Comparison of Total Mesopancreatic Excision and Conventional Pancreaticoduodenectomy in the Surgical Treatment of Pancreatic Head Adenocarcinoma: Early Postoperative Outcomes
Tufan Egeli, Tarkan Unek, Mucahit Ozbilgin, Cihan Agalar, Anıl Aysal Agalar, Ilkay Tugba Unek, Caner Bektas, Gokce Kıran Kazancı, Berkay Sakaoglu, Emre Karadeniz, Ozgul Sagol

TL;DR
This study compares two surgical techniques for pancreatic cancer and finds that one may offer better cancer removal without significantly more complications.
Contribution
The study provides early evidence on the oncological and surgical outcomes of total mesopancreatic excision compared to conventional methods.
Findings
TMpE-PD showed higher R0 resection rates and lymph node yield, though not statistically significant.
TMpE-PD had more postoperative complications, but the surgical technique was not an independent risk factor.
Smaller pancreatic duct diameter was linked to increased complication risk in both groups.
Abstract
Background and Objectives: This study aimed to evaluate and compare the early postoperative outcomes of patients who underwent pancreaticoduodenectomy (PD) with total mesopancreatic excision (TMpE) versus conventional pancreaticoduodenectomy (Co-PD) for pancreatic head ductal adenocarcinoma (PDAC). Materials and Methods: Patients who underwent PD for pancreatic head cancer between January 2021 and December 2024 in our clinic and had a pathological diagnosis of PDAC were included. Patients were stratified into two groups according to the surgical technique performed (TMpE-PD vs. Co-PD). Demographic characteristics and early postoperative clinicopathological data were compared between the groups. Results: A total of 41 patients were included: 17 (41.5%) underwent TMpE-PD and 24 (58.5%) underwent Co-PD. Demographic and clinicopathological parameters were comparable between the groups.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
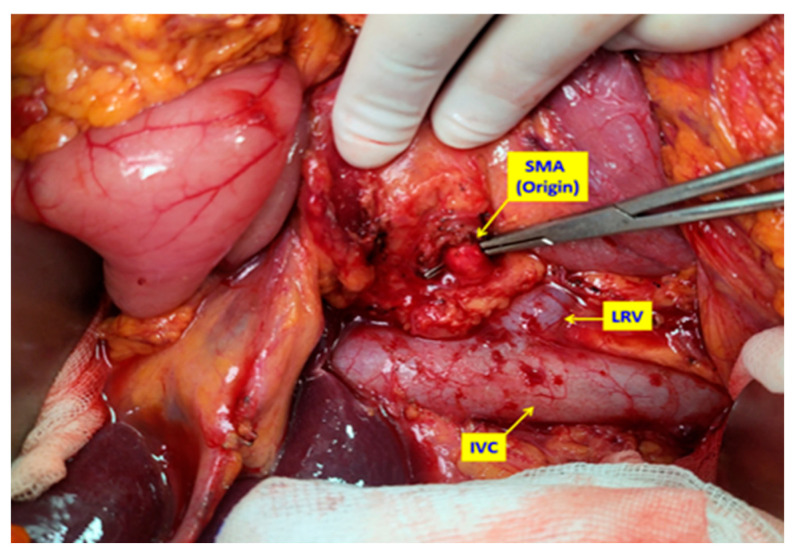 Figure 1
Figure 1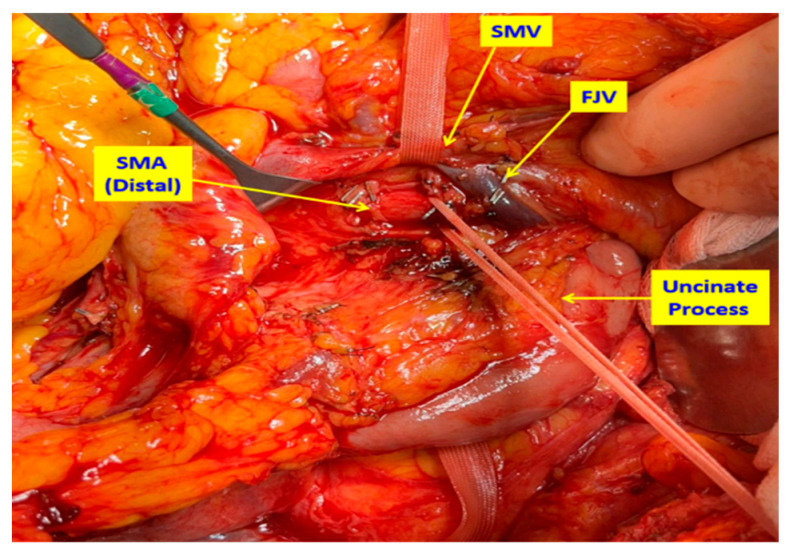 Figure 2
Figure 2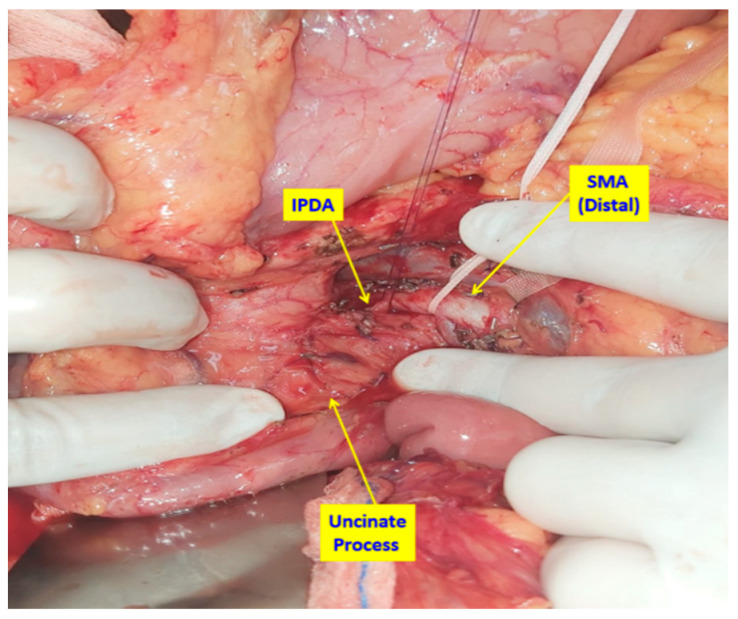 Figure 3
Figure 3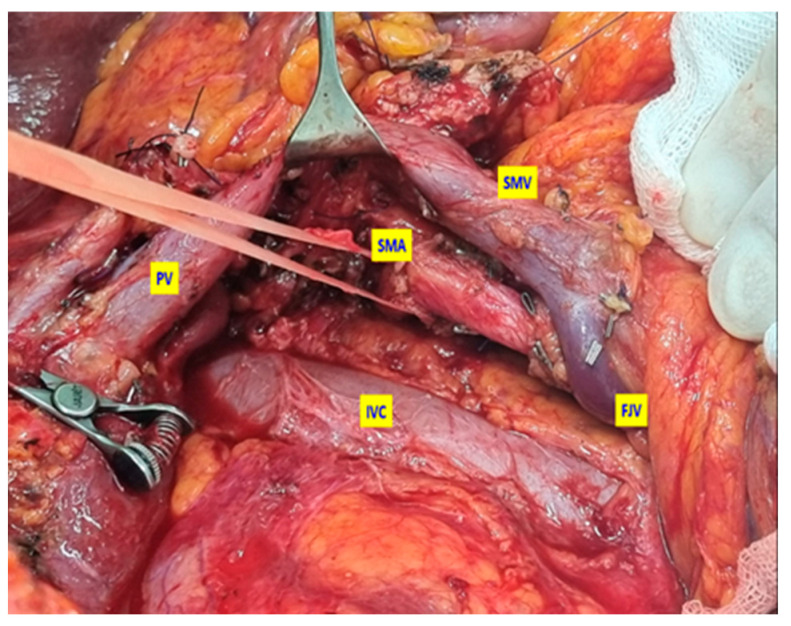 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gastrointestinal Tumor Research and Treatment · Cholangiocarcinoma and Gallbladder Cancer Studies
1. Introduction
