The Impact of SGLT2 Inhibitors on Pulmonary Artery Pressures and Pulmonary Hemodynamics in Patients With Heart Failure: A Systematic Review
Kritick Bhandari, Maria Qadri, Rochak Dhakal, Sagun Ghimire, Gyanendra Jora, Santosh Basyal, Sanjit Kumar Shah

TL;DR
This study finds that SGLT2 inhibitors may lower pulmonary artery pressures in heart failure patients, suggesting potential benefits for lung function.
Contribution
The paper provides the first systematic review of SGLT2 inhibitors' effects on pulmonary hemodynamics in heart failure patients.
Findings
SGLT2 inhibitors significantly reduce mean pulmonary artery pressure at rest in heart failure patients.
Preliminary evidence suggests a trend toward reduced pulmonary artery systolic pressure after SGLT2 inhibitor use.
Secondary outcomes show significant reductions in PCWP, PADP, and NT-proBNP with SGLT2 inhibitors.
Abstract
Heart failure is a major global health burden associated with high morbidity and mortality. Elevated pulmonary artery pressures (PAP) are linked to worse outcomes in heart failure patients. Sodium–glucose cotransporter 2 (SGLT2) inhibitors, initially developed for diabetes, have demonstrated cardiovascular benefits, but their specific effects on pulmonary hemodynamics remain unclear. This systematic review analyzed randomized controlled trials and observational cohort studies evaluating the effects of SGLT2 inhibitors on mean pulmonary artery pressure (mPAP) and pulmonary artery systolic pressure (PASP) in heart failure patients. A comprehensive search of PubMed, Embase, Cochrane Library, and Scopus databases was conducted until August 2024. Studies were appraised using PRISMA and AMSTAR guidelines, the Cochrane bias tool, and the Newcastle–Ottawa Scale. SGLT2 inhibitors reduce PAPs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
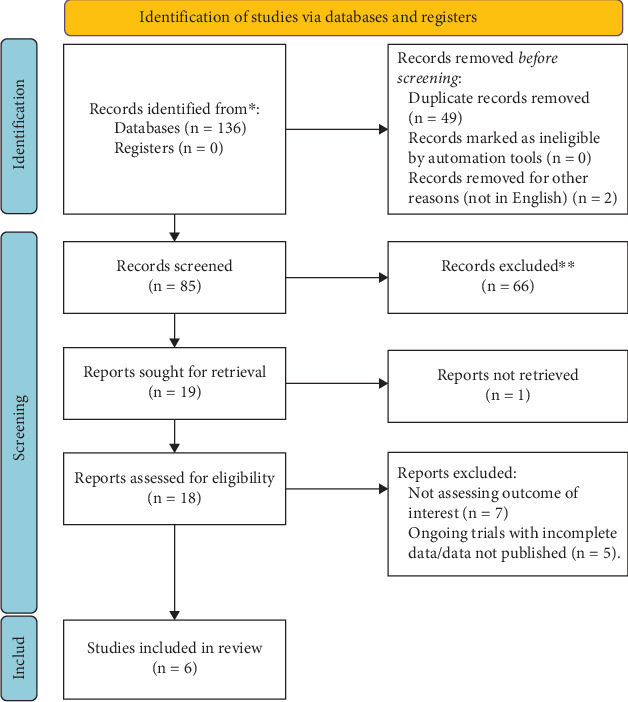 Figure 1
Figure 1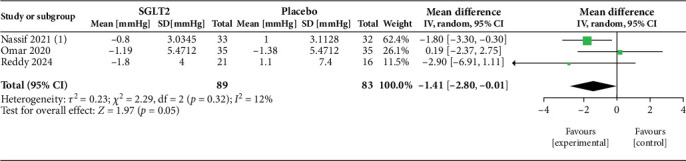 Figure 2
Figure 2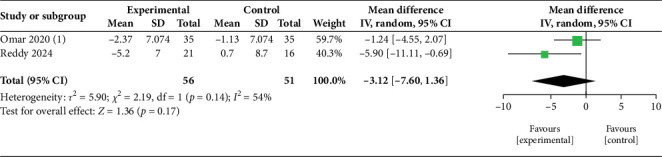 Figure 3
Figure 3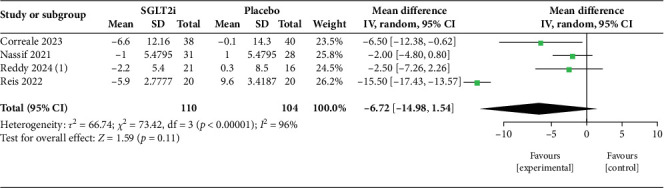 Figure 4
Figure 4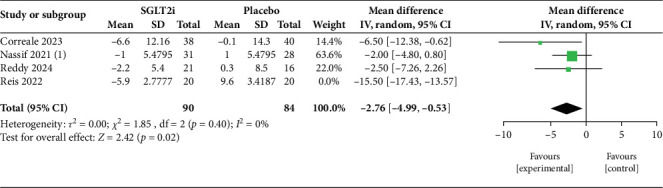 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Cardiovascular Function and Risk Factors · Diabetes Treatment and Management
1. Background
Heart failure (HF) remains one of the most significant health problems of the western world, affecting over 6.7 million Americans over the age of 20, and the prevalence is expected to rise to 11.4 million by 2050 [1]. Patients with HF are frequently classified based on ejection fraction (EF) into three main categories: heart failure with reduced ejection fraction (HFrEF) (EF < 40%), midrange EF (EF between 40% and 49%), and heart failure with preserved ejection fraction (HFpEF) (EF > 50%) [2]. Numerous pharmacological and mechanical interventions have been developed to combat HF, but these have mostly helped improve the quality of life and prognosis of patients with HFrEF [3]. Management lags by a significant amount for patients with HFpEF, despite both having similar prognoses. The pulmonary circulation has been gaining attention in recent years as a potential therapeutic target for HF patients. This is because elevated pulmonary artery pressures (PAPs) have been strongly associated with worse prognosis and increased hospitalization and mortality in HF patients [4]. Many patients with diastolic dysfunction have chronically elevated pulmonary pressures, which results in pulmonary vascular remodeling, pulmonary hypertension (PH), and right ventricular (RV) dysfunction. This increase in RV pressure and RV dysfunction ultimately results in worse prognosis in HF patients [5, 6]. Recent evidence suggests that even subtly elevated mean pulmonary artery pressure (mPAP) can pose a significant threat in HF populations, and as such, greater emphasis on early diagnosis of PH has been placed [7]. Despite being a major public health issue in HF populations, a proper consensus regarding the diagnosis and management of PH is still an area that remains quite unexplored [8]. One of the emerging drugs in HF therapy that has gained significant attention is sodium–glucose cotransporter 2 inhibitors (SGLT2 inhibitors). Originally designed as an antidiabetic medication, this group of drugs has shown promising outcomes in cardiovascular improvements, and its utility in HF patients is being explored [2]. Although SGLT2 inhibitors have demonstrated promising results in reducing cardiovascular events and improving HF outcomes, their specific effects on PAP remain underexplored. Given the limitations of existing recommendations regarding the effect of SGLT2 inhibitors in pulmonary hemodynamics, there was a growing need to explore the potential of these drugs in the pulmonary circulation. This could help address gaps in treatment, offering a more comprehensive strategy for managing HF, particularly in patients with elevated PAP.
