Acute Non-ST-Elevation Myocardial Infarction in a 26-Year-Old Woman: A Case Report
Munish Sharma, Subina Sapkota, Salim Surani, Anjali M Gaalla, Neha Chandna

TL;DR
A 26-year-old woman with hypertension, diabetes, and dyslipidemia experienced a heart attack, highlighting the need for early screening in young individuals with comorbidities.
Contribution
This case report highlights the increasing incidence of premature coronary artery disease in young females with comorbidities.
Findings
The patient had non-ST-elevation myocardial infarction with anteroseptal T-wave inversion and elevated troponin.
Coronary angiography revealed LAD artery stenosis, treated with angioplasty and a drug-eluting stent.
The case emphasizes early cardiovascular screening in young individuals with comorbidities, not just traditional risk factors.
Abstract
Acute coronary syndrome (ACS) in young females is uncommon. The presence of different comorbidities like hypertension, diabetes, and dyslipidemia increases the risk of ACS. Adverse outcomes can be prevented by having early recognition and intervention. A 26-year-old female with a history of hypertension, diabetes mellitus, and dyslipidemia presented with initially intermittent left-sided chest pain radiating to the jaw but progressive in the last five days and associated with left arm numbness. Her ECG showed anteroseptal T-wave inversion, and her troponin level was also elevated. Echocardiography revealed anteroseptal hypokinesia with an ejection fraction of 45%. The diagnosis was made of non-ST-elevation myocardial infarction. Additionally, on coronary angiography, stenosis of the proximal to mid-left anterior descending (LAD) artery was shown, for which she underwent successful…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
