Changes in Speckle Tracking Echocardiography Values of the Descending Thoracic Aorta with Rising Positive End-Expiratory Pressure Levels
María Belén Martínez-Lechuga, Javier Hidalgo-Martín, José Ángel Ramos Cuadra, Julia Manetsberger, Ana Blanco-Serrano, Veronica Todaro, Gabriel Heras-La-Calle, María Leyre Lavilla Lerma, Juan Carlos Fernández-Guerrero, Manuel Ruiz-Bailén

TL;DR
This study shows how changes in breathing pressure affect aorta measurements in heart failure patients using ultrasound tracking.
Contribution
The study introduces speckle tracking echocardiography as a novel method to assess thoracic aorta function in cardiogenic shock patients under varying PEEP levels.
Findings
DTA rotational velocity peaks at 5 cmH2O PEEP and declines at higher levels.
DTA rotational displacement at 5 cmH2O PEEP correlates with patient mortality.
Circumferential strain in the DTA decreases with increasing PEEP.
Abstract
Background and Objectives: The aim of this study is to evaluate the changes in speckle tracking velocity vector analysis (VVI) values within the descending thoracic aorta (DTA) in patients with cardiogenic shock (CS) who are on mechanical ventilation (MV), under varying levels of positive end-expiratory pressure (PEEP). Materials and Methods: Transthoracic echocardiography (TTE) was performed during incremental increases in positive end-expiratory pressure (PEEP) from 0 to 15 cmH2O over 15 to 30 min. The effects of increased PEEP on velocities, displacement, strain (S), and strain rate (SR) were evaluated. DTA speckle tracking values were analyzed to determine their association with patient mortality. A control group of healthy individuals was used to establish normal DTA variables. Results: Sixty-two mechanically ventilated patients were included in this study. The mean age was 62.48 ±…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
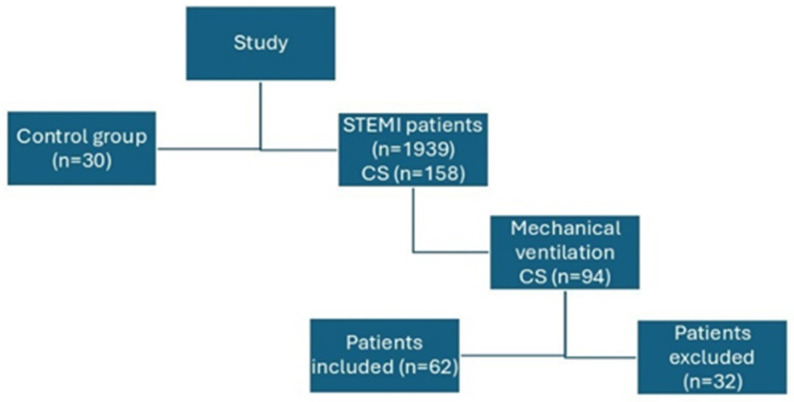 Figure 1
Figure 1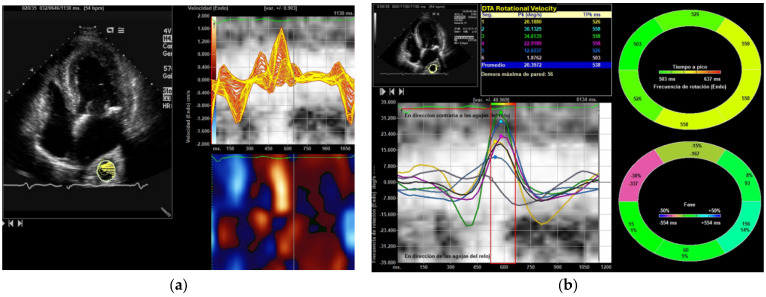 Figure 2
Figure 2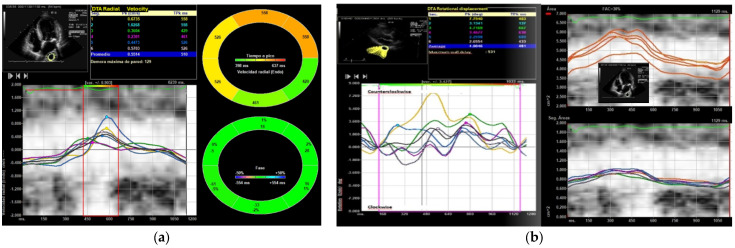 Figure 3
Figure 3- —Servicio Andaluz de Salud, Government of Spain
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Mechanical Circulatory Support Devices · Hemodynamic Monitoring and Therapy
1. Introduction
The incidence of cardiogenic shock (CS) in acute myocardial infarction (AMI) remains at 10% [1], with mechanical ventilation (MV) required in 40–80% of cases [1]. Patients often experience cardiogenic edema with severe hypoxemia, necessitating distinct levels of PEEP to enhance oxygenation and increase lung recruitment. Previous research by our team indicated that varying levels of PEEP could alter ventricular strain and potentially improve mitral regurgitation [2]. Positive end-expiratory pressure (PEEP) is a well-studied intervention commonly used in ICUs. Its use causes significant hemodynamic changes, first noted last century. PEEP can alter extravascular lung water in models of pulmonary and cardiogenic edema, and patients frequently need positive-pressure ventilation (PPV) [3,4].
