Joint Hypermobility: An Under-Recognised Cause of Palpitations, Dizziness, and Syncope in Young Females
Zeina Abu Orabi, Sophie E. Thompson, Jan van Vliet, Kate Gee, Ashwin Roy, Jonathan N. Townend

TL;DR
Joint hypermobility is a common but overlooked cause of dizziness, palpitations, and fainting in young women, often misdiagnosed as stress or anxiety.
Contribution
Highlights joint hypermobility syndromes as a significant yet under-recognized cause of syncope and related symptoms in young females.
Findings
Tilt-table testing revealed orthostatic hypotension, reflex syncope, or POTS in 82% of cases.
Conservative measures improved symptoms in over half of patients, while pharmacological treatments were used for refractory cases.
JH syndromes are multi-system conditions affecting physical and mental health, often dismissed as functional.
Abstract
Background: Symptoms of dizziness, syncope, and palpitations are common presentations in outpatient and emergency care, frequently attributed to stress and anxiety when conventional neurological and cardiac evaluations are normal. Joint hypermobility (JH) syndromes including hypermobile Ehlers–Danlos syndrome (hEDS), and hypermobility spectrum disorders (HSD) are under-recognised as potential causes. Methods: Our retrospective cohort study examined the clinical features, diagnostic findings, and responses to treatment in patients with JH syndromes, who are referred to a specialised syncope clinic within a UK teaching hospital. It involved 218 patients with joint hypermobility, predominantly young females (median Beighton score: 6), reporting chronic orthostatic intolerance, dizziness, and palpitations. Common comorbidities included joint pain, chronic fatigue, gastrointestinal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
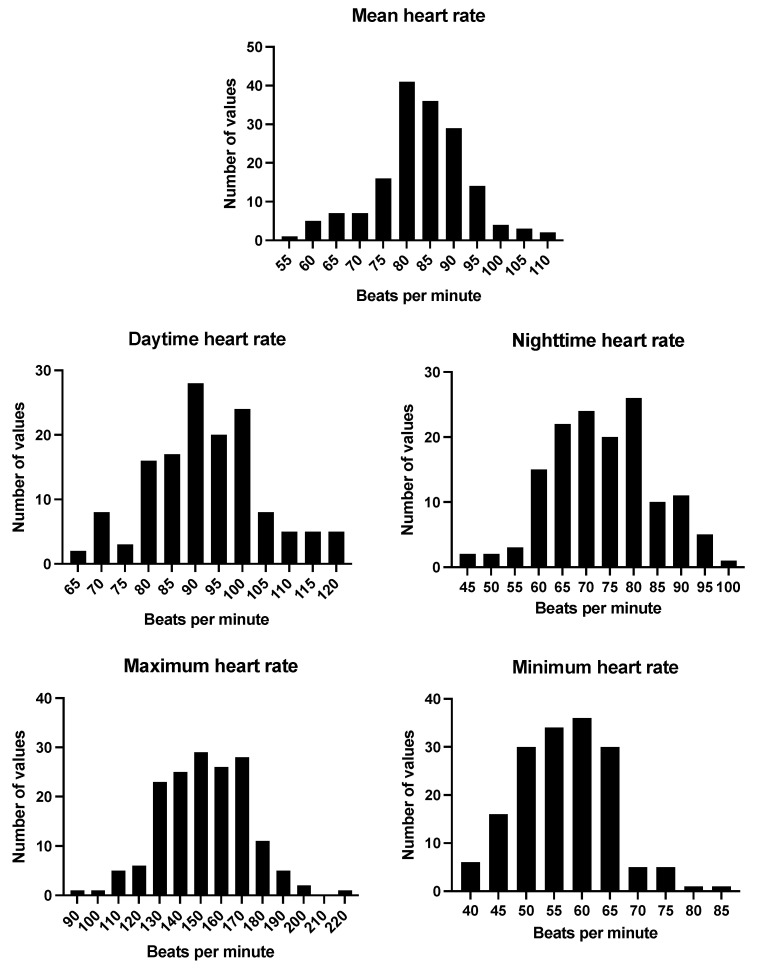 Figure 1
Figure 1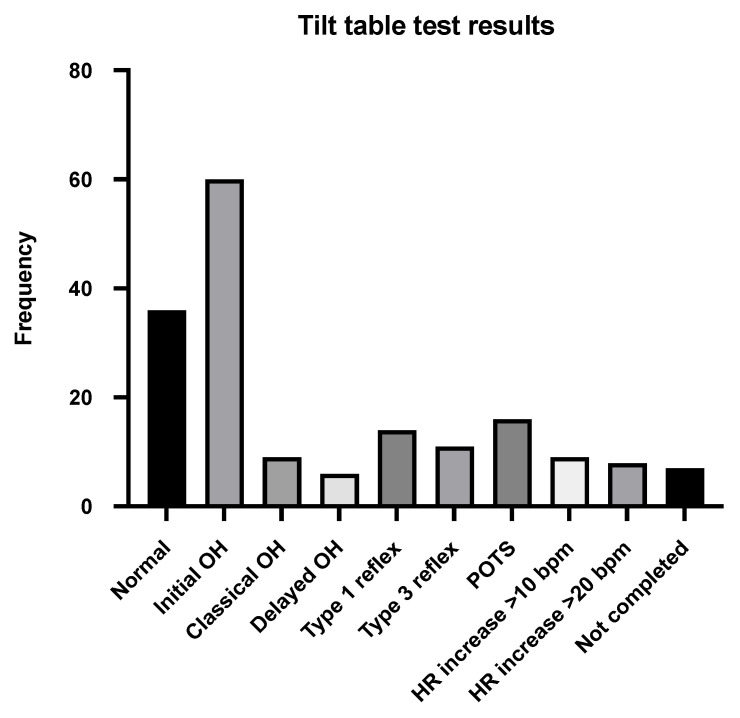 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsConnective tissue disorders research · Cardiovascular Issues in Pregnancy · Cardiomyopathy and Myosin Studies
1. Introduction