This systematic review is aimed at critically exploring and assessing the effects of SGLT2 inhibitors on PAP in patients with HF. The goal is to evaluate the therapeutic efficacy of SGLT2 in the modulation of pulmonary pressures and pulmonary hemodynamics and to assess their impact on overall cardiac function, so as to analyze their potential capacity to improve outcomes in HF patients.
2. Methods
2.1. Study Protocol
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement and AMSTAR (assessing the methodological quality of systematic reviews) guidelines [9, 10]. The PRISMA and AMSTAR checklist is presented in supporting information (Appendices S1 and S4). Additionally, the review methods were established prior to the conduct of the review, and we have registered the systematic review in the database of PROSPERO with ID: CRD42024583533.
2.2. Study Selection
Publications examining mPAP and pulmonary artery systolic pressure (PASP) change values during both rest and physical exercise in HF patients taking SGLT2 inhibitors were identified by a Medline search using a comprehensive search strategy (Appendix S2). Systematic searches of online databases such as Embase, PubMed, Scopus, and Cochrane Library until 22 August 2024 were conducted to find the relevant articles. The search strategy consisted of Medical Subject Headings (MeSH) terms, keywords, and search terms such as: “Heart failure”, “Sodium-Glucose Transporter 2 Inhibitors”, “Pulmonary wedge pressure”, “Heart failure, Diastolic”, and “Heart failure, Systolic”. Appropriate Boolean operators “AND”/”OR” were used between the aforementioned terminologies. We used Zotero to store the studies that were considered eligible, with limitations only to publications in the English language, which could introduce language bias. The details of the search strategy are shown in the supporting information (Appendix S2).
Original randomized control trials (RCTs), observational cohort studies, and case-controlled studies on the impact of SGLT2 inhibitors versus placebo or optimum medical therapies (OMTs) on mPAP or PASP changes were included. RCTs were prioritized for their ability to establish causality and minimize bias through randomization. Observational studies, including cohort and case-control designs, were included to complement RCT findings by reflecting real-world clinical practices and providing insights into broader patient populations and longer follow-up periods. A secondary search reviewed the reference lists of relevant papers. When studies could not be retrieved, their authors were contacted to request a copy of the publication. Duplicate screening was done by Zotero. Two reviewers (K.B. and S.G.) independently screened the studies identified by the searches after the duplicate removal. Differences over the inclusion of studies were resolved by consensus reached after discussion with a third reviewer. The studies were assessed based on key characteristics such as intervention (SGLT2 inhibitors), population (HF patients), and outcomes (PAPs). The final selection was made by comparing these characteristics against predefined inclusion and exclusion criteria.
2.3. Search Techniques
Using the population, intervention, comparison, and outcome (PICO) criteria, a thorough review of the literature was carried out. The details of the search technique are given in the supporting information (Appendix S2).
Inclusion and exclusion criteria:
To accomplish our research objectives, we defined precise inclusion and exclusion criteria. Table 1 provides an overview of our criteria.
2.4. Quality Appraisal
We made use of a variety of quality assessment tools to ensure the validity of the papers we chose. For randomized clinical trials, we used the Cochrane risk of bias tool assessment. The Newcastle–Ottawa tool scale was used to evaluate observational/case-control studies. Only studies with low and intermediate risk of bias were included in the review. The details of quality assessment are presented in the supporting information (Appendix S3).
2.5. Data Extraction and Management
Studies obtained from the electronic databases, supplementary sources, and manual searching were exported to Zotero in a compatible format. Duplicate articles were screened first by Zotero and then manually. Duplicates were then recorded and removed. For multiple publications of the same data in more than one journal, the most inclusive, comprehensive studies, with larger sample sizes and the most recent ones were considered. Basic data extraction was conducted in a Microsoft Excel spreadsheet. Two reviewers (K.B. and M.Q.) extracted the data independently, and a third reviewer conducted a final revision of the collected data.
The spreadsheet captured key information, including study design, sample size, follow-up duration, publication date, participant demographics (age, sex, and ethnicity), drug used, HF type, baseline left ventricular EF, baseline NT-proBNP levels, baseline New York Heart Association (NYHA) functional class, comorbidity at baseline, and outcomes (main and additional).
2.5.1. Data Synthesis and Analysis
The effect measure used for the main outcome (change in mPAP or PASP) and all additional outcomes (pulmonary artery diastolic pressure [PADP], pulmonary vascular resistance [PVR], pulmonary capillary wedge pressure [PCWP], and NT-proBNP) is the mean difference.
Due to the presence of missing data across some studies required for meta-analysis, we opted to tabulate findings from all the studies and create forest plots only from those studies that provided complete datasets. Where possible, we attempted to fill these gaps by extracting missing data following guidelines outlined in the Cochrane Handbook for Systematic Reviews Version 6.5 [11]. For studies that reported changes only in PASP, we derived mPAP using the internationally recognized formula: mPAP = 0.61 × PASP + 1.95 mmHg. The SD for mPAP can also be derived from the formula for PASP. Since the mPAP formula involves a linear transformation of PASP, the standard deviation of mPAP can be obtained as SD_mPAP_ = 0.61 × SD_PASP_. This approach allowed us to synthesize the available data meaningfully while acknowledging the limitations posed by the incomplete datasets. However, the precision of these estimated effects could not be fully reliable, and this lack of accurate data may have affected the robustness of our synthesis. Thus, we did not use the derived data while generating forest plots and only used them in tabular form.
