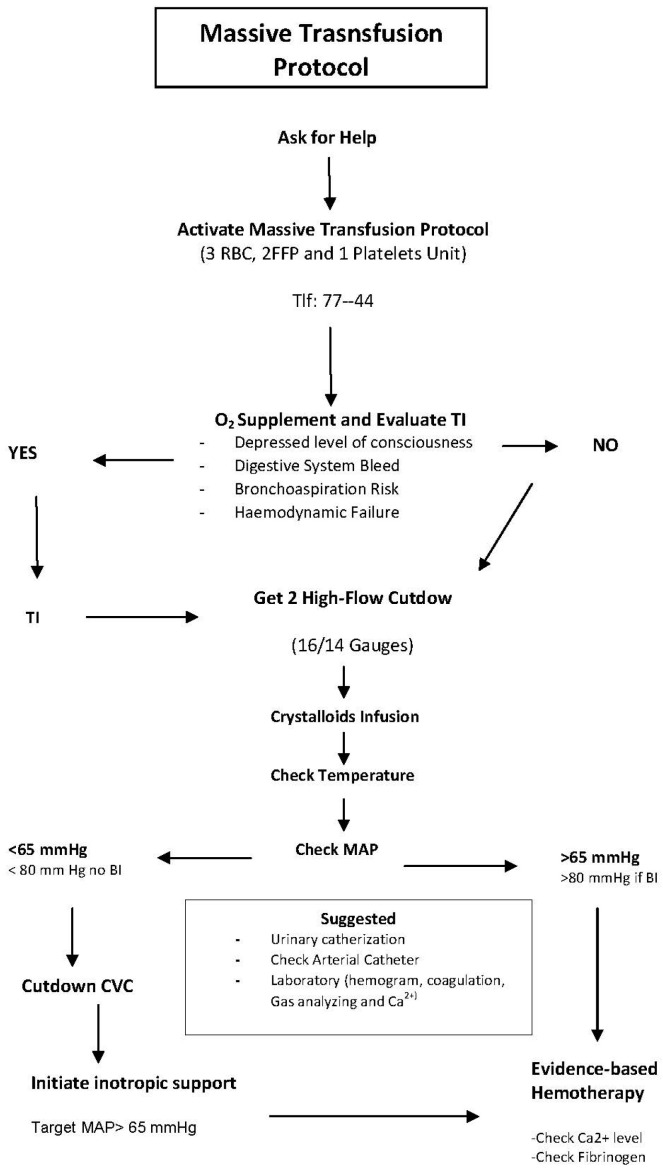 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSimulation-Based Education in Healthcare · Innovations in Medical Education · Patient Safety and Medication Errors
1. Introduction
In complex work environments such as emergency medicine, decisions are often made under conditions of uncertainty and time pressure. Studies have shown that up to 70% of errors in these settings can be attributed to human factors [1,2,3]. One effective strategy to mitigate such errors is the application of Crisis Resource Management (CRM) principles [4].
Originally developed in aviation, CRM has demonstrated its value across various disciplines. Gaba et al. adapted the concept to healthcare, specifically in anesthesiology, under the term Crisis Management Resources in Anaesthesia [5]. CRM focuses on the coordination, utilization, and optimization of all available resources to enhance patient safety. These resources include the healthcare team, their skills and attitudes, equipment, and environmental factors. CRM begins before a crisis occurs, emphasizing that standards designed to manage acute events are equally effective in preventing them. The approach aims to detect errors early and minimize their impact. Although initially developed for perioperative care, CRM principles are highly applicable to emergency medicine [6].
Emergency settings present unique challenges compared to other specialties, including the urgency of decision making for critically ill patients, diverse and sometimes hostile intervention contexts, and the need for coordination across multiple levels of care [7,8,9].
While CRM principles may appear intuitive (see Table 1), their effective application during crises is often difficult. Clinical simulation has emerged as a powerful tool to enhance CRM competencies, enabling healthcare professionals to reflect on and integrate these principles into daily practice. The SEMES Clinical Simulation Group (E-CRM) has been instrumental in adapting CRM methodologies to emergency care, developing tools to standardize workflows and improve patient safety [7,8,9].