Symptoms of dizziness, syncope, and palpitations are common reasons for referral to both outpatient services and the emergency department (ED). Syncope alone is said to account for 1–3% of ED attendances, while palpitations may account for a further 0.5% [1,2]. Frequent approaches involve investigations for epilepsy and/or cardiac evaluations to look for structural abnormalities and arrhythmia, usually involving auscultation, an ECG, ambulatory ECG monitoring, and transthoracic echocardiography (TTE). When no abnormality is apparent, many patients, particularly young adults, are discharged with reassurance that there is ‘no cardiac or neurological abnormality’ along with suggestions of symptoms due to stress and anxiety.
Joint hypermobility (JH) syndromes are well recognised by rheumatologists as causes of joint instability and chronic pain but are often not appreciated by the medical profession as common causes of dizziness, pre-syncope, syncope, and palpitations. While the problem of ‘hypermobility syndrome’ causing joint laxity was first described in 1967, the extra-articular manifestations of orthostatic intolerance together with chronic pain, gastrointestinal dysmotility, psychiatric disease, urinary tract problems, and chronic fatigue were recognised only gradually during the 1980s and 1990s [3]. Why this common problem affecting around 3% of the population and up to 26% of adolescents is so poorly appreciated and understood remains unclear [4,5].
This report describes the experience of a single dedicated syncope clinic based in a large university teaching hospital in the UK. A single physician (JNT) took over the running of this clinic in 2020 and noted that many young adult female patients were being referred by primary care, often following ED attendance, with a constellation of symptoms consisting of dizziness, rapid palpitations, syncope, effort, and orthostatic intolerance. In many cases, the referring doctor questioned a diagnosis of anxiety or postural orthostatic tachycardia syndrome (POTS). Given the number of such patients with a history of JH/hypermobile Ehlers–Danlos Syndrome (hEDS) and the previous reports of an association between JH and POTS, it was decided to look for evidence of JH in all such patients referred to the clinic. Accordingly, from 2020, all new patients with possible POTS (dizziness, palpitations, or syncope) were assessed with a Beighton score in addition to a standard cardiovascular assessment. This report describes the characteristics of a large group of these under-recognised, mainly female patients with chronic disability and aims to characterise their cardiovascular and other symptoms via physical and investigation findings after a uniform diagnostic testing approach.