Pancreaticoduodenectomy (PD, Whipple procedure) with curative intent (margin-negative/R0 resection), combined with adjuvant or neoadjuvant chemotherapy, currently represents the standard treatment for pancreatic ductal adenocarcinoma (PDAC) located in the pancreatic head [1,2,3,4,5,6]. However, only 15–25% of patients are eligible for surgical resection at the time of diagnosis [7]. Despite advances in surgical techniques over the years, R0 resection following PD is reported in only about 50% of cases [8]. Furthermore, local recurrence develops in approximately 80% of patients after PD, even in those considered to have undergone R0 resection, suggesting that true complete resection may not have been achieved [9,10]. Esposito et al. reported that the frequency of R1 resection margins in PD specimens increased from 14% to 76% when reassessed using standardized contemporary pathological evaluation methods [11]. Even in patients undergoing combined PD and chemotherapy for pancreatic head cancer, 5-year survival rates remain around 20–25% [12,13,14]. This poor outcome is attributed to early locoregional recurrence secondary to incomplete (non-curative) resections. Ghaneh et al. demonstrated that non-curative resections significantly reduce both overall and disease-free survival in patients with pancreatic cancer [15].
In 2007, Gockel et al. first introduced the concept of the “mesopancreas” [16]. The mesopancreas is defined as a structure located posterior to the pancreatic head, consisting of neural and lymphatic tissues extending along the mesenteric vascular axis. This region represents a major pathway for tumor spread in PDAC. Gockel emphasized that incomplete resections following PD often result from residual tumor deposits in this area and highlighted the necessity of performing a “total mesopancreatic excision (TMpE)” to achieve true curative resection. Supporting this view, Gadcke et al. demonstrated that the most frequent site of R1 resection after PD was the mesopancreatic region [17]. Subsequent studies have reported that PD with TMpE increases the likelihood of achieving true R0 resection, improves lymph node yield, and thereby confers a survival advantage [18,19,20].
