Natural Molecules, Nutraceuticals, and Engineered Nanosystems: A Comprehensive Strategy for Combating Gardnerella vaginalis-Induced Bacterial Vaginosis
Manoj Dalabehera, Abdulrahman Mohammed Alhudhaibi, Emad M. Abdallah, Tarek H. Taha, Shubham Chaudhari, Alka Kumari, Rudra Narayan Subudhi, Charul Rathore

TL;DR
This paper explores natural compounds and nanotechnology as new ways to treat bacterial vaginosis caused by Gardnerella vaginalis, aiming to improve on current antibiotic treatments.
Contribution
The paper introduces a novel strategy combining natural molecules and nanosystems to combat drug-resistant Gardnerella vaginalis infections.
Findings
Natural compounds and nutraceuticals show antibacterial and antibiofilm properties against G. vaginalis.
Engineered nanosystems enhance the delivery and efficacy of these natural agents.
Nature-inspired therapies demonstrate superior in vitro and in vivo performance compared to traditional antibiotics.
Abstract
Bacterial vaginosis (BV) is a highly prevalent vaginal infection characterized by a dysbiotic shift in the vaginal microbiota, with Gardnerella vaginalis acting as a principal pathogen. Despite its association with adverse reproductive outcomes, BV remains underexplored from both mechanistic and therapeutic standpoints. Standard antibiotic regimens frequently fail due to high recurrence rates driven by multidrug-resistant (MDR) G. vaginalis strains and biofilm formation. In response, natural compounds and nutraceuticals, owing to their intrinsic antibacterial, antibiofilm, and immunomodulatory properties, have emerged as promising candidates for alternative BV therapies. In this paper, we first compile and critically evaluate preclinical and clinical evidence on the efficacy of plant extracts, essential oils (EOs), probiotics, vitamins, proteins, fatty acids, and enzymes against G.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
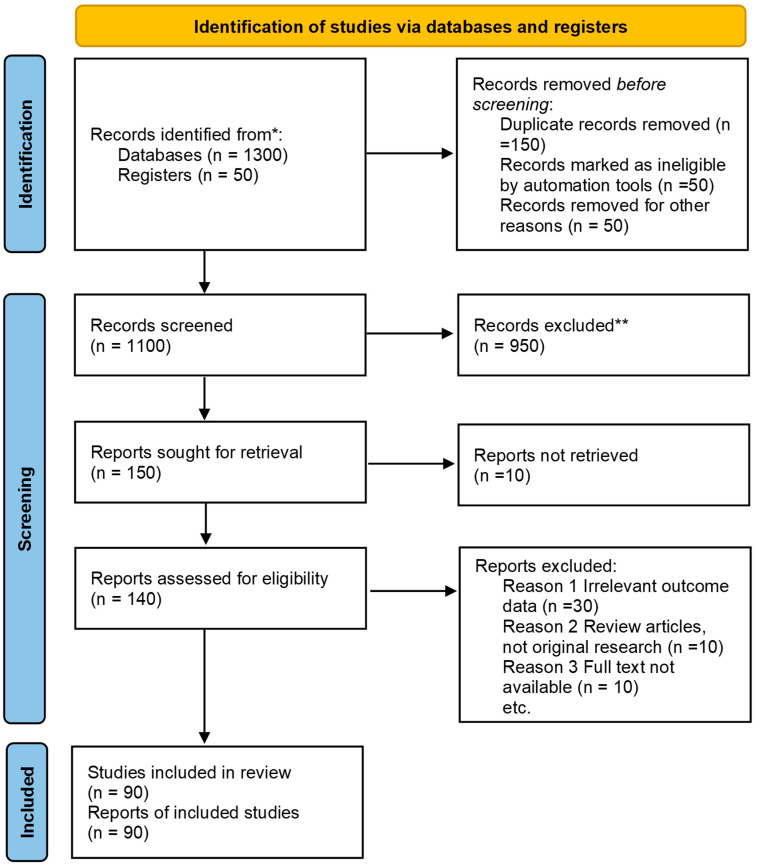 Figure 1
Figure 1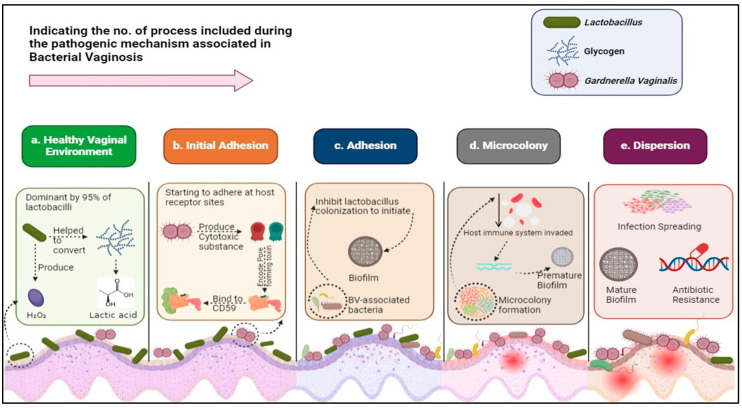 Figure 2
Figure 2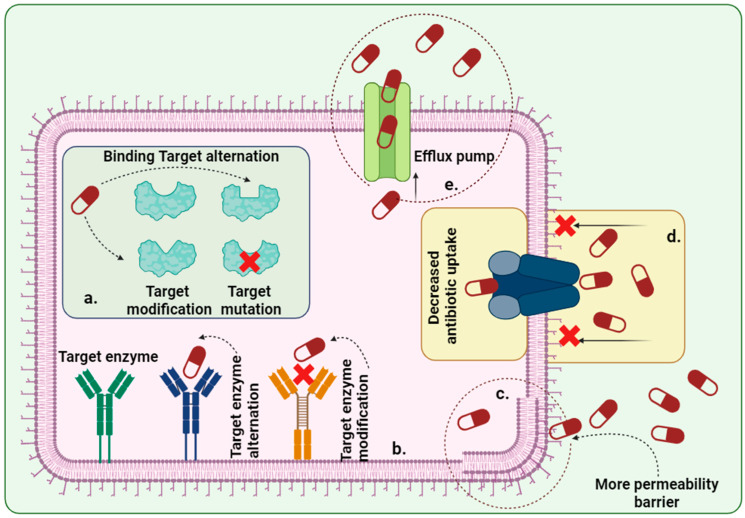 Figure 3
Figure 3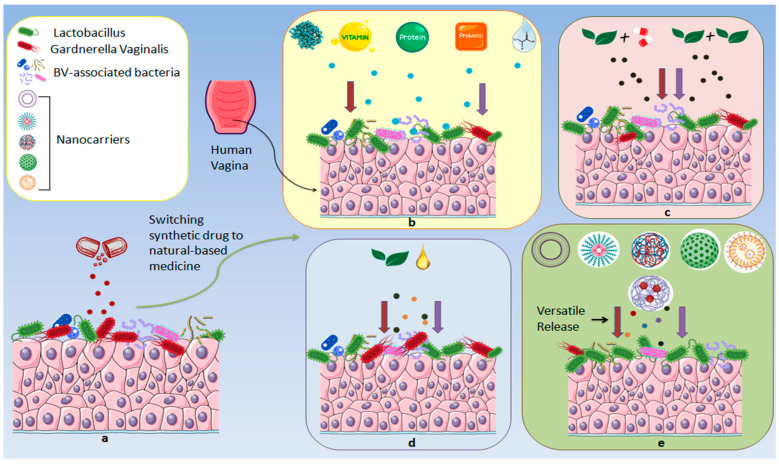 Figure 4
Figure 4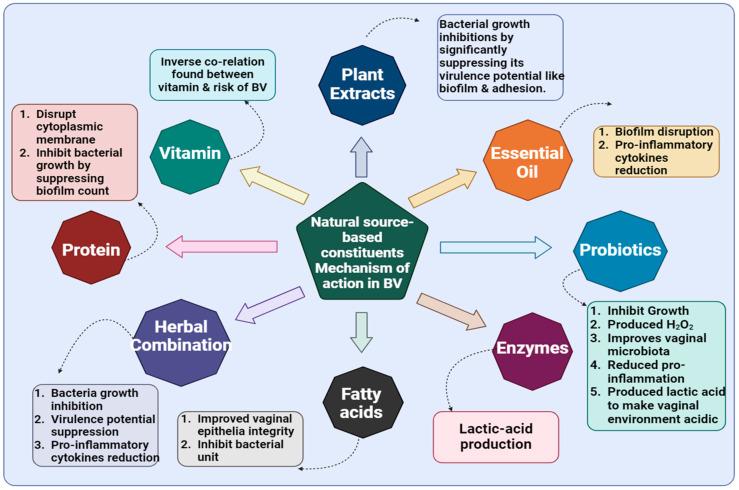 Figure 5
Figure 5| Sl. No. | Combination | Performed Assay/Method | Strains Used | Types of Study | Outcomes | References |
|---|---|---|---|---|---|---|
| Live Bacteria | ||||||
| 1. | Detection of H2O2 Production Study, Analysis of LA Production, Antibacterial Effects of | In vitro (HeLa cell line used) and In Vivo (C57BL/6) | Synergistic potential against | [ | ||
| 2. | Inhibition and Disaggregation of | In vitro | Promising inhibition and disruption of bacterial biofilm were observed. | [ | ||
| 3. | Assay for the Inhibitory Effects of Probiotics Against the Growth of | In vitro (HeLa cells) and In vivo (C57BL/6) | Probiotics comprising a combination of this spp. exhibited desired killing activity against | [ | ||
| 4. | MTZ and oral probiotics (prOVag) | Antibacterial Study |
| Multicentre, randomized, double-blind, placebo controlled trial ( | Clinical and microbiological parameters of BV were improved by this combination. | [ |
| Natural Molecules | ||||||
| 1. | CFU Evaluation, MPO Activity, SLD Activity Assay, MucoadhesionStudy | In vivo (C57BL/6 mice model) | This combination improved vaginal tissue architecture while suppressing bacterial invasion. | [ | ||
| 2. | Antimicrobial Bioassay, Synergy Analysis |
| In vitro | Additive antibacterial activity was demonstrated. | [ | |
| 3. | Carvacrol, α-terpinene, γ-terpinene, ρ-cymene, and linalool | Vaginal Irritation Test, Biofilm Biomass Quantification by Crystal Violet Staining Method, Checkerboard Method for Fractional Inhibitory Concentration | In vitro (Human Vaginal Epithelium (HVESkinEthic) | No cytotoxicity was observed in the tested vaginal tissue. | [ | |
| 4. | Acetic acid and LA (intravaginal combination therapy) | Antimicrobial Study | Patients with vaginal infection | Double blinded randomized controlled feasibility trial (ACTRN 12620001084976) | The BV recurrence rate had drastically reduced. | [ |
| 5. | Subtilosin and glycerol monolaurate | Checkerboard Assays, Antimicrobial Assay | In vitro (first time performed) | From MIC 4.6–25 μg/mL, this herbal combination showed 4-fold growth inhibition of | [ | |
| 6. | Antibacterial Study, Recurrence Assay | Patients with BV | Observational/descriptive study. | 76.9% of patients improved after exposure to combination therapy. | [ | |
| 7. | Antibacterial Study | Patients suffered from BV | Randomized controlled clinical trial (IRCT2016042327534N1) | Recovery of BV in patients was observed. | [ | |
| 8. | Subtilosin and LAE | Bacterial Biofilm Formation Assay, Time Bactericidal Activity of Antimicrobials Against Biofilm-Associated | In vitro | Effective inhibition of | [ | |
| 9. | LAE, e-poly-L-lysine, clindamycin phosphate, and MTZ | Determination of Minimal Inhibitory Concentration (MICs), Checkerboard Assays, and Antibacterial Study | In vitro | Potential antibacterial activity was noticed. | [ | |
| Sl. No. | Types of Performed Study | Experimental Types | Antibacterial Against | Key Findings | References | ||
|---|---|---|---|---|---|---|---|
