microRNA Biomarkers in Paediatric Infection Diagnostics—Bridging the Gap Between Evidence and Clinical Application: A Scoping Review
Oenone Rodgers, Anna De Beer, Thomas Waterfield

TL;DR
This review explores microRNA biomarkers for diagnosing bacterial and viral infections in children, highlighting promising candidates and challenges in clinical application.
Contribution
The study identifies specific miRNAs consistently associated with bacterial and viral infections in children and evaluates their diagnostic potential.
Findings
Three miRNAs (hsa-miR-182-5p, hsa-miR-363-3p, hsa-miR-206) are consistently linked to bacterial infections in children.
Nine miRNAs are associated with viral infections, with diagnostic metrics showing high sensitivity and specificity.
Clinical translation is hindered by poor adherence to diagnostic guidelines and study heterogeneity.
Abstract
Background: Distinguishing between bacterial and viral infections in children remains a significant challenge for clinicians. Traditional biomarkers have limited utility, often leading to antibiotic overprescription due to clinician uncertainty. With rising antimicrobial resistance, novel biomarkers are needed to improve diagnosis. This scoping review examines current host miRNA biomarkers for acute bacterial and viral infections in children (0–18), focusing on study methods, diagnostic metrics, and research gaps to support clinical translation. Results: Of the 1147 articles identified, 36 studies were included. Notably, 72.2% of the studies originated from Asia, and the distribution across the paediatric age groups was relatively even. A total of 17 miRNAs were validated in at least two independent studies. Three miRNAs, hsa-miR-182-5p, hsa-miR-363-3p, and hsa-miR-206, were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
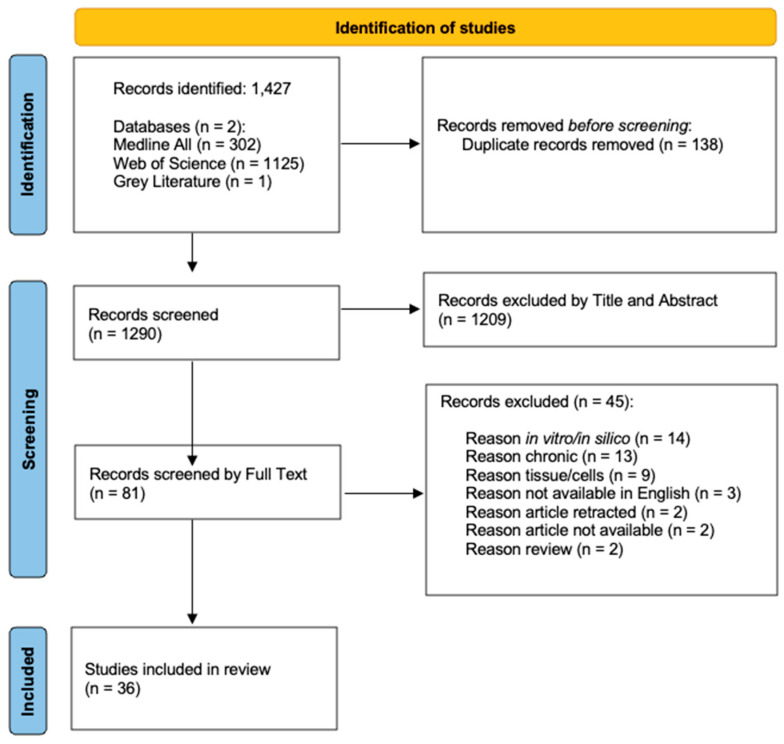 Figure 1
Figure 1| Author [Citation] | Year | Study Methods | RNA Extraction Kit | NGS Kit | Sample Type (Volume) | Normalisation |
|---|---|---|---|---|---|---|
| Jone, et al. [ | 2020 | Microarray | Own Methods | N/A | Serum (3 mL) | hsa-miR-320 |
| Zhang, et al. [ | 2020 | NGS + RT-qPCR | Trizol Reagent | NEBNext Ultra RNA Library Prep Kit for Illumina | Whole blood | U6 |
| Zhang, et al. [ | 2021 | RT-qPCR | Trizol Reagent | N/A | Whole blood | U6 |
| Tian, et al. [ | 2021 | RT-qPCR | Trizol Reagent | N/A | BALF | U6 |
| Mao, et al. [ | 2021 | RT-qPCR | Trizol Reagent | N/A | Serum | U6 |
| Liu, et al. [ | 2024 | RT-qPCR | miRNeasy Serum Kit | N/A | Serum | U6 |
| Kyo, et al. [ | 2024 | NGS | Direct-zol RNA Miniprep Kit | NEXTFLEX® small RNAseq v3 kit with Unique Dual Indexes | Nasal + Nasopharyngeal | N/A |
| Yin, et al. [ | 2021 | Microarray + | Trizol Reagent | N/A | Plasma | Actb |
| Arroyo, et al. [ | 2020 | Viral PCR, + miRNA RT-qPCR | MirVana miRNA isolation kit | N/A | Nasal | cel-mir-39 |
| Janec, et al. [ | 2024 | Luminex® and NGS | miRNeasy Serum/Plasma Kit | NEXTFlex small RNA-Seq v3 | Plasma (100 µL) | N/A |
| Zhu, et al. [ | 2023 | NGS | Direct-zol RNA Miniprep Kit | NEXTFLEX® small RNA-seq v3 kit with Unique Dual Indexes | Nasal + Nasopharyngeal | N/A |
| Savino, et al. [ | 2023 | RT-qPCR | Promega Simply RNA Blood Kit | N/A | Throat swab (1 mL) + Heparinised blood (200 µL) | RNU43 |
| Ernst, et al. [ | 2021 | Microarray | miRNeasy Serum/Plasma Advanced Kit | N/A | Cord plasma + Cord tissue | Global normalisation |
| Huang, et al. [ | 2021 | RT-qPCR + ELSIA | miRNeasy Serum/Plasma Kit | N/A | Plasma (3–5 mL) | U6 |
| Beheshti, et al. [ | 2023 | NGS + ELLA | miRNeasy Kit | Illumina TruSeq Small RNA Prep protocol | Saliva | N/A |
| Jia, et al. [ | 2023 | RT-qPCR + ELISA | Trizol Reagent | N/A | Plasma | U6 |
| Sriprapun, et al. [ | 2023 | RT-qPCR | miRNeasy mini kit | N/A | Serum | hsa-miR-16-5p |
| Torii, et al. [ | 2022 | NGS | miRCURY Exosome Cell/Urine/CSF kit + miRCURY Exosome Serum/Plasma kit | NEBNext Multiplex Small RNA Library Prep Set for Illumina | CSF (31–1418 mL) + Serum (120 mL) | hsa-miR-204-5p |
| Qi, et al. [ | 2014 | Microarray + | mirVana PARIS kits | N/A | Serum (400 µL) | cel-miR-238 |
| Chen, et al. [ | 2014 | Microarray + | Trizol Reagent | N/A | Leukocytes | used but does not mention |
| Wang, et al. [ | 2016 | Microarray + | mirVana PARIS kit | N/A | Serum (100 µL) | Global Normalisation + U6 |
| Gao, et al. [ | 2015 | RT-qPCR | miRNeasy serum/plasma kit + miRNeasy mini kit | N/A | Plasma (200 µL) + PBMCs | U6 + cel-miR-39 |
| Liu, et al. [ | 2015 | RT-qPCR | Trizol Reagent | N/A | PBMCs | GAPDH + U6 |
| Inchley, et al. [ | 2015 | Microarray + | miRNeasy mini kit | N/A | Nasal | RNU24 |
| Dhas, et al. [ | 2018 | RT-qPCR* | miRNeasy Serum/Plasma kit | N/A | Plasma (500 µL) | cel-miR-39 |
| Kawano, et al. [ | 2016 | RT-qPCR | mirVana PARIS Kit | N/A | Plasma | hsa-miR-16 |
| Gutierrez, et al. [ | 2016 | Microarray | SeraMir kit | N/A | Nasal | Global normalisation |
| Min, et al. [ | 2018 | RT-qPCR | Biofluid extraction kit (Exiqon, Inc., Woburn, MA, USA) | N/A | Throat swab + Saliva | hsa-miR-23a-3p |
| Hasegawa, et al. [ | 2018 | Microarray + NGA | Norgen RNA/DNA Purification Kit | Nasal | Global Normalisation | |
| Li, et al. [ | 2019 | RT-qPCR | mirVanaTM miRNA Isolation Kit | N/A | PMBCs | U6 |
| Huang, et al. [ | 2019 | NGS + RT-qPCR | Trizol Reagent | NEBNext® Multiplex Small RNA Library Prep Set for Illumina® | Serum exosomes | N/A |
| Huang, et al. [ | 2018 | NGS + RT-qPCR | RiboPure™ Blood RNA Isolation Kit | Own Method | Whole blood | U6 |
| Cui, et al. [ | 2012 | Microarray + RT-qPCR | mirVana PARIS kit | N/A | Serum (400 μL) | cel-miR-238 |