Nevertheless, several controversies remain regarding TMpE. The anatomical definition of the mesopancreas has not reached universal consensus, with varying descriptions proposed by different authors [21]. Consequently, the optimal extent of TMpE remains a subject of debate. Moreover, different surgical approaches to TMpE have been suggested, and an internationally standardized technique has yet to be established [22]. Furthermore, some studies have reported increased morbidity, including refractory diarrhea and lymphorrhea following TMpE, which may delay the initiation of adjuvant chemotherapy [21,23].
The present study aimed to compare the early postoperative outcomes of pancreatic head PDAC patients who underwent PD with TMpE versus conventional PD (Co-PD) in our institution.
2. Patients and Methods
2.1. Ethical Approval and Patient Selection
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Dokuz Eylul University (Protocol code: 2025/06-26 and date of approval: 19 February 2025). This study was approved by the institutional ethics committee. Patients who underwent pancreaticoduodenectomy (PD) for pancreatic head cancer in our clinic between January 2021 and December 2024 were retrospectively reviewed. Among these, only patients with a pathological diagnosis of pancreatic ductal adenocarcinoma (PDAC) were included. Informed consent was obtained from all patients involved in the study. Patients were stratified into two groups: those who underwent PD with total mesopancreatic excision (TMpE-PD) and those who underwent conventional PD (Co-PD). All procedures were performed by experienced surgeons within our hepatopancreatobiliary (HPB) surgery unit. While some surgeons preferred the Co-PD technique, others routinely performed TMpE-PD in all eligible cases.
2.2. Surgical Technique
In patients undergoing conventional PD (Whipple procedure), the standard, previously described surgical technique was applied [24]. In TMpE-PD cases, surgery was initiated with an artery-first approach. Following a wide Kocher maneuver, the superior mesenteric artery (SMA) was dissected posteriorly, encircled, and suspended. The dissection was extended distally via the uncinate process, allowing both distal and proximal control of the SMA (Figure 1 and Figure 2). Dissection proceeded in a caudo-cranial manner along the pancreatic border toward the SMA origin, at which point the artery was assessed for tumor invasion.
