The Risk Factor Analysis of Gallbladder Gangrene in Acute Acalculous Cholecystitis: A Single-Center Retrospective Study
Jiu-ling Zheng, Shuang-quan Liu, Yan-han Liu, Guo-hua Dai, Hua-guo Feng, Hao-yang Tan

TL;DR
This study identifies risk factors and a new predictive marker for gallbladder gangrene in a specific type of gallbladder inflammation.
Contribution
The systemic immune-inflammation index (SII) is shown to be a novel and effective predictor of gallbladder gangrene.
Findings
Gallbladder gangrene occurred in 45.1% of acute acalculous cholecystitis patients.
SII outperformed other inflammatory markers in predicting gangrenous cholecystitis.
Platelet, PCT, SII, D-dimer, CA19-9, gallbladder enlargement, and effusion are independent risk factors.
Abstract
This research was performed to determine the risk factors for gallbladder gangrene in acute acalculous cholecystitis patients and to assess the predictive ability of inflammatory markers. The study included 226 acute acalculous cholecystitis patients who underwent laparoscopic cholecystectomy within 72 h of onset. The receiver operating characteristic curves were employed to determine the optimal cut-off, specificity, and sensitivity of inflammatory markers in predicting gangrenous cholecystitis. Logistic regression analysis was conducted to ascertain the independent risk factors associated with gallbladder gangrene. The incidence rate of gallbladder gangrene in acute acalculous cholecystitis was 45.1% (102/226). Compared with other inflammatory markers, the systemic immune-inflammation index (SII) demonstrated superior predictive validity (vs. CRP, p = 0.021; vs. WBC, p < 0.001; vs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1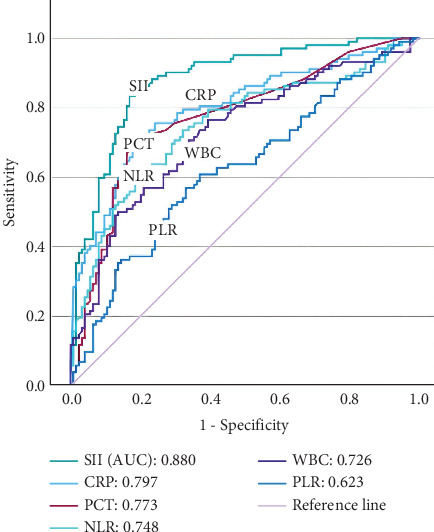 Figure 2
Figure 2- —Chongqing University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatitis Pathology and Treatment · Cholangiocarcinoma and Gallbladder Cancer Studies
1. Introduction
Acute cholecystitis is a common biliary system disease. Gangrenous cholecystitis is a severe type of acute cholecystitis, which is characterized by obvious infection and necrosis of the gallbladder wall [1]. If gangrenous cholecystitis is not treated in time, it may cause a series of serious complications, such as gallbladder perforation, biliary peritonitis, and abscess around the gallbladder [2]. These complications not only increase the difficulty of treatment but also may threaten the lives of patients [3]. However, the timing of surgery for acute acalculous cholecystitis is controversial. If there is a high risk for developing gangrene, emergency surgery may be the best treatment option. Therefore, early identification and accurate evaluation of gangrenous cholecystitis have important clinical significance for optimizing the treatment plan and improving the prognosis in acute acalculous cholecystitis.