| Gao, et al. [ | 2024 | RT-qPCR | Trizol Reagent | N/A | Serum | U6 |
| Hamdy, et al. [ | 2024 | RT-qPCR | miRNeasy Serum/Plasma Kit | N/A | Serum | hsa-miR-16-5p |
| Qi, et al. [ | 2025 | RT-qPCR | Trizol Reagent | N/A | Serum | U6 |
| Author [Citation] | Biomarkers | Clinical Question | Study Methods | Ages | Sample Size | CRP/PCT | Reference Standard | ||
|---|---|---|---|---|---|---|---|---|---|
| Jone et al. [ |
miR-210-3p miR-184 miR-19a-3p | Kawasaki and Febrile Non-Kawasaki | Microarray | Febrile = 3.5–13 years | n = 113 | CRP | Lab confirmed | ||
| Zhang et al. [ |
miR-101-3p PCT | Neonatal Sepsis vs. Respiratory Infection/Pneumonia | RT-qPCR | Neonatal sepsis = 11.88 days | n = 148 | CRP + PCT | Lab confirmed + clinical | ||
| Tian et al. [ |
miR-155 IL-9 | MRSA Pneumonia vs. Bronchial Foreign Bodies | RT-qPCR | <18 years | n = 40 | Guidelines | |||
| Mao et al. [ |
miR-455-5p | Neonatal Sepsis vs. Healthy | RT-qPCR | Neonatal sepsis = 10.21 days | n = 178 | CRP + PCT | Lab confirmed + clinical | ||
| Yin et al. [ |
miR-1323 IL-6 | Mycoplasma Pneumoniae Pneumonia vs. Healthy | Microarray + | MPP =7.1 years | n = 57 | CRP | Lab confirmed | ||
| Janec et al. [ |
miR-136-3p miR-142-5p miR-148b-3p |
miR-182-5p miR-183-5p miR-223-3p |
miR-363-3p miR-629-5p miR-3613-5p | Neonatal Sepsis vs. Healthy | Luminex®
| 1 day | n = 20 | Lab confirmed | |
| Ernst et al. [ |
miR-211-5p miR-223-5p miR-331-5p miR-181d-5p miR-146b-5p |
miR-142-3p miR-193a-5p miR-532-5p miR-363-3p |
miR-15a-5p miR-202-3p miR-206 miR-150-5p | EOS vs. Presumed Sepsis vs. Healthy | Microarray | 1 day | n = 41 | Lab confirmed + Clinical | |
| Huang et al. [ |
miR-497 FABP3 |
GPBB cTnI | Sepsis vs. Sepsis and Myocardial Injury vs. Healthy | RT-qPCR + ELSIA | median age | n = 132 | CRP + PCT | Clinical Guidelines | |
| Jia et al. [ |
miR-492 TNF-α |
IL6 IL-18 | Mycoplasma Pneumoniae Pneumonia vs. Healthy | RT-qPCR + ELSIA | median age | n = 86 | CRP | Lab confirmed | |
| Chen et al. [ |
miR-208a miR-489 miR-618 miR-644 miR-491-3p miR-450a miR-509-3-5p miR-720 |
miR-886-3p miR-486-3p miR-1184 miR-375 miR-637 miR-548a-3p miR-185 miR-761 |
miR-620 miR-122 miR-549 miR-135a miR-611 miR-551b miR-1299 | Neonatal Sepsis vs. Healthy | Microarray + | median age | n = 48 | Lab confirmed + clinical | |
| Dhas et al. [ |
miR-223 miR-132 | EOS vs. Healthy | RT-qPCR | <3 days old | n = 50 | CRP | Clinical only | ||
| Li et al. [ |
miR-29 | Mycoplasma Pneumoniae Pneumonia vs. Healthy | RT-qPCR | median age | n = 78 | CRP | Lab confirmed | ||
| Cui et al. [ |
miR-202 miR-342-5p miR-576-5p |
miR-206 miR-487b | B. Pertussis vs. Healthy | Microarray + | median age | n = 134 | Lab confirmed | ||
| Hamdy et al. [ |
miR-182-5p miR-590-3p | Neonatal Sepsis vs. Healthy | PCR | <21 days | n = 110 | CRP | Lab confirmed | ||
| Author [Citation] | Year | Biomarkers | Clinical Question | Study Methods | Ages | Sample Size | CRP/PCT | Reference Standard | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Jone et al. [ | 2020 |
miR-210-3p miR−184 miR-19a-3p. | Kawasaki and Febrile Non-Kawasaki | Microarray | Febrile = 3.5–13 years | n = 113 | CRP | Lab confirmed | ||
| Zhang et al. [ | 2020 |
miR-1271-5p miR-10a-3p miR-125b-5p |
miR-100-5p miR-30b-3p | Mild or Severe RSV-Associated Pneumonia | NGS + RT-qPCR | Median age | n = 46 | CRP | Lab confirmed + clinical | |
| Liu et al. [ | 2024 |
miR-142-3p | Viral Encephalitis vs. Healthy | RT-qPCR | Median age | n = 196 | Lab confirmed + clinical | |||
| Kyo et al. [ | 2024 |
miR-991-5p miR-125b-2-3p miR-99b-3p | Severity of RSV Bronchiolitis | NGS | Median age | n = 493 | Lab confirmed + clinical | |||
| Arroyo et al. [ | 2020 |
miR-155 | Viral Respiratory Infections vs. Healthy | RT-qPCR + protein detection | Median age | n = 151 | Lab confirmed | |||
| Zhu et al. [ | 2023 |
miR-29 miR-22–3p | Severe Bronchiolitis: No Asthma vs. With Asthma | NGS | Median age | n = 575 | Clinical only | |||
| Savino et al. [ | 2023 |
miR-155 | RSV vs. Healthy | RT-qPCR | Median age | n = 66 | Lab confirmed | |||
| Beheshti et al. [ | 2023 |
miR-140-3p miR-22-5p miR-29 miR-34c-5p |
miR-125a-5p miR-27b-3p miR-203a-3p miR-155-5p | URTIs in the first 12 months after birth | NGS + protein detection | <1 year | n = 146 | Clinical only | ||
| Sriprapun et al. [ | 2023 |
miR-126-3p | Dengue vs. Acute Febrile Illness | RT-qPCR | Median age | n = 90 | Lab confirmed + clinical | |||
| Torii et al. [ | 2022 |
miR-381-3p miR-155 miR-148a miR-664a-3p |
let-7b-5p let-7i-5p miR-483-5p miR-151a |
miR-499a-5p miR-140-3p miR-206-3p | Human Herpesvirus 6 (HHV-6): | NGS | Median age | n = 15 | Lab confirmed | |
| Qi et al. [ | 2014 |
miR-197 miR-363 miR-629 |
miR-132 miR-122 | Varicella vs. Healthy | Microarray + | Median age | n = 102 | Lab confirmed + clinical | ||
| Wang et al. [ | 2016 |
miR-494 miR-29 miR-551a |
miR-606 miR-876-5p miR-30c-5p |
miR-221-3p miR-150-5p | EV71 (Severe + Mild) vs. Healthy | Microarray + | Median age | n = 12 | Clinical only | |
| Gao et al. [ | 2015 |
miR-155-5p miR-34a-5p miR-18b-5p |
miR-181a-5p miR-142-5p miR-134-5p |
miR-18b-5p miR-34a-5p miR-196a-5p | EBV vs. Healthy | RT-qPCR | Median age | n = 30 | Lab confirmed + clinical | |
| Liu et al. [ | 2015 |
miR-26 | RSV vs. Healthy | RT-qPCR | <1 year | n = 40 | Lab confirmed + clinical | |||
| Inchley et al. [ | 2015 |
miR-155 miR-31 miR-203a |
miR-16 let-7d | RSV vs. Healthy | Microarray + | <1 year | n = 61 | Lab confirmed | ||
| Kawano et al. [ | 2016 |