2. Methods
2.1. Population and Data Collection
Patients with JH were identified from an electronic register of patients attending the syncope clinic at the Queen Elizabeth Hospital Birmingham between February 2021 and July 2024. Criteria included a Beighton score of >4 along with a typical symptom constellation of orthostatic intolerance, dizziness, and palpitations. A pragmatic approach to the diagnosis of JH was used using a detailed history examination to determine a Beighton score. No consistent attempt was made to differentiate hEDS from HSD (see Section 4). The clinic was run by a consultant cardiologist who documented each patient in an initial clinic letter and arranged a standard set of investigations. A retrospective review of the hospital’s electronic patient record system was conducted at the beginning of August 2024 to review clinic letters, where data on patient-reported past medical history, medication history, and social history were gathered. Data were also collected on the number of ED attendances and the reason for presentation. Clinical observations were recorded, including blood pressure, pulse rate, height, and weight, as well as the results of initial investigations, which in most cases included TTE, 24 h ambulatory ECG, and a tilt-table test.
2.2. Diagnostics
All investigations were performed according to standard departmental protocols. TTE was performed by accredited technicians according to the British Society of Echocardiography’s minimum dataset [6] and analysed using IntelliSpace Cardiovascular (Philips, Amsterdam, The Netherlands). Ambulatory ECG monitoring was most commonly undertaken for a 24 h period; however, some patients underwent a longer period of monitoring (up to 72 h). Tilt-table testing was performed according to a standard protocol (40 min stand at 70 degrees), without drug provocation [7]. Definitions of abnormalities on tilt-table testing are described in Table 1.
2.3. Statistical Analysis
Data analysis was performed using SPSS (SPSS Inc., Chicago, IL, USA; 28.0.1). Descriptive statistics, frequencies, and percentages were generated. Data are presented as the mean (standard deviation) or median (interquartile range).
2.4. Ethical Considerations
This study was approved by the Clinical Audit Department at the Queen Elizabeth Hospital Birmingham (CARMS: 19486 and date of approval: 24 July 2023). In accordance with the UK National Research Ethics Service guidance, neither individual informed consent nor a formal research ethics committee review was required as the study was undertaken by the direct clinical team using data previously gathered during the course of routine care and sufficiently anonymised.
3. Results
3.1. Demographics
A total of 218 patients with JH attended the syncope clinic between February 2021 and July 2024, with a median follow-up period of 1.2 years (an IQR of 2.2 years; a range of 2 months to 4.7 years). Most patients were female (95.4%) and of white ethnicity (65.1%), with a median age of 24 years (IQR 11.0). The mean BMI of the patients was 26.5 (SD 6.6), though 44.0% of patients were categorised as overweight or obese. Almost one in three (29.4%) patients with JH were not in employment, education, or training. The median Beighton score at the first clinic visit was six (an IQR of three). Although the majority of patients (59.2%) were mildly or moderately limited in terms of mobility by their condition, 18 (8.3%) reported being severely limited, while 6 patients (2.8%) were wheelchair-bound. Psychiatric disease was common, affecting 67.9% of the patients, principally depression (22.9%), anxiety (26.6%), and the combination (13.3%). Almost half (45.9%) of the patients were on psycho-active medication. ADHD and autism affected 7.8% and 7.3% of the patients, respectively. Other common comorbidities included migraine (34.9%), asthma (14.2%), mast cell activation/allergy syndrome (12.4%) and fibromyalgia (6.9%). Baseline characteristics are summarised in Table 2.