Based on the recommendation outlined in the Tokyo Guidelines 2018 [4], the white blood cell (WBC) count can serve as an indicative marker for assessing the severity of acute cholecystitis. Some research showed that the WBC count of patients with gangrenous cholecystitis is higher than that of patients with acute cholecystitis, and 95% of gangrenous cholecystitis' WBC count > 10∗10^9^/L [5, 6]. However, due to the lack of a unified diagnostic standard for WBC count, it is difficult to promote its application in clinical practice. C-reactive protein (CRP), platelet-to-lymphocyte ratio (PLR), and neutrophil-to-lymphocyte ratio (NLR) are additionally recognized as common inflammatory markers in clinical practice. A retrospective study showed that the increase in CRP suggested that the histological state of the gallbladder was poor, which was helpful in identifying gangrenous cholecystitis [7]. When CRP rose to 200 mg/L, the positive predictive value for predicting gangrenous cholecystitis was 50%, and the sensitivity and negative predictive value were 100%. CRP rise was also an effective inflammatory marker for emergency surgery and laparoscopic cholecystectomy converted to open surgery [8]. Recent research showed that NLR in patients with gangrenous cholecystitis will also be significantly increased. CRP and NLR are independent related factors of the severity of acute cholecystitis, which can help the diagnosis and prognosis evaluation of gangrenous cholecystitis [9]. Some studies found a correlation between the inflammatory indices, such as PLR, and the severity of inflammation and postoperative hospital stay in acute calculous cholecystitis [10, 11]. However, the relationship between these inflammatory indices and predicting gangrenous cholecystitis in acute acalculous cholecystitis lacks relevant research.
More and more researchers believe that the hypercoagulable state of elevated platelets can also reflect the severity of the systemic inflammatory response. In recent years, some scholars have proposed a new parameter, which is named “systemic immune-inflammation index (SII)” [12]. SII is a new indicator for integrating neutrophils, lymphocytes, and platelet cell counts, which can better assess the severity of inflammation and blood hypercoagulability. Recent studies have shown that SII can help to distinguish the risk of acute cholecystitis and chronic cholecystitis and can predict the severity of acute cholecystitis [13]. The relationship between SII and acute acalculous gangrenous cholecystitis deserves further investigation.
Therefore, the aim of this study was to determine the risk factors for gallbladder gangrene in acute acalculous cholecystitis patients and to assess the predictive ability of inflammatory markers.
2. Materials and Methods
2.1. Patients
This retrospective study included acute acalculous cholecystitis patients who underwent laparoscopic cholecystectomy at the hepatobiliary surgery department from January 2021 to August 2024. The inclusion criteria were as follows: (1) age exceeding 18 years old; (2) the diagnostic criteria of acute acalculous cholecystitis were according to the Tokyo Guidelines 2018; (3) patients underwent laparoscopic cholecystectomy within 72 h of onset and had a detailed gallbladder pathology report after surgery; (4) patients signed informed consent before receiving treatment; and (5) clinical data were comprehensively recorded. The exclusion criteria were as follows: (1) patients with gallstones, choledocholithiasis, or pancreatitis; (2) patients with malignant tumors such as liver cancer or gallbladder cancer; and (3) patients with serious underlying diseases such as organ failure. Eligible patients were divided into the gangrene group and the non-gangrene group based on gallbladder pathological results.
2.2. Data Collection
From electronic medical record systems, we have compiled the following clinical data: age, gender, vital signs, underlying disease, blood routine tests, coagulation function data, liver and kidney function data, inflammatory cytokine data, imaging examination, and treatment process. Abdominal ultrasound and/or abdominal CT, judged by two senior ultrasound physicians or radiologists, were used to document the thickness of the gallbladder walls, enlarged gallbladder, and pericholecystic fluid collection. The most severe values of laboratory and imaging examination data recorded within 24 h before surgery were selected.
Inflammatory biomarkers were computed utilizing the blood routine test results measured from the same sample (such as neutrophil count, lymphocyte count, and platelets). PLR was derived using the following formula: PLR = platelets/lymphocyte count. Similarly, NLR was computed with the following formula: NLR = neutrophil count/lymphocyte count. SII was calculated employing the following formula: SII = platelets∗neutrophil count/lymphocyte count.
The sample size of this study was calculated by the calculation method of Li and Fine [14].
