Magnesium Depletion Score as an Indicator of Health Risk and Nutritional Status—A Scoping Review
Rebecca B. Costello, Zhongqi Fan, Taylor C. Wallace

TL;DR
This review explores the magnesium depletion score (MDS) as a potential tool to identify people at risk of magnesium deficiency and related health issues.
Contribution
The study evaluates the MDS's clinical applicability and validity across populations through a scoping review.
Findings
48 studies showed adverse health associations with a high MDS.
MDS was inversely correlated with dietary magnesium intake.
MDS shows promise when used alongside traditional dietary assessments.
Abstract
Background/Objectives: Magnesium is an essential nutrient involved in more than 600 enzymatic reactions, and nutritional status is estimated to be critical for many metabolic and biochemical processes in humans. Although magnesium deficiency and inadequacy impacts multiple chronic disease states, signs and symptoms are often nonspecific and nutritional status is difficult to measure. The recently developed magnesium depletion score (MDS) is a promising tool for identifying individuals at risk of magnesium deficiency or inadequacy and associated comorbidities, but its clinical applicability and validity across broad populations remains unclear. Methods: Using the Joanna Briggs Institute (JBI) and JBI Collaborating Center guidelines for conducting scoping reviews, four electronic databases (MEDLINE/ PubMed, Embase, and Scopus) were systematically searched from inception to 20 May 2025 for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
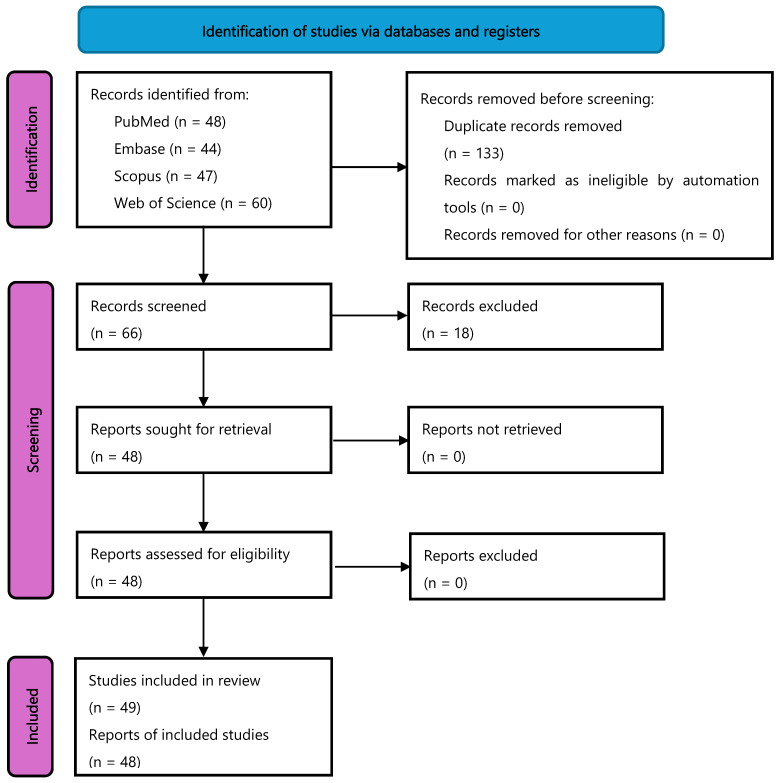 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMagnesium in Health and Disease · Therapeutic Uses of Natural Elements · Plant Micronutrient Interactions and Effects
1. Introduction
Magnesium is an essential nutrient that is involved in numerous metabolic and biochemical process within the cell; the mineral is thought to serve as an activator and cofactor for >200 and >600 enzymes in the human body, respectively [1,2,3]. A large portion of the population fails to consume current recommended intakes of magnesium from food alone (e.g., green vegetables, nuts, seeds, beans, and whole grains) and subsequently are at risk for suboptimal magnesium status; >50% of Americans today do not consume the estimated average requirement (EAR) for magnesium according to recent analysis of the U.S. National Health and Nutrition Examination Survey [4].