Cardiogenic shock mortality is often associated with the left ventricular ejection fraction. Nevertheless, this relationship remains intricate. Despite recent anatomical findings, like those by Torrent Guasp [5,6], cardiovascular pathophysiology still depends on key concepts: contractility, preload, afterload, ventricular interdependence, and diastology. However, the integration of atrial contribution, synchrony, and particularly aortic function remains unclear. Aortic function and its underlying mechanisms remain poorly understood, with limited current research available [7,8]. Systemic inflammation and neurohumoral factors mediate this process. Interestingly, studies indicate that muscle cells in the aorta and the use of levosimendan can enhance aortic relaxation [9]. Echocardiography has improved the diagnostic evaluation of hypoxemia in intensive care units, facilitating earlier identification of heart failure and potentially lowering the incidence of acute respiratory distress syndrome. As a result, echocardiography has become an indispensable tool for managing critically ill patients in intensive care settings [10], particularly in cases of cardiogenic shock, which continues to be associated with high mortality rates [11,12,13,14,15]. Speckle tracking has been employed in all four cardiac chambers, yielding diagnostic data. Previous research, however, has not examined the use of this technique for the aorta. Recently, our research team implemented speckle tracking velocity vector analysis to evaluate the velocity, deformation, and displacement of the descending thoracic aorta (DTA) [7].
Speckle tracking echocardiography has been used in research with mechanically ventilated patients [2,5]. Although the cardiovascular effects of PEEP are well documented, the extent of alterations occurring within the aorta remains undetermined. This variability may be attributable to changes in transmural pressure, variations in ventricular filling, or inherent characteristics of the aorta itself. Furthermore, aortic measurements have potential utility as parameters for evaluating optimal PEEP based on cardiovascular responses. To date, no published studies have applied speckle tracking to the aorta at varying levels of PEEP.
This study examined the effects of increased PEEP levels on strain, strain rate, radial and circumferential velocities, and displacements using speckle-tracking vector velocity imaging (VVI) echocardiography in critically ill CS patients on MV. The study also assessed whether speckle tracking VVI values are independently associated with mortality in cardiogenic shock.
2. Materials and Methods
2.1. Study Design
The present study was a prospective observational clinical study. The cohort was generated from all CS patients admitted in ICU who required MV. Rising levels of PEEP were applied to these patients. Changes in levels of PEEP are usually performed on critically ill patients on MV. CS was defined by the criteria used in the shock trials and specifically in the presence of systolic blood pressure below 90 mmHg that did not respond to volume administration, requiring the use of noradrenaline or adrenaline for at least 1 h [10,11,12,13]. This work was supported by PAIDI CTS 606, Andalusian Health Service Project no, “PI-0585-2012 Ecocardiografía en Medicina Crítica. Detección de la disfunción Miocárdica del Paciente Crítico e interacción entre la ecocardiografía y la ventilación mecánica Servicio Andaluz de Salud. Junta de Andalucía. España”; approved by the local ethics committee and funded by the Department of Health of the regional government of Andalusia, Spain. The data were stored in a dissociated database to ensure the blinding of the study. The present study was limited to Jaén Hospital. The inclusion period was from January 2014 to January 2024, excluding the years 2020 to 2022 due to the COVID-19 pandemic.
Clinical and demographic details were considered. All echocardiographic parameters recommended by the American Society of Echocardiography were duly considered (https://www.asecho.org/).