If no invasion was detected, the tissue plane between the SMA and pancreas was dissected as close as possible to the arterial wall, leaving the mesopancreatic specimen en bloc. At this stage, the inferior pancreaticoduodenal artery (IPDA) and its branches were ligated and divided (Figure 3). The first jejunal vein (FJV) was preserved unless invaded by tumor, in which case it was ligated and divided. Similarly, branches of the first jejunal artery (FJA) were preserved unless infiltration was present, requiring ligation.
During the resection phase, the uncinate process was excised from the retroperitoneum with the mesopancreas included in the specimen (Figure 4).
In cases with SMV invasion, distal and proximal vascular control was established. Following temporary clamping, en bloc resection was performed, and vascular continuity was restored with reconstruction before proceeding with the remaining anastomoses.
In both groups, lymphadenectomy was performed according to the recommendations of the International Study Group of Pancreatic Surgery (ISGPS) [25]. Pancreaticojejunostomy was performed as an end-to-side anastomosis, with the pancreatic capsule sutured to the jejunal seromuscular layer using interrupted 3/0 silk sutures, and duct-to-mucosa anastomosis performed with interrupted 5/0 polydioxanone (PDS) sutures.
Pathological specimens were evaluated macroscopically and microscopically by pathologists specialized in HPB pathology. For macroscopic evaluation, pancreatic surgical margin, retroperitoneal surgical margin, common bile duct surgical margin, and vascular bed surgical margin sampling were performed on all specimens. Microscopic evaluation included tumor type and differentiation, tumor pathologic T and N stages (according to the AJCC 8th Edition), surgical margin status, the number of dissected lymph nodes, and the number of metastatic lymph nodes. All surgical margins were inked, axial slicing of the pancreatic head was performed, and margin reporting followed international consensus definitions. Although no central review was conducted, the pathologists assessing the specimens were blinded to the surgical technique (TMpE vs. Co-PD); therefore, margin evaluation was blinded with respect to surgical approach.
Demographic features, comorbidities, preoperative factors, tumor size, TNM stage, operative time, estimated blood loss, resection margin status (R0 vs. R1), lymph node yield, length of hospital stay, and postoperative complications were recorded. Postoperative complications were classified according to the Clavien–Dindo system [26], with grade III or higher defined as major complications. Postoperative pancreatic fistula (POPF) was classified according to ISGPS criteria [27].
This study evaluated the relationship between surgical techniques and resection margin status (R0/R1) with postoperative complications and investigated risk factors affecting the development of postoperative complications.
2.3. Statistical Analysis
Logistic regression models were built using purposeful selection methods by Hosmer and Lemeshow, with clinically relevant variables retained regardless of univariable significance. Confidence intervals (95% CI) were reported for all effect estimates.
All statistical analyses were performed using jamovi (The jamovi project, Sydney, Australia) software (version 2.6), an open-source statistical package [28]. Normality of distribution for continuous variables was assessed using the Shapiro–Wilk test and visual inspection of Q–Q plots. Continuous variables were expressed as mean ± standard deviation or median (interquartile range), and categorical variables as numbers (percentages). Group comparisons were performed using Student’s t-test or the Mann–Whitney U test for continuous variables, and Chi-square or Fisher’s exact test for categorical variables.
To evaluate prognostic factors associated with complications, clinicopathological variables were first analyzed by univariable methods. Variables with p < 0.25 and those of established clinical relevance were included in the multivariable logistic regression analysis. The purposeful selection method by Hosmer and Lemeshow was applied [29]. Coefficient changes and potential interactions were examined, and clinically significant variables were retained in the final multivariable model. Results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). Two-tailed p values < 0.05 were considered statistically significant.