miR-183-5p miR-210-3p | CMV vs. Healthy | RT-qPCR | Median age | n = 23 | Lab confirmed + clinical | |||
| Gutierrez et al. [ | 2016 |
miR-155 miR-21 | RV vs. non-RV | Microarray | Median age | n = 20 | Lab confirmed | |||
| Min et al. [ | 2018 |
miR-221 | HEV vs. Healthy | PCR | <5 years | n = 59 | Lab confirmed | |||
| Hasegawa et al. [ | 2019 |
miR-149-3p miR-197-3p miR-197-5p miR-296-3p |
miR-149-3p miR-504-3p miR-155-5p | Sole Rhinovirus Infection vs. Sole RSV Infection | Microarray + protein detection | <6 months | n = 32 | Lab confirmed | ||
| Huang et al. [ | 2019 |
miR-103b-5p miR-450a-5p |
miR-98-5p miR-103a-3p | HAdV vs. Healthy | NGS + RT-qPCR | Median age | n = 59 | Lab confirmed + clinical | ||
| Huang et al. [ | 2018 |
miR-381-3p miR-486-5p miR-409-3p miR-486-3p miR-127-3p miR-182-5p miR-99b-5p |
miR-379-5p miR-370-3p let-7e-5p miR-493-5p miR-494-3p miR-101-3p miR-142-3p |
miR-150-5p miR-29a-3p miR-186-5p miR-27a-3p miR-342-3p miR-29b-3p | HAdV vs. Healthy | NGS + RT-qPCR | Median age | n = 6 | CRP | Lab confirmed + clinical |
| Gao et al. [ | 2024 |
miR-425-3p NEAT1 | Viral Induced Myocarditis vs. Healthy | RT-qPCR | 3–8 years | n = 108 | CRP | Lab confirmed + clinical | ||
| Qi et al. [ | 2025 |
miR-200b | Pneumonia vs. Healthy | RT-qPCR | 2–10 years | n = 218 | CRP | Lab confirmed + clinical | ||
| Author [Citation] | Bacterial or | Sensitivity | Specificity | AUC | Cut off Value |
|---|---|---|---|---|---|
| Jone et al. [ | Bacterial + Viral | 76.9% | 76.9% | 0.769 | N/A |
| Zhang et al. [ | Bacterial | 80.2% (with PCT) | 76.1% (with PCT) | 0.904 (with PCT) | 1.202 |
| Mao et al. [ | Bacterial | 80.2% | 85.2% | 0.895 | 1.254 |
| Liu et al. [ | Viral | 75% | 88.04% | 0.8675 | N/A |
| Ernst et al. [ | Bacterial | Cord plasma = 62.5% | Cord plasma = 90% | Cord plasma = 0.79 | Cord plasma = −8.13 |
| Huang et al. [ | Bacterial | miR-497 = 95.65% | miR-497 =83.33% | N/A | miR-497 =2.03 |
| Qi et al. [ | Viral | 93.1% | 72% | 0.872 | −13.03 |
| Min et al. [ | Viral | 100% | 88.89% | N/A | N/A |
| Cui et al. [ | Bacterial | miR-202 = 97.4% | miR-202 = 87.2% | miR-202 = 0.981 | miR-202 = −5.91 |
| Gao et al. [ | Viral | miR-425-3p = 79.63% | miR-425-3p = 77.45% | miR-425-3p = 0.832 | N/A |
| Hamdy et al. [ | Bacterial | miR-182-5P = 62% | miR-182-5P = 100% | miR-182-5P = 0.620 | N/A |
| Qi et al. [ | Viral | 83.3% | 89.8% | 0.909 | N/A |
- —Queen’s University Belfast
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Streptococcal Infections and Treatments · Nosocomial Infections in ICU
1. Introduction
Febrile children present a significant challenge across global healthcare systems. Fever is the most common reason for children to present to Emergency Departments (ED) [1]. In the paediatric European population, antibiotic overprescription is an issue, with prescribing rates approaching 64%, with only approximately 13% benefiting from these prescriptions [1,2]. The global overuse of antibiotics in children results in increased healthcare costs and worsening antibiotic resistance [3]. These issues do not just occur in paediatrics, with global estimates suggesting that antibiotic prescribing has increased by 16.3% between 2016 and 2023 [4]. The most pronounced increases were in upper-middle and low-middle-income countries [4]. It is projected that by 2030 global antibiotic consumption will increase by a further 52.3% above 2023’s value [4]. In 2021 there were 193,000 global paediatric deaths attributed to antimicrobial resistant organisms [5], with a notable increase in antimicrobial resistant paediatric sepsis, where 31.3% of cases were associated with drug-resistant bacterial infections [5]. This surge in antibiotic resistance coupled with the absence of novel antimicrobials is a substantial threat to public health [6].
Clinicians overprescribe antibiotics primarily due to uncertainty. Differentiating between bacterial and viral infections is challenging due to the significant overlap in clinical presentations. The gold standard for diagnosing sterile site bacterial infections is via culturing. However, this process has a long wait time for results and is limited by issues with contamination and difficult-to-culture pathogens [7]. Molecular testing for pathogens has also been shown to be poorly specific, with positive viral testing results often representing colonisation rather than active infection [8]. Therefore, clinicians often rely on biomarkers to ensure appropriate treatment and antimicrobial stewardship efforts for febrile children. The most studied biomarkers are C-reactive protein (CRP) and procalcitonin (PCT) [9]. Clinically, biomarkers can be assessed in numerous biofluid samples, particularly from blood, cerebrospinal fluid, and urine [9]. The most used blood-based biomarker is CRP; however, it is not bacterial infection-specific and substantial elevations occur with other inflammatory or infectious causes [9]. Furthermore, CRP has been found not to improve the selection of a low-risk group of children at ED presentation [10]. Screening with PCT is recommended by three major global clinical practice guidelines [11,12,13]. However, a meta-analysis of the performance of PCT to that of CRP for serious bacterial infections in young infants suggests that they hold similar diagnostic accuracy metrics [14]. PCT is not a biomarker specific to bacterial infection, and its lack of superiority over CRP has led to NICE guidelines not recommending its routine use in the UK [15]. Therefore, the lack of a reliable biomarker leads to uncertainty and over prescribing of antibiotics ‘just in case’.