2.2. Study Protocol
This study is an echocardiographic investigation intended to evaluate aortic response to different levels of PEEP, rather than serving as an epidemiological analysis. As the focus is on echocardiography, information on clinical, hemodynamic, or laboratory variables is limited; interleukin-6 was the only marker consistently measured in all mechanically ventilated patients (Kit Elecsys IL-6, (Bio-Techne, Minneapolis, MN, USA) detection limit of 1.5 pg/mL cobas^®^). Troponin and brain natriuretic peptide were not measured due to changes in testing methods during the study period.
2.3. Inclusion Criteria
The following criteria were applied for the inclusion of patients in the study: (a) patients with ST elevation myocardial infarction (STEMI) who develop CS and have required norepinephrine and MV; (b) having been revascularized by percutaneous cardiovascular intervention; (c) PEEP ≥ 5 cmH_2_O; (d) FiO_2_ ≤ 0.5; and (e) ventilatory plateau pressure ≤ 25 cmH_2_O.
2.4. Exclusion Criteria
Patients were excluded from the study for any of the following reasons: (1) having been managed without echocardiography; (2) poor sound quality; (3) requiring a certain level of PEEP specific to the severity of their condition; (4) refusing to participate in the study; (5) having CS of etiology other than acute coronary syndrome; (6) patients who were transferred to a center with a cardiovascular surgery service (not available in our center); (7) patients who only required the use of noradrenaline during percutaneous coronary intervention, arriving at the coronary unit without vasoactive amines; (8) mechanical complications (6 ventricular septal defects, 8 papillary muscle ruptures, 3 functional mitral insufficiencies requiring surgical repair and 12 cardiac ruptures); (9) aortic valvulopathy ≥ grade 3 and (10) aortic atheroma > 2 Kazt’ grade classification [14].
2.5. Changes in PEEP Levels
Patients requiring varying levels of PEEP as a routine part of the management of their condition were included in the study. All patients were started on ZEEP, and the PEEP was increased by 5 cmH_2_O, until a maximum PEEP of 15 cmH_2_O (ZEEP, PEEP 5, PEEP 10, and PEEP 15 cmH_2_O). This procedure was performed after hemodynamic stability had been achieved and after removing all vasoactive drugs (epinephrine, norepinephrine, dobutamine, and levosimendan), although the entry criterion was to have been admitted with CS. No other breathing pattern was changed. Echocardiography was performed after 15 to 30 min of introducing changes in PEEP levels. Patients were without respiratory drive or were sedated to abolish respiratory drive. Modification of PEEP levels was suspended if the patient showed signs of clinical deterioration, such as (a) decrease in saturation oxygenation, (b) increase in peak or plateau pressures, (c) impairment of protective MV, or (d) hemodynamic changes amounting to 10% (changes in blood pressure or heart rate).
2.6. Control Group
A control group of healthy subjects without CS and with spontaneous breathing was included to establish reference values for our coronary unit via speckle tracking of the DTA. They were compared to CS patients on MV with a PEEP of 5 cmH_2_O, as most patients on MV had at least that level of PEEP.
2.7. Image Acquisition and Processing
Patients underwent an advanced TTE, which was conducted in supine position and was recorded in digital Dicom format. For off-line analysis purposes, we used 2D and 3D and Speckle Tracking Hybrid VVI [15]. Echocardiographic studies were performed with the following echocardiographic equipment available during long-term study period: Sequoia c512, Acuson, SC 2000, Siemens Medical Systems, Mountain View, CA, USA, and Epiq CX50. TTE was performed in the control group and in all patients. Transoesophageal echocardiography (TEE) was only performed when the diagnosis of shock was not clear and mainly to evaluate the mitral valve or when there was suspicion of mechanical complications. were realized. The echocardiographic variables studied have been determined both online and offline, using echocardiographic programs Syngo software 2013, Siemens^®^ U.S. and Tomtec Arena 2020 (https://www.tomtec.de/excellence-in-digital-healthcare/, accessed on 10 October 2024).
The apical four-chamber view was utilized to obtain data on left ventricular function and the DTA analysis. The frame rate varied from 70 to 120 frames per second, incorporating multiple focal points. All images were meticulously adjusted for gain, compression, and dynamic range.