Simulation-based training is increasingly integrated into the continuous education of healthcare professionals—including physicians, nurses, and care assistants—in response to the growing complexity of clinical care and the need for multidisciplinary collaboration [10,11]. This methodology provides a realistic and safe environment for acquiring both technical and non-technical skills, such as leadership, coordination, and communication. These competencies are developed during the experiential phase and reinforced through structured debriefing sessions [12,13].
In this context, we advocate for a robust simulation methodology capable of generating realistic clinical scenarios that evoke emotional engagement, facilitate learning, and serve as a foundation for expert-led analysis and discussion. We hypothesize that the implementation of high-fidelity simulation training based on CRM principles in emergency departments improves team coordination and contributes to the development of standardized clinical protocols, ultimately enhancing patient safety. This paper presents the experience of the Advanced Simulation Centre within the Integrated Healthcare Management of Ciudad Real (Healthcare Service of Castilla-La Mancha, Spain), focusing on its application in the hospital emergency department.
In recent years, the increasing complexity of emergency care and the growing awareness of patient safety have underscored the need for innovative educational approaches. Traditional training methods often fall short in preparing healthcare professionals for the dynamic and unpredictable nature of emergency scenarios. In this context, simulation-based education has emerged not only as a pedagogical tool but also as a strategic resource for fostering clinical excellence and resilience. By replicating high-risk situations in a controlled environment, simulation enables teams to develop critical thinking, reinforce collaborative behaviors, and identify latent safety threats before they manifest in real clinical settings.
Therefore, the objective of this study is to describe and analyze the implementation of a structured simulation-based training program in the emergency department of a tertiary hospital, aimed at enhancing CRM competencies among multidisciplinary healthcare teams. By evaluating the design, execution, and perceived impact of these workshops, we seek to contribute to the development of effective educational strategies that improve patient safety and team performance in high-pressure clinical environments
2. Materials and Methods
Over a four-year period, eight simulation-based workshops were conducted with a multidisciplinary team from the hospital’s emergency department. Two workshops were held each year, in February and November. A prospective cohort of 112 healthcare professionals voluntarily participated in this training program, which was developed at the Advanced Simulation Center of the General University Hospital of Ciudad Real. The cohort included 39 physicians, 51 nurses, and 22 nursing assistants. This represents approximately 60% of the total staff working in the emergency department. Each workshop was conducted with 14 professionals, which matches the maximum capacity of the Simulation Center (12–14 participants per session). Recruitment was voluntary among staff members currently working in the emergency department, and selection was based on the order of registration on the hospital’s training platform. Previous participants were excluded from subsequent workshops. Only healthcare professionals currently working in the emergency department were eligible for inclusion in the study; prior participation in any of the workshops was considered an exclusion criterion.
The workshops were conducted in a simulation-based training environment, involving healthcare professionals and following the same work schedule in all sessions (see Appendix C). No biomedical interventions were performed, and no sensitive personal data were collected. The only evaluation conducted was a satisfaction survey completed by the participants. All individuals provided informed consent and signed confidentiality and image release agreements prior to participation. The teaching team consisted of two simulation instructors, one assistant/confederate, and one emergency department professional.
The development of these workshops followed a structured four-phase process, outlined chronologically below:
Phase 1: Preliminary Needs Analysis
A teaching team was assembled, consisting of two simulation instructors, one assistant/confederate, and two emergency department professionals. This team conducted a comprehensive analysis of training needs, considering both individual clinical expectations and team-wide requirements. Key patient safety aspects were also identified for inclusion in the training.
Phase 2: Definition of Objectives and Scenario Design
Each workshop included three high-fidelity simulation scenarios (see Table 2), with each scenario targeting two clinical skill objectives and two behavioral or CRM (Crisis Resource Management) objectives. The simulations were conducted in a fully equipped simulation suite, including a realistic clinical environment, a control room, and a debriefing room (Figure 1). A robust audiovisual system enabled real-time viewing and playback during debriefing sessions.
Phase 3: Workshop Implementation
Each training session lasted six hours and included 14 participants (4 physicians, 6 nurses, and 4 care assistants). In each workshop, three clinical scenarios were developed: a patient with sepsis, a polytrauma patient, and a patient with a difficult airway (see Appendix B). Following each scenario, a structured debriefing was conducted with the entire team. The educational methodology integrated both technical skills (e.g., manual ventilation techniques) and non-technical competencies such as leadership, communication, and teamwork, all within a multidisciplinary framework. A key innovation was the identification of systemic factors contributing to patient risk, offering a broader perspective on safety improvement.