The focus for paediatric infection diagnostics revolves around circulating biomarkers, as they are relatively non-invasive and easily integrated into clinical workflows. Any new diagnostic tool must therefore offer a like-for-like replacement or be combined with current testing to be viable in practice. The search for the ideal biomarker for paediatric infection diagnostics has largely underperformed [16]. Previous efforts primarily targeted single protein biomarkers, but researchers are now exploring biomarker panels that include both proteins and other biomolecules. The growing application of omics approaches has led to the identification of many potential biomarker candidates across a range of clinical disciplines; however, their integration into routine clinical practice has been slow [17,18]. Significant hurdles have impacted the success of novel diagnostics for clinical use. These include large discrepancies in the diagnostic criteria used for clinical research and the consequential variations in biomarker discovery results and reliability. Furthermore, when promising candidates have been identified, these markers are rarely validated in large external cohorts [19,20]. Even when validation studies have been conducted, a key barrier to clinical implementation is the lack of protocol consistency in validation studies. This prevents meaningful cross-study comparisons, impedes biomarker prioritisation, and ultimately stagnates clinical biomarker outputs. A further complication arises from the high demands placed on clinical biomarkers. To be considered for implementation, candidates must demonstrate substantial improvements over existing tests in heterogeneous populations, while also offering a favourable cost–benefit profile. In the context of infection diagnostics, this means outperforming established markers such as CRP and PCT, which are inexpensive, readily available, and often considered ‘good enough’ for continued clinical use. This is highlighted by the routine use of PCT in some healthcare systems, particularly in the United States. However, PCT is not routinely implemented in the UK due to a lack of cost–benefit ratio supporting widespread use.
Former work has identified host-RNA signatures in paediatric infectious disease [21] that show promise for alternative routes to infection differentiation. Among these alternative routes are microRNA (miRNA), short non-coding RNAs that regulate post-transcriptional gene expression, which may offer novel diagnostic insight. Compared to classical protein biomarkers, miRNAs present several advantages for paediatric infection diagnostics. They demonstrate high sensitivity and specificity, undergo rapid changes in abundance in response to disease, and are readily accessible through minimally invasive sampling of biofluids such as blood, saliva, or urine [22]. Furthermore, miRNAs demonstrate excellent physicochemical stability within biofluid samples, particularly in whole blood, serum, and plasma [23,24], which makes miRNAs particularly suitable for clinical diagnostics. Of particular interest is the timing of miRNA abundance changes, which may occur more rapidly than the protein biomarkers in current clinical use. This characteristic could make miRNAs especially valuable for early diagnosis in paediatric hospital triage, where timely clinical decisions are critical. By enabling faster identification of infectious causes, miRNA-based diagnostics have the potential to reduce delays commonly associated with conventional methods such as blood cultures or screening via CRP or PCT which tend to rise late in the disease course. However, miRNA as targets for bacterial and viral differentiation have not been fully established.
The literature on paediatric infection diagnostics utilising miRNA targets is highly varied and relatively scarce. Given the early stage of research in this area and the broad scope of the research question, a scoping review is an appropriate methodological approach to the topic. This scoping review aims to summarise the published human miRNA signatures associated with acute bacterial and viral infections in children. This review also aims to examine the methodologies and diagnostic metrics used across studies to identify research gaps and support the advancement of clinically translatable applications.
2. Results
2.1. Search Selection and Study Characteristics
A total of 1147 articles were identified: 302 articles from the Ovid Medline All database, 1125 articles from the Web of Science Core Collection, and a singular article from the grey literature search. A total of 138 duplicate records were removed, leaving 1290 articles to be screened. A total of 1209 articles were removed by title and abstract; this culminated in 81 articles for full-text review. Following the full-text review, 45 articles were excluded, resulting in 36 articles to be included within the study. Reasons for exclusion during the full-text review are presented in the PRISMA-ScR flow diagram (Figure 1).
The included articles were published between 2012 and 2025, all of which were cohort studies. Studies were predominantly conducted in China (20/36; 55.6%) [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42], the United States (8/36; 22.2%) [43,44,45,46,47,48,49,50], Japan (2/36; 5.5%) [51,52], Czech Republic (1/36; 2.8%) [53], Italy (1/36; 2.8%) [54], Thailand (1/36; 2.8%) [55], Taiwan (1/36; 2.8%) [56], Norway (1/36; 2.8%) [57], India (1/36; 2.8%) [58], Egypt (1/36; 2.8%) [59], and Singapore (1/36; 2.8%) [60]. Within these, 35 (97%) articles recruited patients who were hospitalised [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,49,50,51,52,53,54,55,56,57,58,59,60] and 1 (2.8%) article recruited non-hospitalised children [48].
2.2. Characteristics of Populations
The characteristics of the studies and populations are shown in Table 1. The eligible studies involved a total of 3885 subjects, ranging from 6 to 575 subjects per study. The percentages of female subjects per study ranged from 14% to 67%. Within the 36 included studies, children aged from newborn to 13 years were investigated. For the purposes of this study, neonates were classified as 0 to 28 days old, infants were classified as 29 to 364 days old, toddlers were classified as 1 to 5 years old, and children were classified as 5 to 13 years old. Within these categories there were 9 neonatal studies (9/36; 25%) [26,28,34,47,48,52,53,58,59], 7 infant studies (7/36; 19.4%) [25,36,40,44,46,54,57], 9 toddler studies (9/36; 25%) [33,38,39,45,49,50,51,56,60], and 11 studies on children (11/36; 30.6%) [27,29,30,31,32,35,37,41,42,43,55]. The majority of the studies compared infection to healthy controls (24/36; 66.6%) [28,29,30,32,33,34,35,36,37,38,39,40,45,49,52,53,54,57,58,60], while fewer investigated infection to another disease state (9/36; 25%) [26,27,31,43,46,47,50,51,55], and an additional three studies investigated the severity of disease (3/36; 8.3%) [25,44,56].
A total of 14 studies included bacterial infections (14/36; 38.8%) [26,27,28,29,31,32,34,37,40,43,47,53,58,59], and 23 studies included viral infections (23/36; 63.8%) [25,30,33,35,36,38,39,41,42,43,44,45,46,48,49,50,51,52,54,55,56,57,60], of which 1 study included bacterial and viral infections (2.8%) [43]. The bacterial infections included within the studies were as follows: sepsis (173/449; 38.5%), Mycoplasma pneumoniae (129/449; 28.7%), Bordetella pertussis (66/449; 14.7%), methicillin-resistant Staphylococcus aureus (30/449; 6.7%), Staphylococcus aureus (19/449; 4.2%), Escherichia coli (7/449; 1.6%), Acinetobacter baumannii (5/449; 1.1%), Klebsiella species (4/449; 0.9%), Enterococcus (3/449; 0.7%), Neisseria meningitidis (2/449; 0.4%), Group A Streptococcus (2/449; 0.4%), Group B Streptococcus (2/449; 0.4%), pneumococcal meningitis (2/449; 0.4%), Salmonella serotype Typhi (1/449; 0.2%), and Listeria monocytogenes (1/449; 0.2%).