3. Results
A total of 41 patients were included in the study, of whom 17 (41.5%) underwent TMpE-PD and 24 (58.5%) underwent Co-PD. Demographic and clinicopathological parameters were comparable between the two groups, with no statistically significant differences (Table 1). The median operative time was slightly longer in the TMpE-PD group compared to the Co-PD group (485 min vs. 423 min; p = 0.067). Venous resections and reconstruction were performed in five patients (2 TMpE-PD, 3 Co-PD). Only one of these patients (Co-PD) had received neoadjuvant therapy; in the remaining four cases, vascular resection had not been anticipated preoperatively.
Although not statistically significant, the TMpE-PD group showed higher R0 resection rates (58.8% vs. 45.8%; p = 0.412) and greater lymph node yield (33.9 vs. 29.1; p = 0.757) compared to the Co-PD group. Pancreatic duct diameter and gland texture were similar between groups.
Postoperative outcomes are summarized in Table 2. Overall complication rates were higher in the TMpE-PD group compared with the Co-PD group (82.4% vs. 63.4%; p = 0.034). However, when only surgical complications were considered, there was no significant difference between the two groups (70.6% vs. 58.5%; p = 0.187). Although not statistically significant, the incidence of major complications (Clavien–Dindo grade ≥ III) was lower in the TMpE-PD group compared to the Co-PD group (11.8% vs. 25.0%; p = 0.414).
Readmission within the first 30 days occurred in one patient (5.9%) in the TMpE-PD group and three patients (12.5%) in the Co-PD group (p = 0.628). Clinically relevant POPF (Grade B–C) rates were low and comparable between the groups (TMpE-PD 5.9% vs. Co-PD 8.3%; p = 1.000). Chylous fistula developed in two patients (14%) in the TMpE-PD group, whereas none occurred in the Co-PD group. Neither group experienced delayed gastric emptying, refractory diarrhea, or post-pancreatectomy hemorrhage affecting clinical course.
Overall, hospital mortality due to POPF occurred in two patients (4.8%), one from each group. Additionally, two further deaths (4.8%) occurred in the Co-PD group within 90 days postoperatively, both related to comorbidities.
Analysis of parameters potentially associated with postoperative complications revealed no statistically significant predictors (Table 3).
Only a smaller pancreatic duct diameter was identified as a risk factor approaching statistical significance (p = 0.053).
After the initial evaluation, variables with p values < 0.25, including sex (OR:2.57 CI 0.69–9.55, p = 0.158), pathological stage (OR:2.73 CI 0.72–10.27, p = 0.138), and pancreatic duct diameter (OR:0.75 CI 0.56–1.00, p = 0.053) were selected for further models. The adjusted model also included pancreatic gland texture (OR:3.00 CI 0.44–20.44, p = 0.262) due to its known clinical importance.
In multivariable logistic regression analysis, the surgical technique (TMpE-PD vs. Co-PD) was not found to be an independent risk factor for the development of postoperative complications (OR: 0.64; 95% CI: 0.14–2.83; p = 0.56). Similarly, no direct association was observed between resection margin status (R0 vs. R1) and complication development (Table 4).
Discussion
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive malignancies, with approximately 80% of cases located in the pancreatic head [30,31]. In eligible patients, surgical resection with R0 margins remains the most effective treatment option [2,3,4,5]. Pancreaticoduodenectomy (PD) is the standard surgical procedure for pancreatic head adenocarcinomas, and technical advancements and modifications have been introduced over the years [32]. Nevertheless, even in patients undergoing curative-intent PD, early recurrence rates of 59.7–91.1% have been reported, most frequently attributed to R1 resection margins [33,34].
Total mesopancreatic excision (TMpE) has been proposed as a surgical technique with the potential to improve R0 resection rates and thereby reduce locoregional recurrence [16]. Excision of the mesopancreas during PD has been advocated to achieve more favorable oncological outcomes [17,35]. However, the definition of the mesopancreas remains controversial, with varying descriptions proposed by different authors [36,37,38]. As a result, no consensus has yet been reached regarding the optimal extent of TMpE. Furthermore, the absence of adequately powered randomized controlled trials limits the evidence on the efficacy and safety of TMpE [22].