Strong evidence suggests that magnesium deficiency contributes to cardiovascular disease [5,6], the metabolic syndrome and type 2 diabetes [7,8], and osteoporosis [9]. Magnesium insufficiency may likely be a contributor to these long-term health ailments, as it has been consistently linked to increases in subclinical low-grade chronic inflammation. Along these lines, evidence from epidemiological analyses and/or clinical trials suggest regular nut and/or legume consumption (two sources high in magnesium) to have beneficial impacts on multiple chronic disease states, as well as in reducing oxidative stress, inflammation, visceral adiposity, hyperglycemia, insulin resistance, and endothelial dysfunction [10].
The signs and symptoms of magnesium deficiency and insufficiency are numerous, nonspecific, and widespread [11]. However, magnesium status is difficult to measure and may be best defined by dietary intake coupled with serum magnesium concentrations and urinary magnesium excretion [12].
The magnesium depletion score (MDS) is an aggregate of several risk factors affecting the absorption and excretion of magnesium. The MDS has been used to identify individuals with abnormal magnesium absorption and/or excretion that may result in a deficient magnesium status. The score was originally derived from the assessment of nutritional status using the magnesium load retention study [13]. This test determines the percent of a magnesium load that is retained by the body by measuring the percent of the load that is excreted in the urine within 24–48 h of administration. It is currently the only tool to assess adequacy of body magnesium stores. Following development of the MDS, the same author group then validated it against a cohort of participants enrolled in the U.S. National Health and Nutrition Examination Survey (NHANES) for greater applicability [13]. The MDS is noninvasive and is calculated as a composite of the following factors:
- Current use of diuretics counted as 1 point.
- Current use of proton pump inhibitor (PPI) counted as 1 point.
- Heavy drinker (defined as >1 drink/d for women and >2 drinks/d for men) counted as 1 point.
- Mildly decreased kidney function, defined as estimated glomerular filtration rate ≥ (eGFR) 60 mL/(min × 1.73 m^2^) < eGFR 90 mL/min × 1.73 m^2^, counted as 1 point.
- Chronic kidney disease defined as eGFR < 60 mL/min × 1.73 m^2^ counted as 2 points.
An MDS >2 has been used to indicate magnesium deficiency associated with increased risk for systemic inflammation and cardiovascular mortality in adults [13]. A score of >3 combined with a dietary magnesium intake below the US recommended dietary allowance (RDA) has been used to indicate magnesium deficiency associated with osteoporosis [9]. These data suggest that sample size and/or disease entity may influence the cut-point indicative of magnesium deficiency. This new suggested method of magnesium status assessment, especially for individuals with diseases and/or ailments associated with magnesium deficiency, needs further evaluation and validation before being accepted for general use.
This scoping review sought to answer the following question: What is the extent of available evidence investigating the application of the magnesium depletion score as an indicator of health risk and nutritional status?
2. Materials and Methods
We utilized the Joanna Briggs Institute (JBI) and JBI Collaborating Center guidelines for conducting scoping reviews [14,15] and report results per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) checklist [16]. We also followed the suggested framework by Arksey and O’Malley [17], which consists of the following components: defining the review question, identifying relevant articles, charting the data, and summarizing the findings. The Population–Concept–Outcome (P-C-O) approach was used to assist in the structure of our search strategy and eligibility criteria. The protocol was preregistered on Open Science Framework (https://osf.io/vka6h) prior to data extraction.
2.1. Data Sources and Search Strategy
A trained librarian within the George Washington University Himmelfarb Health Sciences Library assisted a study investigator (T.C.W.) in developing and implementing a comprehensive web-based search of the MEDLINE/PubMed (National Library of Medicine, Bethesda, MD, USA), Embase (Wiley, West Sussex, UK), Web of Science (Clarivate, Philadelphia, PA, USA), and Scopus (Elsevier, Mérignac, France), databases from inception to 20 May 2025. The complete search strategy is provided in Table S1.