The standard echocardiographic parameters, as recommended by the American Society of Echocardiography, were evaluated, including the quantification of left ventricular systolic ejection fraction (LVEF) using both 2D and 3D methods. Additionally, parameters derived from speckle tracking echocardiography, such as strain (S), strain rate (SR), longitudinal and radial displacement, and velocities in the left ventricle, were assessed. Furthermore, we analyzed radial and rotational velocity, radial and circumferential strain, strain rate, as well as rotational and radial displacement in the descending thoracic aorta (DTA) using Speckle Tracking Vector Velocity Imaging (VVI) analysis. The region of interest was meticulously delineated manually.
2.8. Statistical Analysis
The Kolmogorov–Smirnov test was used to assess the normality of the variables. After confirming the normality of the variables, quantitative variables were analyzed using ANOVA and Student’s t-test. The Levene statistic was used to evaluate variance homogeneity. When equal variances were assumed, the Bonferroni test and Tukey post hoc test were applied to control the probability of Type I error. The Anova test was used to evaluate the changes in the different clinical and echocardiographic variables with different PEEP levels. Student’s t-test was employed to assess the differences between the control group and the group treated with 5 cmH_2_O of PEEP, as this level of PEEP is the most used. The correlation between left ventricle ejection fraction, left and right ventricular strain, and DTA variables were studied using Pearson’s correlation coefficient. The degree of agreement between the strain values obtained in the parasternal long axis and the apical four-chamber planes was evaluated using Bablok regression and a Bland–Altman plot. Results were presented using means and standard deviations. A p value < 0.05 was considered statistically significant.
A multivariate logistic regression analysis was conducted, with “deceased” designated as the dependent variable and only echocardiographic data serving as independent variables. Statistical analyses were performed using IBM SPSS version 30 (Chicago, IL, USA).
3. Results
3.1. Cardiogenic Shock Patients
A total of 1893 STEMI patients were included during the study period, 158 developed CS (8.4%), 94 (59.49%) required MV. We excluded 15 patients admitted for apparent septic shock and acute respiratory failure initially attributed to possible infections, who were later shown to have suffered an AMI. Six patients with a mean age of 52.38 ± 18.32 years were transferred to a different hospital for extracorporeal membrane oxygenator (ECMO) implantation, after implantation of balloon counterpulsation or impella catheter and maintained in SCAI D shock; they were also excluded. Eleven patients initially included in the study, recovered from CS, presented weaning failure with grade 2–3 functional mitral regurgitation and normal LVEF. All of them underwent stress TEE and grade 4 mitral regurgitation was observed. They were transferred to mitral valve surgery and excluded. One of those patients who was excluded because she was initially diagnosed with sepsis, had a thrombus in the thoracic aorta seen on TEE. She had thoracic aortic velocities, displacements and strain of almost 0, and there was no change with increases in PEEP level.
A total of sixty-two patients with CS were enrolled in the study (Figure 1), of whom 29 (46.78%) were female. Risk factors and complications are detailed in Table 1. The mean APACHE II score was 22.91 ± 13.45. The average LVEF measured 27.12 ± 0.015% and the lateral right ventricular strain was −15.64 ± 0.11. The mean age was 62.48 ± 11.22 years, and the mean ICU length of stay was 15.32 ± 12.22 days. In total, 28 patients (45.61%) died.
The mean Interleukin-6 (IL-6) value among the 62 patients requiring mechanical ventilation was 137.12 ± 5.29 pg/mL, which, in bivariate analysis, was associated with increased mortality (84.89 ± 7.33 pg/mL in survivors versus 165.06 ± 11.17 pg/mL in deceased patients; Student’s t-test, p < 0.001). IL-6 levels correlated with DTA rotational displacement (R^2^ = 0.39, p = 0.001). Hemodynamic and ventilatory parameters are presented in Table 2.
3.2. Changes in PEEP Levels
With increasing PEEP level from 0 to 15 cmH_2_O increased SpO_2_, peak and plateau pressures, but no clear changes in hemodynamic variables were observed. With this increase in PEEP levels there was a significant increase in left ventricular strain and strain rate, although LVEF also seemed to increase, although not significantly. Right ventricular function did not differ significantly. With increasing PEEP, the delay times between the different ventricular segments in the strain and strain rate decreased, and there may be greater synchrony in the left ventricle with increasing PEEP (Table 3).