3.2. Symptoms
Patients had been experiencing symptoms for a median of 5.0 years (an IQR of 7.0) prior to their first visit to the syncope clinic. The predominant cardiovascular symptom was dizziness upon standing (77.1%), followed by syncope (10.1%) and palpitations (9.6%). Although not the predominant symptom in most, palpitations were common as a secondary symptom, affecting around half of the patients (50.9%). Additionally, non-cardiovascular symptoms were highly prevalent. The commonest were gastrointestinal (40.4%), migraine (34.9%), chronic pain (34.4%), joint pain/dislocation (28.0%), and chronic fatigue (25.2%). ED attendance data was available from 2018 onwards. Over a 6-year period (2018–2024), 136 of these patients attended ED at trust hospitals at least once. In total there were 861 ED attendances between 136 patients. Cardiovascular complaints were a common reason for emergency presentation, with 116 attendances due to non-specific chest pain, 45 with shortness of breath, 45 with dizziness or pre-syncope, 25 with palpitations, and 12 with syncope. Almost one-third of those admitted were classified as having seizures (n = 46).
3.3. Cardiovascular Investigations
3.3.1. Baseline Physiological Parameters
The mean heart rate of the patients not on rate-limiting medications in the clinic was 99 beats per minute (bpm) (an SD of 17.1). In those taking rate-limiting medications already (n = 7), the clinic heart rate was 81 bpm (an SD of 13.0). The mean systolic blood pressure in the clinic was 125 mmHg (an SD of 13.9), and the mean diastolic blood pressure was 80 mmHg (an SD of 8.5). A minority of patients were identified as having postural hypotension in the clinic, with a fall in systolic BP of > 20 mmHg upon standing (10.6%).
3.3.2. Electrocardiography and Ambulatory Monitoring
All patients had a baseline ECG. This was normal in most (76.1%). Sinus tachycardia (heart rate (HR) > 100 bpm) was identified in 27 patients (12.4%), while sinus bradycardia was seen in 2 patients (0.9%). ST/T wave changes were identified in 23 patients (10.6%). Other notable ECG findings detected included a long QT interval (n = 1), right-axis deviation (n = 2), and intraventricular conduction delay (right bundle branch block (RBBB) or incomplete RBBB, n = 2). Of the 165 patients who had complete ambulatory ECG monitoring, the average 24 h HR of patients off rate-limiting medications was 83 bpm (an SD of 9.9). All patients showed a physiological fall in nocturnal heart rate; the mean daytime HR was 92 bpm (SD 12.2), and the nighttime HR was 74 bpm (SD 10.9). No significant arrhythmias (other than sinus tachycardia) were detected amongst the cohort on Holter monitoring. The ECG findings and heart rate data are summarised in Table 3 and Figure 1.
3.3.3. Transthoracic Echocardiography
TTE was performed in 198 patients, of which the majority were normal (83.9%). Five patients (2.3%) were noted to have elongation of the anterior mitral valve leaflet, and three (1.4%) had bileaflet bowing of the mitral valve without significant prolapse. Seven patients (3.2%) had mild valvular regurgitation (mitral in three, tricuspid in two, aortic in one, and pulmonary in one). Incidental findings included a small pericardial effusion and a small perimembranous ventricular septal defect (VSD). One patient was already known to have mild–moderate aortic stenosis under follow-up elsewhere. None had significant aortic root dilatation.
3.3.4. Tilt-Table Testing
Around three-quarters of patients had a tilt-table test (n = 162, 74.3%). This was normal in just 36 patients (16.5%), including 3 who had symptoms during the test. The test was not fully completed in seven patients (3.2%). Initial orthostatic hypotension (OH) was the most common abnormality during tilt-table testing, as identified in 60 (27.5%) patients. Nine patients (4.1%) had classical OH, while six (2.8%) had delayed OH. Type 1 mixed reflex syncope was seen in 14 patients (6.4%), and type 3 vasodepressor reflex syncope was seen in 11 patients (5.0%). A group of patients demonstrated abnormal heart rate responses. Sixteen patients (7.3%) met the diagnostic criteria for POTS, with a sustained increase in heart rate within 10 min of tilt of >30 bpm. Nine patients (4.1%) displayed an increase in heart rate of >10 bpm within 10 min, and eight patients (3.7%) showed an increase in heart rate of >20 bpm within 10 min. (Table 3 and Figure 2).