We used tables to organize and visually display the results of individual studies. These tables summarized key characteristics of the included studies, such as study population, demographics, baseline values, intervention type (e.g., empagliflozin [EMPA] vs. dapagliflozin [DAPA]), and main outcomes (e.g., changes in mPAP and PASP) and secondary outcomes (PADP, PCWP, PVR, and NT-proBNP). To explore potential causes of heterogeneity among study results, we conducted subgroup analyses. Specifically, we compared rest and exercise hemodynamics to determine whether the effects of SGLT2 inhibitors differed based on the physiological state during measurements. Additionally, we performed subgroup analyses comparing the effects of EMPA and DAPA to assess any variations in their impact on PAPs. These analyses helped identify whether differences in treatment or hemodynamic conditions contributed to heterogeneity in the study outcomes.
To assess the risk of bias due to missing results in the synthesis, we considered potential reporting biases, such as selective outcome reporting or incomplete reporting of key data. We reviewed each study to determine if all prespecified outcomes were fully reported, as per their protocols or methods sections. Additionally, we checked for discrepancies between reported outcomes in the main text and supporting information. Studies that failed to report key outcomes, such as changes in PAPs (mPAP or PASP), were flagged as potentially having a risk of bias.
In cases where data appeared to be missing or selectively reported, we attempted to obtain missing data by consulting supporting information or by referencing the Cochrane Handbook for Systematic Reviews to fill in gaps, particularly regarding methodological details. However, if missing data could not be retrieved, these studies were noted, and their potential impact on the overall conclusions was considered in the narrative synthesis.
2.6. Outcomes
2.6.1. Primary Outcome
-
- Change in mPAP: mPAP reflects the average pressure within the pulmonary artery. It is measured in millimeters of mercury and is calculated using the formula: mPAP = 1/3 PASP + 2/3 PADP. It can also be estimated from PASP using the formula: mPAP = 0.61 PASP + 1.95 mmHg.
Data on mPAP from all available studies were sought, and mPAP values on baseline and the final follow-up were recorded, regardless of the method of measurement (e.g., direct hemodynamic measurements via right heart catheterization (RHC) or noninvasive echocardiographic estimation).
- 2. Change in PASP: The peak pressure in the pulmonary artery during the systolic phase of the cardiac cycle.
Data on PASP from all available studies were sought, and PASP values on baseline and the final follow-up were recorded, regardless of the method of measurement (e.g., direct hemodynamic measurements via RHC or noninvasive echocardiographic estimation).
2.6.2. Secondary Outcomes
-
- Change in PADP: An additional measure of PAP, collected when available. In clinical studies of HF, mPAP and PASP tend to be reported more frequently than PADP. To avoid potential gaps or inconsistencies in the studies, PADP was considered a secondary outcome in our study. Further, mPAP is often derived using PASP and PADP, so including all three parameters could introduce redundancy.
-
- Change in PVR: Represents the pressure in the arteries that supply blood to the lungs.
-
- Change in PCWP: An indirect measure of the left atrial pressure, relevant in assessing HF status.
-
- Change in NT-proBNP levels: NT-proBNP is a biomarker often used to assess the severity of HF and its progression.
3. Results
3.1. Study Selection
Altogether, 136 articles were obtained from the databases of Embase, PubMed, Scopus, and Cochrane Library from inception until 22 August 2024. From the initial search results, 49 duplicate articles were removed and two articles were removed because they were not in the English language. From the remaining 85 articles, 66 articles were removed by screening the title and abstract. Full-text review was done thoroughly on the remaining 19 articles, out of which 13 articles were excluded based on the eligibility criteria. Finally, six full-text articles were included in the analysis. The PRISMA diagram tailoring the details of the study selection process is shown in Figure 1.
3.2. Study Characteristics
These six studies [12–17] mentioned below (Table 2) included 346 HF patients in total, with their sample size ranging from 38 to 78. The studies include RCTs and cohort studies conducted from the year 2020–2024. Most of the studies have reported a mean age of the patients to lie between the mid-60s and late 70s. All studies, with the exception of Reddy et al. [13], comprised a predominant male population. However, in the study by Jariwala and Gururaj [16], the demographic data could not be extracted. Only three of the six retrieved studies had any available data on ethnicity [13–15] and those were primarily white populations. Hypertension, atrial fibrillation, and diabetes mellitus were the main comorbidities in the population. In addition to that, obesity, ischemic heart diseases, chronic kidney disease, chronic obstructive pulmonary disease, and anemia were reported. All included participants were on OMT for HF, while only those participants included in the study by Omar et al. [14] and Correale et al. [17] had additional glucose lowering therapies as baseline medications. Of the six, three studies measured PAPs using echocardiography [12, 16, 17], whereas in two studies, RHC was performed [13, 14] and one study used an implanted PAP sensor (CardioMEMS) (Table 3) [15]. Only one of our studies involved HFpEF [13] patients and two studies involved a population with HFrEF [12, 14], while the rest included HF irrelevant of EF. The most prevalent NYHA classes among the subjects in order of frequency were II, III, and IV. In addition, levels of NT-proBNP varied from 100 to 200 pg/mL to values as high as 2300 pg/mL. Two studies [12, 13] used DAPA as the drug in the intervention group. EMPA was the intervention group drug in three studies [14–16]. Correale et al. [17] used an SGLT2 inhibitor in their intervention group, but this was not specified. The six studies included varied significantly in follow-up duration, assessment techniques, and participant backgrounds, introducing potential heterogeneity in the study.
3.3. Risk of Bias Within Studies
The risk of bias for each included study was assessed using both the Cochrane Risk of Bias 2 (ROB 2) tool for randomized controlled trials and the Newcastle–Ottawa Scale (NOS) for nonrandomized studies. Detailed assessments, including domain-specific evaluations of selection, comparability, and outcome/exposure risks, are provided in the supporting information (Appendix S3). The ROB 2 tool evaluates bias across several domains including the randomization process, deviations from intended interventions, and outcome measurement, while the NOS assesses the quality of cohort and case-control studies based on selection, comparability, and exposure/outcome ascertainment. All of the studies had a low or intermediate risk of bias and thus were included in our review.
