Vascular Graft Infections Due to Listeria spp.: A Comprehensive Review of the Literature
Tommaso Lupia, Marco Casarotto, Gianfranco Fonte, Saverio Marena, Francesca Paola Giunta, Fabrizio Buffolo, Silvia Corcione, Francesco Giuseppe De Rosa

TL;DR
This paper reviews rare but serious Listeria infections in vascular grafts, summarizing patient data, diagnostic methods, and treatment approaches.
Contribution
The study provides a comprehensive review of Listeria vascular graft infections and evaluates novel antibiotics for treatment.
Findings
Most Listeria vascular graft infections occurred in abdominal aortic grafts with a median delay of 28 months post-implantation.
Ampicillin combined with aminoglycosides was the primary treatment, with low mortality and no recurrence reported.
Computed tomography and positron emission tomography CT were key diagnostic tools for these infections.
Abstract
Vascular graft infections are rare but serious complications of vascular surgery. Listeria monocytogenes represents an exceedingly rare yet potentially life-threatening cause. We present a narrative review according to the Scale for the Assessment of Narrative Review Articles (SANRA) criteria, summarizing the existing literature regarding Listeria vascular graft infections. Moreover, we have revised novel potential antibiotics against Listeria spp. A systematic search identified 23 studies involving 39 patients. Most infections affected abdominal aortic grafts (50%), with a median interval of 28 months from graft implantation to infection. Common comorbidities included hypertension (30.8%) and diabetes (18%), with 24% of patients being immunocompromised. Diagnosis was supported by blood cultures (45%) and imaging, particularly computed tomography (CT, 90%) and positron emission…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
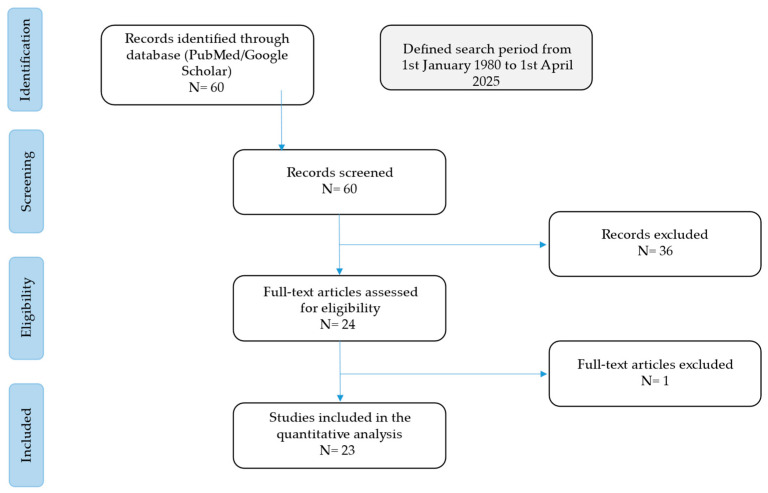 Figure 1
Figure 1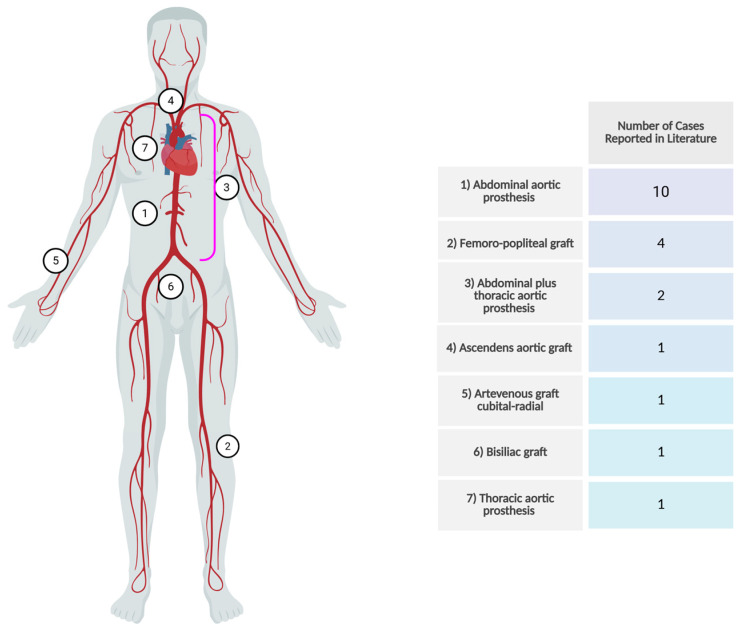 Figure 2
Figure 2| Author | Year | Type of Study | Patients | Sex | Age | Type of Graft | Other Seedings | Time from Prosthesis Implantation | |
|---|---|---|---|---|---|---|---|---|---|
| Rohde et al. [ | 2004 | Case Report | 1 | M | 51 | Ascendens Aortic prosthesis | No | 6 months | |
| Miranda et al. [ | 2022 | Case Report | 1 | M | 72 | Abdominal Aortic prosthesis | No | 9 years | |
| Ahadzada et al. [ | 2021 | Case Report | 1 | M | 80 | Abdominal Aortic prosthesis | No | 7 months | |
| Berchiolli et al. [ | 2022 | Case Report | 1 | M | 72 | Abdominal Aortic prosthesis | No | 3 years | |
| Lauk et al. [ | 2020 | Case Report | 1 | M | 70 | Thoracic and abdominal Aortic prosthesis | No | 5 years | |
| Chavada et al. [ | 2014 | Case Series | 1 | M | 83 | Femoro-popliteal graft | No | 2 years | |
| Ma et al. [ | 2019 | Case Report | 1 | M | 66 | Abdominal Aortic prosthesis | Psoas abscess | 18 months | |
| Tanner-Steinmann et al. [ | 2011 | Case Report | 1 | M | 59 | Abdominal Aortic prosthesis | No | 2 years | |
| Saleem et al. [ | 2008 | Case Report | 1 | M | 67 | Abdominal Aortic prosthesis | No | 10 months | |
| Foulex et al. [ | 2019 | Case Report | 1 | M | 76 | Abdominal Aortic prosthesis | No | NA | |
| Heikkinen et al. [ | 1999 | Case Report | 1 | M | 77 | Abdominal Aortic prosthesis | No | 3 months | |
| Silvestri et al. [ | 2017 | Case Report | 1 | M | 72 | Thoracic and abdominal Aortic prosthesis | No | 7 years | |