3.3. Descending Thoracic Artery Aorta
DTA artery mean diameter was 27.82 ± 3.45 mm with no substantial changes. However, there were very significant changes in its fractional shortening area, rotational velocity, radial velocity, strain, strain ratio, and rotational displacement. The radial displacement increases greatly with 5 cmH_2_O but drops to ZEEP levels with further increases in PEEP, with no statistical significance. In all these parameters generated by speckle tracking using VVI analysis a clear pattern could be observed. When treating patients with 0 cmH_2_O of PEEP (ZEEP) the minimum value is obtained in all analyzed values, and after applying 5 cmH_2_O the maximum increase in all values is produced, especially in their rotational velocity (which increases by double).
After raising the PEEP level to 10 cmH_2_O almost all its parameters, except for the two types of displacement, continued to be higher than the initial value, and after increasing to 15 cmH_2_O, the values returned to those obtained without PEEP or slightly higher. Interestingly, after applying ≥10 cmH_2_O we observed an increased loss of echocardiographic DTA due to the worsening of the acoustic window and the impossibility of speckle tracking use. The DTA rotational displacement correlates with left ventricular longitudinal strain, right ventricular longitudinal strain, but not with LVEF assessed by 2 and 3D echocardiography (Pearson’s r 0.32, and 0.41, respectively, p < 0.001). DTA rotational velocity correlate only with left ventricular strain (Pearson’s r 0.26, p < 0.001). Logistic binary regression identified left ventricular strain [OR 0.75 (95% CI 0.45–0.91), p < 0.05], rotational velocity [OR 0.38 (95% CI 0.12–0.88), p < 0.05], and rotational displacement [OR 0.55 (95% CI 0.38–0.85), p < 0.05] as echocardiographic variables associated with death in the DTA group with 5 cmH_2_O of PEEP (Figure 2 and Figure 3).
Patients in the control group had higher diastolic pressure, lower respiratory rate, higher ejection fraction, higher systolic velocities on tissue Doppler imaging of the mitral annulus, greater left ventricular deformity, better right ventricular function, but nevertheless with the use of 5 cmH_2_O of PEEP the speckle tracking values of the thoracic aorta increased (Table 4).
4. Discussion
This echocardiographic study attempts to evaluate the changes produced in the parameters derived from speckle tracking by VVI analysis in the DTA in patients in CS requiring MV. Although the work also provides some epidemiological data on CS, we do not intend to perform an epidemiological study, as we lack crucial clinical and angiographic variables to be able to make any assertion on CS and the study design is not appropriate for this purpose. Incidence appears to be lower than that reported in the Spanish ARIAM registry [16,17] and other registries [1]. Spanish registry in 2011 [18] we already perform echocardiography in almost 100% of patients with CS, and most patients are followed up nearly daily.
The mean age of patients in this study is lower than the ages reported in the ARIAM registry [14], the RESCUE registry (66 years) [19], the Shock registry [11], CardShock (68.7 years) [20], and several other registries [21,22,23,24,25,26,27]. The rate of MV in this study was lower than that in the RESCUE registry, but within the previously described ranges for CS (40 to 80%) [28].
The average length of stay observed in this study is comparable to findings from other registries, particularly the RESCUE study (12 days) [19]. Observed mortality rates were lower than those reported in the ARIAM registry [14] and the Shock registry (61%) [11], but higher than those found in the Korean RESCU register (33.6%) [19] and CardShock (36.5%) [20].
In summary, the population included in this echocardiographic study is like that of other registries. Interestingly, we have performed stress echocardiography to detect weaning failure and severe valvular heart disease; an option that we consider very valid in critically ill patients in whom the degree of mitral regurgitation is in doubt or in the presence of weaning failure [29,30].
PEEP—and positive-pressure ventilation in general—has been shown to improve ventricular function [2]. Furthermore, and although it might be a false response to transmural pressure changes, benefits in left atrial remodeling have been shown in patients with sleep apnea hypopnea syndrome [31,32]. One finding that confirmed previous results from by our group showed that PEEP could improve left ventricular synchrony, which would translate into an improvement of significant left ventricular function [19]. Speckle tracking could predict the cardiological evolution of sleep apnea-hypopnea syndrome [33] and could even decrease latent systolic dysfunction in these patients [34].