2.2. Study Selection and Data Extraction
Search results for each database were downloaded and imported into Rayyan AI software (Rayyan Systems Inc.; Cambridge, MA, USA, https://www.rayyan.ai), where duplicates were detected primarily through article DOIs and removed prior to screening. Articles were screened to prespecified eligibility criteria presented in Table S2. This scoping review included peer-reviewed and English-language clinical trials and observational studies that assessed potential relationships between the newly proposed MDS on human health outcomes. We did not restrict eligibility based on study duration, participant age, participant health status, health outcomes, or date of publication. Independent dual title and abstract screening was conducted (Z.F. and T.C.W.), with conflicts being resolved through consensus. Remaining articles underwent similar independent dual full-text screening (Z.F. and T.C.W.) utilizing the same inclusion and exclusion criteria. The investigators met to discuss and reconcile any discrepancies through consensus. Reference lists of all included articles were hand-searched prior to data extraction to ensure retainment of all relevant articles. Standardized data-extraction forms were created in Microsoft Excel (version 16.93.1; Microsoft, Redmond, WA, USA) to extract information on study design, population, sample size, intervention/exposure, estimated magnesium intake (in mg/d), duration or follow-up, main outcomes, and overall findings related to MDS. One investigator (Z.F.) extracted data from all included articles, after which a second investigator (T.C.W.) quality checked all extracted data to ensure their accuracy. Discrepancies were resolved through consensus between the two investigators. Descriptive statistics were calculated using Microsoft Excel software. Number (n) and percent frequency (%) are used to describe categorical variables.
3. Results
3.1. Characteristics of Included Articles
Our literature search strategy identified 66 articles for title and abstract screening, after the removal of duplicates. Of these articles, 48 met our eligibility criteria and moved forward to full-text screening. All 48 articles screened in full text met our eligibility criteria and were included in the scoping review. These articles contained 39 cross-sectional and 15 prospective cohort investigations, as well as a single secondary analysis of a randomized controlled trial (Table 1 and Table 2). Data cycles from NHANES represented within all 48 articles with results of the secondary analysis of a clinical trial also being co-published alongside the Fan et al., 2021 [13] NHANES analysis. Figure 1 provides the PRISMA flow diagram of studies.
The NHANES data cycles examined varied, with the widest spread being 1988–2018 for a prospective study by Xing et al. [59]. One cross-sectional study covered only one NHANES data cycle for years 2013–2014 in adults aged >60 years [31], and four articles included both cross-sectional and prospective data reported from 10 cycles (1999–2018) [26,47,48,53]. The largest sample size included 44,588 adults (aged ≥18 years) [48] over 10 NHANES cycles. The age ranges varied as well but only included adults aged ≥18 years, and several articles enrolled participants at age ≥40 years. One prospective analysis by Jiang et al. [26] enrolled older adults (aged >60 years) with frailty. The duration of prospective cohort analyses ranged from 12 weeks to a median of 31 years. The largest prospective analysis enrolled 16,394 adults from 1999 to 2018 NHANES data cycles [54].
3.2. MDS Scoring Parameters
The MDS scoring parameters (0–5) also varied across included articles. Twenty-seven articles reported individual MDSs of 0 to ≥3. Two articles reported individual MDSs of 0 to ≥4, and 10 articles reported individual MDSs of 0 to 5. Four articles used a broad scoring category of <2 or >2. As the individual MDSs increased from 0 to 5, the percentage of participants in each category decreased.
Because the GFR is a key component of the MDS, the majority of articles utilized the Chronic Kidney Disease Epidemiology Collaboration (CKDEPI) equation by Levy et al. [62] updated in 2021, as included in the NHANES. For scoring alcoholic beverage consumption, the majority of articles utilized the NHANES questionnaire derived from the 2015–2020 Dietary Guidelines for Americans Food Patterns Equivalent database [63]. The quantity of alcohol intake was defined as 1–2, 3–4, and ≥5 drinks/drinking day for men and 1, 2–3, and ≥4 drinks/drinking day for women. According to NHANES analytic guidelines, reports of <1 drink/drinking day were rounded up and coded as 1 drink/drinking day.
3.3. Health Outcomes
Health outcomes across observational analyses were multifaceted, ranging from mortality, disease, and disease event risk to self-reported sleep quality and biomarker measures (e.g., high-sensitivity C-reactive protein). The most studied health outcomes were all-cause and cardiovascular mortality and cardiovascular disease or related biomarker measures. Table 3 presents characteristics of analyses investigating the effects of MDS on health outcomes.