| Mercurio et al. [ | 2021 | Case Report | 1 | M | 83 | Abdominal Aortic prosthesis | Spondylodiscitis | 1 months | |
| Zardi et al. [ | 2022 | Case Report | 1 | M | 71 | Aorto-bi-iliac endograft | No | 2 months | |
| Gauto et al. [ | 1992 | Case Series | 1 | M | 59 | Femoro-popliteal graft | Endocarditis | 1 year | |
| De Nietet al. [ | 2018 | Case report | 1 | M | 81 | Abdominal Aortic prosthesis | No | 5 years | |
| Zeitlin et al. [ | 1982 | Case report | 1 | F | 51 | Arteriovenous graft radial artery | No | 5 months | |
| Van Noyen et al. [ | 1993 | Case report | 1 | M | 75 | Femoro-popliteal bypass | No | 3 years | |
| Heysell et al. [ | 2015 | Case report | 1 | F | 68 | Thoracic Aortic prosthesis | No | 2 years | |
| Walker et al. [ | 2015 | Case report | 1 | M | 70 | Femoro-popliteal graft | No | 1 year | |
|
|
|
|
|
|
|
| |||
| Rohde et al. [ | Arterial hypertension, hyperlipoproteinemia | NA | Yes (bacteriemia 7 |
| No | S penicillin, gentamicin, | |||
| Miranda et al. [ | NA | NA | No | Negative | No | Not reported | |||
| Ahadzada et al. [ | Arterial hypertension, hyperlipoproteinemia, CAD | NA | Not confirmed (non-bloody | Negative | No | Not reported | |||
| Berchiolli et al. [ | Arterial hypertension, DM, CAD | NA | No |
| No | Not reported | |||
| Lauk et al. [ | CAD | NA | No | Negative | Yes | Not reported | |||
| Chavada et al. [ | Atrial fibrillation | Undercooked meat | No | Not performed | No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Ma et al. [ | Arterial hypertension | NA | Not confirmed (abdominal pain and fever 4 weeks before admission) |
| No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Tanner-Steinmann et al. [ | Kidney transplant | NA | Not confirmed (non-bloody diarrhea 8 weeks before admission) | Negative | No | Not reported | |||
| Saleem et al. [ | COPD, DM, CAD | Livestock farmer | No | Negative | No | Not reported | |||
| Foulex et al. [ | COPD, DM, CAD | NA | Not confirmed (non-bloody diarrhea 10 days before admission) | Negative | Yes | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Heikkinen et al. [ | Obesity, arterial hypertension | NA | No | Negative | No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Silvestri et al. [ | Giant cell arteritis, DM, arterial hypertension | NA | Not confirmed (abdominal pain and fever 8 weeks before admission) |
| No | Not reported | |||
| Mercurio et al. [ | DM, arterial hypertension, PM | NA | No |
| No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Zardi et al. [ | DM, arterial hypertension, splenectomy | NA | No | Negative | No | Not reported | |||
| Gauto et al. [ | Rheumatoid arthritis, CAD, arterial hypertension | NA | No |
| No | Not reported | |||
| De Nietet al. [ | Arterial hypertension | NA | No | Negative | No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Zeitlin et al. [ | DM, arterial hypertension, CKD | NA | No |
| No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Van Noyen et al. [ | Arterial hypertension, COPD | NA | No | Not performed | No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Heysell et al. [ | Idiopathic cardiomyopathy, AF | Unpasteurized dairy | Not confirmed (diarrhea 3 months before admission) |
| No | S penicillin, gentamicin, trimethoprim-sulfamethoxazole | |||
| Walker et al. [ | NA | NA | No |
| Yes | Not reported | |||
|
|
|
|
|
|
|
| |||
| Rohde et al. [ | No | No | Yes | No | Yes | No | |||
| Miranda et al. [ | No | Positive | Yes | No | No | No | |||