The viral infections included within the studies were as follows: Respiratory syncytial virus (1026/1738; 59%), Rhinovirus (218/1738; 12.5%), Respiratory syncytial virus and Rhinovirus coinfection (69/1738; 4%), Enterovirus (62/1738; 3.6%), Dengue virus (60/1738; 3.5%), Hand, foot, and mouth disease (59/1738; 3.4%), Adenovirus (53/1738; 3%), Herpesviridae species (45/1738; 2.6%), Varicella-zoster virus (39/1738; 2.2%), Epidemic B virus (22/1738; 1.3%), Human metapneumovirus (22/1738; 1.3%), Epstein–Barr virus (16/1738; 0.9%), Congenital cytomegalovirus (13/1738; 0.7%), Parotid virus (11/1738; 0.6%), Parainfluenza (11/1738; 0.6%), Influenza (11/1738; 0.6%), and Haemophilus influenza (1/1738; 0.1%).
2.3. Reference Standards
The reference standards for diagnosis and categorisation of the patients were as follows: six studies relied on clinical guidelines and clinical diagnosis alone (6/36; 16.7%) [27,31,46,48,56,58]. Laboratory-confirmed infection was used as the reference standard for 13 studies (13/36; 36.1%) [29,32,37,40,43,45,49,50,51,53,54,57,60], and 17 studies used combined laboratory-confirmed infection with clinical diagnosis (17/36; 47.2%) [25,26,28,30,33,34,35,36,38,39,44,47,52,55]. The laboratory-confirmed infection methods were as follows: PCR (13/30; 43.3%) [25,29,33,36,41,42,44,45,49,50,51,52,59,60], antibodies (4/30; 13.3%) [30,32,35,38], blood culture (5/30; 16.6%) [26,34,47,53], PCR with antigen/antibody/culture (4/30; 13.3%) [37,39,40,57], antigen alone (1/30; 3.3%) [54], and laboratory tests completed but specifics not mentioned (3/30; 10%) [28,43,55].
Of the six the studies relying only on clinical guidelines and clinical diagnosis alone, two studies [27,31] relied on clinical guidelines (2/6; 33.3%). These guidelines were the diagnostic criteria for pneumonia in the 2016 clinical practice guidelines of the American Society of Infectious Diseases and the American Thoracic Society [61], and the diagnostic criteria for sepsis was based on the Expert Consensus on the Diagnosis and Treatment of Septic Shock (Infectious Shock) in Children (2015 Edition) [62]. The remaining four studies [46,48,56,58] relied on clinical diagnosis for bronchiolitis, diagnosis of pneumonia, prescription for albuterol, prescription of oral steroids, clinical symptoms of enterovirus infection, or clinically diagnosed neonatal sepsis.
2.4. Study Methodologies
Within the 36 included studies, RT-qPCR was the most common methodology (27/36; 75%). The majority of the studies utilised relative RT-qPCR (26/27; 96.3%), with the remaining study utilising absolute RT-qPCR. This was followed by microarray (10/36; 27.7%), then next-generation sequencing (8/36; 22.2%), protein detection (5/36; 13.8%), and viral PCR testing (1/36; 2.8%). Table 2 summarises the methodologies of the included studies.
2.5. RNA Extraction Methods
The RNA extraction methodology most commonly used was Trizol reagent, with no reference to specific kits (11/36; 30.6%), followed by the miRNeasy Serum/Plasma Kit (7/36; 19.4%), mirVana PARIS Kit (6/36; 16.7%), miRNeasy Mini Kit (3/36; 8.3%), Direct-zol RNA Miniprep Kit (2/36; 5.6%), miRNeasy Serum/Plasma Advanced Kit (1/36; 2.8%), miRCURY Exosome Cell/Urine/CSF kit (1/36; 2.8%), miRCURY Exosome Serum/Plasma Kit (1/36; 2.8%), Promega simply RNA Blood Kit (1/36; 2.8%), System Biosciences SeraMir Kit (1/36; 2.8%), Exiqon biofluid extraction Kit (1/36; 2.8%), Norgen RNA/DNA Purification Kit (1/36; 2.8%), RiboPure™ Blood RNA Isolation Kit (1/36; 2.8%), and one study using their own methodology (1/36; 2.8%).
2.6. Next-Generation Sequencing Methods
Studies investigating samples via next-generation sequencing used a variety of methodologies, with PerkinElmer NEXTFLEX^®^ small RNAseq v3 kit being the most commonly used (3/8; 37.5%), followed by NEBNext Multiplex Small RNA Library Prep Set for Illumina (2/8; 25%), NEBNext Ultra RNA Library Prep Kit for Illumina (1/8; 12.5%), Illumina TruSeq Small RNA Prep protocol (1/8; 12.5%), and one study using its own methodology (1/8; 12.5%).
2.7. Sample Type and Volume
The most common sample type recruited for the studies was serum (10/36; 27.8%), followed by nasal secretions, throat swabs, and saliva (9/36; 25%), plasma (9/36; 25%), whole blood (6/36; 16.7%), bronchoalveolar lavage (1/36; 2.8%), and cerebrospinal fluid (1/36; 2.8%). Sample volumes were only reported for 11/36 studies: for plasma samples the median volume was 200 µL (range from 100 µL to 5000 µL), and for serum samples the median volume was 800 µL (range from 100 µL to 3000 µL). There was also one study reporting a throat swab sample volume of 1 mL [54], and another reporting 1 mL of cerebrospinal fluid [51].
2.8. Normalisation miRNA
A total of 31 studies referenced a methodology for normalisation. The majority of the studies referenced a specific reference molecule (26/31; 83.9%), whereas studies using global mean normalisation methods were less common (4/31; 12.9%). Six of the studies reported to use human endogenous miRNA (6/31; 19.4%). Endogenous normalisers included the following: hsa-miR-320, hsa-miR-204-5p, hsa-miR-23a-3p, and hsa-miR-16(-5p), and were used three times. A total of 17 studies (17/31; 54.8%) reported using non-miRNA references, of which U6 accounted for 14 of the studies (14/31; 45.2%). Five studies reported using spiked-in RNA (5/31; 16.1%) including cel-miR-39 and cel-miR-238. One study reported using normalisation methodology but was unspecific in their description (1/31; 3.2%).
2.9. Included Current Blood-Based Biomarkers
Of the 36 included studies, 13 (36.1%) reported to have incorporated current clinical biomarkers of infection, including CRP and PCT. CRP was mentioned in all 13 of the studies (100%), whereas PCT was only referred to in 3 studies (23.1%).
2.10. Novel miRNA Biomarkers Identified
Discovered within the 36 included studies, there were 164 human miRNAs identified with paediatric infection. There were 16 miRNAs that were identified more than once across the studies, shown in Table 3: hsa-miR-155 (6/36; 16.7%), hsa-miR-29 (5/36; 13.9%), hsa-miR-206 (4/36; 11.1%), hsa-miR-142-3p (3/36; 8.3%), hsa-miR-182-5p (3/36; 8.3%), hsa-miR-155-5p (2/36; 5.5%), hsa-miR-101-3p (2/36; 5.5%), hsa-miR-140-3p (2/36; 5.5%), hsa-miR-142-5p (2/36; 5.5%), hsa-miR-142-3p (2/36; 5.5%), hsa-miR-150-5p (2/36; 5.5%), hsa-miR-183-5p (2/36; 5.5%), hsa-miR-210-3p (2/36; 5.5%), hsa-miR-34 (2/36; 5.5%), hsa-miR-363-3p (2/36; 5.5%), and hsa-miR-486-3p (2/36; 5.5%). These duplications account for 47 miRNAs from the total of 164 identified, and the remaining 117 miRNAs were only identified once across the studies.
2.11. Bacterial Infection-Associated miRNA
Table 4 summarises the miRNA associations with acute bacterial infections. From the 14 studies that included bacterial samples, 64 miRNAs were identified, with 3 of the miRNAs being validated across two separate studies. hsa-miR-182-5p (2/14; 14.3%), hsa-miR-363-3p (2/14; 14.3%), and hsa-miR-206 (2/14; 14.3%) were all identified with neonatal sepsis [47,53,59].