2.3. Statistical Analysis
The SPSS Statistics software (Version 23, New York, United States) was used for statistical analysis in this retrospective study. Continuous data were presented as medians accompanied by interquartile ranges (25th–75th percentile) or as means ± standard deviations. These data were subsequently subjected to comparative analysis utilizing either the Mann–Whitney U test or the Student's t-test according to whether they conform to a normal distribution. Dichotomous data were presented as frequencies (percentages) and compared by the chi-square or Fisher's exact test as appropriate. The receiver operating characteristic (ROC) curves were employed to determine the optimal cut-off, specificity, and sensitivity of inflammatory biomarkers in predicting gangrenous cholecystitis. The area under the curve (AUC) was used to verify predictive performance and was categorized according to the widely accepted classification scale described by Micić et al. [15]. The differences between inflammatory indicators' AUC were analyzed by the calculation method of DeLong et al. [16]. Univariate analysis for each factor was performed by logistic regression analysis. The continuous variable was dichotomized based on optimal cut-off values by ROC curve. Variables with p values less than 0.1 in univariate analysis were included in the multivariate regression model using the “forward LR” method to determine independent risk factors. The two-tailed p value < 0.05 was considered a statistically significant difference.
3. Results
3.1. Baseline Characteristics
There were 226 patients with acute acalculous cholecystitis who underwent laparoscopic cholecystectomy within 72 h of onset included in this study. According to postoperative pathological reports, these patients were categorized into two groups: the gangrene group (n = 102) and the non-gangrene group (n = 124), as shown in Figure 1.
The incidence rate of gangrenous cholecystitis in acute acalculous cholecystitis was 45.1% (102/226). Compared with non-gangrene group patients, the gangrene group patients' median age was older (61.0 vs. 55.5, p = 0.001). The inflammatory markers (CRP, WBC, PCT, NLR, PLR, and SII) of the gangrene group were higher than those of the non-gangrene group. The levels of D-dimer and carbohydrate antigen 19-9 (CA19-9) between the two groups were statistically different. There were also statistical differences in gallbladder ultrasound between the two groups. The median gallbladder wall of gangrene group patients was thicker than that of non-gangrene group patients (0.5 vs. 0.3 cm, p < 0.001). The incidence rates of gallbladder enlargement and effusion in the gangrene group were higher than those in the non-gangrene group (63.7% vs. 18.5%, p < 0.001; 31.4% vs. 1.6%, p < 0.001).
There were also notable statistical differences observed in the perioperative conditions between the two groups. The median operative time and postoperative hospitalization time of gangrene group patients were longer than those of non-gangrene group patients (71.5 vs. 50.5 min, p < 0.001; 3 vs. 2 days, p < 0.001). The median intraoperative bleeding of gangrene group patients was more than that of non-gangrene group patients (30.0 vs. 10.0 mL, p < 0.001). The conversion rate of gangrene group patients was higher than that of non-gangrene group patients (5.9% vs. 0.0%, p = 0.020).
The baseline characteristics of the two groups of patients are outlined in Table 1.
3.2. Prediction Value of Inflammatory Markers
Furthermore, the predictive values of the inflammatory markers (CRP, WBC, PCT, NLR, PLR, and SII) for gallbladder gangrene in acute acalculous cholecystitis patients were comprehensively analyzed utilizing the ROC curves (Figure 2). The AUC for SII was determined to be 0.880 (p < 0.001), and the cut-off threshold was established at 1659.0∗10^9^/L. The AUC for CRP was determined to be 0.797 (p < 0.001), and the cut-off threshold was established at 19.02 mg/L. The AUC for WBC was determined to be 0.726 (p < 0.001), and the cut-off threshold was established at 7.72∗10^9^/L. The AUC for PCT was determined to be 0.773 (p < 0.001), and the cut-off threshold was established at 0.12 ng/mL. The AUC for NLR was determined to be 0.748 (p < 0.001), and the cut-off threshold was established at 7.28. The AUC for PLR was determined to be 0.623 (p = 0.001), and the cut-off threshold was established at 199.11. Compared with other inflammatory markers, SII had a larger AUC that demonstrated superior predictive validity (vs. CRP, p = 0.021; vs. WBC, p < 0.001; vs. PCT, p = 0.004; vs. NLR, p < 0.001; vs. PLR, p < 0.001; Table 2).
Based on the sensitivity and specificity of SII (α = 0.05, allowance error was less than 0.05), the sample size of this study was calculated as 170 patients.