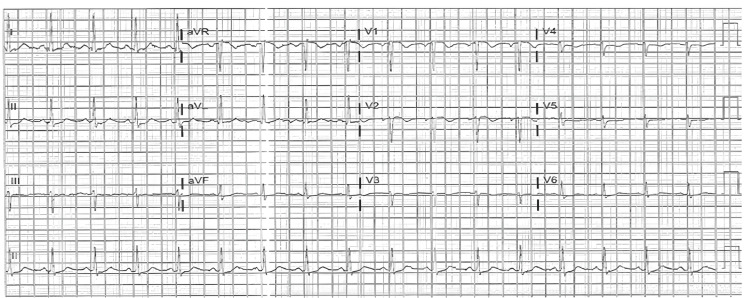 Figure 1
Figure 1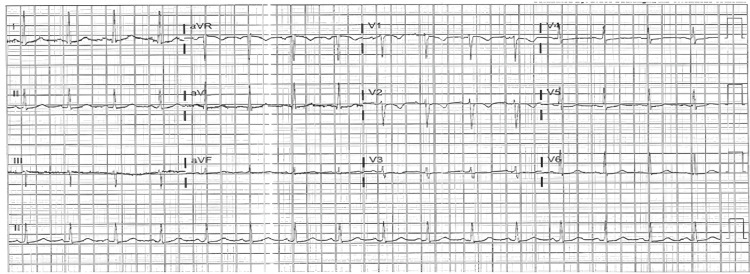 Figure 2
Figure 2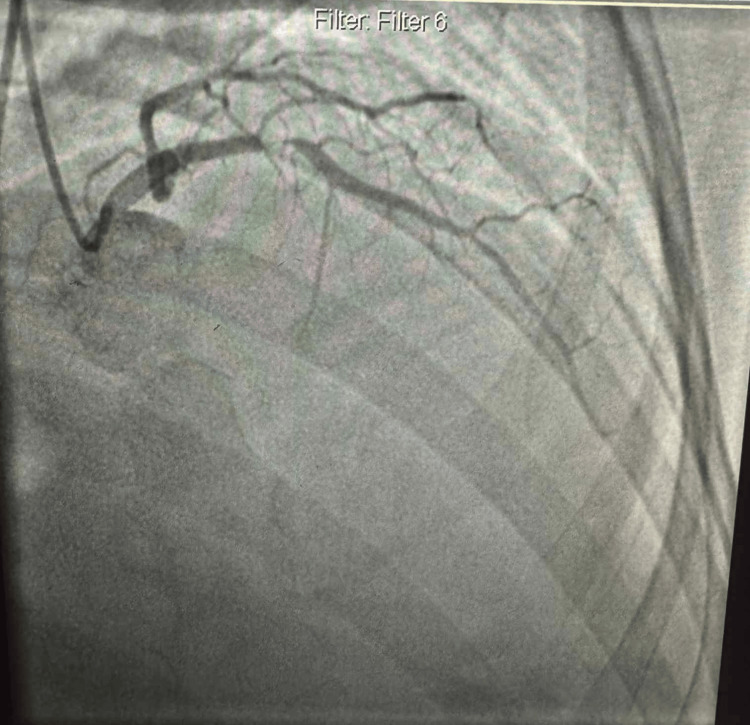 Figure 3
Figure 3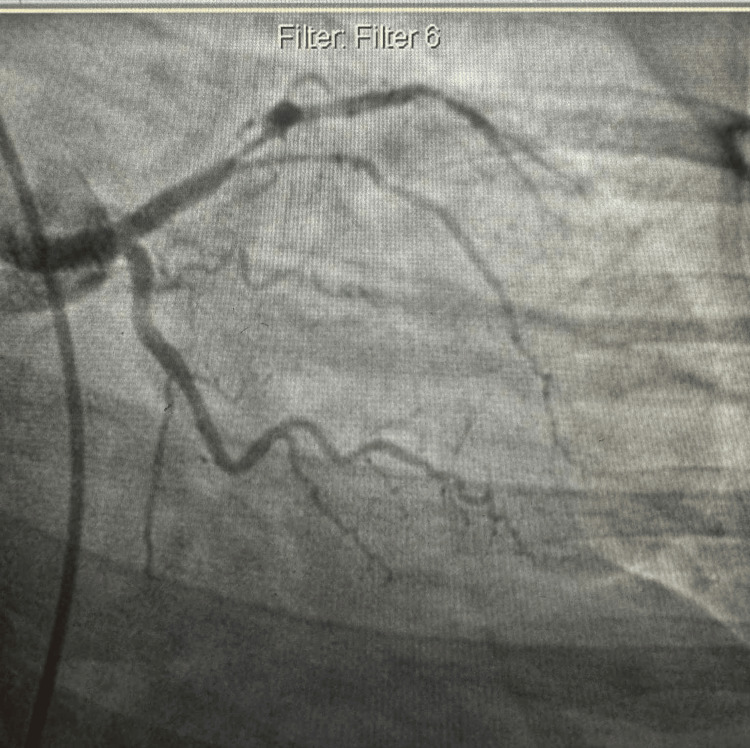 Figure 4
Figure 4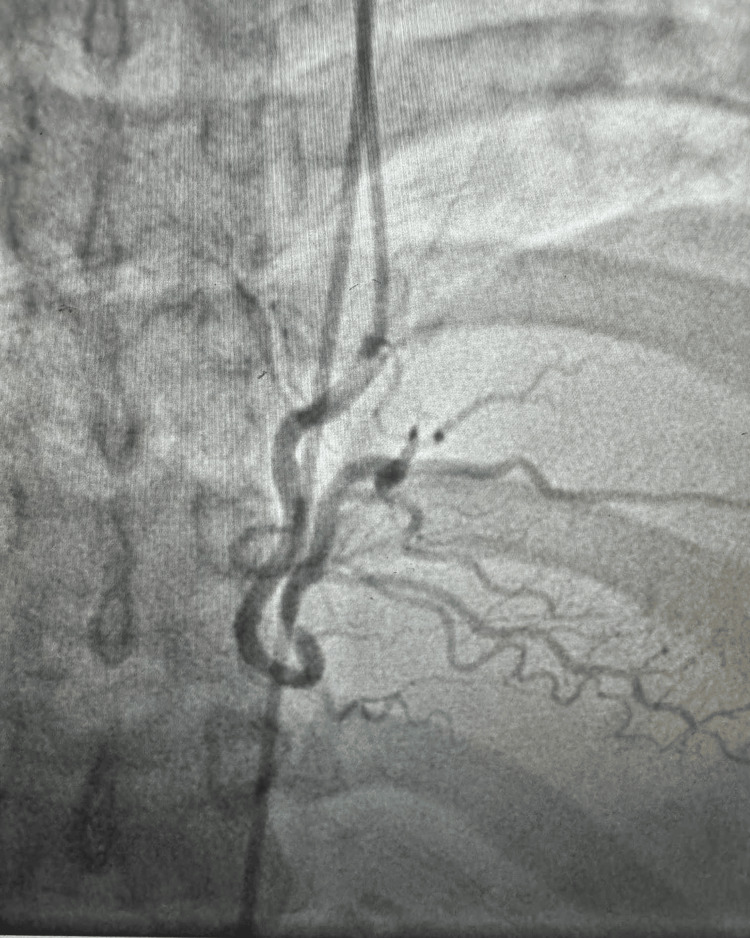 Figure 5
Figure 5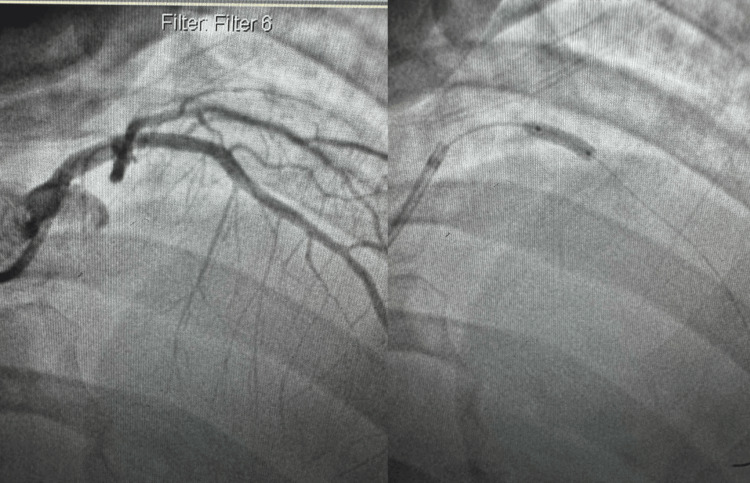 Figure 6
Figure 6| Lab values | Ranges | |
| WBC | 9.9 | 4.8-10.8 10 x 3/ul |
| RBC | 4.13 L | 4.30-6.00 10 x 6/UL |
| Hemoglobin | 8.9 L | 11.5-16G/dl |
| Hematocrit | 28.2 L | 35-48% |
| MCV | 68.3 L | 80-100 fl |
| MCH | 21.6 L | 26-34 pg |
| MCHC | 31.6 L | 32-36 g/dl |
| PLT | 244 | 130-450 10 x 3/ul |
| Sodium | 138 | 135-145 mmol/l |
| Potassium | 3.5 | 3.5-5.0 mmol/l |
| Chloride | 105 | 95-112 mmol/l |
| Glucose, quant | 148 H | 70-100 |
| Calcium | 7.9 | 8.7-10.7 mg/dl |
| BUN | 16 | 6.0-20.0 mg/dl |
| CO2 | 25 | 21-31 mmol/l |
| Creatinine | 0.94 | 0.05-1.20 mg/dl |
| Anion gap | 11.5 | 8-16 |
| GFR | >60 | - |
| Calculated osmolality | 280 | 270-300 mosm/kg |
| PT | 12.9 H | 11.0-12.8 secs |
| INR | 1.1 | 0.9-1.1 |
| POC glucose whole blood | 357 CH | 70-100 mg/dl |
| CK-MB | 6.1 CH | 0-3.9 ng/ml |
| Troponin I | 2684 NG/L | Below 0.04 ng/l |
| Pregnancy test | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Acute Myocardial Infarction Research · Cardiac Imaging and Diagnostics
Introduction