| Ahadzada et al. [ | No | No | Yes | No | Yes | No | |||
| Berchiolli et al. [ | No | Positive | Yes | No | Yes | No | |||
| Lauk et al. [ | No | No | Yes | No | No | No | |||
| Chavada et al. [ | No | Positive | Yes | No | No | No | |||
| Ma et al. [ | Negative | No | Yes | No | No | Yes | |||
| Tanner-Steinmann et al. [ | No | No | Yes | Yes | No | Yes | |||
| Saleem et al. [ | No | No | Yes | No | Yes | Yes | |||
| Foulex et al. [ | Negative | Positive | Yes | No | Yes | Yes | |||
| Heikkinen et al. [ | No | Positive | Yes | No | No | Yes | |||
| Silvestri et al. [ | NA | NA | NA | NA | NA | NA | |||
| Mercurio et al. [ | No | No | Yes | Yes | Yes | No | |||
| Zardi et al. [ | No | Positive | Yes | No | No | No | |||
| Gauto et al. [ | No | No | Yes | No | No | No | |||
| De Nietet al. [ | No | No | Yes | No | Yes | No | |||
| Zeitlin et al. [ | No | No | No | No | No | No | |||
| Van Noyen et al. [ | No | Positive | Yes | No | No | Yes | |||
| Heysell et al. [ | No | No | Yes | No | No | Yes | |||
| Walker et al. [ | No | Negative | Yes | No | No | Yes | |||
| Author | Percutaneous Drainage | Surgery | Treatment | Duration | SAT (Lifelong) or | Recurrence | Outcome |
|---|---|---|---|---|---|---|---|
| Rohde et al. [ | No | No | ampicillin (6 weeks) + gentamicin (4 weeks) followed by amoxicillin (8 weeks) | 109 days | No | No | 12 months FU |
| Miranda et al. [ | No | Yes | ampicillin + gentamicin | 28 days | SAT amoxicillin | No | 6 months FU |
| Ahadzada et al. [ | Yes | No | IV benzylpenicillin | 48 days | SAT amoxicillin | No | 10 months FU |
| Berchiolli et al. [ | Yes | Yes | ampicillin-sulbactam | Not reported | Not reported | No | 3 months FU |
| Lauk et al. [ | Yes | No | meropenem + vancomycin (1 week) followed by amoxicillin + gentamicin (21 days) | 29 days | SAT piperacillin-tazobactam | No | 24 months FU |
| Chavada et al. [ | No | Yes | ampicillin (1 week) followed by meropenem (5 weeks) | 42 days | Consolidation amoxicillin 6 months | No | 6 months FU |
| Ma et al. [ | No | No | ampicillin (4 weeks) + gentamicin for 8 weeks followed by trimetoprim-sulfametoxazole IV for 12 days | 42 days | Consolidation trimetoprim-sulfametoxazole 13.5 months | No | 20 months FU |
| Tanner-Steinmann et al. [ | Yes | Yes | ampicillin (4 weeks) followed by ampicillin + gentamicin (4 week) | 42 days | Consolidation trimetoprim-sulfametoxazole 24 months | No | 30 months FU |
| Saleem et al. [ | Yes | No | amoxicillin-clavulanic + trimetoprim-sulfametoxazole | 28 days | Consolidation trimetoprim-sulfametoxazole 6 months | No | 12 months FU |
| Foulex et al. [ | No | Yes | amoxicillin | 42 days | No | No | 6 months FU |
| Heikkinen et al. [ | Yes | Yes | ampicillin + netilmicin (2 weeks) followed by doxycycline (4 weeks) | 42 days | No | No | 10 months FU |
| Silvestri et al. [ | NA | NA | NA | NA | Not described | No | NA |
| Mercurio et al. [ | Yes | No | ampicillin + gentamicin (2 weeks) followed by ampicillin (4 weeks) | 42 days | No | No | 12 months FU |
| Zardi et al. [ | No | Yes | meropenem + vancomycin (3 weeks) followed byclaritromicine (12 weeks) | 105 days | No | No | 9 months FU |
| Gauto et al. [ | No | No | ampicillin + trimetoprim-sulfametoxazole | 56 days | No | No | 18 months FU |
| De Niet et al. [ | Yes | Yes | amoxicillin | 28 days | SAT trimetoprim-sulfametoxazole | No | 6 months FU |
| Zeitlin et al. [ | No | Yes | vancomycin | 42 days | No | No | 9 months FU |