3.4. Response to Management
At the time of the first clinic visit, 52 patients (23.9%) were already implementing conservative measures such as increased fluid (2–3 L daily) and salt intake. Over half of the patients (n = 127, 58.3%) responded favourably to conservative measures. Some patients had already been initiated on medical treatment prior to their first clinic visit, including 26 (11.9%) on a beta-blocker, 21 (9.6%) on ivabradine, and 5 (2.3%) on fludrocortisone. Medical management in the syncope clinic included introduction of a new medication or dose increase and was initiated in 128 (58.7%) patients. The dose of an existing cardiovascular medication was increased in 14 patients (6.4%). Overall, 56 (43.8%) patients reported complete symptomatic responses to medical therapy. Over a quarter of patients (n = 36, 28.1%) reported some improvement in their symptoms with medical management. Only 8 (6.3%) patients did not respond to medical therapy, and 28 (21.9%) have not yet been followed up to assess their response (Table 4).
4. Discussion
This retrospective analysis from a single UK hospital demonstrates that there are many young female patients with JH syndromes and long-standing, disabling cardiovascular symptoms for which no cause has been identified and for whom no effective treatment has been provided. Most have been in frequent medical contact in primary and secondary care. This report illustrates the importance of a thorough history and routine rapid joint assessment using the Beighton score to reveal the diagnosis. This adds little time or expense to the consultation. We also provide new information on the low prevalence of echocardiographic abnormal findings and on the high prevalence of abnormalities from investigations by ambulatory monitoring and tilt testing in patients with JH. Our report draws attention to additional physical problems related to JH including joint pain, chronic fatigue, chronic pain, gastrointestinal and urinary problems, and migraine, which were all highly prevalent. Lastly, psychological problems and disorders including anxiety and depression, with autism and ADHD being heavily over-represented, a finding consistent with previous reports of a strong association between JH syndromes and autistic spectrum disorder [8,9]. The association of POTS and orthostatic intolerance with JH syndromes is not a new finding [10,11], but our study demonstrates the high prevalence of this disorder in young women presenting with symptoms suggestive of POTS and the substantial co-morbidity that is often present.
Considerable and understandable confusion surrounds the precise diagnosis and classification of JH syndromes, with frequent changes in terminology. Most recently, in 2017, the previous term ‘joint hypermobility syndrome’ was renamed as ‘hypermobility spectrum disorders’ (HSD) [12]. In addition, type III Ehlers–Danlos syndrome was renamed ‘hypermobile Ehlers–Danlos syndrome (hEDS)’ and given a new set of diagnostic criteria to differentiate it from HSD. By definition, hEDS is currently genotype-negative, and the criteria are clinical. They involve evidence of JH assessed using the Beighton score; dermatological, skeletal, dental, valvular, or aortic abnormalities (including at least mild mitral valve prolapse or aortic root dilatation); or a family history of chronic pain or recurrent dislocation and exclusion of other connective tissue disorders [13]. If significant hypermobility is present on the Beighton score but a patient does not fit the criteria for hEDS or another of the EDSs, the patient is diagnosed as HSD. The two disorders are difficult to clinically differentiate (indeed, they are widely considered as the same disorder), and as both are associated with the same symptoms and management strategies, there seems little practical reason in attempting to differentiate them in the clinical setting.
Our data demonstrates that standard cardiological investigations for JH syndromes are most helpful to exclude alternative underlying causes. Ambulatory ECG monitoring excluded arrhythmia but showed no diagnostic features other than frequent daytime sinus tachycardia. All patients had a normal fall in heart rate at night. TTE identified a small number of patients with mitral valve abnormalities of low clinical significance. There is a weak association between valvular abnormalities and hEDS, and this is even weaker for HSD. A study of 258 patients by Rashed et al. found that mitral valve prolapse (7.5%) and thoracic aortic root dilatation (15.2%) were common in both hEDS and HSD, although aortic dilatation was more prevalent in those meeting the diagnostic criteria for hEDS (20.7%) than HSD (7.7%) [14]. Additionally, five patients experienced extra-aortic complications including spontaneous carotid artery dissection and coronary artery dissection [10]. A study of a similar size by Asher et al. noted a similar prevalence of mitral valve prolapse (6.4%) and 1.6% with aortic root dilatation [15]. For context, the prevalence of mitral valve prolapse in the general population is estimated at 2.6% [16], while aortic dilatation is estimated at 1.4–4.0% [17,18]. Given the low prevalence of abnormalities and the fact that most were minor findings requiring no intervention, there is a valid argument against the routine use of TTE in these patients unless clinically indicated.