| 1. | 1. AntiSLD assay | In vitro (HeLa) and in vivo (murine model) |
| Potential improvement of Vaginal epithelial cell exfoliation observed. | [ | ||
| 2. | 1. Measurement of cytokines in vaginal tissues | In vitro (HeLaand in vivo (C57BL/6) | This probiotics strain provided the desired anti- | [ | |||
| 3. | Serum carotenoids | Antibacterial study | Cross-sectional | Patients (1252) suffered from BV | Serum carotenoids were found to be negatively associated with BV. | [ | |
| 4. | VagiBIOM | 1. Vaginal swabs, DNA isolation, and microbiome analysis | Randomized, double-blind, placebo-controlled pilot study ( | Patients (92) | Beneficial effects on the vaginal microbiome are demonstrated. | [ | |
| 5. |
| 1. SLD activity assay | In vitro (A-431 and HeLa cell lines) andin vivo (C57/Bl6 female mice) | Significant inhibition of | [ | ||
| 7. | 1. Antibacterial activity of | In vitro (HeLa cell line), a randomized, double-blinded trial ( | Promising bacterial adhesion inhibition observed. | [ | |||
| 8. | 1. Co-aggregation assay | In vitro (HeLa cell line) | This study demonstrated that gene expression related to | [ | |||
| 9. | 1. Evaluation of the ameliorative effect of | In vivo (Female C57BL/6 mice) | [ | ||||
| 10. | Probiotic | 1. Histopathological analysis | In vivo (seven-week-old 57BL/6J female mice) | [ | |||
| 1. Auto-aggregation and co-aggregation assays | In vitro (HMVII, a vaginal epithelial cell line (BCRJ 0316)) | Vaginal microbiome improved. | [ | ||||
| 1. Antibacterial tests in vitro by agar spot and well diffusion tests | In vitro | Upregulation of the transcription levels of antimicrobial resistance genes in | [ | ||||
| 11 | LA | 1. Lactate dehydrogenase (LDH) assay | In vitro (VK2 E6/E7 (Vk2) vaginal epithelial cell line) |
| Vaginal microbiome improved. | [ | |
| 1. LA determination | In vitro | Vaginal pathogens, including | [ | ||||
| 1. Histopathological examination | In vivo (Female BALB/c) | Significant growth inhibitions of the tested bacteria were observed. | [ | ||||
- —Imam Mohammad Ibn Saud Islamic University (IMSIU)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive tract infections research · Reproductive System and Pregnancy · Urinary and Genital Oncology Studies
1. Introduction
As one of the most prevalent vaginal disorders worldwide, bacterial vaginosis (BV) affects nearly 30% of women of reproductive age and exhibits recurrence rates exceeding 50% within six months due to the rise in the antibiotic-resistant Gardnerella vaginalis strain [1,2]. Vaginal dysbiosis has been linked to an increased risk of HIV and other sexually transmitted infections, as well as pelvic inflammatory disease. Additionally, it has been connected to negative pregnancy outcomes, including preterm delivery and infections in both mothers and newborns [3].
BV is a dysbiosis of the vaginal microbiota that is defined by a change in the dominance of different anaerobic bacteria from Lactobacilli [4,5]. It is the most prevalent vaginal condition in women who are of reproductive ageworldwide and is identified as a clinical condition in which there is an overgrowth of bacteria in the vagina, resulting in a thin, gray/off-white, homogenous, and malodorous adherent secretion from the vagina [6,7,8]. This discharge is more noticeable after sexual activity and menstruation and has a pHhigher than 4.5 [9]. It also has an unpleasant fishy smell, with the patient’s most common complaint being itching in the perineal area [10,11]. Bacteria, namely G. vaginalis, Atopobium vaginae, Megasphaera phylotypes, Leptotrichia aminionii, Mobiluncus spp., Prevotella spp., Mycoplasma hominis, Bacteroides spp., and Sneathia, are among the causative spp. that have been found in recent studies to be responsible for BV [12,13].
G. vaginalis is also associated with adhering to vaginal epithelial cells, forming “clue cells,” which are diagnostic for BV. BV is often asymptomatic, but about half of affected individuals report malodor and mild irritation. This microorganism is a small, non-spore-forming, nonmotile Coccobacillus that displays Gram-variable staining due to its thin cell wall. G. vaginalis is known for biofilm formation, which enhances its persistence and resistance within the vaginal ecosystem. The bacterium produces virulence factors such as vaginolysin, proteases, and sialidase (SLD), contributing to tissue colonization and immune evasion.
Metronidazole (MTZ) is a first-line antibiotic for BV, but G. vaginalis exhibits considerable resistance, especially in recurrent cases. Approximately 68% of isolates resist MTZ, while most remain sensitive to clindamycin. Genomic studies have identified specific clades intrinsically resistant to MTZ, which correlates with treatment failures. Biofilm formation further contributes to poor antibiotic penetration and increases recurrence. Recurrence of BV, predominantly driven by Gardnerella vaginalis, is common following standard MTZ therapy. More than 50% of treated women experience recurrence within 6–12 months, particularly those with behavioral risk factors such as inconsistent condom use or retention of pretreatment sexual partners. Biofilm resilience and the presence of MTZ-resistant clades are significant contributors to recurrence.