Predominantly, the studies investigating bacterial samples compared infection to healthy controls (9/14; 64.3%), whereas fewer comparisons were made between infection and other disease (5/14; 35.7%). Most of the studies related to paediatric or neonatal sepsis (8/14; 57.1%), followed by studies on pneumonia and respiratory infection (5/14; 35.7%), and one study comparing Kawasaki Disease to febrile controls with bacterial infection (1/14; 7.1%).
2.12. Viral Infection-Associated miRNA
Table 5 summarises the miRNA associations with acute viral infections. From the 23 studies that included viral samples, 100 miRNAs were identified. Ten of these miRNAs of were validated by at least two separate studies: hsa-miR-155 (5/23; 21.7%), hsa-miR-29a-3p (4/23; 17.4%), hsa-miR-155-5p (2/23; 8.7%), hsa-miR-150-5p (2/23; 8.7%), hsa-miR-140-3p (2/23; 8.7%), hsa-miR-142-3p (2/23; 8.7%), hsa-miR-149-3p (2/23; 8.7%), hsa-miR-210-3p (2/23; 8.7%), and hsa-miR-34a-5p (2/23; 8.7%).
The majority of the studies investigating viral samples compared infection to healthy controls (14/23; 60.9%), whereas fewer studies compared infection to infection, or included severity of the same infection (8/23; 37.8%). One study (1/23; 4.3%) was also a prospective cohort study with no comparator group. A large proportion of the viral studies focused on respiratory infections (16/23; 69.6%), whereas the remaining studies were systemic viral infections or not specifically grouped (7/23; 30.4%).
Table 6 summarises the infection groupings per infection sub-type. From the 100 miRNAs associated with viral infection, 68% can be grouped into an infection type. There were 14 miRNAs (14/68; 20.6%) associated with respiratory syncytial virus, 24 (24/68; 35.3%) associated with human adenovirus infection, 8 (8/68; 11.8%) associated with rhinovirus infection, and 22 (22/68; 32.4%) associated with systemic viral infection. In contrast, of the 64 miRNAs associated with bacterial infection, 59 (90.6%) can be grouped into an infection type. A total of 50 miRNAs (50/59; 84.7%) were associated with sepsis, and 9 (9/59; 15.3%) were associated with Mycoplasma pneumoniae and respiratory infections.
2.13. Diagnostic Accuracy of Biomarkers
No studies included reported adhering to the Standards for Reporting Diagnostic accuracy studies (STARD) guidelines [63]. Within the included 36 studies, 12 (12/36; 33.3%) studies included sensitivity and specificity metrics for their biomarkers. The summary of diagnostic accuracy metrics can be found in Table 7. Articles reporting diagnostic accuracy were mostly published in 2021 (4/12; 33.3%). However, studies reporting metrics have been published between 2012 and 2025. Of the studies reporting, nine also included an area under the curve value (9/12; 75%), and six studies reported cut-off values for their biomarkers (6/12; 50%). Reporting diagnostic accuracy characteristics such as sensitivity and specificity did not equate to reporting all diagnostic accuracy metrics. None of the included studies reported positive or negative predictive values for their biomarkers. The miRNA biomarker range in sensitivity across these 12 studies was from 70% to 100%, and the specificity ranged from 72% to 100%. The range for the area under the curve across the nine studies reporting the value was 0.62 to 0.99.
3. Discussion
The studies relating to paediatric infection included within this scoping review were conducted between 2012 and 2025, with most published between 2021 and 2023. This reflects that miRNA research remains in its infancy following its discovery in C. elegans in the early 1990s [64]. Due to the infancy of miRNA research, it remains a highly specialised field with minimal miRNA biomarker research for paediatric infection. Interestingly, the studies included were primarily conducted in Asia (72.2%), with the majority originating in China (55.6%). The remaining studies were conducted in the United States (22.2%) or Europe (8.3%). This may reflect the funding priorities of different regions, namely the China Precision Medicine Initiative, which was launched in 2015 [65], that may have supported miRNA biomarker discovery in paediatric infection.
The risk of serious bacterial infections varies with age, and the included articles were well distributed across all paediatric age ranges with relatively even numbers of articles relating to neonatal, infant, and toddler studies (ranging between 19.4% to 25%). There was a slight increase in publications relating to older children (30.6%). This relatively balanced distribution of ages across publications is encouraging, as each age group encounters unique physiological challenges that influence both their susceptibility to infection and potentially their miRNA response to infection. Unfortunately, none of the studies comprised cohorts that spanned all the age ranges, which removes the opportunity to assess the influences of age and infection types on alterations in miRNA biomarkers.
The studies included within this review were primarily conducted with paediatric inpatients (97%). This is likely to have proven an easy first step in miRNA discovery. The issue with this approach is that the results may not reflect the clinical setting where they are intended for use. The next phase of miRNA research needs to focus on different populations such as including emergency presentations or sequential monitoring of specific cohorts of sick children. The generalisability of the results was often confounded further as only 19.4% of the studies investigated multiple sources of infection/undifferentiated illness. The majority of the studies investigated specific confirmed infections compared to healthy controls (66.7%). The case–control designs make the discovery of differentially expressed miRNA more achievable but risk identifying non-specific immune activation markers. Future research needs to assess which miRNAs are differentially expressed compared to different infectious populations with the use of febrile controls as opposed to healthy controls.
In addition to variations in the populations and settings, the methodologies employed were diverse and non-standardised across the 36 studies. RT-qPCR investigation was used by 75% of the studies, followed by microarray for 27.7%, and next-generation sequencing for 22.2%. Techniques such as PCR and microarray are typically closed or moderately open hypothesis approaches, limiting the discovery of novel biomarkers. Fortunately, the financial barriers to next-generation sequencing are decreasing [18], which could drive more widespread adoption of this methodology in future research. Paediatric-specific protocols for next-generation sequencing are also being developed [66], which may increase the productivity of miRNA biomarker discovery for children. For all types of miRNA investigation, samples must first have their total RNA extracted. Unfortunately, there is no consensus on the optimal methodology for RNA extraction from different biofluids. The subsequent results from the studies are therefore difficult to compare as each RNA extraction kit will hold its own biases, significantly altering the miRNA profiles extracted [67,68]. The most common sample types were serum, nasal and throat swabs, saliva, and plasma, making up 77.8% of the sample types investigated. Studies investigating circulating miRNA were relatively even between serum and plasma samples (27.8% and 27.3%, respectively), and there were fewer whole blood studies (16.7%). Although plasma and serum are the preferred sample type choice for circulating miRNA discovery, serum can contain an altered miRNA profile to plasma due to the clotting process releasing miRNA from platelets [69]. However, the miRNA content of plasma can also be altered due to different processing times post-phlebotomy [69]. The consensus is that both plasma and serum are suitable for circulating miRNA studies, but results should not be directly compared [69]. Generally, whole blood is avoided in circulating miRNA biomarker discovery because its cellular material is rich in miRNA, which can interfere with the overall miRNA profiles detected [67].