3.4. Result
3.4.1. Primary Outcome
Our study included several papers that have explored the efficacy of two SGLT2i drugs separately: DAPA and EMPA. The primary outcomes of our review have been tabulated in Table 4 and demonstrated in Figures 2, 3, 4, and 5. These trials compared the intervention group with either placebo or optimum treatment, concerning their effects on cardiac hemodynamics. The principal findings suggest that SGLT2 inhibitors, compared with placebo or standard care, are associated with meaningful reductions in pulmonary pressures, although the strength and consistency of these effects vary according to clinical setting (rest vs. exercise), study design, and drug type.
3.4.1.1. mPAP
Three studies [13–15] contribute to the pooled estimate of changes in mPAP at rest (Figure 2). The random-effects meta-analysis shows a reduction in mPAP with SGLT2i (MD = −1.41 mmHg; 95% CI: −2.80 to −0.01; p = 0.05). Between-study heterogeneity is low (I^2^ = 12%; τ^2^ = 0.23; χ^2^ = 2.29, df = 2; p = 0.32), supporting a fairly consistent direction of effect across studies. Two studies [13, 14] are pooled to show the effect of exercise on mPAP hemodynamics (Figure 3). The summary effect is not statistically significant (MD = −3.12 mmHg; 95% CI: −7.60 to 1.36; p = 0.17). Heterogeneity is moderate (I^2^ = 54%; τ^2^ = 6.90; χ^2^ = 2.19, df = 1; p = 0.14), suggesting some variability in exercise hemodynamic response, driven largely by the study showing a larger reduction, yet still insufficient for a confident pooled difference. Statistical heterogeneity also likely reflects differences in population characteristics (HFrEF vs. HFpEF).
3.4.1.2. PASP
For PASP, four studies [12, 13, 15, 17] were included in the pooled analysis (Figure 4). The combined effect suggested a reduction with SGLT2i but did not achieve statistical significance (MD = −6.72 mmHg; 95% CI: −14.98 to 1.54; p = 0.11). Heterogeneity was very high (I^2^ = 96%), reflecting wide methodological and population differences between trials, particularly between DAPA- and EMPA-based studies. Importantly, the leave-one-out sensitivity analysis (Figure 5) demonstrated that exclusion of a single high-influence study markedly reduced heterogeneity (I^2^ = 0%) and yielded a statistically significant reduction in PASP (MD = −2.76 mmHg; 95% CI: −4.99 to −0.53; p = 0.02). This highlights that while overall results are sensitive to study-level variability, the underlying direction of effect consistently favors SGLT2i therapy.
Taken together, these findings support the conclusion that SGLT2 inhibitors lower pulmonary pressures in patients with HF, though the magnitude and statistical robustness of the effect vary. The consistency of effect direction, the low heterogeneity in resting mPAP, and the robustness of the PASP signal after sensitivity analysis lend confidence that SGLT2 inhibitors contribute meaningfully to hemodynamic improvement in HF. Nevertheless, further high-quality, head-to-head randomized trials are required to directly compare DAPA and EMPA, standardize exercise protocols, and extend follow-up to determine long-term clinical implications of pulmonary pressure reduction.
3.4.1.3. Subgroup Analysis
- A. Hemodynamics at rest and exercise:
The analysis of pulmonary hemodynamic parameters in patients with HF during rest and exercise revealed a trend toward greater reduction in mPAP and PASP (Table 5). At rest, pooled analysis of three studies [13–15] (Figure 2) demonstrated a modest but borderline significant reduction in mPAP with SGLT2i (MD = −1.41 mmHg; 95% CI: −2.80 to −0.01; p = 0.05). Heterogeneity was low (I^2^ = 12%), suggesting reasonable consistency across trials despite differences in patient populations and measurement techniques. Exercise hemodynamics showed nonsignificant reductions in mPAP. In the study by Reddy et al. [13], the patients underwent exercise to volitional exhaustion, and values were measured via echocardiography; DAPA caused a substantial decrease in mPAP compared to placebo during exercise (−5.9 mmHg, p = 0.02), with a comparable reduction in PASP (−5.3 mmHg); however, the latter did not reach statistical significance. EMPA, in Omar et al.'s [14] study, showed a marginally significant reduction in mPAP during exercise (−2.37 mmHg, p = 0.056), suggesting a trend toward improvement. They used a cycle ergometer exercise test until volition and calculated pulmonary pressures via RHC. The pooled effect across two studies [13, 14] (Figure 3) showed a nonsignificant reduction in mPAP (MD = −3.12 mmHg; 95% CI: −7.60 to 1.36; p = 0.17), with moderate heterogeneity (I^2^ = 54%). This reflects variability in exercise protocols and hemodynamic responses, although both studies favored SGLT2i over placebo. The trend toward larger benefit under stress conditions aligns with the hypothesis that these agents may improve pulmonary vascular compliance or left heart unloading when circulatory demand is increased. More studies are necessary to find out the exact impact of SGLT2 inhibitors on pulmonary hemodynamics during exercise. Further, such changes in pulmonary hemodynamics during exercise may be normal for HF pathophysiology and not specifically due to SGLT2 inhibitors. The heterogeneity due to the different types of exercise tests used and the method of measuring the variables should also be considered.
- B. DAPA Versus EMPA:
Two notable studies with DAPA as the intervention drug, Reis et al. [12] and Reddy et al. [13], demonstrated statistically significant impacts on the primary outcomes. Reis et al. [12] found a 5.9 mmHg reduction in PASP in the intervention group compared to a 9.6 mmHg increase in PASP in the placebo group on a 6-month follow-up. The calculated/derived mPAP in their study reduced from 24.27 to 20.33 mmHg (mean reduction of 3.94 mmHg) in the intervention group compared to a 5.86 mmHg increase in the control group (20.13 mmHg at baseline vs. 25.99 mmHg at follow-up). Reddy et al. [13] demonstrated that DAPA had a significant impact on mPAP during exercise with a mean of 5.9 mmHg reduction in mPAP after 24 weeks compared to placebo. Even during rest, mPAP value was 2.8 mmHg lower in the intervention compared to the control (1.8 mmHg reduction in mPAP in the intervention group compared to a 1.0 mmHg increase in mPAP in the control) after 24 weeks follow-up; however, the resting hemodynamics were not statistically significant. Similarly, the PASP at rest was 2.6 mmHg lower in the DAPA group compared to placebo after 24 weeks (p = 0.27). But, the exercise PASP had a statistically insignificant (p = 0.08) reduction, 5.3 mmHg lower in the DAPA group compared to the placebo.