Tilt-table testing was arguably the most useful investigation; however, only 9.9% met the diagnostic criteria for POTS, i.e., a rise in heart rate of more than 30 bpm with symptoms. The frequent presence of resting tachycardia, however, meant that although tachycardia within 10 min of head up tilt was common, the incremental change in heart rate was usually well under 30 bpm. The test did however show a high rate of other abnormalities including initial and late OH and reflex syncope. Identification of autonomic dysfunction helped guide management. Initial management focused on conservative measures such as wearing supportive activewear, increasing water intake to 2–3 L daily, increasing salt intake (>5 g/day), and engaging in low-impact physical activities such as Pilates to improve fitness and core stability. Conservative measures proved effective in over half of the patients. For patients who did not respond adequately, pharmacological treatments were considered. In those who demonstrated inappropriate tachycardia or an abnormal tachycardic response upon tilt-table testing, ivabradine was often offered. Ivabradine, a selective IF channel blocker, has been evaluated in very few small, randomised trials for inappropriate sinus tachycardia and POTS, with results indicating improvements in symptom burden, functional ability, and quality of life [19,20]. Patients with objective OH identified through tilt-table testing and persistent dizziness despite salt and water loading were offered fludrocortisone or midodrine if fludrocortisone was not tolerated or ineffective. We acknowledge that limited data exist on the use of these medications in younger populations and that robust safety data for use during pregnancy is lacking, an important consideration given the predominance of women of childbearing age. Most patients in our cohort experienced complete resolution of their symptoms, demonstrating the effectiveness of this stepwise approach.
Cardiovascular autonomic features in hypermobility syndromes were first described in 1999 and further characterised in 2003 when a study of 48 patients with ‘joint hypermobility syndrome’ found symptomatic OH, POTS, and uncategorized orthostatic intolerance in 78% of patients versus 10% of controls [21,22]. The mean age at presentation of 24 years in our study is consistent with previous reports [23]. Using objective tests in patients and controls, greater blood pressure responses to a cold pressor test and evidence of pharmacological α-adrenergic and β-adrenergic hyperresponsiveness were demonstrated [18]. Other studies have noted an association between POTS and JH, and it has been estimated that over half with POTS have generalised joint laxity, although our experience would suggest that this is an underestimate [24]. Despite these publications, which are often from over 20 years ago, knowledge about the association of disorders involving cardiovascular autonomic function and JH is not widespread amongst physicians, including cardiologists. In patients without known JH presenting with cardiovascular symptoms, the diagnosis is often not considered and joints are not examined.
The mechanisms underlying the multi-organ symptoms of JH remain poorly understood. An attractive but unproven theory attributes OH and tachycardia to excessive blood pooling in hyper-elastic peripheral vessels, compensatory tachycardia, and reduced blood pressure. Others suggest a ‘dysautonomia’ in which an increased sympathetic tone affects the heart only, with a diminished sympathetic response at the vascular level, limiting the ability to increase blood pressure in response to stimuli such as tilting [25,26]. Small fibre peripheral neuropathy, affecting sympathetic fibres, has also been described [27]. Other mechanisms reported in the literature include adrenergic hyper-responsiveness [28], high circulating levels of histamine and mast cell activation [29], and an association with Arnold Chiari malformation, which can be associated with impaired cardiac autonomic control and resolved following decompressive surgery [30,31]. These diverse mechanisms with a paucity of good-quality supportive evidence highlight the need for further research into the pathophysiology of JH to enable appropriate specific therapies to be developed.