Phase 4: Identification of Implementation Areas
After each workshop, the teaching team prepared a summary report outlining areas for improvement and potential safety interventions. These reports were submitted to the Head of Service, Unit Supervisor, and, where appropriate, the Health Risk Commission and hospital management.
At the end of the workshops, all participants were asked to complete an evaluation survey (see Table 3) to assess the course objectives, methodology, and supporting materials. Each item is rated on a scale from 0 to 5, and the results are presented as mean values and standard deviations.
3. Results
The development of the workshops enabled the identification opportunities and develop local protocols/recommendations aimed at improving patient safety. One of the main outcomes was the creation of a protocol for the distribution of roles and responsibilities among healthcare professionals during resuscitation scenarios. Emphasis was placed on pre-established role assignments at the onset of resuscitations, which are now updated with each shift change to ensure consistency and preparedness.
Additionally, the need for a unified airway management protocol was identified to standardize criteria and streamline preparation. The massive transfusion protocol (see Figure 2) and the protocol for differentiating urgency/emergency in triage (see Table A1) were also revised. To further support process standardization, cognitive aids and visual tools were introduced, providing accessible resources for health professionals (see Table A2).
Among the tools implemented was the SBAR technique—a structured communication model designed to ensure accurate and efficient transfer of patient information. SBAR consists of four components:
Situation: Describe the current situation, including name, role, unit, and relevant changes in the patient’s condition or treatment plan.
Background: Provide clinical background such as age, sex, diagnosis, and ongoing treatments.
Assessment: Present an evaluation of the patient’s condition based on signs and symptoms.
Recommendation: Offer a recommendation or request specific instructions.
This tool has been successfully disseminated and standardized within the unit, improving communication between professionals and across care units such as the mobile ICU and intensive care unit.
The workshops also led to the formation of a multidisciplinary working group tasked with reviewing the triage process in the emergency department. This included evaluating the personnel involved and refining assessment criteria to optimize patient flow and prioritization.
Student evaluations were completed by the 112 participants and were very positive, with an average of 4.96 ± 0.268 out of 5 in relation to the objectives and contents of the course and an average of 4.87 ± 0.426 in relation to the methodology and documentation.
4. Discussion
We believe that effective crisis management requires specific skills that can be identified, taught, and practiced. There are well-established examples in fields such as aviation and the military, as well as in medical specialties like anesthesiology, where professionals operate under similar conditions of dynamism, pressure, complexity, uncertainty, and risk [1,5,7,13]. In this context, it is essential to actively address human factors and errors, and to develop strategies that can be applied across emergency services. In highly complex environments, experience and knowledge alone are often insufficient. Mistakes frequently occur in dynamic situations, many of which could be prevented through prior training [14,15,16].
Theoretical knowledge alone is not enough in crisis management; practical training is equally important [5,13]. Resource management during critical events requires structured analysis and reflection (debriefing), guided by experienced instructors following simulation-based scenarios. These sessions allow participants to evaluate their actions and reflect on cognitive processes, psychomotor skills, and emotional responses to enhance future performance. We firmly believe that this approach significantly enhances learning and facilitates the transfer of acquired skills to real clinical settings, or at least initiates actions to improve service delivery (e.g., protocols and cognitive aids). Importantly, this is achieved without compromising patient or staff safety [12,17,18,19,20,21,22].
The Advanced Simulation Centre of Integrated Care Management in Ciudad Real not only reviews clinical practices in response to critical incidents but also proactively identifies systemic risks to patient safety. Communicating these risks to relevant stakeholders (e.g., Risk Commission and hospital management) enables a proactive approach to safety and contributes to a safer healthcare organization [23].
The discussion phase of the debriefing process is crucial, involving deep, transparent, and shared reflection on individual and team behaviors. A psychologically safe environment is established to support this analysis. Instructors guide participants through effective debriefing techniques, such as “Debriefing with Good Judgment,” which begins with curiosity and seeks to understand the rationale behind specific actions. This method allows for tailored feedback based on the gap between expected and observed performance, helping participants develop more effective responses in future scenarios [24,25,26,27,28,29].
The implementation of brief, on-site training sessions incorporating interprofessional briefings could be an effective strategy for improving collaboration among healthcare professionals without significantly disrupting clinical workflows [30].