EMPA has shown more variable results. In the study by Nassif et al. [15], EMPA was associated with a 1.9 mmHg reduction in mPAP (intervention vs. control group); however, this finding was not statistically significant. EMPA also reduced PASP compared to placebo, but the reduction was not statistically significant. Omar et al. [14] reported modest reductions in mPAP in the intervention group during exercise, but this was a marginally significant finding. However, the resting hemodynamics in their study showed conflicting findings, with greater reduction of mPAP in the placebo group (−1.38 mmHg) compared to intervention (−1.19 mmHg), but this was not statistically significant. Jariwala and Gururaj [16] found that the PASP remained rather constant while comparing the efficacy of adding EMPA on HF patients under OMT with those on OMT alone. The effect of EMPA, as seen in the studies by Omar et al. [14] and Nassif et al. [15], produced modest effects. This could be because these trials were conducted for a shorter duration (12 weeks) compared to the trials by Reis et al. and Reddy et al. [12, 13], which took around 6 months. In contrast, Jariwala and Gururaj [16] reported no change in PAPs even after 9 months of therapy.
Most trials demonstrate a drop in PAPs when SGLT2 therapies are used compared to controls; however, there are still inconsistencies in their effectiveness, as demonstrated by the variability in responses according to the duration of therapy (Table 6). Nevertheless, the consistent reduction of pulmonary pressures with this group of drugs over most of the trials could not be solely by chance, and further research is required to build upon these findings. However, since the studies varied in terms of baseline characteristics and follow-up duration, the findings should be carefully speculated upon, and further research is warranted before we can formulate a solid conclusion regarding the superiority of a particular SGLT2i group. This variability suggests potential differences in how these drugs affect pulmonary pressures, emphasizing the need for more targeted research.
- C. HFrEF Versus HFpEF:
Because of the scarcity of research studies directly comparing HFrEF and HFpEF patients, we could not extract the comparative efficacy of SGLT2 inhibitors between these subgroups. From limited data derived from two studies, it is seen that DAPA could reduce pulmonary pressure in both HF populations (Table 7). In HFrEF, Reis et al. [12] reported a significant PASP reduction with DAPA (−5.9 mmHg, p < 0.001), whereas the control group showed an increase (+9.6 mmHg). Similarly, in the HFpEF subgroup, Reddy et al. [13] found a significant reduction in mPAP during exercise (−5.9 mmHg, p = 0.02) and a trend toward PASP reduction (−5.3 mmHg, p = 0.08), though resting hemodynamics were not statistically significant. In HFpEF, EMPA showed minimal effects, with Omar et al. reporting nonsignificant PASP reductions at rest (−1.19 mmHg, p = 0.23) and during exercise (−2.37 mmHg, p = 0.056). The control group experienced comparable changes, indicating no substantial benefit. There was no data for the efficacy of EMPA in the HFrEF group. Despite the scarcity of data, it is seen that the pulmonary hemodynamics have a consistent trend toward reduction with SGLT2 inhibitors intervention compared to control.
3.4.2. Secondary Outcome
SGLT2 inhibitor drugs, such as DAPA and EMPA, have shown significant effects on various hemodynamic parameters when compared to placebo in patients with HF (Table 8).
DAPA demonstrated notable improvements in PCWP and NT-proBNP levels. In the study by Reddy et al. [13], DAPA reduced PCWP significantly, with a change of −3.5 mmHg at rest and −6.1 mmHg during exercise, compared to minimal changes in the placebo group. These reductions were statistically significant (p = 0.03 and p = 0.02, respectively). NT-proBNP levels also showed a greater reduction with DAPA, highlighting its beneficial impact on HF biomarkers. Only Reddy et al. [13] demonstrated the impact over PVR. The changes in PVR were not significant, with only minimal variations between the DAPA and placebo groups.
EMPA also demonstrated significant improvements in key outcomes. In the study by Omar et al. [14], EMPA reduced PADP during both rest and exercise. At rest, the change was minimal (from 14 to 13 mmHg), but during exercise, the reduction was more pronounced, dropping from 32 to 29 mmHg. PCWP also showed significant reductions with EMPA, with a decrease of −2.16 mmHg at rest and −4.14 mmHg during exercise, compared to smaller changes in the placebo group. Additionally, NT-proBNP levels were significantly reduced, as seen in Nassif et al. [15], where a greater proportion of patients on EMPA experienced a ≥ 20% reduction in NT-proBNP levels (34% in the EMPA group vs. 7% in the placebo group, p = 0.01).
Overall, both DAPA and EMPA demonstrated improvements in reducing PCWP and NT-proBNP levels, with DAPA showing a tendency toward stronger effects on PCWP during exercise and EMPA showing significant reductions in NT-proBNP levels, indicating their potential benefits in managing pulmonary pressures and HF symptoms. Reis et al. [12] demonstrated that DAPA significantly enhanced RV–PA coupling over 24 weeks, as evidenced by an increase in TAPSE/PASP from 0.52 to 0.66. In contrast, the control group showed deterioration in coupling. Similarly, Jariwala and Gururaj [16] found that EMPA combined with OMT led to a notable increase in TAPSE/PASP (0.252→0.300), with the change largely attributed to improved RV function rather than reduced PASP. Correale et al. [17] corroborated these findings, reporting a striking rise in TAPSE/PASP (0.63→0.88) with SGLT2 inhibitor therapy, driven by both increased TAPSE and decreased PASP. Likewise, in the study by Reddy et al. [13], while no significant benefit in RV–PA coupling was observed at rest, exercise testing revealed a statistically significant improvement in RVs'/PA Ea with DAPA (p = 0.04), suggesting enhanced physiological adaptability under stress.
4. Discussion
Our systematic review has evaluated the efficacy of SGLT2 inhibitors in improving PAPs and pulmonary hemodynamics in the HF population. The data comes from four RCTs and two observational studies comparing SGLT2 inhibitors with the control group. The principal findings of our analysis indicate that SGLT2 inhibitors, when compared to placebo, demonstrate a meaningful impact on reducing PAPs and improving pulmonary hemodynamics in the HF population. It is imperative to conduct more structured research to derive an exact conclusion on the efficacy of DAPA versus EMPA and their impact on rest versus exercise and HFpEF versus HFrEF. This systematic review represents the most comprehensive examination to date, comprising a cohort of 346 participants. It encompasses a comprehensive review of all existing data regarding the change in PAPs and pulmonary hemodynamics in the context of SGLT2 inhibitors therapy.