It is projected that the global cost of treating symptomatic BV may reach $4.8 billion in the future, as it is the most frequent vaginal infection occurring in females [14,15,16]. Oral or intravaginal administration of the currently recommended first-line antimicrobial agents, including MTZ and clindamycin, is a widely used therapy for BV. These agents provide broad-spectrum activity against anaerobic bacteria associated with the condition [17]. However, due to limitations such as multidrug resistance (MDR), severe adverse events, and recurrence complaints, there is a demand for steering towards constituents derived from natural sources, which might stand a chance as an alternative approach [18,19,20]. Moreover, the integration of nanomaterials provides the desired therapeutic activity by sidestepping negative attributes associated with naturally based molecules, which may prove to be a useful asset in addressing the problem of BV recurrence [21,22].
The current study aims to outline and critically discuss emerging MDR patterns in G. vaginalis-induced BV, identify and characterize novel bioactive molecules from natural sources, and evaluate the potential of nano-enabled herbal formulations for targeted, sustained vaginal delivery. Additionally, we critically appraise clinical trial evidence on herbal and nutraceutical interventions to determine their efficacy, safety, and impact on recurrence rates, while mapping the global patent landscape to underscore recent innovations in this field.
2. Methodology
In this paper, we performed a systematic literature review (Registration No.CRD420251089821, PRISMA checklist in the Table S1) of peer-reviewed articles, clinical trial reports, and patent filings published up to May 2025, sourcing records from The Lancet, PubMed, Springer, ScienceDirect, Nature, Taylor and Francis, Google Scholar, the WIPO PatentScope database, and major clinical trial registries. Search terms included “bacterial vaginosis,” “G. vaginalis,” “antibacterial resistance,” “natural bioactives,” “nutraceuticals,” “nanoherbal formulations,” “herbal clinical trials,” and “patents.” We included original research articles, in vitro and in vivo studies, human clinical trials, and patent documents that explicitly investigated antimicrobial activity against G. vaginalis or BV recurrence, design, and evaluation of nano-enabled herbal delivery systems (Figure 1).
Exclusion criteria comprised non-English publications, conference abstracts lacking full text access, studies focused on non-vaginal pathogens or synthetic compounds only, articles with low methodological quality, and patents without demonstrable utility data. Retrieved records were screened by title and abstract, and full texts were assessed independently by two reviewers; disagreements were resolved through consensus.
3. Mechanisms of Gardnerella vaginalis Pathogenicity
BV is also known as nonspecific G. vaginalis, and its pathogenic mechanism occurs due to the replacement or displacement of Lactobacillus spp. by an increase of 100 to 1000 times of various aerobic and anaerobic facultative bacteria; however, G. vaginalis is primarily involved throughout the process [23,24]. In a healthy vagina, Lactobacillus maintains the homeostasis of vaginal microbiota by converting glycogen (produced by vaginal epithelial cells with the assistance of α amylase) into lactic acid (LA), which further helps maintain an acidic medium in the vagina [4,25]. An acidic medium is highly suitable for preventing bacterial overgrowth; moreover, Lactobacillus spp. also produces hydrogen peroxide (H_2_O_2_), which inhibits other anaerobic bacteria, including G. vaginalis, as it is an important element in the vaginal defense system [26,27]. Lactobacillus also enhances vaginal flora by producing antimicrobial and anti-inflammatory products like bacteriocins and biosurfactants (Figure 2, step 1) [28].
Research indicates that several risk factors and behaviors are linked to pathogenic initiation of BV, such as age, marital and employment status, occupation, multiple exposure of antibiotics, reduced host estrogen production, sexual activity, younger age at first intercourse, more frequent episodes to receptive oral sex, use of spermicides, STDs, working in the sex industry, contraceptive use, frequency of vaginal intercourse, and race/ethnicity [1,29,30,31,32]. In step 2, G. vaginalis and other BV-associated bacteria (BVAB), like Prevotella, Mycoplasma, Ureaplasma, and Mobiluncus spp., initially adhere to the vaginal epithelium and produce vaginolysin and cholesterol-dependent cytolysin, which helps suppress the host’s innate immune response [33,34]. These cytotoxic substances further encode a pore-forming toxin, which binds the host’s complementary regulatory molecule CD59 [35,36]. In step 3, G. vaginalis promotes P. bivia growth, and these two bacteria produce an enzyme like SLD, which degrades the vaginal epithelium mucin layer [37]. Bacterial adhesion interacts between cell appendages, carbohydrates, and cell surfaces to initiate biofilm while inhibiting Lactobacillus colonization in the vaginal micro-ecosystem [38,39]. During this process, theBapL protein in G. vaginalis is highly expressed, which helps to initiate bacterial biofilm production [28,40]. In step 4, in the early stage, G. vaginalis and Prevotella are first to initiate microcolony formation while continuously changing normal Lactobacillus, which later helps to facilitate BVAB to provide a simultaneously anaerobic vaginal environment to favorably disrupt the host epithelial barrier [41]. After the successful formation of a microcolony, extracellular DNA in G. vaginalis stimulates the production of extracellular matrix (EPS), which further provides structural stability and integrity to biofilm [42,43]. This colony formation jeopardized the host’s inflammatory and immune system to the biofilms [41]. In step 5, infections are ready to spread [44]. Biofilm helps bacteria by not allowing them to be fully killed or removed by antibiotics and the host immune system; therefore, the persistent presence of bacterial biofilm further causes the recurrence of BV [45,46]. In this stage, clinical symptoms of BV, including vaginal discharge, appear in women’s vaginas (Figure 2) [25,40,47].
4. Characterizing the Resistance Profile of Gardnerella vaginalis
Various currently available marketed medicines are used for the management of BV. However, due to multiple exposures and fast-developing resistance, it is necessary to adapt natural-based constituents and integrate them with nanomaterials for better therapeutic purposes [9,39]. Table 1 lists a compilation of current drug formulations with various adverse events. According to various established reports, bacterial resistance occurred due to drug molecules not reaching target sites and target enzymes because of target site, enzyme modification, and mutation, respectively [48]. Another reason for resistance is the pumping out of antibiotic constituents from the bacterial cellular membrane through efflux pumps and decreasing their uptake, so that the concentrations of drug molecules decrease and their antibacterial efficacy [49,50]. Bacterial membrane permeability is also an important factor for drug resistance, leading to a smaller amount of drug entering the membrane (Figure 3) [51].
5. Naturally Derived Agents Against BV
There are various molecules derived from natural sources, such as plants and microorganisms, that have been proven to have promising therapeutic activity in BV (Table 1). Moreover, Table 2 lists the synergistic activity of various naturally sourced molecules with potential relevance to G. vaginalis.
5.1. Synergistic Applications of Herbal Therapies
5.1.1. Live Bacteria
Naturally sourced constituents and their combination have emerged as having promising antibacterial activity, which outcomes could sidestep current conventional therapies’ associated side effects and MDR [63,64,65]. However, synergistic data, specifically if steering into molecules derived from natural sources, has not yet been explored across BV. In this section, we have compiled various studies. For instance, Choi et al. [64] investigated the effect of Lactobacilli strains (Ligilactobacillus salivarius, Limosilactobacillus fermentum, Lactiplantibacillus plantarum, Lacticaseibacillus paracasei, and Lacticaseibacillus rhamnosus) in HeLa cells and a G. vaginalis-infected mouse model. In this study, it has been demonstrated that maximum production of H_2_O_2_ and LA was observed with inhibition of G. vaginalis growth up to 80%. This combination was orally administered to infected C57BL/6 mice at 5 × 10^8^ and 5 × 10^9^ colony-forming units (CFUs)/mouse daily for 2 weeks. The higher dose notably alleviated G. vaginalis counts in the vaginal tract, reduced neutrophil-associated myeloperoxidase (MPO) activity, and suppressed pro-inflammatory cytokines. Histopathological analysis confirmed the inhibition of vaginal epithelial cell exfoliation without any side effects occurring, which highlights its potential insights in BV [64]. Sabbatini et al., 2020, first demonstrated the antibiofilm properties of Saccharomyces cerevisiae and L. rhamnosus combination. In their study, G. vaginalis biofilm cell inhibition and disaggregation of S. cerevisiae at 10^7^–10^8^ CFU/mL of prepared biofilm were observed after combination therapy administration. Moreover, S. cerevisiae (10^6^ CFU/mL) with MTZ (4 µg/mL) enhanced antibiotic activity. This therapy outlines its mechanism by proteases and inhibition of SLD [65]. Similarly, Jang et al., 2017 [66] investigated oral administration of a probiotic mixture (PM) containing HN001 (L1), Gla 14 (L2), and lactoferrin RCXTM either orally or intravaginally over 14 days at doses of 5 × 10^8^ to 5 × 10^9^ CFU/mouse/day. This investigation aims to evaluate the significant suppression of vaginal dysbiosis. Oral and intravaginal administration of probiotic mixtures has led to the potential alleviation of G. vaginalis-induced cell disruption in vaginal epithelial cells, demonstrating its anti-BV efficacy without any side effects being noticed. Moreover, compared to vaginal administration, oral administration of PM was found to be more effective in terms of regulating both vaginal and systemic innate modulating (suppression of NF κB activation, MPO activity) and adaptive immunity (downregulation of Th17 marker RORγt and upregulation of Treg marker Foxp3) [66]. This clinical study demonstrated a combination of probiotics with conventional treatment for BV and aerobic vaginitis. Heczko et al., 2015, evaluated 578 women with recurrent episodes of BVAV. Participants were orally administered (500 mg twice daily for 7 days) plus either a probiotic (prOVag^®^) or a placebo. The probiotic contained three strains: L. fermentum 57A, L. plantarum 57B, and L. gasseri 57C (≥10^8^ CFU). Results showed that probiotic supplementation extended the symptom-free interval by up to 51% (mean 71.4 vs. 47.3 days, p = 0.0125), with potential actions (76%) in patients with MTZ-resistant G. vaginalis (p = 0.0053). Additionally, the probiotic group demonstrated speedy recovery of Lactobacillus counts, compared to the placebo [67].