A further challenge with miRNA acellular biofluid investigations is the lack of standardised normalisation miRNA for PCR techniques [70]. This contrasts with working with cellular samples, for which consistent housekeeping genes can be relied upon for normalisation [71]. A total of 54.8% of the studies reported using non-miRNA references, of which U6 accounted for 45.2%. Those included were small nucleolar RNAs (snoRNAs), RNU24, RNU43, and RNU6B (U6), which are considered poor candidates for normalisation due to disease-specific dysregulation [72], and their lack of stability in biofluids [73]. Additionally, miRNAs (18–25 nucleotides) are much smaller than snoRNAs (60–300 nucleotides), leading to differences in extraction efficiency, as methods often favour smaller RNAs. Therefore, miRNA normalisation markers should be preferred over non-miRNA molecules. The impacts of using snoRNAs as normalisation markers within these studies significantly reduces the reliability of the results and their interpretation. Spike-in RNA of a similar nucleotide length to endogenous miRNAs was used for normalisation in 16.1% of the studies. This method reduces variation more effectively than snoRNAs but does not account for differences in sample handling or processing. This may therefore introduce non-biological differences between the samples and significantly impact the data interpretation [74]. Global mean normalisation, used in 12.9% of studies, helps address issues with non-endogenous molecules by averaging endogenous miRNA across samples. However, it may over-normalise low expression samples, potentially masking true biological differences. Therefore, the best approach is to identify cohort-specific endogenous miRNA within the specific experimental samples. Within the included studies, 19.4% reported the use of endogenous miRNA; however, they did not report the assessment of the stability of their chosen normaliser within their specific cohorts.
In the context of clinical diagnostics, there is a critical need for rapid, streamlined workflows that can be readily automated to accommodate high-throughput demands. Given that approximately 75% of miRNA biomarker discovery studies to date have employed RT-qPCR, one viable route for clinical translation is the development of algorithm-based approaches. RT-qPCR can be implemented within existing clinical laboratory infrastructure, with raw Ct values subsequently normalised using either a validated endogenous reference miRNA or an exogenous spike-in control of a similar length. This normalisation enables consistent quantification across samples and facilitates the simultaneous detection of miRNA panels, with the normalised values serving as inputs to a diagnostic algorithm. The algorithm can then generate a single composite risk score, offering a clinically interpretable output to support diagnostic decision-making. Like RT-qPCR, digital PCR (dPCR) would still require a diagnostic algorithm to interpret miRNA expression levels. However, dPCR offers key advantages, including absolute quantification without the need for reference genes or standard curves, and greater precision at low input levels [75], making it especially suitable for plasma-derived miRNAs from paediatric samples. By partitioning reactions into thousands of nanolitre-sized compartments, dPCR enables direct molecule counting, reducing technical variability and improving reproducibility across laboratories [76]. It can also support multiplexed detection of miRNA panels [75], which is essential for clinical diagnostics. Adoption is currently limited by higher costs, driven by specialised equipment, proprietary reagents, and lower throughput, but as platforms become more accessible, dPCR holds strong potential for enhancing the standardisation, sensitivity, and clinical utility of miRNA-based diagnostics.
Novel miRNAs demonstrate clear potential as diagnostic biomarkers but current evidence regarding diagnostic test accuracy is lacking. Only 12 (33.3%) studies reported sensitivity and specificity data on their novel biomarkers. Within these studies, nine (83.3%) studies reported an area under the curve value and a separate six (50%) reported cut-off values for their biomarkers. None of the studies included within the review reported positive or negative predictive values. The lack of diagnostic metrics reported may unintentionally exaggerate the novel biomarkers’ clinical potential and substantially limit the understanding of the marker’s discriminatory power. These issues are reflected in that none of the 12 studies reported test accuracy in compliance with STARD guidance [63]. To improve consistency and comparability, future research must standardise approaches to population sampling, biological fluid handling, and the reporting of outcomes. All miRNA biomarker research outputs should aim to include full reporting of sensitivity, specificity, area under the curve, and positive and negative predictive values. This should also include an agreement of reference standards, and the inclusion of comparator biomarkers such as CRP and PCT. Additionally, researchers may benefit from using the Biomarker Toolkit [17], which is designed to support successful biomarker translation, and acts as a framework to improve study design and strengthen outcomes.
There were 16 miRNAs that were identified more than once across the studies, with the most commonly identified being hsa-miR-155 (6/36; 16.7%), hsa-miR-29 (5/36; 11.1%), hsa-miR-206 (/36; 11.1%), hsa-miR-142-3p (3/36; 8.3%), hsa-miR-182-5p (3/36; 8.3%), and hsa-miR-363-3p (3/36; 8.3%). There was an imbalance between bacterial- and viral-associated miRNA validations; however, this is likely to do with more studies relating directly to acute viral infection in children. There were three validated bacterial-associated miRNAs: hsa-miR-182-5p, hsa-miR-363-3p, and hsa-miR-206. There were nine validated viral-associated miRNAs: hsa-miR-155, hsa-miR-29, hsa-miR-155-5p, hsa-miR-150-5p, hsa-miR-140-3p, hsa-miR-142-3p, hsa-miR-149-3p, hsa-miR-210-3p, and hsa-miR-34a-5p. There were four miRNAs that were validated across all miRNAs identified, but not in the distinct bacterial and viral categories: hsa-miR-101-3p, hsa-miR-142-5p, hsa-miR-183-5p, and hsa-miR-486-3p. These miRNAs replicated across multiple studies, regardless of infection category, are more likely to represent non-specific infection markers. Conversely, miRNAs associated exclusively with acute bacterial or viral infections are more likely to be of clinical interest.
4. Materials and Methods
4.1. Protocol
The review adhered to the PRISMA-ScR guidelines [77] and followed the published protocol [78], which can be found at MedRxiv doi: https://doi.org/10.1101/2025.04.11.25325664.
4.2. Eligibility Criteria
The study included published prospective and retrospective cohort studies reporting host miRNA associated with bacterial and viral infections in English. Children aged between 0 and 18 years were included in the analysis. Studies reporting miRNAs in comparison to healthy controls, infection states compared to other infection states, or individuals of different degrees of infection were included. The inclusion and exclusion criteria are shown in Table 8.
4.3. Information Sources
The databases searched include Medline All and Web of Science, alongside searching for grey literature including Google, Google Scholar, and open Theses. The date the searches were completed was 19 May 2025. All screened articles were written in English. The search strategy is provided in Supplementary File S1.
4.4. Selection of Sources of Evidence
The citations identified in the searches were uploaded into Rayyan [79], a screening and data extraction tool for undertaking systematic or scoping reviews. Two reviewers (OR and ADB) screened titles and abstracts, while one reviewer (OR) screened the selected articles for full-text review.
4.5. Data Charting Process and Data Items
Following full-text review, the included studies’ data was extracted into an Excel spreadsheet. The following items were extracted: title, year of publication, authors, DOI, date of publication, country of study, population (e.g., children with fever), setting (e.g., emergency department, UK), clinical question (e.g., bacterial vs. viral), main study methods, Next-Generation Sequencing kit, RNA extraction kit, normalisation, ages of patients, % female, total sample size, sample size study focus, sample size comparator, bacterial numbers and infections, viral numbers and infections, inclusion of CRP/PCT, reference standard, conditions of statistics, biomarkers, biomarker sensitivity %, biomarker specificity %, AUC, positive predictive value, negative predictive value, biomarker cut-off value, sample type, and sample volume.
4.6. Synthesis of Results
The data were synthesised descriptively, with findings presented as percentages of the total number of included studies. In some cases, with studies reporting a specific metric, the reported ranges of specific metrics were also reported. Studies were grouped according to key variables such as infection type (bacterial or viral), methodology, miRNA biomarkers, or diagnostic metric.
5. Conclusions
This scoping review highlights that miRNA research in paediatric infection is a novel and developing field. Children exhibit a diverse range of developing physiologies and therefore it is expected that their miRNA biomarkers may change with age. The evenly distributed age groups across the included studies suggest that no group has been disproportionately emphasised or overlooked. The research to date has focused on hospitalised children and most of the studies have focused on specific infections rather than undifferentiated febrile illness. None of the studies reported test accuracy metrics in accordance with STARD guidance and there is a lack of standardisation for how miRNA test accuracy is reported. The primary miRNA detection methodology was PCR, followed by microarray, and then next-generation sequencing. The normalisation techniques in the studies were also generally poor, with many using the small nuclear RNA U6, which is unstable in biofluid samples.