Numerous studies have consistently highlighted the positive effects of SGLT2 inhibitors on pulmonary pressures, reinforcing the findings from the studies included in our review (Table 9). A statistically significant decrease in key measures like PASP, mPAP, PADP, and NT-proBNP levels was observed across all the observational studies [18–24], often within relatively short follow-up periods. These reductions are comparable to the outcomes seen in controlled trials, which similarly demonstrated improvements in pulmonary hemodynamics. What stands out from these observational studies is the consistency in the direction of the results, despite having some differences in patient populations, follow-up duration, and study designs. Likewise, a randomized controlled trial exploring the efficacy of combining sacubitril/valsartan with DAPA in patients with pulmonary hypertension secondary to left heart disease (PH-LHD) found that the group that received both drugs showed notable improvements in mPAP and PASP in comparison to the control group that took only sacubitril/valsartan [25]. Such consistency in reducing PASP and mPAP, along with improvements in HF biomarkers, as seen in several RCTs and observational studies, suggests that SGLT2 inhibitors offer robust and replicable benefits across diverse real-world settings. This reinforces the evidence supporting the broader use of these agents for improving pulmonary hemodynamics in HF patients.
Pulmonary hemodynamic parameters are crucial for evaluating and treating patients with HF [26–29]. They offer essential information regarding the hemodynamic conditions of the pulmonary circulation, which frequently suffers in HF due to increased left-sided filling pressures, resulting in PH [30]. The pathophysiological distinctions between combined precapillary postcapillary pulmonary hypertension (CpcPH) and isolated postcapillary pulmonary hypertension (IpcPH) are also clarified by such hemodynamic measures. We looked at the significance of a number of pulmonary hemodynamic indicators, including mPAP, PASP, PADP, PCWP, PVR, and NT-proBNP, highlighting their influence on HF patients and their prognostic value. One important indicator of cardiac stress and volume overload is NT-proBNP, whose elevated levels are associated with worse outcomes in HF via raising pulmonary pressures and impairing functional status [31, 32]. mPAP > 20 mmHg defines PH and correlates with poor prognosis due to elevated pulmonary pressures and RV dysfunction [7, 30, 33, 34]. PASP and PADP are also valuable: elevated PASP reflects impaired functional capacity and higher mortality risk, while increased PADP indicates rising left atrial pressure from LV dysfunction [31, 35]. PCWP serves as a surrogate for left atrial pressure; its elevation signals fluid overload, pulmonary congestion, and worse HF outcomes [35, 36]. PVR reflects pulmonary vascular disease, impaired RV function, and is strongly predictive of adverse prognosis. Specifically, PVR levels greater than 3 Wood units are commonly found in patients with significant pulmonary vascular disease [7, 37], affecting treatment decisions and predicted outcomes. Certain hemodynamic measures are closely linked to clinical outcomes, including mortality and major adverse cardiac events (MACE). For example, variations in mPAP are closely tied to negative clinical outcomes in patients with pulmonary arterial hypertension (PAH), showcasing considerable prognostic capability [26]. Likewise, the diastolic pressure gradient (DPG) serves as a significant predictor of mortality for patients with PH stemming from left heart disease [29]. A reduction in PCWP is significant for managing PH and HF. Lower PCWP can improve cardiac filling and reduce pulmonary congestion, potentially enhancing exercise capacity and reducing hospitalization rates [38]. We found that SGLT2i shows a generally favorable trend toward improved RV–PA coupling metrics (Table 8) [12, 13, 16, 17]. Reddy et al. [13], hypothesized that a decrease in exercise PCWP with SGLT2 inhibitors is probably a major mediator of improved pulsatile pulmonary vascular load and RV–PA coupling during exertion. A key limitation in the interpretation of RV–PA coupling is the heterogeneity in how the parameter was assessed. A key limitation is heterogeneity in assessment: only Reddy et al. [13] used RVs'/Ea, a load-independent metric, whereas others [12, 16, 17] relied on TAPSE/PASP, a less reliable surrogate under varying RV geometry or load. Standardized use of RVs'/Ea in future trials may yield clearer insights into the cardiopulmonary benefits of SGLT2 inhibitors.
Implementing invasive hemodynamic evaluations can improve risk prediction models, facilitating customized management approaches for HF patients [29]. PAP-guided HF therapy has demonstrated favorable outcomes in reducing HF-related hospitalization [39]. Notably, two trials, the CHAMPION [40] and GUIDE-HF [41], reported significant reductions in HF-related hospitalization. Another prospective study analyzing PAP-guided therapy in patients with symptomatic HF after implant CardioMEMS showed that HF-related hospitalization decreased by 62% post- versus preimplant [42, 43]. A recent meta-analysis aggregated results from several of these randomized trials and concluded that using PAP monitoring to guide the treatment of HF patients reduces episodes of worsening HF and subsequent hospitalizations [44]. Ongoing monitoring of hemodynamic shifts also helps in treatment modifications, which can enhance patient outcomes [26, 45]. By incorporating these hemodynamic indicators into clinical routines, healthcare professionals can refine treatment strategies, boost survival rates, and elevate the overall quality of patient care.
The impact of SGLT2 inhibitors on Ipc-LHD and CPC-LHD remains an intriguing yet largely unexplored area of research. In IpcPH, the main cause of increased PAPs is the reverse transmission of raised left ventricular filling pressures. By promoting natriuresis and osmotic diuresis without neurohormonal activation, SGLT2 inhibitors reduce LV preload and pulmonary venous congestion [22, 46]. Several trials [13–15] support the unloading effect of SGLT2 inhibitors, with consistent reductions in PCWP and PADP (Table 8) observed within weeks of therapy, both at rest and during exercise. These consistent improvements in postcapillary pressures strongly support the utility of SGLT2 inhibitors in IpcPH. In contrast, CpcPH involves not only elevated left-sided pressures but also increased PVR (PVR ≥ 3 WU) due to vascular remodeling, endothelial dysfunction, and inflammation. The studies included in this review have failed to address the changes in PVR. Besides offering similar hemodynamic relief in CpcPH as in IpcPH, their additional impact on the pulmonary vasculature as shown in preclinical models implies possible advantages of SGLT2 inhibitors for both PH subgroups [47, 48]. Evidence regarding CpcPH is developing, but it is not yet very strong, reflecting the difficulties in reversing preexisting vascular issues. In one study of individuals with exercise-induced PH (a precursor to CpcPH), SGLT2 inhibitors notably reduced the slope of PCWP to cardiac output (PCWP/CO) during physical activity (3.9 ± 1.2 vs. 2.4 ± 1.2 mmHg/L/min) and improved the distance covered in a 6-min walk, indicating improved pulmonary vascular compliance [49]. The possibility of vascular remodeling reversal, suggested by animal models, warrants further investigation in dedicated CpcPH human trials. Because of the lack of adequate data related to CpcPH, the exact effects of these novel drugs on CpcPH could not be estimated, and this limitation would be an interesting target for future studies to bridge the gap of evidence.