Only three cross-sectional analyses failed to find a beneficial relationship between lower MDS and health or nutritional status. Two of these cross-sectional analyses failed to show a relationship with MDS on serum klotho levels [34,52], and the third failed to show a relationship with depression [18]. Two prospective analyses showed a high MDS to be associated with cardiovascular and all-cause mortality but failed to show any relationship with cancer mortality [55,60].
Dietary magnesium intakes were reported in most articles that utilized data cycles from the U.S. NHANES (Table 4). Twenty-three articles reported magnesium intakes by MDS, and all articles providing mean dietary intake levels showed suboptimal magnesium intake below the EAR (<350 magnesium/d) at all MDS levels. Twenty-three articles provided a subgroup analysis of magnesium intakes based on disease or health condition at baseline (e.g., hypertension vs. non-hypertensive), and 18 articles evaluated intakes by cut-offs based on the EAR, RDA, tolerable upper intake level (UL), or median intakes. Only seven articles reported magnesium intake from dietary supplements, with all indicating suboptimal intake from total diet (food + dietary supplements) [13,22,36,45,55,56,58]. Thirteen articles commented on lower magnesium intake being associated with higher MDSs.
4. Discussion
This scoping review highlights the MDS as a new methodology for the determination of magnesium deficiency based on five criteria, and a higher MDS denotes a greater degree of magnesium deficiency. The MDS methodology was applied across 48 articles using well-established NHANES criteria and methodology, data collection, standardized questionnaires (ethyl alcohol intake), and GFR values determined by standardized protocol. Findings of this scoping review suggest that the MDS methodology can serve as a valid tool to assess magnesium deficiency, as it has demonstrated reproducibility and is highly correlated with disease outcomes. The MDS is noninvasive and cost-effective compared to biochemical tests and integrates multiple risk factors, offering a holistic assessment of nutritional status. However, the MDS may better reflect long-term magnesium status compared to serum levels alone, which can fluctuate acutely. There is also a need to appreciate the numerous factors affecting serum magnesium concentrations when considering the reliability of this as a measure of magnesium status, such as diurnal variation, strenuous exercise, various medications, and disease states [5]. It should be noted, however, that the MDS is heavily dependent on kidney function, with the GFR contributing 1 to 2 points; and GFR decreases with age. In addition to chronic kidney disease, high blood pressure, and diabetes, a decrease in GFR is also indicative of disorders such as microinflammation, endothelial dysfunction, oxidative stress, and increased aortic pressure [64]. Liu and colleagues [29] recently demonstrated that dietary magnesium intake and GFR were inversely correlated with risk of stroke, and participants with low dietary magnesium intake had higher stroke risk than those with normal (>254 mg/d) magnesium intake. In this scoping review, two cross-sectional analyses [23,48] evaluating stroke outcomes found that increasing MDS was associated with an increased risk of stroke in individuals with low dietary intakes of magnesium (<254 mg/d). In a prospective study, Xing [59] found that heavy drinking was the most influential factor among the four MDS scoring items that affected mortality outcomes in patients with kidney disease (GFR < 60) and these patients had the lowest mean survival time. Use of PPIs and diuretics was not as highly correlated with survival time. This finding suggests that sample size or disease entity may influence the MDS cut-point indicative of magnesium deficiency and needs further evaluation and validation before being accepted for general use [5].
Regarding the health outcomes under study, the data consistently demonstrated a higher MDS to be associated with an increased risk of all-cause and cause-specific mortality, as well as numerous biomarkers, surrogate endpoints, and chronic disease outcomes. We note the consistent relationship between a higher MDS with increased risks of outcomes known to be associated with low magnesium intake and/or status, such as CVD and hypertension, CKD and impaired kidney function, diabetes and glucose–insulin dynamics, and related biomarkers. Higher MDS was also associated with elevated hs-CRP levels, consistent with the existing scientific literature linking low magnesium intake or status to increased hs-CRP. The scoping review also identified correlations between a higher MDS and several outcomes not traditionally associated with low magnesium intake or status, such as gout and periodontitis. It is possible that a higher MDS reflects poor overall health rather than being causally related to the health outcomes described in this scoping review of observational data from NHANES (see Limitations section).