5.1.2. Natural Molecules
Scuderi et al., 2023, have investigated the therapeutic efficacy of pea protein, grape seedextract, and LA combination (daily intravaginal dose of 0.2 g/mouse for 7 days) and its mechanistic insights. The results revealed a significant reduction in G. vaginalis proliferation and a significant reduction (35.85% in CFU for pretreatment vs. 11% for posttreatment) in the number of neutrophil infiltrations, SLD activity, and inflammatory markers. Due to its bioadhesive property, the product containing grape seed extract, LA, and pea protein can be used as an alternative treatment approach in the future [68]. Donkor et al., 2023, have demonstrated the combined activity of Senna alata, Ricinus communis, and Lannea barteri extracts, and the minimum inhibitory concentration (MIC) of this was found to be significantly lowered as compared to the individual value. Notably, combinations like L. barteri aqueous + S. alata ethanol and S. alata aqueous + R. communis ethanol showed synergy (FICI ≤ 0.5). For E. coli (0.97 to 1.17 mg/mL), S. aureus (0.97 to 4.69 mg/mL), P. aeruginosa (0.50 to 1.17 mg/mL), K. pneumonia (1.17 to 3.12 mg/mL) and C. albicans (2.34 to 4.69 mg/mL), it was observed that they might stand a chance as promising antibacterial therapy without any antagonistic interactions [69]. Sousa et al. [70] demonstrated the antibacterial efficacy of Thymbra capitata essential oils (EOs). To study the potential synergistic effect, two EOs of T. capitata were characterized to test their antimicrobial activities. It was found that carvacrol (MIC ~0.04–0.08 µL/mL) and ρ-cymene exhibited a potent synergistic antibacterial effect towards Gardnerella spp. Carvacrol and linalool at sub-MICs were revealed to be more efficient in the elimination of biofilm cells, but no cytotoxicity was found, further extending exploration necessity [70]. Strydom et al. [71] designed a randomized, double-blind, placebo-controlled feasibility trial on intravaginal combination therapy of 3% acetic acid and 2% LA, and the active groups were noted. A notable reduction in symptomatic recurrence, from a baseline annual mean of 7.9 episodes to ~1 episode, andgood tolerance was noticed during this intervention. Nonetheless, compared to conventional fluconazole (150 mg weekly), which often demonstrates > 50% relapse (denotes the return of infection due to incomplete eradication of the initial causative organism) within 3–6 months and involves systemic side effects, this combination therapy offers a localized, low-risk, drug-free alternative [71]. Noll et al., 2012, in their study, first investigated the combination effect against G. vaginalis, which is a causative agent for BV. It was investigated that subtilosin had a synergistic effect with antimicrobial agents, and it was effective in inhibiting the growth of GV [72]. Mazhar et al., 2017, investigated the safety and therapeutic efficacy of a cranberry extract, Bacillus coagulans, and turmeric extract combination to prevent recurrent episodes. Results showed that the recurrence (referring to new episodes of infection occurring after successful treatment) rate was significantly reduced after administration of combination therapy for 12 weeks [73]. Motlagh A et al., 2017, investigated the efficacy of Prangos ferulacea-based vaginal cream on patients suffering from BV. Authors have demonstrated the elevation of the recovery rate after administration and suppressed instances of resistance to G. vaginalis, which highlights its potential and could be used as an alternative to current medications like MTZ [74]. Algburiet al., 2015, investigated the synergistic effect of subtilosin and lauramide arginine ethyl ester (LAE) against biofilms of G. vaginalis. When used alone, the minimum bactericidal concentration (MBC B) of clindamycin towards G. vaginalis was 20,000 μg/mL, and MTZ was 500 μg/mL. In contrast, combining clindamycin with subtilosin reduced its MBC B more than sixfold (to 2.9 mg/mL), and MTZ combined with subtilosin showed an eightfold reduction in required dose (62.5 μg/mL vs. 500 μg/mL). Similarly, LAE suppressed the doses of antibiotics by enhancing permeability and biofilm penetration. Notably, these combinations inhibit healthy vaginal Lactobacilli biofilms, a significant advantage over antibiotics alone [75]. Noll et al., 2012, first demonstrated the anti-G. vaginalis activity of subtilosin, LAE, e-poly-L-lysine, clindamycin phosphate, and the MTZ combination, and in their study, they observed that significant growth inhibition was noticed with a lower risk of bacterial resistance at lower MIC (2–25 μg/mL). The triple combinations (e.g., subtilosin + LAE + 0.5 × MIC GML) maintained synergy while preserving Lactobacillus viability and significantly inhibiting other pathogens. Mechanistically, these compounds employ membrane disruption, signal interference, and pore formation [76].
5.2. Comparative Study of Natural vs. Synthetic Drugs for BV
Comparative data play a crucial role in understanding potent anti-G. vaginalis action between constituents derived from natural sources and conventional therapies. Moreover, this paragraph of the paper critically analyzed the comparative insights and the necessity of using natural molecules (Table 3).
Khazaeian et al. [77] designed a triple-blind, parallel, randomized clinical trial by randomly allocating subjects into two groups, such as n = 35 (sucrose vaginal gel) and n = 35 (MTZ vaginal gel), to compare their antibacterial effect. Outcomes of their study demonstrated that the presence of vaginal discharge and clue cells was reported to be comparatively suppressed after administration of sucrose gel compared to antibiotic gel comprising MTZ. It was also noticed that both vaginal gels have significantly similar potential; however, the sucrose vaginal gel showed no side effects compared to the conventional one, which significantly highlights its significance as an alternative therapy [77]. Baig et al. [78] compared the anti-G. vaginalis efficacy of Kakrasingi (n = 31) as the intervention group and MTZ (n = 31) as the standard group patients by conducting a randomized (1:1), standard-controlled, single-center study. In their study, investigators noticed that clinical (54.83%), microbiological (51.61%), and therapeutic (51.61%) cure rates improved in the intervention group of patients compared to MTZ (51.61%, 45.16%, and 45.16%), respectively. Although both Kakrasingiand MTZ showed good efficacy, the herbal powder showed effects with no adverse effects, which depicts its promising efficacy compared to conventional [78].
A double-blind, randomized controlled trial was conducted by Afzali et al., 2020, to assess the anti-G. vaginalis potential of Quercus brantii Lindl-loaded vaginal cream (n = 42) and MTZ vaginal gel (n = 42) on reproductive-aged women. Findings of their study were that Quercus vaginal cream showed comparatively more effective potential than gel comprising MTZ, without any side effects. Investigators have also concluded that, for reproductive-aged women, oak gall herbs could give desired antibacterial action and are safely recommended, as three patients who administered MTZ gel exhibited effects like vaginal burning [79]. Similarly, Zare et al., 2018, compared, for the first time, the effects of vaginal cream containing Quercus brantii Lindl. (n = 84) with the MTZ tablet (n = 84) on BV by conducting a randomized clinical trial. Within their investigation, it was found that 73.8% of patients benefited (relieved from clinical symptoms like vaginal discharge, itching, erythema, edema, etc.) after exposure to the herbal cream without any side effects, whereas in the MTZ group, there were only 50% of patients who benefited after the treatment. They have also concluded that Q. Lindl is a potential herb that could be further studied and alternatively used in the future for desired antibacterial effects [80].