SGLT2 inhibitors have shown significant benefits in cardiovascular outcomes, including reductions in HF-related hospitalizations, mortality, and symptom burden, in notable trials. The therapeutic effect of SGLT2 inhibitors in HF was first demonstrated in the empagliflozin cardiovascular outcome event trial in Type 2 diabetes mellitus patients removing excess glucose (EMPA-REG OUTCOME) trial [50] where it was noted that there was a significant reduction in the secondary endpoint of HF hospitalizations when compared with placebo. The canagliflozin and cardiovascular and renal events in Type 2 diabetes (CANVAS) [51], the dapagliflozin and cardiovascular outcomes in Type 2 diabetes (DECLARE TIMI) [52], and a pooled analysis by McGuire et al. [53] trials built upon this finding and came to similar conclusions in their study. These findings piqued the interest regarding the capacity of SGLT2 inhibitor to work beyond diabetes, tempting researchers to conduct trials directed toward HF outcomes. As such, several placebo-controlled clinical trials were then conducted to evaluate the effects of SGLT2 inhibitors in the chronic HF population with and without Type 2 diabetes. DAPA-HF (dapagliflozin and prevention of adverse outcomes in heart failure) [54] and EMPEROR-Reduced (empagliflozin outcome trial in patients with chronic heart failure with reduced ejection fraction) [55] studied patients with chronic HFrEF, and EMPEROR-Preserved (empagliflozin outcome trial in patients with chronic heart failure with preserved ejection fraction) [56] evaluated patients with chronic HFpEF. SGLT2 inhibitors were able to demonstrate a ~25% relative reduction in the composite end point of hospitalization for HF or cardiovascular death when compared with placebo in all these trials. The efficacy of SGLT2 inhibitors in exercise hemodynamics has been studied using cardiopulmonary exercise tests (CPETs), but the results varied across studies, with one study indicating improvements [57], while others showing no effects [58–60]. EMPA was associated with lower rates of hospitalization at 1 year compared with DAPA in a recent cohort study that compared the outcomes in reducing all-cause mortality and hospitalizations in patients with HF [61]. Another retrospective study by Hao et al. [62] also found that EMPA (vs. DAPA) resulted in greater increases in left ventricular EF and NYHA class improvements. But similar improvements in cardiovascular outcomes were observed between EMPA and DAPA compared with placebo in a recent meta-analysis [63]. These variations in findings could be due to a difference in adherence across studies. Thus, future researchers should also consider the adherence in the study population while conducting comparative research of the SGLT2 inhibitor drugs.
SGLT2 inhibitors are believed to reduce pulmonary pressures through several mechanisms. Inflammation is a notable contributor to HF. The anti-inflammatory potential of this novel drug stems from its ability to repress the endothelial expression of adhesion receptors, proinflammatory cytokines, and chemokines [64]. Specifically, DAPA can inhibit hyperglycemia-induced upregulation of intercellular adhesion molecule-1 (ICAM-1), while EMPA inhibits certain chemokines such as monocyte chemoattractant protein-1 (MCP-1). SGLT2 inhibitors have demonstrated a reduction in extracellular matrix production, suppression of collagen synthesis and remodeling, and inhibiting the proliferation and migration of vascular smooth muscle cells, highlighting their potential role in inhibiting pulmonary vascular remodeling [64–66]. SGLT2 inhibitors ensure the bioavailability of nitric oxide, a potent vasodilator, whose critical reduction leads to increased PAP seen in PH [67]. Their diuretic effect likely decreases pulmonary congestion, reducing the load on the right ventricle [20, 23]. The resultant volume contraction and hemoconcentration were attributed as the cause of reduction in cardiovascular mortality in a mediation analysis of the EMPA-REG outcome trial [68]. Besides their effect on the pulmonary circulation, numerous theories have tried to elucidate the cardioprotective mechanisms of SGLT2 inhibitors. These theories have explored the role of SGLT2 inhibitors in blood pressure lowering, cardiac energy metabolism, anti-inflammation, weight loss, diuresis/natriuresis, preventing cardiac remodeling, preventing ischemia/reperfusion injuries, decreasing oxidative stress, and so on. Although further research is necessary to explore the full potential of this novel drug, such multifaceted mechanisms offer a promising outlook for SGLT2 inhibitors in the management of HF and PH.
Multiple animal studies have provided more details on the cardioprotective mechanisms of SGLT2 inhibitors with respect to pulmonary hemodynamics. Both a general SGLT inhibitor and a specific SGLT2 inhibitor, canagliflozin, demonstrated targeted dilatation of pulmonary arteries in an in vitro analysis conducted on pulmonary and coronary arteries of diabetic mice [69]. Chowdhury et al. [70] showed that EMPA significantly reduced mPAP and RVSP in their studies on monocrotaline-induced PAH rat models [70]. In addition, Chowdhury et al. showed that EMPA decreased arterial wall thickening and pulmonary arteriolar muscularization in these rats, suggesting that SGLT2 inhibitors might prevent certain injurious structural pulmonary vascular changes. However, a similar study utilizing DAPA failed to demonstrate significant improvements in survival or vascular remodeling in monocrotaline-induced PAH rat models [71]. Yusuke et al. found pulmonary vascular remodeling in PH-LHD models was improved with tofogliflozin, suggesting SGLT2 inhibitors might be effective in treating PH-LHD [47]. While these studies provide diverse views on the efficacy of SGLT2 inhibitors in the pulmonary hemodynamics of HF patients, it must be noted that cross-pollination of research findings from animal studies to clinical practice in humans might not be an evidence-based approach in forming scientifically sound conclusions.