Despite published reports and perhaps because of a lack of clarity on mechanisms of the disease, levels of scepticism about JH syndromes and the contribution of physiological abnormalities to the cardiovascular symptom burden are high, and this may be an example of gender differences in symptoms and/or bias in diagnosis [32]. Women remain under-represented in cardiovascular research and suffer from worse cardiovascular outcomes [33,34]. Studies show that women with cardiovascular conditions are more likely to have their symptoms misattributed to anxiety, delaying appropriate diagnosis and management [35,36]. Our findings would support this. It is unclear whether the mental health problems, including anxiety and ‘hypervigilance’ reported in patients with JH, are an intrinsic part of the disorder related to autism [8,9] or are largely a result of chronic stress related to pain and other disabling symptoms with no effective medical recognition or management. Structural and functional brain abnormalities have been reported [37].
This study is limited by the retrospective nature of data collection, relying on electronic medical records including patient-reported medical and social histories. Although efforts were made to address missing data, this was not always possible. Additionally, this study focused solely on patients with JH referred to the syncope clinic, potentially overestimating the prevalence of cardiovascular symptoms in the broader JH population and reducing the apparent prevalence of non-cardiovascular symptoms. No external validation of the JH diagnosis was made, but there is no available genetic or other biomarker for HSD or h-EDS. We highlight the utility of specialised investigations such as tilt-table testing but acknowledge that such resources may not be readily available in all centres.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Carthy F. Mc Mahon C. Geary U. Plunkett P. Kenny R. Cunningham C. Management of syncope in the Emergency Department: A single hospital observational case series based on the application of European Society of Cardiology Guidelines Europace 20091121622410.1093/europace/eun 32319038976 · doi ↗ · pubmed ↗
- 2Probst M. Mower W. Kanzaria H. Hoffman J. Buch E. Sun B. Analysis of emergency department visits for palpitations (from the National Hospital Ambulatory Medical Care Survey)Am. J. Cardiol.20141131685169010.1016/j.amjcard.2014.02.02024698469 PMC 4011931 · doi ↗ · pubmed ↗
- 3Fikree A. Aziz Q. Grahame R. Joint hypermobility syndrome Rheum. Dis. Clin. North. Am.20133941943010.1016/j.rdc.2013.03.00323597972 · doi ↗ · pubmed ↗
- 4Russek L. Errico D. Prevalence, injury rate and symptom frequency in generalized joint laxity and joint hypermobility syndrome in a “healthy” college population Clin. Rheumatol.2016351029103910.1007/s 10067-015-2951-925930211 · doi ↗ · pubmed ↗
- 5Kumar B. Lenert P. Joint Hypermobility Syndrome: Recognizing a Commonly Overlooked Cause of Chronic Pain Am. J. Med.201713064064710.1016/j.amjmed.2017.02.01328286166 · doi ↗ · pubmed ↗
- 6Robinson S. Rana B. Oxborough D. Steeds R. Monaghan M. Stout M. Pearce K. Harkness A. Ring L. Paton M. A practical guideline for performing a comprehensive transthoracic echocardiogram in adults: The British Society of Echocardiography minimum datase Echo Res. Pract.20207 G 59G 9310.1530/ERP-20-002633112828 PMC 7923056 · doi ↗ · pubmed ↗
- 7Kenny R. O’Shea D. Parry S. The Newcastle protocols for head-up tilt table testing in the diagnosis of vasovagal syncope, carotid sinus hypersensitivity, and related disorders Heart 20008356456910.1136/heart.83.5.56410768910 PMC 1760829 · doi ↗ · pubmed ↗
- 8Romeo D.M. Moro M. Pezone M. Venezia I. Mirra F. De Biase M. Polo A. Turrini I. Lala M.R. Velli C. Relationship and New Prospectives in Joint Hypermobility in Children with Autism Spectrum Disorder: Preliminary Data J. Pers. Med.202313172310.3390/jpm 1312172338138950 PMC 10744756 · doi ↗ · pubmed ↗