The most interesting result of this study is that we have been able to quantify the values of the DTA in CS patients and that these values have also varied with the levels of PEEP introduced. This represents a new avenue for research on the interaction between aorta and MV; but it also implies that its values are associated with mortality in CS. Interestingly, this study may suggest that evaluating DTA values could indicate the optimal PEEP level and serve as a prognostic marker in shock scenarios. In CS and heart failure more broadly, numerous variables affect the response; however, aortic pathology is typically not considered as a predictor variable. The aorta can be divided into three parts: ascending aorta, aortic arch and descending aorta. Primarily, its functions involve opening and closing the aortic valve and assisting with ventricular ejection [35]. An important challenge involves evaluating this activity, with diameter measurements frequently serving as indicators of remodeling [36]. Cardiac resonance is essential for identifying physiological changes [37]. Echocardiography is limited to detecting diameters, atheromatous plaques, remodeling, or complications such as acute aortic syndrome. Speckle tracking is a fundamental tool in cardiology; however, there is no software that uses this technology to evaluate the aorta [38]. VVI speckle tracking was applied in the thoracic aorta to establish baseline measurements and monitor changes in velocities, strain, strain rate, and DTA displacement at different levels of PEEP. However, in the multivariable analysis, only rotational displacement was identified as a variable associated with mortality. Also, rotational displacement correlated with LV and RV longitudinal strain and LV strain rate.
The explanation is still unknown, but we believe that what is being measured is the behavior of the aorta, and that rotational displacement is probably a more precise parameter than its velocities (especially radial velocity) or its strain. Undoubtedly, we consider it a strong and potentially accurate parameter.
The observed correlation may be attributable to the anatomical linkage between the heart and the aorta, potentially facilitating the transmission of cardiac motion and flow into the aortic vessel. Additionally, these findings may also reflect both the physiological state and aorta remodeling.
The value associated with mortality is DTA rotational displacement at 5 cmH_2_O PEEP, suggesting this may represent the optimal level. Alterations in aortic geometry resulting from transmural pressure and aortic muscle activity could account for these findings. A PEEP less than 10 cmH_2_O may be advantageous for aortic function, whereas 15 cmH_2_O might be harmful, thereby assisting in identifying the most appropriate PEEP setting.
Therefore, we believe that aortic assessment could have prognostic value in certain pathologies or shock situations. Previous studies have reported that patients with aortic atherosclerosis or a rigid aorta may exhibit symptoms of heart failure, independent of their underlying cardiovascular condition [38,39]. The aorta plays a key role in cardiovascular function and warrants further study. Speckle tracking may improve our understanding of its physiology. Heart failure after aortic repair could demonstrate this reciprocal relationship [40]. This is exploratory work, but it implies that specific software based on speckle tracking could be developed to assess aorta function.
The results may also be conditioned by the degree of inflammation [41,42,43]; in fact, the present study shows that interleukin 6 is related to displacement and rotational aorta. Other authors have suggested anti-inflammatory drugs to limit the severity of aortic pathology [43].
Pathological aortic remodeling could affect not only the aortic valve but also the entire cardiovascular pathophysiology. Another variable (although not used in this study) which could provide information on the hemodynamic situation is the time velocity integral in the abdominal aorta. This value could be correlated with the circulation at that level and the hemodynamic situation. It is an easy measurement, evaluable in the subcostal plane.
Limitations
One limitation of this study is the lack of specific software designed for aortic assessment using speckle tracking. While VVI speckle tracking was employed to monitor changes in the thoracic aorta, current echocardiographic tools are limited and do not fully capture the complexity of aortic motion or remodeling [7]. The different systolic peaks are determined; the software is intended for speckle tracking of the ventricular mass but is used on the aortic wall, which could lead to issues. Nonetheless, credible patterns have emerged that may demonstrate improved safety and efficacy when assessed with software specifically developed for the aorta. Therefore, while the study presents an innovative concept, its findings should not be widely extrapolated. It is appropriate only to propose the hypothesis that Speckle Tracking could be applied to evaluate the aorta, and that the resulting values may correlate with outcomes in cardiogenic shock. However, our results are not generalizable. Further research and technological advances may include the development of specialized aortic analysis software, enabling more precise assessment of the vessel’s dynamic properties in both healthy individuals and CS patients.