3.3. Risk Factor Analysis
The results of the univariate and multivariate logistic regression analysis revealed that platelet, PCT, SII, D-dimer, CA19-9, gallbladder enlargement, and gallbladder effusion were independent risk factors of gallbladder gangrene in acute acalculous cholecystitis patients. The comprehensive findings are presented in Table 3.
4. Discussion
Gangrenous cholecystitis is a common severe acute cholecystitis in clinical practice. Its condition progresses rapidly and has a high mortality rate. Once diagnosed as missed, it may cause serious consequences. Our study found that the operative time, intraoperative blood loss, conversion to open surgery rate, and postoperative hospitalization time of gangrenous cholecystitis patients were higher than those of non-gangrene cholecystitis patients. It is particularly important to early identify acute acalculous cholecystitis patients at high risk of gallbladder gangrene and take timely treatment. Recently, some studies have found the factors for predicting gallbladder gangrene, such as age, gender, inflammatory markers, and gallbladder ultrasound [17–19]. CA19-9, as a gastrointestinal cancer-related antigen, is not only highly expressed in pancreatic cancer and biliary tract cancer but also occasionally detected in benign biliary diseases, such as cholelithiasis, cholecystitis, and cholangitis [20, 21]. Our study revealed that the levels of CA19-9 in gangrene cholecystitis patients were higher than those in non-gangrene cholecystitis patients. The multivariate analysis result also confirmed that the high level of CA19-9 was an independent risk factor for gallbladder gangrene in acute acalculous cholecystitis.
The gallbladder imaging examination also plays an important role in the diagnosis of gangrenous cholecystitis. A recent study reported that gallbladder wall edema, gallbladder dilation, and fluid accumulation around the gallbladder should be used as predictive indicators for gangrenous cholecystitis [22]. Our study found that compared with non-gangrenous cholecystitis patients, gangrenous cholecystitis patients had thicker gallbladder walls. Gallbladder enlargement and gallbladder effusion were independent risk factors for gallbladder gangrene. Local special changes in the gallbladder often indicate the presence of gallbladder gangrene. Some studies showed that contrast-enhanced ultrasound, computerized tomography scan, and magnetic resonance imaging can also be used as supplementary inspection methods for gangrenous cholecystitis [8, 19, 23, 24].
This retrospective study indicated that the inflammatory markers were important factors in predicting gallbladder gangrene in acute acalculous cholecystitis patients. Compared with non-gangrenous cholecystitis patients, the inflammatory markers of gangrenous cholecystitis patients were significantly increased. These inflammatory markers had demonstrated good predictive ability for gallbladder gangrene. Compared with other inflammatory markers, SII had a higher predictive ability. The SII performed best for predicting gallbladder gangrene in acute acalculous cholecystitis patients. The multivariate analysis results showed that PCT and SII were the independent risk factors of gallbladder gangrene. Other inflammatory indicators were not independent risk factors of gallbladder gangrene, though the inflammatory indicators were increased in gangrenous cholecystitis. Compared to other inflammatory markers, SII comprehensively reflects the inflammatory state and blood hypercoagulability. Our study revealed that high levels of platelet and D-dimer were the independent risk factors of gallbladder gangrene. It seems to suggest that local blood circulation disorder and microthrombus formation may be the important factors leading to gallbladder gangrene in acute acalculous cholecystitis. For acute acalculous cholecystitis patients, we should pay more attention to changes in local circulatory function rather than inflammatory response. We speculate that early anticoagulant therapy and improving microcirculation (within 72 h of onset) may reduce the risk of developing gallbladder gangrene. It requires further research to confirm this hypothesis and explore potential mechanisms.