| Van Noyen et al. [ | No | Yes | amoxicillin-clavulanic acid + gentamicin | NA | Not described | Death | |
| Heysell et al. [ | No | No | vancomycin | 42 days | SAT doxicycline | No | 36 months FU |
| Walker et al. [ | No | Yes | Not described | NA | Not described | No | Not reported |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Vascular Procedures and Complications · Central Venous Catheters and Hemodialysis
1. Introduction
Infection of a vascular graft prosthesis is a rare, although serious, complication of vascular surgery. The overall infection rate is around 2%, varying between 1% and 6% among different types of grafts [1]. Numerous factors appear to contribute, including emergency procedures, demographic characteristics, and various underlying comorbidities [1]. Over the years, causative agents have diversified; current papers indicate that coagulase-negative Staphylococci (CoNS) represent around 42% of cases, followed by Staphylococcus aureus at 29% [2]. Other bacteria, such as Listeria monocytogenes, are rare. Listeria spp. is a facultative anaerobic, Gram-positive bacillus that proliferates on blood agar and exhibits partial β-hemolysis [2]. There are seven recognized species of Listeria, although L. monocytogenes is the predominant source of human illnesses [2,3]. It often impacts pregnant women, infants, older adults, and the immunocompromised population [2,3]. This vulnerability can be somewhat elucidated by the dual nature of the response to this infection, which encompasses both innate and adaptive immunity, heavily dependent on macrophage activation through T-cell lymphokines [4]. L. monocytogenes is prevalent in nature, particularly among the fecal flora of animals, and is a significant contributor to zoonotic diseases, with a case-fatality rate that may attain 20% [2]. Listeriosis, excluding perinatal instances, is predominantly foodborne. Numerous foods have been recognized as vectors of illness, including milk, soft cheese, ready-to-eat pork products, hot dogs, and delicatessen turkey, among others [5,6,7]. Other uncommon mechanisms of transmission have been documented, including maternal–fetal transmission through the placenta, exposure during parturition, or direct contact with aborted calves and infected poultry, which is mainly reported among agricultural workers and veterinarians [2,3]. In susceptible people, listeriosis may manifest in three different clinical presentations: bacteremia (with or without septic shock); central nervous system involvement, commonly meningitis or meningoencephalitis; or pregnancy-associated and neonatal listeriosis; which account, respectively, for 31%, 52%, and 14% of the cases reported in the literature [2]. Moreover, in otherwise healthy persons, it often results in self-limiting febrile gastroenteritis [1,2]. Grif and colleagues have recorded the temporary presence of L. monocytogenes in the feces of healthy persons [8].
Uncommon infections have been reported affecting the skin (e.g., pyogranulomatous rash), peritoneal cavity, arthroskeletal tissue, lungs and pleural cavity, cardiovascular system, urinary tract, biliary tract, and the eye, each generally representing fewer than 1% of the overall listeriosis cases [2,9,10,11,12]. In 2010, the global burden of the illness comprised 23,150 cases, 5463 fatalities, and 172,823 disability-adjusted life years [2].