Early reports of TMpE emphasized artery-first approaches to PD, particularly dissection beginning with the superior mesenteric artery (SMA) [18,20]. The artery-first approach offers several advantages, including early assessment of arterial invasion and avoidance of unnecessary resection in non-resectable cases [39]. For TMpE-PD, this strategy is regarded as technically advantageous. Studies comparing TMpE-PD with Co-PD have reported higher rates of R0 resection and greater lymph node yield with TMpE-PD. In a recent meta-analysis, Silva et al. also demonstrated that TMpE-PD achieved significantly higher R0 resection rates and lymph node retrieval compared with Co-PD [22].
Despite its potential oncological benefits, TMpE is associated with certain disadvantages. The procedure requires meticulous dissection along the adventitial plane of the SMA, which increases technical complexity and may prolong operative time. Furthermore, the more extensive dissection of the mesopancreatic tissue has the potential to increase perioperative morbidity. Extensive dissection around the SMA has been associated with potential morbidity, including refractory diarrhea and high-output chylous leakage due to neural and lymphatic injury [20,21,22,23]. For this reason, several authors have emphasized the need to avoid overly aggressive dissection. Refractory diarrhea not only increases morbidity but also delays the initiation of adjuvant chemotherapy [40,41,42]. Some reports have suggested that early use of antidiarrheal agents may help manage this complication [22,43]. In our series, no patients in the TMpE-PD group developed refractory diarrhea. In patients who developed diarrhea, dietary modifications, probiotics, and antidiarrheal medications were effective for symptom control. Chylous fistula occurred in two patients (14.8%) in the TMpE-PD group but in none of the Co-PD group, consistent with previous reports linking this complication to more extensive lymphatic dissection.
These findings highlight a central dilemma for surgeons: whether to accept an increased risk of postoperative morbidity—particularly refractory diarrhea—in exchange for potentially superior oncological clearance. The decision ultimately depends on defining the optimal extent of mesopancreatic dissection required for TMpE. Although multiple techniques have been described, no universally standardized and internationally accepted definition of the procedure exists to date [17,18,19,20,21,22,44,45,46].
Inoue et al. were the first to describe a systematic supracolic artery-first mesopancreatic excision for periampullary tumors, defining three levels of dissection of increasing extent [47]. They reported that TMpE-PD, compared with Co-PD, was associated with reduced operative time and blood loss. More recently, Nagakawa et al. proposed a refined TMpE technique based on four intense neurofibrous tissue (NFT) zones around the SMA (A, B, C, D areas), which provided a structured framework for dissection [48]. Compared with conventional PD, this approach achieved shorter operative times, reduced blood loss, and improved rates of R0 resection and lymphadenectomy.
In our institution, TMpE-PD is performed using a posterior and uncinate process combined artery-first approach, as described in the Methods section. The principle is to achieve early SMA control, assess resectability, and perform PD with en bloc removal of the mesopancreas. The extent of dissection is individualized intraoperatively, with the extension of resection margins determined when tumor infiltration is observed. Thus, oncological advantage is prioritized while balancing the relative risk of increased postoperative morbidity. We believe that in TMpE-PD, the extent of resection should be tailored to each patient based on intraoperative findings.
Considering that all tumors in this study were PDAC, our approach most closely resembles the level 2 dissection described by Inoue et al. Although statistical significance was not reached, TMpE-PD cases demonstrated trends consistent with the literature, including higher R0 resection rates and greater lymph node yields compared with Co-PD cases. In univariable analysis, overall complications were more frequent in the TMpE-PD group; however, when limited to surgical complications, no significant differences were observed. Moreover, major complications (Clavien–Dindo grade ≥ III) were more frequent in the Co-PD group. Multivariable logistic regression analysis demonstrated no significant differences in postoperative complication rates between the two groups. Similarly, no relationship was found between resection margin status (R0 vs. R1) and complication development. These findings suggest that more aggressive dissection to achieve R0 resection does not necessarily translate into higher postoperative morbidity. Among all cases, only a smaller pancreatic duct diameter approached significance as a risk factor for complications.