Durićet al., 2021, assessed a controlled clinical study by randomly allocating women into two groups (Group A—113 and Group B—97) by preparing formulations like VagitoryA (Calendulaeextractumoleosum, Bursae pastoris, Hypericiextractum, Millefoliiextractum), VagitoryB (TTO), and VagitoryC (H. extractum). In this present study, researchers have compared these herbal vagitories with each other and probiotics to characterize their antibacterial efficacy in BV. From the results data, it was found that only mild dryness in the vagina was observed in women after contact with TTO administration. Except for that, all vagitories exhibited positive effects on clinical symptoms like vaginal discharge, itching, redness, etc., with no reported serious side effects [81]. Masoudi et al., 2016, have compared the antibacterial therapeutic potential of Myrtus communis and Berberis vulgaris with MTZ vaginal gel in infected married women by designing a randomized clinical trial. Findings in their study exhibited that the group of patients in M. communis and B. vulgaris reported an effective response than MTZ. Authors also concluded that this herbal-based gel showed desired antibacterial action without any relapse and could be used further, while 30% of patients receiving MTZ experienced a relapse action [82]. Shabanianet al., 2019, designed a double-blind clinical trial to compare the antibacterial potential of B. vulgaris gel (intervention group) with MTZ gel by allocating women into two groups. Results in the present study showed that patients taking the herbal-based gel reported a continuous improvement of symptoms after 7 days than the synthetic drug. Moreover, after 21 days of intervention, total removal of symptoms associated with recurrent episodes was observed by the researcher. Investigators also demonstrated that B. vulgaris gel showed potential antibacterial effects and could be used in the future across vaginal infections [83]. The present study aims to compare the therapeutic antibacterial efficacy of garlic-loaded tablets with oral MTZ by designing a randomized controlled clinical trial on 120 married women. Outcomes from their study unfolded as both treatments showed better effects, but considering side effects and complications associated with MTZ, the investigator concluded that herbal-based therapy could be a potential alternative in the future (Mohammadzadeh et al., 2014) [84]. Wijgert et al., 2020, performed a comparative study between vaginal probiotics containing Lactobacilli with standard MTZ-based treatment to evaluate their potential in recurrence episodes. In their study, lower recurrence rates were observed after probiotic exposure, as it is known to improve vaginal microbiota [76]. Hakimi et al., 2017, conducted a triple-blind randomized controlled study to compare a probiotic-loaded vaginal gel with an oral MTZ tablet in recurrent cases. Results exhibited that, after 90 days of probiotic treatment, an 84% healing rate was observed in women, whereas only 62% improvement was noticed in the MTZ group [85]. Critically comparing this to conventional treatments, antibiotics like MTZ or clindamycin, though effective in short-term pathogen clearance, often lead to recurrence rates exceeding 50% due to disruption of normal flora and lack of microbiota restoration. In contrast, LM5 addresses both infection control and ecological restoration of the vaginal microbiome. These natural molecules support the superior mucosal protection, anti-inflammatory activity, and biofilm disruption capability of natural agents over conventional antibiotics. Importantly, these natural compounds did not damage reconstituted human vaginal epithelial tissues, and no bacterial recovery was observed even after 24 h in fresh medium, suggesting long-lasting antimicrobial action.
6. Nutraceutical Approaches to BV: Focus on Probiotic Strains (L. gasseri, L. helveticus, L. rhamnosus, L. acidophilus, L. plantarum, L. delbrueckii, L. fermentum, and L. salivarius)
According to various established reports, nutraceuticals nowadays have exhibited desired antibacterial efficacy in vaginal infections, i.e., BV [86,87,88]. Daily life nutraceuticals have emerged as having promising anti-G. vaginalis efficacy by maintaining vaginal microflora; therefore, in this section, we have discussed potential nutraceuticals and their mechanistic insights towards G. vaginalis induction. For instance, Zhang et al., 2022, have demonstrated in vitro and in vivo anti-G. vaginalis inhibitory activity of L. gasseri spp. From the in vitro assay, it was revealed that adhesion ability and biofilm formation on the vaginal epithelium were effectively inhibited by L. gasseri. G. vaginalis SLD activity suppression and modulation of interleukin-1β and TNF-α have been observed in an in vivo study. Investigators also concluded that L. gasseri could be a potential alternative treatment option, as it enhances vaginal tissue inflammatory cell infiltration (Table 4) [89].
Kim et al., 2022, have demonstrated in vitro and in vivo antibacterial mechanisms of L. helveticus (HY7801) towards G. vaginalis biofilm formation and epithelial cell adhesion.An in vivoassay confirmed that pro-inflammatory cytokines and G. vaginalis counts in vaginal mucosa have been efficiently suppressed in murine models after exposure to HY7801. This Lactobacillus spp. also helped to boost H_2_O_2_ and maximum LA production in the vagina, observed in an in vitro assay, and downregulated the expression of genes associated with G. vaginalis virulence properties, hence evident to be a promising candidate for BV [90]. Attasi et al., 2010, have evaluated the anti-G. vaginalis potential of LA and demonstrated that, at 100 mM concentration, G. vaginalis showedpromising killing activity. It was also observed by LA, at a 65 mM concentration; LA enhances significant G. vaginalis killing activity of H_2_O_2_ [91]. Li et al., 2023, have loaded LAB strains such as L. crispatus, L. rhamnosus, L. salivarius, and L. plantarum into bacterial consortia transplantation to overcome G. vaginalis-induced BV. This transplantation successfully produced adequate LA and H_2_O_2_, hence regulating the vaginal microbiota. The authors concluded that this might be a potential treatment across BV, but still, more studies are needed to carry out for its successful implementation [92].
Zhi Tan et al., 2024, have investigated the correlation between serum carotenoids like α-carotene, β-carotene, β-cryptoxanthin, lycopene, and lutein/zeaxanthin and the development of BV. Findings showed that all serum carotenoids exhibited an inverse association. It was also noticed that a comparatively lower incidence of BV was shown by α-carotene and β-cryptoxanthin, and β-carotene, followed by a negative correlation amongst all carotenoids [93]. Vivekanandan et al., 2024, have evaluated VagiBIOM Lactobacillus suppository by designing a randomized, double-blind, placebo-controlled pilot study involving patients. Results exhibited that clinical symptoms significantly returned to baseline after a 28-day intervention of herbal therapy administration. Authors also concluded that this VagiBIOM suppository holds tremendous antibacterial activity, which could be an alternative to current standard medication [94]. Sabbatini et al., 2018, have first demonstrated an in vitro and in vivo assay to evaluate the ability of S. cerevisiae-based probiotics against G. vaginalis-induced infections. From the murine model outcome study, it was noticed that SLD and epithelial exfoliation activity effectively inhibited and suppressed G. vaginalis adherence to vaginal mucosa and reduced inflammation without any side effects noticed. Hence, it could be a potential therapeutic alternative and could be used in the future for better outcomes [95]. Lin et al., 2021, have investigated the in vitro antibacterial efficacy of four Lactobacillus strains (L. rhamnosus, L. acidophilus, L. rhamnosus, and L. plantarum), each administered at 1 × 10^10^ CFU daily against G. vaginalis. These treatments exhibited statistically significant reductions in Nugent scores over 4 weeks (e.g., GMNL-74 and GMNL-185 mean reduction from 5.44 to below 3, p < 0.01), with improved clinical symptoms like vaginal discharge color, odor, and itching. From the antimicrobial assay, it was noticed that maximum inhibition (18.27 ± 3.02) and adherence of bacteria to HeLa were exhibited. Additionally, GMNL-74 and GMNL-185 strains comparatively inhibit maximum G. vaginalis adherence capacity and hold potential antibacterial activity against G. vaginalis and could be a suitable alternative therapy to conventional [96].
The present study focused on Lactobacillus strains loaded with probiotics and their anti-G. vaginalis potential across BV treatment. Anin vitro study showed that maximum adherence was exhibited by DM8909 (593 ± 112) and ZX27 (209 ± 13) strains, and produced the highest amount of LA. Gene expression assay showed that all strains effectively alter G. vaginalis genes (gtf, bcrA, mds, vly, and sld), which are associated with biofilm and MDR. Authors have concluded that these probiotic mixtures enable overcoming MDR and hold promising actions [97]. Moon et al., 2022, have investigated the in vitro and in vivo anti-G. vaginalis potential of CH88 cell-free supernatant, and in their study, G. vaginalis growth and biofilm formation were significantly inhibited. Thein vivo assay exhibited significant suppression of CFU in the mice model vaginal fluid and regulated immune response. This research data highlights nutraceutical activity and hence could be used as an alternative to conventional therapy [98].