Overall, 17 miRNAs across the 36 studies included within the review were validated more than twice. Three miRNA, hsa-miR-182-5p, hsa-miR-363-3p, and hsa-miR-206, were validated to be associated with bacterial infection in children. Nine miRNAs, hsa-miR-155, hsa-miR-29a-3p, hsa-miR-155-5p, hsa-miR-150-5p, hsa-miR-140-3p, hsa-miR-142-3p, hsa-miR-149-3p, hsa-miR-210-3p, and hsa-miR-34a-5p, were validated to be associated with viral infection. A further six miRNAs, hsa-miR-101-3p, hsa-miR-142-5p, hsa-miR-182-5p, hsa-miR-183-5p, hsa-miR-363-3p, and hsa-miR-486-3p, were validated regardless of infection category but are assumed to most likely be general immune activation biomarkers. Across the 12 studies reporting diagnostic accuracy metrics, miRNA biomarkers exhibited a sensitivity ranging from 70% to 100%, and a specificity ranging from 72% to 100%. The area under the curve across the studies demonstrated a range from 0.62 to 0.99. This strongly suggests that miRNA biomarker discovery, with more rigorous study design, could have good potential for paediatric infection diagnostics in the future. However, due to the lack of adherence to the STARD guidelines and the large heterogeneity between the included studies, no clinically meaningful conclusions can be made at this time.
6. Research Gaps
From the synthesis of results generated within this scoping review, there are some research gaps within the field of paediatric infection diagnostics utilising miRNA targets. Firstly, there is a global incentive to increase research outputs on paediatric miRNA during acute infection. Although there is a growing interest in the field, the literature is still scarce, and the general knowledge of miRNA during infection and health of children is poorly understood. Most of the studies within this review have been conducted in Asia; there was also eight studies in the United States, and only three studies were conducted in Europe. It is possible that miRNA signatures may differ depending on the race of the child, and this should be more extensively explored to encompass all races of children to reduce bias. This review also highlights that while the included studies collectively cover all age groups relatively evenly, individual studies do not encompass the full age ranges present in paediatrics. This may limit the understanding of whether the identified miRNAs of interest are influenced by age.
With the accessibility of next-generation sequencing increasing for researchers, there should also be a focus on miRNA discovery via open hypothesis methods rather than moderately closed or closed hypothesis. This removal of pre-defined assumptions by focusing on next-generation sequencing will likely result in the discovery of more novel potential candidates with reduced bias. If next-generation sequencing is also prioritised, the identification of cohort-specific normalisation markers can also be enhanced, ensuring that the best possible normalisation can occur for biofluid samples. Following rigorous biomarker discovery, it is crucial that researchers also prioritise the validation of promising candidates. Currently, biomarker research is marked by an oversaturation of discovery efforts, with few candidates reaching clinical application, often due to flawed study designs and insufficient follow-up validation. Future research should include the development of standardised protocols tailored to specific sample types, including RNA extraction, sequencing, and PCR analysis. Such standardisation would enhance comparability across studies and increase the likelihood of successful clinical translation.
Given the global health priority of improving antimicrobial stewardship, there is a clear need for increased research into bacterial infection-specific biomarkers in children. Future studies should encompass a broad range of bacterial infections rather than focusing on individual pathogens. Such an approach would provide greater confidence that an miRNA-based point-of-care test could offer clinicians valuable guidance on antibiotic treatment decisions. Included within these improved study designs should be a more standardised methodology for reference standard choices, where there are clear definitions of infection, based on clinical and laboratory data. Finally, significant efforts should be made to include fully expansive diagnostic accuracy testing of the novel biomarkers, adhering to the STARD guidelines, and their comparisons to current testing biomarkers. Without this, there will be no progression of these novel biomarkers towards clinical use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hagedoorn N.N. Borensztajn D.M. Nijman R. Balode A. von Both U. Carrol E.D. Eleftheriou I. Emonts E. van der Flier M. de Groot R. Variation in antibiotic prescription rates in febrile children presenting to emergency departments across Europe (MOFICHE): A multicentre observational study P Lo S Med.202017 e 1003208 Available online: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003208(accessed on 14 March 2025)10.1371/journal.pmed.100320832813708 PMC 7444592 · doi ↗ · pubmed ↗
- 2van de Maat J. van de Voort E. Mintegi S. Gervaix A. Nieboer D. Moll H. Oostenbrink R. Antibiotic prescription for febrile children in European emergency departments: A cross-sectional, observational study Lancet Infect. Dis.201919382391 Available online: https://www.thelancet.com/action/show Full Text?pii=S 1473309918306728(accessed on 14 March 2025)10.1016/S 1473-3099(18)30672-830827808 · doi ↗ · pubmed ↗
- 3Hersh A.L. Shapiro D.J. Pavia A.T. Shah S.S. Antibiotic Prescribing in Ambulatory Pediatrics in the United States Pediatrics 201112810531061 Available online: https://pubmed.ncbi.nlm.nih.gov/22065263/(accessed on 14 March 2025)10.1542/peds.2011-133722065263 · doi ↗ · pubmed ↗
- 4Klein E.Y. Impalli I. Poleon S. Denoel P. Cipriano M. Van Boeckel T.P. Pecetta S. Bloom D. Nandi A. Global trends in antibiotic consumption during 2016-2023 and future projections through 2030 Proc. Natl. Acad. Sci. USA 2024121 e 2411919121 Available online: https://www.pnas.org/doi/abs/10.1073/pnas.2411919121(accessed on 14 March 2025)10.1073/pnas.241191912139556760 PMC 11626136 · doi ↗ · pubmed ↗
- 5Naghavi M. Vollset S.E. Ikuta K.S. Swetschinski L.R. Gray A.P. Wool E.E. Aguilar G. Mestrovic T. Smith G. Han C. Global burden of bacterial antimicrobial resistance 1990–2021: A systematic analysis with forecasts to 2050 Lancet 202440411991226 Available online: https://www.thelancet.com/action/show Full Text?pii=S 0140673624018671(accessed on 14 March 2025)10.1016/S 0140-6736(24)01867-139299261 PMC 11718157 · doi ↗ · pubmed ↗
- 6Costelloe C. Metcalfe C. Lovering A. Mant D. Hay A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis BMJ 2010340 c 2096 Available online: https://www-bmj-com.qub.idm.oclc.org/content/340/bmj.c 2096(accessed on 14 March 2025)10.1136/bmj.c 209620483949 · doi ↗ · pubmed ↗
- 7Rentschler S. Kaiser L. Deigner H.P. Emerging Options for the Diagnosis of Bacterial Infections and the Characterization of Antimicrobial Resistance Int. J. Mol. Sci.202122456 Available online: https://www.mdpi.com/1422-0067/22/1/456/htm(accessed on 14 March 2025)10.3390/ijms 2201045633466437 PMC 7796476 · doi ↗ · pubmed ↗
- 8Shah P. Voice M. Calvo-Bado L. Rivero-Calle I. Morris S. Nijman R. Brodericka C. Dea T. Eleftherioue I. Galassini R. Relationship between molecular pathogen detection and clinical disease in febrile children across Europe: A multicentre, prospective observational study Lancet Reg. Health Eur.202332100682 Available online: https://www.thelancet.com/action/show Full Text?pii=S 2666776223001011(accessed on 14 March 2025)10.1016/j.lanepe.2023.10068237554664 PMC 10405323 · doi ↗ · pubmed ↗