Acute coronary syndrome (ACS) consists of ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, and unstable angina. Among these, non-ST-elevation myocardial infarction (NSTEMI) remains a significant cause of morbidity and mortality worldwide. However, its presentation in young females, especially under 30 years of age, is relatively rare and often underrecognized [1]. Previously, it was considered a condition predominantly affecting males. However, recent studies suggest an alarming increase in cardiovascular events in young women due to metabolic syndrome components such as hypertension, diabetes, and dyslipidemia [1]. In this case, we present a 26-year-old female with no history of smoking or alcohol use who developed NSTEMI but with a history of hypertension, dyslipidemia, and diabetes mellitus, and required urgent percutaneous coronary intervention (PCI) for LAD artery stenosis.
According to the WHO, cardiovascular diseases are the cause of most non-communicable disease (NCD) deaths. About 19 million deaths in 2021. Metabolic changes that increase the risk of NCDs include high blood pressure, obesity, overweight, diabetes, and abnormal blood lipids. Among these, the leading metabolic risk factor globally is elevated blood pressure; about 25% of global NCD deaths are attributed to this, followed by raised blood glucose and overweight/obesity. Among the cardiovascular diseases, coronary artery disease (CAD) is the most common cause. In the USA, about one in 20 adults aged 20 and older has CAD. In 2023, about one out of every six deaths from cardiovascular diseases was in adults younger than 65 years old [2-3].