Few studies have documented vascular prosthesis infections caused by L. monocytogenes [13,14,15], and even fewer studies have addressed the involvement of endovascular prostheses. This paper aims to present a comprehensive review of the literature of vascular prosthesis infection caused by L. monocytogenes. Moreover, we have revised the literature regarding novel antibiotics available against this bacterium.
2. Methods
The current narrative review followed the Scale for the Assessment of Narrative Review Articles (SANRA) flow-chart (Figure 1) [16].
The main aim of this work is to summarize current evidence on vascular graft infections due to Listeria spp., focusing on clinical presentations, management, and outcomes.
A search was run on Google Scholar and PubMed using the terms (“Listeria monocytogenes” OR “Listeriosis” OR “Listeria”) AND (“Aortic Diseases” OR “Aortic Aneurysm” OR “Aortic Graft Infection” OR “Vascular Graft Infection” OR “Graft Infection” OR “Prosthetic Infection” OR “Endograft Infection”). Results were limited to papers published between 1 January 1980 and 1 April 2025. Studies were filtered for practice guidelines, guidelines, meta-analyses, systematic reviews, narrative reviews, case series, and case reports. The results were filtered to include only humans, and patients over 18 years old.
Our search strategy permitted the identification of 60 papers, of which 36 were excluded by title and abstract evaluation. Then, the reviewers studied titles and abstracts. Subsequently, 24 papers were included. One paper was excluded because it was not possible to find the full text. Finally, a quality assessment of full-text studies was performed by two independent reviewers (MC and TL). The researchers reviewed the summary of all articles and ultimately used data from full articles to compile this review paper. The researchers assessed the inclusion of all titles and abstracts without language limitations in English. We duplicated other studies previously included and excluded papers with no methods described, along with papers not strictly related to the aim of the study.
Moreover, we have revised the literature regarding new antibiotic molecules with an activity in vitro or in vivo against Listeria spp.
We performed descriptive statistics on the entire study population. Data were analyzed using standard statistical methods. Variables were described with medians, absolute values, and rates. Three studies were discussed separately from the others because they included both endovascular graft and non-graft infections.
3. Results
The final analysis comprised 23 papers with a total of 39 participants. We identified 18 case reports and two case series, encompassing a total of 20 patients, as presented in Table 1. Additionally, three publications were retrospective studies involving 19 patients, and their findings are elaborated upon in a specific paragraph.
The median age was 70 years (range 51–83), with a predominance of males (N = 18; 90%). Two studies did not report patient comorbidities; nevertheless, among the others, the most prevalent condition was arterial hypertension (N = 12; 30.8%), followed by diabetes mellitus (DM) in seven instances (18%), whereas coronary artery disease was noted in five individuals (25%). Three individuals (15%) had a diagnosis of COPD in their medical history. Notably, four patients (24%) were immunocompromised for various reasons: one was a kidney transplant recipient, one was on steroid treatment for giant cell arteritis, one was on drugs for rheumatoid arthritis, and one had undergone a splenectomy some years prior to the infection. The majority of infections were associated with abdominal aortic grafts (N = 10; 50%), followed by femoro-popliteal grafts (N = 4; 20%) and thoracic aortic grafts (N = 2; 10%). Other types of less common vascular prostheses involvement are depicted in Figure 2.
The duration from implant to graft infection exhibited considerable variability, with a median of 28 months (range 1 month to 9 years). Only three patients (15%) reported traditional risk factors for listeriosis, such as the consumption of undercooked meat, employment as a livestock farmer, and the intake of unpasteurized dairy products. Only one patient had confirmed bacteremia caused by L. monocytogenes seven weeks prior to the detection of transplant infection. Six patients (30%) had symptoms (i.e., non-bloody diarrhea, fever, or stomach discomfort) indicative of Listeria spp. infection in the three months before admission. Nine (45%) had positive blood cultures, consistently for L. monocytogenes. In seven cases, graft cultures validated the diagnosis by yielding growth of L. monocytogenes. A CT scan with contrast was conducted in 18 instances (90%), whilst MRI was utilized for certain occurrences. A PET scan was conducted in seven instances (35%).
Three instances of infection seeding were documented, specifically, one case of endocarditis, one case of psoas abscess, and one case of spondylodiscitis. Antimicrobial susceptibility was reported in 10 individuals (50%), with all isolates demonstrating susceptibility to penicillin, aminoglycosides, and trimethoprim-sulfamethoxazole.