Some limitations need to be pointed out in the current research. First, the retrospective and single-center nature of our study limits causal inference and generalizability. Selection bias is inherent as we only included patients who underwent surgery within a specific timeframe, excluding those managed conservatively or with drainage, potentially underestimating the true incidence and spectrum of gallbladder gangrene. Second, the diagnosis of gangrene relied solely on postoperative pathology, leaving the status of nonsurgical patients unknown and introducing diagnostic verification bias. Third, due to retrospective data constraints, we were unable to include important inflammatory cytokines such as IL-6 and TNF-α, which might offer additional predictive value. Fourth, although we performed a sample size calculation, our cohort remains relatively modest, potentially limiting the power to detect smaller effect sizes or less common risk factors. The dichotomization of continuous variables, while practical for clinical application, may oversimplify complex biological relationships. Fifth, despite multivariate adjustment, residual confounding from unmeasured factors such as detailed sepsis criteria, prior treatments (antibiotics, anticoagulants), and granular comorbidity severity could influence our results. Finally, our study focused on short-term perioperative outcomes; long-term follow-up data regarding recurrence, survival, or quality of life are lacking. Future prospective, multicenter studies incorporating a broader range of biomarkers, including cytokines, and including both surgical and nonsurgical patients with long-term follow-up are warranted to validate and extend our findings.
5. Conclusion
This study found that platelet, PCT, SII, D-dimer, CA19-9, gallbladder enlargement, and gallbladder effusion were independent risk factors for gallbladder gangrene in acute acalculous cholecystitis. Compared with other inflammatory markers, SII demonstrated a superior predictive efficacy. SII could serve as a novel, straightforward, and potent predictive indicator for gallbladder gangrene in acute acalculous cholecystitis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maddu K. Phadke S. Hoff C. Complications of Cholecystitis: A Comprehensive Contemporary Imaging Review Emergency Radiology 20212851011102710.1007/s 10140-021-01944-z 34110530 · doi ↗ · pubmed ↗
- 2Taveras L. R. Scrushy M. G. Cripps M. W. From Mild to Gangrenous Cholecystitis, Laparoscopic Cholecystectomy is Safe 24 Hours a Day American Journal of Surgery 20232261838610.1016/j.amjsurg.2023.01.02936746709 · doi ↗ · pubmed ↗
- 3Orlandini B. Daams F. Fockens P. Voermans R. P. van Wanrooij R. L. Endoscopic Drainage and Necrosectomy for Inoperable Gangrenous Cholecystitis Endoscopy 202355329529610.1055/a-2006-436936854297 PMC 9974331 · doi ↗ · pubmed ↗
- 4Yokoe M. Hata J. Takada T. Tokyo Guidelines 2018: Diagnostic Criteria and Severity Grading of Acute Cholecystitis (With Videos) Journal of Hepato-Biliary-Pancreatic Sciences 2018251415410.1002/jhbp.5152-s 2.0-8503715725129032636 · doi ↗ · pubmed ↗
- 5Gomes C. A. Soares C. Di Saverio S. Gangrenous Cholecystitis in Male Patients: A Study of Prevalence and Predictive Risk Factors Annals of Hepato-Biliary-Pancreatic Surgery 2019231344010.14701/ahbps.2019.23.1.3430863805 PMC 6405364 · doi ↗ · pubmed ↗
- 6Chang W. C. Sun Y. Wu E. H. CT Findings for Detecting the Presence of Gangrenous Ischemia in Cholecystitis AJR American Journal of Roentgenology 2016207230230910.2214/ajr.15.156582-s 2.0-8497953673127249326 · doi ↗ · pubmed ↗
- 7Mahmood F. Akingboye A. Malam Y. Thakkar M. Jambulingam P. Complicated Acute Cholecystitis: The Role of C-Reactive Protein and Neutrophil-Lymphocyte Ratio as Predictive Markers of Severity Cureus 2021132 e 1359210.7759/cureus.1359233796428 PMC 8006862 · doi ↗ · pubmed ↗
- 8Menéndez-Sánchez P. León-Salinas C. Amo-Salas M. Méndez-Cea B. García-Carranza A. Association of Laboratory and Radiologic Parameters in the Diagnosis of Acute Cholecystitis Revista de gastroenterologia de Mexico (English) 201984444945410.1016/j.rgmx.2018.09.0012-s 2.0-8506008191030665720 · doi ↗ · pubmed ↗