The present study demonstrated in vivo anti-G. vaginalis activity of three lactic acid-producing bacteria (LAB), such as Ligilactobacillus salivarius MG242, Limosilactobacillus fermentum MG901, and Lactiplantibacillus plantarum MG989 (Kim et al., 2022). In their study, they found that up to 43% of G. vaginalis growth inhibition was observed after oral administration of LAB. Moreover, vaginal epithelial tissue exfoliation reduction and pro-inflammatory downregulation were observed after exposure to LAB; hence, it could be a better alternative for ameliorating BV [99]. In another study by Pessoa et al., 2017, they investigated Lactobacilli strains such as L. fermentum 5.2, L. plantarum 6.2, and L. plantarum 7.1, which were collected from cocoa fermentation against G. vaginalis. Outcomes showed that all strains have significantly interfered with the growth of G. vaginalis by high hydrophobicity and auto-aggregation mechanisms. These insights significantly suppressed bacterial growth in vaginal microflora without demonstrating any side effects [100]. Zhao et al., 2020, studied anti-G. vaginalis activity of four L. plantarum strains (ZX1, ZX2, ZX27, and ZX69), which were collected from Mongolian yogurt. Outcomes showed that maximum antibacterial potential (13.67 ± 1.70) exhibited by the ZX27 strain and all tested strains were able to alter G. vaginalis virulence gene expression, which was necessary for its pathogenic transitions; hence, it could be used as an alternative in the future as it showed promising activity [101].
7. Protein Roles in BV Pathogenesis and Management
Preclinical studies demonstrate that proteins play a crucial role in the management of vaginal infections by modulating the host immunity and restoring vaginal microbial balance (Table 5). For instance, Pino et al., 2017, conducted an open, prospective, randomized trial in women with bacterial vaginosis and demonstrated the antibacterial activity of lactoferrin. Their results showed that vaginal lactoferrin positively modulated the vaginal microbiome by enhancing Lactobacillus abundance and reducing pathogenic bacteria such as G. vaginalis and P. bivia. Notably, L. helveticus remained a dominant species in the vaginal mucosa before and after lactoferrin therapy [102]. Alanwaret al.,2023, conducted a randomized controlled clinical trial in women with recurrent BV during the third trimester of singleton pregnancies. Their findings demonstrated that lactoferrin exerted beneficial antibacterial effects on the vaginal environment [103]. Pino et al., 2022, investigated the in vitro anti-G. vaginalis (MTZ resistance) potential of bovine lactoferrin (iron-binding glycoprotein), and in their study, they have noticed that lactoferrin inhibited the growth of G. vaginalis in a concentration-dependent manner (32, 16, 8, 4, 2, 1, and 0.5 mg/mL), including MTZ-resistant strains. Authors have also investigated the antibacterial efficacy of lactoferrin without an iron source and observed that lactoferrin still did not support G. vaginalis growth; hence, it could be a potential alternative treatment option [104]. The present study focused on the in vitro evaluation of Endolysin against the biofilm community of associated bacteria (Johnston et al., 2023). The authors performed an Endolysin treatment of a polymicrobial biofilm study, and they observed that the endolysin protein showed a positive impact towards suppression of G. vaginalis biofilm by reducing the live bacteria count. Significant reduction in G. vaginalis viability was noticed after endolysin exposure; hence, it could be an effective alternative option for biofilm manipulation [105].
An in vitro study by Moreno et al., 2022, targeted the biofilm of G. vaginalis by identifying endolysin candidates. Maximum G. vaginalis biofilm prevention occurred by endolysin candidates such as CCB2M94_8 and CCB7.1, and comparatively higher disruption of biofilm was observed by CCB7.1 (MIC-50 µg/mL) and CCB8.1 (MIC-200 µg/mL) endolysin. Moreover, investigators also concluded that this could be a promising future alternative innovation across recurrent BV treatment approaches, as it avoids MDR caused by antibiotics and promotes healthy vaginal flora [106]. In this present study, Luo et al., 2023, have included the National Health and Nutrition Examination Survey (NHANES), which further demonstrated a correlation between homocysteine (HCY) and prevalence. Their study showed that HCY was positively associated with BV, which further resulted in the lower serum level of HCY being efficaciously helpful towards management and prevention [107]. Alla et al., 2001, have isolated a bacteriocin from Lactobacillus acidophilus (vaginal strain) and evaluated itsin vitro anti-G. vaginalis activity. Authors have concluded that this biologically active protein efficaciously inhibited the G. vaginalis strain and could be used further [108]. Turovskiy et al., 2009, evaluated the anti-G. vaginalis efficacy of bacteriocin, which is isolated from healthy vaginal bacteria. In their study, they have investigated that bacteriocin protein was able to alter the G. vaginalis cytoplasmic membrane and suppress its virulence potential [109].
8. Fatty Acid Roles in BV Pathogenesis and Management
In several research studies, fatty acids have been found to maintain the acidic pH of the vagina, thereby supporting the growth of protective Lactobacillus species (Table 6). For example, Strandberg et al., 2010, have assessed the in vitro anti-G. vaginalis efficacy of the Glycerol Monolaurate (GML) fatty acid in BV patients. In their study, a ≥3-log drop was observed in common fungicidal unit (CFU/mL) for G. vaginalis bacteria after administration of GML for 24 h at a 10 μg/mL concentration. Authors also demonstrated that GML potentially inhibited the growth of G. vaginalis by stabilizing the vaginal microbiome with exhibiting anti-inflammatory action [110]. Schwecht et al., 2023, have evaluated LA potential, and in their study, results demonstrated that LA and butyric, succinic, and acetic acids have improved barrier integrity of vaginal epithelium and ameliorated inflammatory effects [111].
9. Natural Compounds and Essential Oils in BV
Constituents derived from both plant and microbial sources could be a path to promising antibacterial activity in the history of mankind [104,105,114]. In this section of this critical review, we have discussed natural molecules and their novel pattern insights in depth towards inhibiting responsible pathogens (Table 7). Fan et al., 2023, studied the in vivo antimicrobial potential of Sophora favescens against 30 MTZ–resistant clinical strains of G. vaginalis from BV patients. In their study, they have learned that, at MIC 0.3125 to 1.25 mg/mL, S. favescens inhibited MTZ resistance in G. vaginalis growth; also, at MBIC 0.625 to 1.25 mg/mL, this alkaloid has significantly eradicated bacterial biofilms. Authors have also noticed that, after exposure to S. favescens alkaloid, bacterial biofilm shape changed from thick to flaky, which further indicated that this herbal approach not only disrupts the bacterial biofilm but also changes its microstructure and morphology [115]. Nord et al., 2019, have first evaluated the antimicrobial activity of Spathullin A (6,7-dihydroxy-5,10-dihydropyrrolo[1,2-b] isoquinoline-3-carboxylic acid) and Spathullin B (5,10-dihydropyrrolo[1,2-b] isoquinoline-6,7-diol) against Gram-negative and -positive bacteria. Outcomes revealed that spathullin B showed higher antibacterial potential against tested strains (E. coli and S. aureus, etc.) at MIC < 1 µg/mL than the spathullin A compound. Investigators concluded that, due to some issues associated with spathullin A (stability) and spathullin B (toxicity), they could be of low interest as further medication across BV unless a suitable formulation is developed [116]. Askari et al., 2020, conducted a randomized clinical trial to evaluate the anti-BV potential of myrtle and oak gall (MOGS) and also compared its activity with MTZ and placebo. Outcomes revealed that vaginal discharge improved more after administration of MOGS (mean 0.64 ± 0.50) than MTZ (1.55 ± 0.82); moreover, clinical signs and symptoms of BV were significantly suppressed by MOGS. Hence, it might be used further for developing new treatment options [117].