In terms of treatment, 11 patients (55%) had surgical intervention and source control, whereas 9 patients (45%) were managed solely by medical therapy. ßeta-lactam constituted the most recommended antibiotic class for first-line therapy, with IV ampicillin administered in eight instances (40%), followed by IV amoxicillin or amoxicillin-clavulanate (N = 4; 20%), as reported in Table 2.
Combination treatment was administered in 10 instances (50%), with IV gentamicin being the most used adjunct antibiotic (N = 6; 30%). The median duration of first-line treatment was 51 days (ranging from 28 to 109 days). Four patients (20%) had consolidation antibiotic therapy, characterized by a minimum duration of 6 months of treatment. Lifelong suppressive antibiotic therapy was prescribed in five patients (25%). Trimethoprim-sulfamethoxazole was the most prescribed antibiotic for consolidation therapy (N = 3, 75%), but amoxicillin was the chosen antibiotic for maintenance therapy (N = 2, 40%).
The median follow-up time was 12 months (ranging from 3 to 36 months). One patient died during therapy. The follow-up period was not recorded in two instances. No incidences of recurrence were documented.
3.1. Retrospective Studies
Despite the absence of specific clinical data, we chose to incorporate three retrospective investigations due to the substantial number of cases documented about patients with L. monocytogenes vascular graft infections.
Ljungquist and colleagues performed retrospective observational single-center research in Sweden to elucidate the technique of direct aneurysm sac-guided suction to identify the microbiological etiology in a cohort of patients with vascular graft or endograft infections. Four L. monocytogenes graft infections were identified, leading to the conclusion that this surgical method may effectively ascertain the microbiological etiology of both open and endovascular graft infections, especially when conventional culture techniques are integrated with 16S rRNA/18S rRNA [37].
Cernohorsky and colleagues presented a retrospective cohort study conducted in two big hospitals in the Netherlands to elucidate the occurrence of endograft infection following endovascular repair of abdominal (EVAR) and thoracic aortic aneurysm (TEVAR), identifying one case attributed to L. monocytogenes. The patient received conservative surgical intervention and was treated with a combined therapy of intravenous amoxicillin/clavulanic acid and intravenous trimethoprim-sulfamethoxazole, followed by consolidation therapy with oral trimethoprim-sulfamethoxazole [38].
Shoai-Tehrani and colleagues retrospectively characterized 71 culture-confirmed Listeria monocytogenes-associated endovascular infections reported to the French National Reference Centre for Listeria from 1993 to 2018. Specifically, 14 instances pertained to prosthetic endovascular infections. The stated median age was 74, with a predominant majority of men (91%). The predominant location of infection was the descending aorta (N = 7; 50%), followed by the femoro-popliteal graft (N = 6; 42%). Cardiovascular disease was the predominant comorbidity reported (76%), encompassing hypertension (27%), coronary artery disease (23%), and atrial fibrillation (13%). Immunosuppressive diseases were identified in 50% of the individuals [39].
All patients were administered at least one antibiotic active against Listeria spp., with ßeta-lactams used in 90% of instances. Among all patients, 84% were provided with combination therapy.
Most of those patients started combination antimicrobial treatment with amoxicillin and an aminoglycoside [40]. Shoai-Tehrani and associates discovered that the death rate was markedly elevated in individuals with endocarditis compared to those with vascular infections (41% versus 12%, p = 0.009).
3.2. Potential Novel Antibiotics Against Listeria spp.
Given the need for prolonged therapies in this cohort of patients, we aimed to explore the available literature concerning novel compounds active against Listeria monocytogenes. Oritavancin, a novel long-acting lipoglycopeptide, demonstrates promising in vitro activity against Listeria monocytogenes isolates, as assessed by broth microdilution, with MIC 50 findings of ≤0.008 mg/L, as reported in Table 3 [41].
Additionally, Dalbavancin was assessed in seldom isolated Gram-positive bacteria, demonstrating promising in vitro efficacy against Listeria monocytogenes (MIC 0.06/0.12 μg/mL) isolates [42]. Sader et al. found restricted efficacy of the fifth-generation cephalosporin, ceftaroline, against some strains of Listeria monocytogenes [43]. Daptomycin was assessed against clinical isolates of infrequently reported Gram-positive microorganisms, including viridans group streptococci, Corynebacterium spp., Micrococcus spp., and L. monocytogenes, which demonstrated elevated daptomycin minimum inhibitory concentrations (MIC 50 and MIC 90, 2 and 4 μg/mL, respectively) compared to other evaluated organisms [44]. Additionally, a promising intracellular effectiveness of tedizolid against L. monocytogenes (MIC 0.125 mg/L) isolates was documented in a pioneering work [45,46]. Furthermore, the inherent properties particular to the antibiotic class suggested a possible efficacy of meropenem/vaborbactam, delafloxacin, plazomicin, tigecycline, and eravacycline against L. monocytogenes, despite the absence of in vitro or in vivo evidence for these innovative therapeutic drugs at the time of this research. To our knowledge, no ongoing trials involving novel antibiotics and L. monocytogenes are registered at the time of our paper submission.