Here, we used a small sample of patients with CS, which may limit patient selection and introduce potential bias. Furthermore, the changes detected with PEEP demonstrated patterns that indicate possible alterations in aortic physiology and may warrant further investigation regarding its relevance for determining optimal PEEP levels at the cardiovascular level. Additionally, as this study is exploratory, its findings should be validated in larger patient groups and under varying clinical conditions.
Although there are limitations, this study indicates that incorporating speckle tracking in the aorta may offer valuable insights. Establishing reference values could facilitate a better understanding of aortic pathologies and cardiovascular interactions, potentially contributing to the interpretation of heart failure semiology.
5. Conclusions
Increasing PEEP affects DTA speckle tracking values. Speckle tracking can assess the thoracic aorta, and parameters like rotational displacement may relate to cardiogenic shock prognosis. Further research into aorta-specific speckle tracking technology is recommended.
Speckle tracking VVI has not previously been used to assess the aorta; this study applies it to the DTA, comparing values in healthy individuals and those with cardiogenic shock. The results show that these values vary with mechanical ventilation settings and may be linked to mortality in cardiogenic shock.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Samsky M.D. Morrow D.A. Proudfoot A.G. Hochman J.S. Thiele H. Rao S.V. Cardiogenic Shock After Acute Myocardial Infarction: A Review JAMA 202132618401850 Erratum in JAMA 2021, 326, 2333. https://doi.org/10.1001/jama.2021.2138110.1001/jama.2021.1832334751704 PMC 9661446 · doi ↗ · pubmed ↗
- 2Ruiz-Bailén M. Cobo-Molinos J. Castillo-Rivera A.M. Iniesta-Carricondo M.C. Pola Gallego de Guzmán M.D. Cárdenas-Cruz A. Increasing Levels of Positive End-expiratory Pressure Improve the Left Ventricular Strain J. Thorac. Imaging 20173233333910.1097/RTI.000000000000026928489667 · doi ↗ · pubmed ↗
- 3Ruiz-Bailén M. Fernández-Mondéjar E. Hurtado-Ruiz B. Colmenero-Ruiz M. Rivera-Fernández R. Guerrero-López F. Vázquez-Mata G. Immediate application of positive-end expiratory pressure is more effective than delayed positive-end expiratory pressure to reduce extravascular lung water Crit. Care Med.199927380384 Erratum in Crit. Care Med. 1999, 27, 169610.1097/00003246-199902000-0004610075064 · doi ↗ · pubmed ↗
- 4Franchi F. Faltoni A. Cameli M. Muzzi L. Lisi M. Cubattoli L. Cecchini S. Mondillo S. Biagioli B. Taccone F.S. Influence of positive end-expiratory pressure on myocardial strain assessed by speckle tracking echocardiography in mechanically ventilated patients Bio Med Res. Int.2013201391854810.1155/2013/91854824066303 PMC 3771268 · doi ↗ · pubmed ↗
- 5Ross D.N. Torrent-Guasp’s anatomical legacy Eur. J. Cardiothorac. Surg.200629(Suppl. 1)S 18S 2010.1016/j.ejcts.2006.03.00516564699 · doi ↗ · pubmed ↗
- 6Abraham-Foscolo M.M. Blanco R. Chiabrando J.G. Llamedo M.C. Arenaza D.P. Falconi M.L. Torrent Guasp’s helicoid pattern myocardial calcification Arq. Bras. Cardiol.202211899299510.36660/abc.2021037035613202 PMC 9368865 · doi ↗ · pubmed ↗
- 7Ruiz-Bailén M. Hidalgo-Martín J. Manetsberger J. Clau-TerréF. Martínez-Gámez J. Dagomar Lohman J. Lavilla-Lerma M.L. Matallana-Zapata D.F. Ballesteros-Barroso M. Rivera-Fernández R. Usefulness of vector velocity imaging in the descending thoracic aorta Med. Intensiva (Engl. Ed.)202550222410.1016/j.medine.2025.50222440450433 · doi ↗ · pubmed ↗
- 8Kundel V. Trivieri M.G. Karakatsanis N.A. Robson P.M. Mani V. Kizer J.R. Kaplan R. Fayad Z. Shah N. Assessment of atherosclerotic plaque activity in patients with sleep apnea using hybrid positron emission tomography/magnetic resonance imaging (PET/MRI): A feasibility study Sleep Breath.2018221125113510.1007/s 11325-018-1646-229508121 PMC 6425735 · doi ↗ · pubmed ↗