Yadav et al., 2019, have performed anti-E. coli activity of Azadirachta indica, Cichorium intybus (leaves), and Trigonella graecum, and in their study, they have demonstrated that a maximum antibacterial activity of 20.7 ± 1.15 and 18.0 ± 1.0 was observed after exposure of A. indica water extracts and hydro alcoholic extracts of T. foenum graecum, and could be used in the future as an alternative [118]. Selis et al., 2021, have aimed to characterize antibacterial actions of five Lactobacillus strains, such as L. casei, L. fermentum, and L. plantarum, isolated from Theobroma grandiflorum. From an in vitro antimicrobial assay, it was revealed that the maximum anti-G. vaginalis potential (35.55 ± 2.98) and G. vaginalis inhibition zone (IZ) (21.00 ± 0.00 mm) exhibited by Lp90 and Lc24 Lactobacillus,comparatively, produced maximum H_2_O_2_. All strains produced better efficacy by stabilizing vaginal pH [119]. Essential oils have also demonstrated potent activity against vaginal infections (Table 8). For instance, Machado et al., 2017, have studied and compared in vitro anti-G. vaginalis activity, and in their study, they demonstrated that, at MIC 0.16 μL/mL, both T. capitata EO and carvacrol revealed efficacious antibacterial potential. Biofilm biomass reduction in G. vaginalis has been observed by both EOs and carvacrol at a 0.64 μL/mL concentration. Authors have confirmed that EOs showed more biofilm disruption activity than carvacrol; hence, it could stand out as an efficacious therapy [120]. Rosca et al., 2022, evaluated, for the first time, antimicrobial assays against polymicrobial biofilm formed by six spp. At an MIC ranging from 0.16 to 0.31 µL mL^−1^, EOs exhibited antibacterial activity against all spp., whereas MTZ showed MIC 8–32 µL mL^−1^ against G. vaginalis. The potential of EOs revealed that the biofilm of all spp. was significantly inhibited and stands out as an efficacious alternative [121].
Bogavac et al., 2016, have evaluated the antibacterial efficacy of Rosmarinus officinalis EO against E. coli, which is also responsible for BV development. From an in vitro antimicrobial study, it was learned that, at MIC/MFC of 12.5 mg/mL, EO revealed a promising effect and could be a futuristic alternative to synthetic medication [122]. Within theirin vitro and in vivo anti-G. vaginalis study, Trinh et al., 2011, investigated Artemisia princeps Pamp. EO (active compound: eucalyptol and α-terpineol) potential. At MIC 0.06% (v/v), growth of G. vaginalis was more inhibited by α-terpineol than eucalyptol; also, both of the herbal compounds significantly suppressed viable G. vaginalis numbers in vaginal mucosa. Authors have also noticed that both of these compounds also potentially inhibited pro-inflammatory cytokines and ameliorated BV [123]. Schwiertz et al., 2006, demonstrated the antibacterial efficacy of ten EOs (lemongrass, palmarosa, tea tree, neroli, manuka, lavender, rosemary, thyme linalool, geranium, and clary sage), and, in their in vitro study, they found that every EO was able to significantly inhibit G. vaginalis growth at 1–2.5 μL/mL (MIC and MBC); however, maximum G. vaginalis growth inhibitions were noticed by lemongrass, palmarosa, lavender, and geranium EO administration [124].
10. Vitamins’ Roles in BV Pathogenesis and Management
Vitamins contribute to the management of BV by demonstrating potent antimicrobial activity (Table 9). For instance, Mojtahedi et al., 2023, have conducted a case–control study to evaluate the association between 25-hydroxy vitamin D and incidence of BV for further therapeutic advancement. Key findings of their study were that lower serum levels of vitamin D were observed in BV cases, and it also exhibited an inverse association with 25-hydroxy vitamin D. The authors concluded that deficiency of this vitamin could cause/elevate incidence. However, further studies should be conducted to evaluate its potential across BV [125]. This meta-analysis study aims to assess the vitamin D deficiency and BV risk association in pregnant women [126]. Analysts have concluded that vitamin D is inversely associated with adverse health outcomes and a high incidence of BV in women. Vitamin D supplementation/intake could give a positive/effective impact on the incidence of BV, especially in pregnant women, and further studies still need to be carried out to develop an alternative treatment in the future [126].
In this cross-sectional study, Cui et al., 2023, have included NHANES in the years 2001–2004, which demonstrated an association between folate and the development and pathogenesis of BV. In their study, investigators found that serum folate has a negative/inverse association. Investigators also observed that adequate supplementation with folate could give potential antimicrobial efficacy and suppress the associated pathogenic risk, which could be a suitable alternative treatment option [127]. Alizadeh et al., 2017, evaluated the antibacterial effect of vaginal tablets containing vitamin C on the treatment and recurrence by designing a triple-blind randomized clinical trial. In their study, the intervention group was administered vitamin C with oral MTZ for 7 days, and after that, the results showed that, comparatively, maximum clinical symptoms associated were suppressed/reduced in the intervention group than in patients treated with the placebo group (Placebo + MTZ). Researchers also demonstrated that 84.8% of patients were more satisfied with vitamin C in the MTZ treatment group than with the placebo (75.6%) [128]. In another study by Krasnopolskya et al., 2013, they designed a randomized, double-blind, placebo-controlled, parallel-group clinical trial to evaluate vitamin C vaginal tablets (200 mg ascorbic acid) on recurrent episodes. In their study, investigators concluded that 6.8 and 14.7% of patients (vitamin C group) and 14.7 and 32.4% of patients (placebo group) experienced recurrence of BV after 3 and 6 months of treatment therapy. Constant use of vitamin C helped to reduce the incidence of its recurrent form, and that could be useful further as an alternative to synthetic medication [129].
11. Miscellaneous Factors in BV Pathogenesis and Management
Hymes et al., 2013, have studied the in vitro and in vivo anti-G. vaginalis potential of DNase, and in this work, the authors targeted the eDNA, which is associated with G. vaginalis biofilm. Outcomes revealed that DNase significantly inhibits and disrupts bacterial biofilm, and not only does it do that, but it also potentiates antibiotics’ efficacy against G. vaginalis biofilm. Authors also observed that DNase inhibits bacterial colonization; hence, it could stand out as an alternative therapy option [112]. Sarabia et al., 2020, demonstrated SLD inhibition of G. vaginalis by producing a monoclonal antibody (mAb) in MAP8 format. In this study, investigators observed that anti-SLD mAb efficiently suppressed SLD activity in G. vaginalis and could be used in the future by reducing complications associated with BV [113].
12. Herbal Nanoformulations for BV
In this section, we analyzed nanotechnology-based delivery systems that have brought numerous advances to improve the therapeutic properties of herbal drugs. These systems offer technical optimizations, such as sustained, controlled, and targeted drug release, which enhance bioavailability, improve site-specific delivery, and reduce systemic side effects for more effective patient-specific applications [25,130,131]. Integration of natural source constituents with nanomaterials overcomes drawbacks associated with herbal drugs, like stability, compatibility, etc. This technology reframes the therapeutic properties by improving its bioavailability. Table 10 outlines a detailed compilation of novel formulations comprising natural-based constituents used in BV.
Kaczmarek et al., 2022, demonstrated that a chitosan-based system with Scutellariae baicalensis radix (SBE) extracts acts as a potential implementation towards vaginal infections like BV. In their in vitro antimicrobial assay, they have compared the potential of SBE, SBE-loaded Cs, MTZ, and clindamycin with each other to evaluate therapeutic efficacy. They further observed that, at MIC-800 µg mL^−1^ and a ratio of 2:1, SBE (27.0 ± 2.0) and SBE/Cs (25.0 ± 2.0) exhibited a better maximum IZ than the marketed medication (MTZ and clindamycin), which were tested at MIC 1000 µg mL^−1^ against G. vaginalis. They have also concluded that an herbal extract-loaded chitosan system could be a better alternative in the future for vaginal drug delivery, as it refines the vaginal microbiome by reducing inflammation [132]. A mucoadhesive chitosan tablet system containing Chelidonii herba extracts has been formulated by Paczkowska et al., 2020, to overcome vaginal bacterial infection. Findings showed that, out of all formulations, F3 with HPMC in it exhibited maximum mucus adhesion in porcine vaginal mucosa. From this study, it was concluded that this formulation could be a good alternative candidate across BV (Table 10), as it has shown potential antibacterial efficacy with considerable inflammation [133].
Arrue et al., 2023 formulated biosurfactants from probiotic Bacillus spp. at concentrations such as 1% (BNE1%) and 3.33 wt% (BNE3.33%) in a nanoemulsion system and evaluated their antibacterial potential against E. coli, which is a potential spp. This helps in developing BV. The results showed that probiotic-based BNE3.33% nanoemulsion was potentially able to inhibit bacterial adhesion and disrupt bacterial cell integrity. The BNE3.33% formulation exhibited a low MIC of 0.5 mg/mL, demonstrating effective antimicrobial activity compared to all other formulations [134]. Bouaouina et al., 2022 have evaluated the antimicrobial action of Origanum glandulosum Desf by encapsulating it into a nanoemulsion-based system. In Vitro antibacterial assay showed that, at MIC-0.62%, O. glandulosum oil exhibited an efficacious IZ of 13 mm, whereas herbal-based nanocapsules and nanoemulsions showed IZ of 11 and 20 mm against MDR bacteria spp. Authors also learned that nanoemulsion potentially inhibited bacterial biofilm than nanocapsule, which could be used further for an alternative treatment option [135]. Tomás et al., 2023 have incorporated Thymbra capitata EO (TCEO) into a suitable vaginal sheet system to evaluate its anti-G. vaginalis potential. A cellular toxicity study demonstrated that, at adequate concentration, the herbal vaginal sheet revealed nontoxic action to the HEC 1A cell line, and an antimicrobial assay revealed that the TCEO vaginal sheet was significantly able to inhibit G. vaginalis load and its biofilm at 0.32 µL/mL concentration. At last, researchers concluded that these herbal-based vaginal sheets significantly inhibited G. vaginalis with dose-dependent concentration [136].