4. Discussion
In this paper we aimed to review the literature on vascular graft infections due to Listeria monocytogenes, with a focus on treatment and the activity of novel antibiotics against these bacteria.
Most of the patients (90%) included in this review were males, with a median age of 74 years old. According to recent evidence, male sex and older adults are at higher risk for vascular graft infections compared to the general population, and older males seem to have a higher rate of vascular surgery interventions compared to the general population [47]. Moreover, Listeria spp. infection is most often seen in the first 30 days of life or in patients older than 60 [48], and a recent meta-analysis showed an increase in listeriosis-related mortality with age [2]. This age-related higher prevalence in the elderly was probably linked to immunosenescence, impaired innate and adaptive immunity, and higher prevalence of immunocompromised comorbidities in older people [2,3,4]. Cardiovascular diseases, including arterial hypertension, were the most frequently reported comorbidities in the general population, probably reflecting the prevalence of these conditions in the population collected in this review [49]. The second most frequently reported comorbidity was diabetes mellitus (18%). This finding is consistent with data from the literature, such as those from the MONNALISA registry, in which 22% of patients with invasive listeriosis were affected by diabetes [50]. Although the patients were, on average, older, it is possible that impaired immunity in individuals with diabetes contributes to the increased risk of invasive Listeria monocytogenes infections. Excluding diabetes, only a minor part of patients reported other conditions causing immunodepression (25%) such rheumatological diseases and transplant recipients, as reported in Table 1.
Abdominal aortic grafts were the most common site of vascular infections in the papers included in this review; this probably reflects the epidemiology of surgery intervention [50]. Time from vascular prosthesis implantation to infection was highly variable, probably reflecting different times of exposure. Regarding Listeria spp. exposure, only a minority of the studies included in the review provided information on exposures presenting a risk of this infection. In fact, Listeria monocytogenes can theoretically contaminate a large and diverse array of food products, so it can be difficult to spot the source of infection [2]. We found that the mean time from possible Listeria spp. exposure or symptoms compatible with gastroenteric Listeria infection to the vascular graft infection was about 6 weeks. This is in line with the infection pathophysiology reported in the literature from experimental data in animals and clinical information. Initially, Listeria monocytogenes traverses the intestinal barrier and translocates to mesenteric lymph nodes and the liver and spleen [2]. Early stages are usually asymptomatic but can sometimes manifest as nonspecific febrile illness and gastroenteritis [2].
The most common microbiological diagnosis was through positive blood cultures; nevertheless, more than half of the patients (55%) had negative blood cultures, and microbiologic diagnosis was obtained via culturing percutaneous drained aspirations or biopsy taken during surgery.
Although an injected CT scan was the most common radiological diagnostic method in this literature review, we found that PET/TC was used during the diagnostic process in seven cases (35%), and for follow-up in three cases (15%). As recently suggested by the Management of Aortic Graft Infection Collaboration (MAGIC) [51], the diagnosis of vascular infection derives from the combination of clinical, biochemical, and microbiological findings, as well as imaging.
PET/TC reported high sensitivity and negative predictive value in the diagnosis of vascular graft infections and a potential role in imaging follow-up during treatment [51,52]. However, given its lower specificity, positive results should be confirmed, for example, with white blood cell scintigraphy, especially in early graft infections [52]. No definitive data on white blood cell scintigraphy were available from the article collected.
Most of the patients were treated conservatively with a combination of ampicillin plus an aminoglycoside. Nonetheless, it must be noted that clear evidence supporting the efficacy of combination therapy in Listeria monocytogenes infections is lacking in the literature [53]. Almost half of patients (45%) were treated with medical treatment (without source control being feasible) and 55% were treated with both surgery and antibiotics.
Only one patient died, and no case of relapse or recrudescence were reported. This result, although limited by the low sample size of this cohort, diverges from other results in the literature, where mortality for bacteriemia is around 27%.