Simulation-based training also serves as a tool for identifying potential patient safety risks, aiming to maximize its impact on both patients and healthcare professionals. By incorporating the health risk management cycle into the simulation process, risks can be proactively identified and analyzed before harm occurs. This methodology supports the implementation of improvement strategies that can be extended across clinical and administrative processes within the organization. In addition, these workshops may serve as a valuable mechanism for identifying operational deficiencies within the department and for promoting the development of new clinical protocols or guidelines aimed at enhancing patient care and management [31]
This study presents several important limitations that should be acknowledged. First, the absence of a control group limits the ability to draw causal inferences regarding the effectiveness of the intervention. Second, the voluntary nature of participation may have introduced selection bias, as individuals more motivated or interested in simulation-based training may have been more likely to enroll. Third, the use of self-reported measures—particularly those related to satisfaction and perceived learning—may be subject to measurement bias. Fourth, no checklists or objective performance measures were collected during the simulation scenarios, which limits the ability to assess changes in technical or non-technical skills. Fifth, the findings are based on data from a single institution, which restricts the generalizability of the results to other healthcare settings. Sixth, it has not yet been possible to study the actual adoption of the protocols developed during the workshops, and no implementation metrics are currently available, as the process remains in a developmental phase. Finally, this study did not include patient-level outcome data, which limits the ability to assess the direct impact of the training on clinical practice and patient safety.
5. Conclusions
This study presents the implementation of innovative simulation-based training techniques for crisis resource management in the emergency department. The initiative showcases the use of simulation as an increasingly valuable educational tool that facilitates effective teamwork training. Through this project, healthcare professionals were able to develop competencies that are otherwise difficult to acquire in conventional training environments, ultimately enhancing workplace safety—particularly in areas such as the massive transfusion protocol.
The integration of this methodology into the continuous professional development of healthcare teams has introduced new stimuli and motivation, fostering a culture of safety and collaboration within emergency care settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Billings C.E. Reynard W.D. Human Factors in Aircraft Incidents: Results of a 7-Year Study Aviat. Space. Environ. Med.1984559609656497826 · pubmed ↗
- 2Howard S.K. Rosekind M.R. Katz J.D. Berry A.J. Fatigue in Anesthesia: Implications and Strategies for Patient and Provider Safety Anesthesiology 2002971281129410.1097/00000542-200211000-0003512411816 · doi ↗ · pubmed ↗
- 3Smith-Coggins R. Howard S.K. Mac D.T. Wang C. Kwan S. Rosekind M.R. Sowb Y. Balise R. Levis J. Gaba D.M. Improving Alertness and Performance in Emergency Department Physicians and Nurses: The Use of Planned Naps Ann. Emerg. Med.200648596604596–604, 604.e 1-310.1016/j.annemergmed.2006.02.00517052562 · doi ↗ · pubmed ↗
- 4Butterworth J.F. Mackey D.C. Wasnick J.D. Morgan and Mikhail’s Clinical Anesthesiology 7th ed.Mc Graw-Hill Education New York, NY, USA 20229781260473795
- 5Gaba D.M. Fish K.J. Howard S.K. Burden A.R. Crisis Management in Anesthesiology Preceded by (work) Gaba, D.M.Saunders Amsterdam, The Netherlands 20149781455738090
- 6Rall M. Oberfrank S. [Human Factors and Crisis Resource Management: Improving Patient Safety]. TT—“Human Factors” Und “Crisis Resource Management”: Erhöhung Der Patientensicherheit Unfallchirurg 201311689289910.1007/s 00113-013-2447-524097240 · doi ↗ · pubmed ↗
- 7Carne B. Kennedy M. Gray T. Review Article: Crisis Resource Management in Emergency Medicine Emerg. Med. Australas.20122471310.1111/j.1742-6723.2011.01495.x 22313554 · doi ↗ · pubmed ↗
- 8Reznek M. Smith-Coggins R. Howard S. Kiran K. Harter P. Sowb Y. Gaba D. Krummel T. Emergency Medicine Crisis Resource Management (EMCRM): Pilot Study of a Simulation-Based Crisis Management Course for Emergency Medicine Acad. Emerg. Med.20031038638910.1197/aemj.10.4.38612670855 · doi ↗ · pubmed ↗