Case presentation
A 26-year-old female presented with symptoms of left-sided chest pain on and off, with left arm numbness. According to her, the chest discomfort started three days ago. She developed acute chest pain while dancing, which radiated to the right side of her jaw. Initially, she thought it was a tooth problem, but the pain did not subside, and she was taken to the emergency room and was later found to have elevated troponin. On admission, the patient seemed to be comfortable. Her blood pressure was 133/90 mmHg, and her heart rate was 106 beats per minute. On review of the cardiovascular system, she had chest pain with radiation to the jaw and left arm, and left arm numbness in the neurological system; however, the systemic examination was unremarkable.
Her past history was significant for hypertension, diabetes on insulin glargine, and hyperlipidemia on statin, with no history of smoking or alcohol consumption. In the emergency room, she was started on a heparin drip using a weight-based protocol, an aspirin and Plavix loading dose, and nitroglycerin 0.4 mg sublingual as needed.
Investigations
The ECG showed a normal sinus rhythm with some anteroseptal T-wave inversion. Additionally, echocardiography revealed a mild decrease in left ventricular systolic function with anteroseptal hypokinesia and 45% of ejection fraction, mild mitral and tricuspid insufficiency, and mild left atrial dilation. Her troponin level was 2684 nanograms/liter (normal range less than 4 ng/l), creatinine kinase-MB 6.1 nanograms/liter (0-3.9 ng/ml), and creatinine kinase was around 100 U/L (MOU2) (25 to 200 U/L). The detailed lab data are shown in Table 1.
With elevated cardiac enzymes, abnormal electrocardiography (Figures 1-2), and an echocardiogram, the diagnosis of ACS (NSTEMI) was confirmed. The patient underwent a coronary angiogram, revealing stenosis of the proximal to mid-left anterior descending (LAD), for which she underwent percutaneous transluminal coronary angioplasty, and a drug-eluting stent of the proximal and mid-LAD was performed (Figures 3-6). The lesion appeared as severe (almost 99%) stenosis in the proximal to mid LAD with thrombolysis in myocardial infarction 3 flow. Intravascular imaging was not performed in this case. However, spontaneous coronary artery dissection (SCAD) was considered part of the differential. There were no typical features of SCAD, such as multiple radiolucent lumens, contrast staining, or long smooth narrowing without atherosclerotic changes.
12-lead ECG demonstrating sinus tachycardia with a heart rate of approximately 105 beats per minute. There are non-specific ST-segment and T-wave abnormalities noted, without acute ST-segment elevation or depression. No pathological Q waves or significant arrhythmias are observed.ECG: electrocardiogram
12-lead ECG demonstrating sinus tachycardia with a heart rate of approximately 105 beats per minute. There are non-specific ST-segment and T-wave abnormalities noted, without acute ST-segment elevation or depression. No pathological Q waves or significant arrhythmias are observed.ECG: electrocardiogram
Coronary angiography in the right anterior oblique view revealed a severe mid-LAD stenosis, while the circumflex artery appeared patent.LAD: left anterior descending
Coronary angiography in the anterior-posterior caudal view revealed a severe mid-LAD stenosis, while the circumflex artery appeared patent.
Coronary angiography showed no significant diseases in the right coronary artery.
Coronary angiography image in the right anterior oblique view showing balloon angioplasty and deployment of a drug-eluting stent in the proximal to mid-segment of the LAD artery. Post-stenting, the LAD is patent with no residual stenosis.LAD: left anterior descending
The patient's hospitalization course was stable, and she was discharged home within 48 hours on a low-dose aspirin regimen (81 mg), clopidogrel (75 mg) daily, and atorvastatin (40 mg) daily, in addition to her home insulin regimen, as mentioned before. The patient was stable and doing well at her outpatient follow-up visits, with the latest visit occurring six months post-procedure.
Discussion
This case shows an evolving pattern of premature CAD in young women. Here, our patient had major metabolic risk factors: hypertension, diabetes mellitus, and dyslipidemia. These factors synergistically contribute to endothelial dysfunction, atherosclerosis, and plaque instability. Despite her young age, the presence of these comorbidities placed her at significant risk.
ACS in a 26-year-old female is often not recognized since it is typically common in the middle-aged or older population due to the increasing obesity, diabetes, and chronic kidney disease, and the increasing detection of myocardial necrosis by troponin [4]. Therefore, it is important to maintain a high index of suspicion for myocardial infarction even in young patients, especially those with multiple comorbidities.