13. Underlying Mechanisms of BV
In this section, we have critically discussed novel mechanistic insights regarding herbal molecules in BV while minimizing MDR [137,138]. Natural molecules, nutraceuticals, vitamins, enzymes, proteins, plant-derived compounds, EOs, and fatty acids exhibit broad mechanistic insights by targeting dysbiosis and biofilm. A healthy vagina is a Lactobacillus-dominated microbiota that prevents overgrowth of anaerobic bacteria, i.e., G. vaginalis, which exhibits pathogenic transition and leads to virulence factors (Figure 1). Nutraceuticals and plant-derived molecules can disrupt adhesion and biofilm integrity through interference with quorum sensing, key enzymes, and modulation of host cell surface molecules, potentially restoring a vaginal microbiome. Vitamins, especially vitamin C, may lower vaginal pH and support epithelial barrier function, indirectly supporting Lactobacillus growth. Enzymes such as DNases or proteases can degrade ECM in biofilms, enhancing the susceptibility of pathogenic bacteria to host immunity and antimicrobial agents. Proteins can directly lyse bacterial membranes or modulate immune responses, enhancing the clearance of BVAB. EOs and fatty acids disrupt G. vaginalis membranes and inhibit biofilm formation. Nanomaterials, such as Au or chitosan NPs, offer targeted delivery and enhanced site-specific penetration, enabling antimicrobial action or delivery of bioactive compounds while protecting the healthy microbiome (Figure 4). Additionally, these molecules act through diverse mechanisms (Figure 5), modulating immune responses and directly killing or suppressing BVAB without observed toxicity, offering promising alternatives to conventional therapies, especially in the context of biofilm-associated resistance (Figure 3) and recurrent episodes.
14. Critical Analysis of Patent Literature on BV
Patent data plays a vital role for investigators to focus more on naturally based constituents loaded into novel formulations, which might gain attention as an alternative to conventional therapies in terms of potential, MDR, and recurrence rate [139], summarizing a comprehensive patent showcasing a diverse and evolving therapeutic arsenal targeting BV, encompassing plant-based interventions, EOs, vitamins, probiotics, proteins, enzymes, and NPs-based systems (Table 11). Plant-derived formulations, particularly from traditional Chinese medicine and herbal combinations, exhibited anti-inflammatory and biofilm inhibitory properties with no toxicity noticed. This evident research data holds immense potential and might stand as an alternative. Several entries emphasize the effectiveness of epigallocatechin gallate and traditional blends in suppository or douche forms, with claims of suppressed recurrence and hormonal balance restoration. EOs have been explored for their antimicrobial and anti-inflammatory efficacy, showing promising results like microbial clearance and symptom reduction without irritation. Notable innovations in the probiotic sector have been observed, such as targeting BV directly but also restoring vaginal flora and maintaining vaginal pH using strains like L. crispatus, L. acidophilus, and Bifidobacterium spp. Investigators also integrate folic acid or employ delivery innovations such as layered condoms and effervescent vaginal tablets for sustained microbial balance and infection prevention. Vitamin-based supplements, especially ascorbic acid, vitamin E, and complex B, often in combination with probiotics or plant extracts, showed enhanced mucosal immunity, restored tissue health, and supported microbiome recovery. Moreover, protein-based interventions, like CXCL12, are outlined in immunological modulation alongside microbial targeting. Collectively, these patents summarize a necessary shift toward multi-mechanistic, biocompatible, and microbiota-supportive interventions. The incorporation of natural molecules with targeted delivery systems addresses MDR and recurrence.
15. Conclusions
This review highlights the promising potential of natural bioactive compounds, such as berberine, curcumin, thymol, allicin, and TTO, as adjunct or alternative therapies for G. vaginalis-induced BV. These phytoconstituents exhibit strong antimicrobial, anti-inflammatory, and immunomodulatory effects, selectively inhibiting BV pathogens while supporting beneficial Lactobacillus spp. Clinical evidence, including a randomized trial, shows curcumin to be as effective, if not more so, than MTZ in treating BV, with fewer side effects and an 82% cure rate versus 42% for MTZ two weeks post treatment. However, the clinical utility of these compounds is constrained by poor solubility, instability in vaginal environments, and rapid systemic clearance. NP-based delivery systems, such as liposomes, solid lipid NPs, polymeric NPs, and vaginal nanogels, address these challenges by enhancing solubility, stability, targeted delivery, mucoadhesion, and controlled release. Safety, manufacturing scalability, regulatory compliance, and patient acceptability, particularly concerning intravaginal use, must be thoroughly investigated. Additionally, exploration of synergistic formulations combining nanoherbal agents with probiotics (e.g., L. crispatus LACTIN V) is notably lacking, even though live biotherapeutics show promise in reducing BV recurrence. The future of BV management lies in a personalized, multi-targeted nanomedicine approach. Integrating robust phytocompounds with advanced delivery technologies, alongside precision microbiome-directed strategies, could revolutionize treatment by maximizing efficacy and minimizing resistance and harm. Finally, harnessing the synergistic power of natural molecules and nanotechnology offers a multifaceted, next-generation therapeutic paradigm for BV, one that could overcome current limitations and usher in safer, more effective, and patient-friendly treatments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zeng X. An R. Li H. Risk factors of recurrent bacterial vaginosis among women of reproductive age: A cross-sectional study Open Med.2023182023074310.1515/med-2023-0743 PMC 1042626637588657 · doi ↗ · pubmed ↗
- 2Wnorowska U. Piktel E. Daniluk T. Paprocka P. Savage P.B. DurnaśB. Bucki R. Ceragenins Prevent the Development of Murine Vaginal Infection Caused by Gardnerella vaginalis Pharmaceuticals 202417144510.3390/ph 1711144539598357 PMC 11597204 · doi ↗ · pubmed ↗
- 3Dalabehera M. Subudhi R.N. Boateng J. Choonara Y.E. Chaudhari S. Chellappan D.K. Kanojia N. Mnqiwu K. Singh T.G. Negi P. Metallic and lipid nanoparticles against multidrug resistant candida: Advances and translational hurdles Expert Opin. Drug Deliv.2025 accepted 10.1080/17425247.2025.255601440891288 · doi ↗ · pubmed ↗
- 4Mitra A. Gultekin M. Ellis L.B. Bizzarri N. Bowden S. Taumberger N. Bracic T. Vieira-Baptista P. Sehouli J. Kyrgiou M. Genital tract microbiota composition profiles and use of prebiotics and probiotics in gynaecological cancer prevention: Review of the current evidence, the European Society of Gynaecological Oncology prevention committee statement Lancet Microbe 20245 e 291e 30010.1016/S 2666-5247(23)00257-438141634 · doi ↗ · pubmed ↗
- 5Vodstrcil L.A. Muzny C.A. Plummer E.L. Sobel J.D. Bradshaw C.S. Bacterial vaginosis: Drivers of recurrence and challenges and opportunities in partner treatment BMC Med.20211919410.1186/s 12916-021-02077-334470644 PMC 8411528 · doi ↗ · pubmed ↗
- 6Abou Chacra L. Fenollar F. Diop K. Bacterial Vaginosis: What Do We Currently Know?Front. Cell. Infect. Microbiol.20211167242910.3389/fcimb.2021.67242935118003 PMC 8805710 · doi ↗ · pubmed ↗
- 7Savicheva A.M. Molecular Testing for the Diagnosis of Bacterial Vaginosis Int. J. Mol. Sci.20232544910.3390/ijms 2501044938203620 PMC 10779368 · doi ↗ · pubmed ↗
- 8Khedkar R. Pajai S. Bacterial Vaginosis: A Comprehensive Narrative on the Etiology, Clinical Features, and Management Approach Cureus 202214 e 3131410.7759/cureus.3131436514655 PMC 9735379 · doi ↗ · pubmed ↗