This study has several limitations. Its retrospective, single-center design and relatively small sample size limit the generalizability and statistical power of the findings. The retrospective, single-center design and relatively small sample size inherently limit causal inference and statistical power. The absence of propensity score matching may introduce selection bias. Different surgeons performed each technique, creating potential performance bias. Neoadjuvant therapy was underrepresented, reducing generalizability. Long-term outcomes (recurrence, survival) were not available due to short-term analysis. The regression model was exploratory and not validated.
4. Conclusions
Total mesopancreatic excision (TMpE) represents a promising surgical strategy for pancreatic head PDAC, offering improved locoregional clearance and the potential for superior oncological outcomes. Our findings, consistent with the current literature, suggest that TMpE-PD provides oncological advantages without increasing the risk of postoperative morbidity. However, the optimal extent of TMpE remains undefined, and further high-quality, multi-center studies with standardized protocols are warranted to establish international consensus and strengthen the evidence base. In conclusion, TMpE demonstrated non-significant trends toward higher R0 resection rates and greater lymph node yields compared with conventional PD. While these findings suggest potential oncologic benefit, definitive conclusions cannot be drawn from this dataset. Further multi-center prospective studies with standardized protocols are necessary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Are C. Dhir M. Ravipati L. History of pancreaticoduodenectomy: Early misconceptions, initial milestones and the pioneers HPB 20111337738410.1111/j.1477-2574.2011.00305.x 21609369 PMC 3103093 · doi ↗ · pubmed ↗
- 2Conroy T. Pfeiffer P. Vilgrain V. Lamarca A. Seufferlein T. O’Reilly E.M. Hackert T. Golan T. Prager G. Haustermans K. Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up Ann. Oncol.202334987100210.1016/j.annonc.2023.08.00937678671 · doi ↗ · pubmed ↗
- 3Neoptolemos J.P. Stocken D.D. Friess H. Bassi C. Dunn J.A. Hickey H. Beger H. Fernandez-Cruz L. Dervenis C. Lacaine F. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer N. Engl. J. Med.20043501200121010.1056/NEJ Moa 03229515028824 · doi ↗ · pubmed ↗
- 4Okusaka T. Nakamura M. Yoshida M. Kitano M. Ito Y. Mizuno N. Hanada K. Ozaka M. Morizane C. Takeyama Y. Clinical Practice Guidelines for Pancreatic Cancer 2022 from the Japan Pancreas Society: A synopsis Int. J. Clin. Oncol.20232849351110.1007/s 10147-023-02317-x 36920680 PMC 10066137 · doi ↗ · pubmed ↗
- 5Springfeld C. Ferrone C.R. Katz M.H.G. Philip P.A. Hong T.S. Hackert T. Büchler M.W. Neoptolemos J. Neoadjuvant therapy for pancreatic cancer Nat. Rev. Clin. Oncol.20232031833710.1038/s 41571-023-00746-136932224 · doi ↗ · pubmed ↗
- 6Strobel O. Neoptolemos J. Jäger D. Büchler M.W. Optimizing the outcomes of pancreatic cancer surgery Nat. Rev. Clin. Oncol.201916112610.1038/s 41571-018-0112-130341417 · doi ↗ · pubmed ↗
- 7Pedrazzoli S. Di Carlo V. Dionigi R. Mosca F. Pederzoli P. Pasquali C. Klöppel G. Dhaene K. Michelassi F. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: A multicenter, prospective, randomized study Ann. Surg.199822850851710.1097/00000658-199810000-000079790340 PMC 1191525 · doi ↗ · pubmed ↗
- 8Augustinus S. Schafrat P.J.M. Janssen B.V. Bonsing B.A. Brosens L.A.A. Busch O.R. Crobach S. Doukas M. van Eijck C.H. van der Geest L.G.M. Nationwide impact of centralization, neoadjuvant therapy, minimally invasive surgery, and standardized pathology reporting on R 0 resection and overall survival in pancreatoduodenectomy for pancreatic cancer Ann. Surg. Oncol.2023305051506010.1245/s 10434-023-13465-937210448 PMC 10319672 · doi ↗ · pubmed ↗