4.1. Strengths and Limitations
The results from this structured systematic review should be interpreted in the context of several potential limitations. One of the major limitations of this study is the small sample size and short follow-up duration, which restricts the generalizability of the findings. The study includes only a small number of heterogeneous studies, involving only 346 patients in total, and might not be large enough to draw strong, generalizable conclusions. This limits the comprehensiveness of findings and may not provide sufficient power for robust conclusions. In addition, the heterogeneity in study designs and measurement techniques considerably undermines the comparability and reliability of the findings. Specifically, pulmonary pressures were assessed using different methodologies: one study utilized continuous monitoring via a CardioMEMS device, two employed RHC, and three relied on echocardiography. While CardioMEMS and RHC are regarded as more accurate and reliable, echocardiography is inherently operator-dependent and may be subject to variability in measurement accuracy. Furthermore, several studies derived mPAP using estimation equations rather than direct measurement, thereby introducing additional uncertainty into the results. This variability in both measurement techniques and study designs—including differences in follow-up duration, patient selection criteria (e.g., HFpEF vs. HFrEF), and endpoints (rest vs. exercise hemodynamics)—complicates direct comparisons across studies and limits the generalizability of our conclusions. These limitations affect the strength of the conclusions and suggest the need for more uniform methodologies and larger trials to further clarify the effects of SGLT2 inhibitors on PAPs.
Despite these limitations, the study also has several strengths. The use of a comprehensive and systematic review process, following PRISMA guidelines, ensured a rigorous and transparent selection of relevant studies. Additionally, the inclusion of studies with multiple measurement techniques provides a broad perspective on the impact of SGLT2 inhibitors across different settings and patient populations. Furthermore, the study's focus on exploring the effects of SGLT2 inhibitors on pulmonary hemodynamics in HF, an area with limited prior research, addresses an important clinical gap and offers valuable insights for future studies.
To enhance the robustness and clinical applicability of future research, it is imperative to adopt standardized methodologies. We recommend that future studies employ direct measurement methods such as RHC or validated implantable devices like CardioMEMS rather than relying solely on echocardiographic estimations or derived calculations. Larger, multicenter trials are encouraged as these will improve statistical power and provide more definitive insights into the impact of SGLT2 inhibitors on pulmonary hemodynamics. Consistent recording and calculation of key parameters, such as mPAP, PVR, and PCWP, are essential to enhance the depth and comparability of results. Longer follow-up periods are necessary to evaluate the sustained impact of SGLT2 inhibitors on pulmonary pressures and related outcomes. By addressing these methodological concerns, future research can yield more reliable and generalizable findings, ultimately advancing our understanding and management of PH in HF patients.
5. Conclusion
In conclusion, this systematic review highlights the potential benefits of SGLT2 inhibitors, particularly DAPA and EMPA, in improving pulmonary hemodynamics and reducing PAPs in HF patients. The review demonstrated that these drugs show promising results in reducing mPAP and PASP. This effect highlights their potential to improve outcomes for patients with HF, particularly those with elevated pulmonary pressures.
Additionally, reductions in key markers such as PCWP and NT-proBNP further suggest that SGLT2 inhibitors can play a significant role in managing PH and HF. However, the difference in the outcome for trials using DAPA and those with EMPA, as well as between rest and exercise conditions, suggests these drugs may have distinct effects on pulmonary hemodynamics, and these effects may vary based on the physiological setting warranting further research. While both drugs show promise, the current evidence base comprising a handful of studies for each drug may not be sufficient to draw definitive conclusions. It is important to acknowledge that not all research has employed the gold standard methods for measuring pulmonary pressures. More comparative research between DAPA and EMPA, especially in diverse clinical settings, is needed to fully understand their differential effects on rest versus exercise hemodynamics. Overall, this review reinforces the growing evidence supporting the use of SGLT2 inhibitors in managing pulmonary pressures and improving cardiovascular outcomes in HF patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bozkurt B. Ahmad T. Alexander K. HF STATS 2024: Heart Failure Epidemiology and Outcomes Statistics An Updated 2024 Report From the Heart Failure Society of America Journal of Cardiac Failure 20253116611610.1016/j.cardfail.2024.07.00139322534 · doi ↗ · pubmed ↗
- 2Lam C. S. P. Chandramouli C. Ahooja V. Verma S. SGLT-2 Inhibitors in Heart Failure: Current Management, Unmet Needs, and Therapeutic Prospects Journal of the American Heart Association 2019820 e 01338910.1161/JAHA.119.0133892-s 2.0-8507316632531607208 PMC 6818035 · doi ↗ · pubmed ↗
- 3Ponikowski P. Voors A. A. Anker S. D. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) Developed With the Special Contribution of the Heart Failure Association (HFA) of the ESC European Heart Journal 201637272129220010.1093/eurheartj/ehw 1282-s 2.0-8498039610827206819 · doi ↗ · pubmed ↗
- 4Kalogeropoulos A. P. Siwamogsatham S. Hayek S. Echocardiographic Assessment of Pulmonary Artery Systolic Pressure and Outcomes in Ambulatory Heart Failure Patients Journal of the American Heart Association 201431 e 00036310.1161/JAHA.113.0003632-s 2.0-8489860483524492947 PMC 3959670 · doi ↗ · pubmed ↗
- 5Gerges C. Gerges M. Lang M. B. Diastolic Pulmonary Vascular Pressure Gradient Chest 2013143375876610.1378/chest.12-16532-s 2.0-8487497000723580984 · doi ↗ · pubmed ↗
- 6Guazzi M. Pulmonary Hypertension in Heart Failure Preserved Ejection Fraction: Prevalence, Pathophysiology, and Clinical Perspectives Circulation: Heart Failure 20147236737710.1161/CIRCHEARTFAILURE.113.0008232-s 2.0-8490000664524643889 · doi ↗ · pubmed ↗
- 7Maron B. A. Kovacs G. Vaidya A. Cardiopulmonary Hemodynamics in Pulmonary Hypertension and Heart Failure: JACC Review Topic of the Week Journal of the American College of Cardiology 202076222671268110.1016/j.jacc.2020.10.00733243385 PMC 7703679 · doi ↗ · pubmed ↗
- 8Vanderpool R. R. Saul M. Nouraie M. Gladwin M. T. Simon M. A. Association Between Hemodynamic Markers of Pulmonary Hypertension and Outcomes in Heart Failure With Preserved Ejection Fraction JAMA Cardiology 20183429830610.1001/jamacardio.2018.01282-s 2.0-8504600734729541759 PMC 5875307 · doi ↗ · pubmed ↗