Regarding the duration of antibiotic treatment, we found considerable heterogeneity in the literature. Most frequently, at least 4 to 6 weeks of first line treatment were prescribed, followed by either consolidation therapy (defined as at least 6 months of treatment), lifelong suppressive antibiotic therapy in similar proportions (25% vs. 20%, respectively), or nothing (35%).
In the review of novel compounds with potential in vitro or in vivo activity against Listeria spp. we have reported interesting preliminary data on the in vitro activity of two new long-acting antibiotics, dalbavancin and oritavancin [41,42,54,55]; nevertheless, data should be confirmed in vivo and in larger studies. Given the need for prolonged therapies in this cohort of patients, the long-acting compounds profile in terms of efficacy and safety seems promising, also due to the potential anti-biofilm activity in graft infections [54,55]. Regarding antibiotics with a potential activity against Listeria spp., we also look with interest to tedizolid and delafloxacin, especially for the possibility of both oral and intravenous administration and the interesting pharmacokinetic profile and vascular graft penetration [56,57]. Despite that, data regarding delafloxacin and tedizolid activity were only based on in vitro activity and data should be confirmed in vivo and in larger studies.
5. Conclusions
In conclusion, while vascular graft infections due to Listeria monocytogenes remain a rare clinical entity, our review highlights the need for greater standardization in diagnostic and therapeutic approaches. The current literature, based largely on retrospective data and case reports, underscores the importance of heightened clinical suspicion. At risk patients could be older male adults with abdominal aortic grafts, including those without a classical immunocompromised past medical history. PET-CT may be considered in the diagnosis and follow-up of vascular graft infections without surgical indications, especially in case of prolonged or suppressive antibiotic treatment. Further research is needed to better define optimal management strategies for vascular graft infections due to Listeria monocytogenes, including duration of antibiotic therapy, as well as the need for surgical intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chiesa R. Astore D. Frigerio S. Garriboli L. Piccolo G. Castellano R. Scalamogna M. Odero A. Pirrelli S. Biasi G. Vascular prosthetic graft infection: Epidemiology, bacteriology, pathogenesis and treatment Acta Chir. Belg.200210223824710.1080/00015458.2002.1167930512244902 · doi ↗ · pubmed ↗
- 2Koopmans M.M. Brouwer M.C. Vázquez-Boland J.A. van de Beek D. Human Listeriosis Clin. Microbiol. Rev.202336 e 000601910.1128/cmr.00060-1936475874 PMC 10035648 · doi ↗ · pubmed ↗
- 3Swaminathan B. Gerner-Smidt P. The epidemiology of human listeriosis Microbes Infect.200791236124310.1016/j.micinf.2007.05.01117720602 · doi ↗ · pubmed ↗
- 4Zenewicz L.A. Shen H. Innate and adaptive immune responses to Listeria monocytogenes: A short overview Microbes Infect.200791208121510.1016/j.micinf.2007.05.00817719259 PMC 2042024 · doi ↗ · pubmed ↗
- 5Farber J.M. Peterkin P.I. Carter A.O. Varughese P.V. Ashton F.E. Ewan E.P. Neonatal listeriosis due to cross-infection confirmed by isoenzyme typing and DNA fingerprinting J. Infect. Dis.199116392792810.1093/infdis/163.4.9271901339 · doi ↗ · pubmed ↗
- 6Schwartz B. Hexter D. Broome C.V. Hightower A.W. Hirschhorn R.B. Porter J.D. Hayes P.S. Bibb W.F. Lorber B. Faris D.G. Investigation of an outbreak of listeriosis: New hypotheses for the etiology of epidemic Listeria monocytogenes infections J. Infect. Dis.198915968068510.1093/infdis/159.4.6802494267 · doi ↗ · pubmed ↗
- 7Riedo F.X. Pinner R.W. Tosca M.L. Cartter M.L. Graves L.M. Reeves M.W. Weaver R.E. Plikaytis B.D. Broome C.V. A point-source foodborne listeriosis outbreak: Documented incubation period and possible mild illness J. Infect. Dis.199417069369610.1093/infdis/170.3.6938077731 · doi ↗ · pubmed ↗
- 8Grif K. Patscheider G. Dierich M.P. Allerberger F. Incidence of fecal carriage of Listeria monocytogenes in three healthy volunteers: A one-year prospective stool survey Eur. J. Clin. Microbiol. Infect. Dis.200322162010.1007/s 10096-002-0835-912582739 · doi ↗ · pubmed ↗