This patient had strong risk factors, including hypertension, diabetes mellitus, and dyslipidemia. These likely contribute to accelerated atherosclerosis and early CAD. Her presentation with elevated troponin and non-ST changes on ECG led to the diagnosis of NSTEMI, and left heart catheterization, selective coronary angio, and left ventricular angiogram findings suggest CAD with critical stenosis of the proximal to mid-LAD artery. Additionally, the patient underwent percutaneous transluminal coronary angioplasty and a drug-eluting stent of the proximal LAD artery and was discharged in stable condition.
From the study of risk factors of ACS in young age, risk factors like diabetes mellitus, high BMI, obesity, hypercholesterolemia, hypertension, smoking, and family history increased the acute coronary risk in young women. A total of 7,042 patients met the inclusion criteria for this meta-analysis, as reported in seven studies [5]. Screening methods, such as routine blood pressure measurement, fasting lipid profile, hemoglobin A1c, or fasting blood glucose testing, along with assessment of BMI/waist circumference, can aid in early diagnosis in young adults with a family history or multiple risk factors.
Additionally, from the study of Modifiable Risk Factors in Young Adults With First Myocardial Infarction, 1,462,168 young adults with a first acute myocardial infarction (mean age 50 +-7 years, 71.5% men, 58.3% White), of whom 19.2% were 18 to 44 years of age. In the 18- to 44-year-old group, smoking (56.8%), dyslipidemia (51.7%), and hypertension (49.8%) were most prevalent, and 90.3% of patients had at least one risk factor. Women had a higher prevalence of diabetes mellitus, hypertension, and obesity, and men had a higher prevalence of dyslipidemia, drug abuse, and smoking [6]. SCAD, anomalous origin or course of coronary artery, coronary vasospasm, stress-induced cardiomyopathy, myocarditis, and myopericarditis are some of the cardiac differential diagnoses that should be kept in mind in a young patient presenting with ACS-like symptoms.
According to the 2025 American College of Cardiology/American Heart Association/American College of Emergency Physicians/National Association of Emergency Medical Service Physicians/Society for Cardiovascular Angiography Intervention guideline for the management of patients with ACS, our patient underwent PTCI targeting the LAD [7]. This patient was at intermediate to high risk of ischemic event and was an appropriate candidate for revascularization, an invasive approach with intent to proceed with revascularization recommended during hospitalization to reduce MACE [7]. Early diagnosis and aggressive secondary prevention are essential to reduce future cardiovascular events and mortality.
Conclusions
This case highlights the importance of recognizing premature atherosclerosis, particularly in patients with multiple risk factors. Additionally, a high index of suspicion for ACS in young women, especially those with multiple cardiovascular risk factors, should be maintained. It reinforces the fact that traditional age and gender stereotypes should not guide clinical judgment. It supports early cardiovascular screening, risk factor control, and timely intervention to reduce the global burden. Early diagnosis through appropriate imaging and biomarkers, timely PCI, and aggressive risk factor modification remain the cornerstone of management. Secondary prevention can also be done by taking statins, ACE inhibitors, beta blockers, antiplatelets, and strict lifestyle modification for long-term prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute myocardial infarction in women: a scientific statement from the American Heart Association Circulation Mehta LS Beckie TM De Von HA 91694713320162681131610.1161/CIR.0000000000000351 · doi ↗ · pubmed ↗
- 2Noncommunicable diseases 2025 https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
- 3Heart disease facts 2024 https://www.cdc.gov/heart-disease/data-research/facts-stats/index.html
- 4Harrison's principles of internal medicine, 21e Loscalzo J Fauci A Kasper D Hauser S Longo D Jameson JL New York (NY)Mc Graw Hill 2022 https://accessmedicine.mhmedical.com/book.aspx?bookid=3095
- 5The risk factors of acute coronary syndrome in young women: a systematic review and meta-analysis Curr Cardiol Rev Siagian SN Christianto C Angellia P Holiyono HI 16112221096919202310.2174/1573403 X 19666221116113208 PMC 1028099736397628 · doi ↗ · pubmed ↗
- 6Modifiable risk factors in young adults with first myocardial infarction J Am Coll Cardiol Yandrapalli S Nabors C Goyal A Aronow WS Frishman WH 5735847320193073271110.1016/j.jacc.2018.10.084 · doi ↗ · pubmed ↗
- 72025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines Circulation Rao SV O'Donoghue ML Ruel M 771862151202510.1161/CIR.000000000000130940014670 · doi ↗ · pubmed ↗