Limitations
The findings reported here are affected by the limitations of the literature included in this review. Although the data were collected from large datasets, there is some heterogeneity in reporting the results: some authors chose to report means for all components of the MDS tool, and most did not. The MDS scoring methodology varied among included articles, with some reporting scales of 0–2 and others reporting on a scale of 0–5. Some authors chose to report MDS by disease and non-disease subgroups. This scoping review indicates a lack of prospective cohort analyses (aside those using the U.S. NHANES and U.S. National Death Index) of sufficient duration and a lack of RCTs testing whether MDS-guided interventions (e.g., magnesium supplementation, reduced PPI use) improve clinical outcomes. Thus, the findings are limited to NHANES cohorts with varying duration of follow-up, the dietary intake measures were stratified by varying means of classification, and the analyses were conducted exclusively in adults aged ≥18 years. Importantly, prospective analyses of NHANES are limited to all-cause and major disease mortalities recorded in sufficient numbers within the U.S. National Death Index (e.g., CVD, cancer). This constrains our ability to determine which disease outcomes are most influenced by a higher MDS, beyond the evident elevated risk of CVD mortality and the comparatively weaker or null association with cancer mortality. These types of NHANES analyses are further limited by reliance on a single baseline calculated MDS rather than repeated measures widely available in other prospective cohorts.
5. Conclusions
This scoping review synthesized existing evidence reporting the clinical applicability and validity of MDS across broad populations. There is consistent evidence from existing observational studies that demonstrate a high MDS is associated with adverse health status in humans. Higher MDS was also shown to be inversely correlated with dietary magnesium intake across existing observational studies. The MDS, particularly when utilized alongside traditional dietary intake assessment, offers promise as a tool for more rapidly identifying individuals at risk of magnesium deficiency (or insufficiency), and associated comorbidities, although large clinical trials are needed to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bairoch A. The ENZYME database in 2000 Nucleic Acids Res.20002830430510.1093/nar/28.1.30410592255 PMC 102465 · doi ↗ · pubmed ↗
- 2de Baaij J.H. Hoenderop J.G. Bindels R.J. Magnesium in man: Implications for health and disease Physiol. Rev.20159514610.1152/physrev.00012.201425540137 · doi ↗ · pubmed ↗
- 3Caspi R. Billington R. Ferrer L. Foerster H. Fulcher C.A. Keseler I.M. Kothari A. Krummenacker M. Latendresse M. Mueller L.A. The Meta Cyc database of metabolic pathways and enzymes and the Bio Cyc collection of pathway/genome databases Nucleic Acids Res.201644 D 471D 48010.1093/nar/gkv 116426527732 PMC 4702838 · doi ↗ · pubmed ↗
- 4Cowan A.E. Jun S. Tooze J.A. Eicher-Miller H.A. Dodd K.W. Gahche J.J. Guenther P.M. Dwyer J.T. Potischman N. Bhadra A. Total usual micronutrient intakes compared to the dietary reference intakes among U.S. adults by food security status Nutrients 2019123810.3390/nu 1201003831877853 PMC 7019721 · doi ↗ · pubmed ↗
- 5Nielsen F. Magnesium Principles of Nutritional Assessment 3rd ed. Gibson R.S. Oxford University Press New York, NY, USA 2024 Chapter 23.c.Available online: https://nutritionalassessment.org/magnesium/index.html(accessed on 23 August 2025)
- 6Rosique-Esteban N. Guasch-FerréM. Hernández-Alonso P. Salas-SalvadóJ. Dietary magnesium and cardiovascular disease: A review with emphasis in epidemiological studies Nutrients 20181016810.3390/nu 1002016829389872 PMC 5852744 · doi ↗ · pubmed ↗
- 7Dibaba D.T. Xun P. Fly A.D. Yokota K. He K. Dietary magnesium intake and risk of metabolic syndrome: A meta-analysis Diabet. Med.2014311301130910.1111/dme.1253724975384 PMC 4198467 · doi ↗ · pubmed ↗
- 8Hruby A. Meigs J.B. O’Donnell C.J. Jacques P.F. Mc Keown N.M. Higher magnesium intake reduces risk of impaired glucose and insulin metabolism and progression from prediabetes to diabetes in middle-aged americans Diabetes Care 20143741942710.2337/dc 13-139724089547 PMC 3898748 · doi ↗ · pubmed ↗