Traditional Korean Medicine Services and Its Association with Knee Surgery and Opioid Use in Patients with Knee Osteoarthritis: A Nationwide Retrospective Study in Korea
Hwang Woo Seok, Ho-Yeon Go, Won-Hyung Ryu, Yoon Jae Lee, In-Hyuk Ha, Doori Kim

TL;DR
This study found that traditional Korean medicine services may reduce the need for knee surgery and opioid use in patients with knee osteoarthritis.
Contribution
The study provides empirical evidence on the impact of traditional Korean medicine on knee surgery and opioid use in knee osteoarthritis patients.
Findings
TKMS group had significantly lower hazard ratios for knee surgery and opioid use.
Results were consistent across different treatment windows in sensitivity analyses.
TKMS may reduce reliance on high-risk medications and unnecessary surgeries.
Abstract
Objectives: This study aimed to assess the impact of traditional Korean medicine services (TKMS) on subsequent knee surgery and opioid use in patients diagnosed with knee osteoarthritis (KOA). Methods: This retrospective cohort study used National Health Insurance Review and Assessment Service claims data from 2015 to 2017 to identify patients treated for KOA (M17) in 2016. Patients with at least two Korean medicine (KM) clinic visits within 6 weeks of the initial diagnosis formed the TKMS group, while those without visits to KM clinics formed the n group. Propensity score matching (PSM) (1:1) was applied and the incidence of knee surgery and opioid use was followed up for one year. Kaplan–Meier survival curves and Cox proportional hazards models estimated time-to-event outcomes and hazard ratios (HRs). Sensitivity analyses were performed to verify the results across varied treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
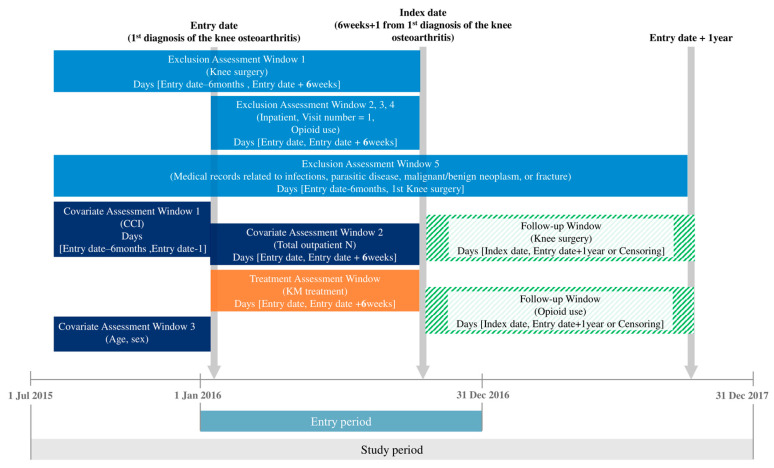 Figure 1
Figure 1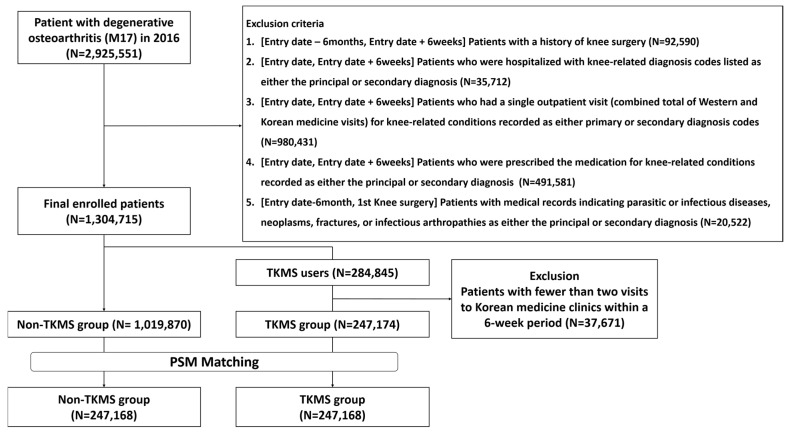 Figure 2
Figure 2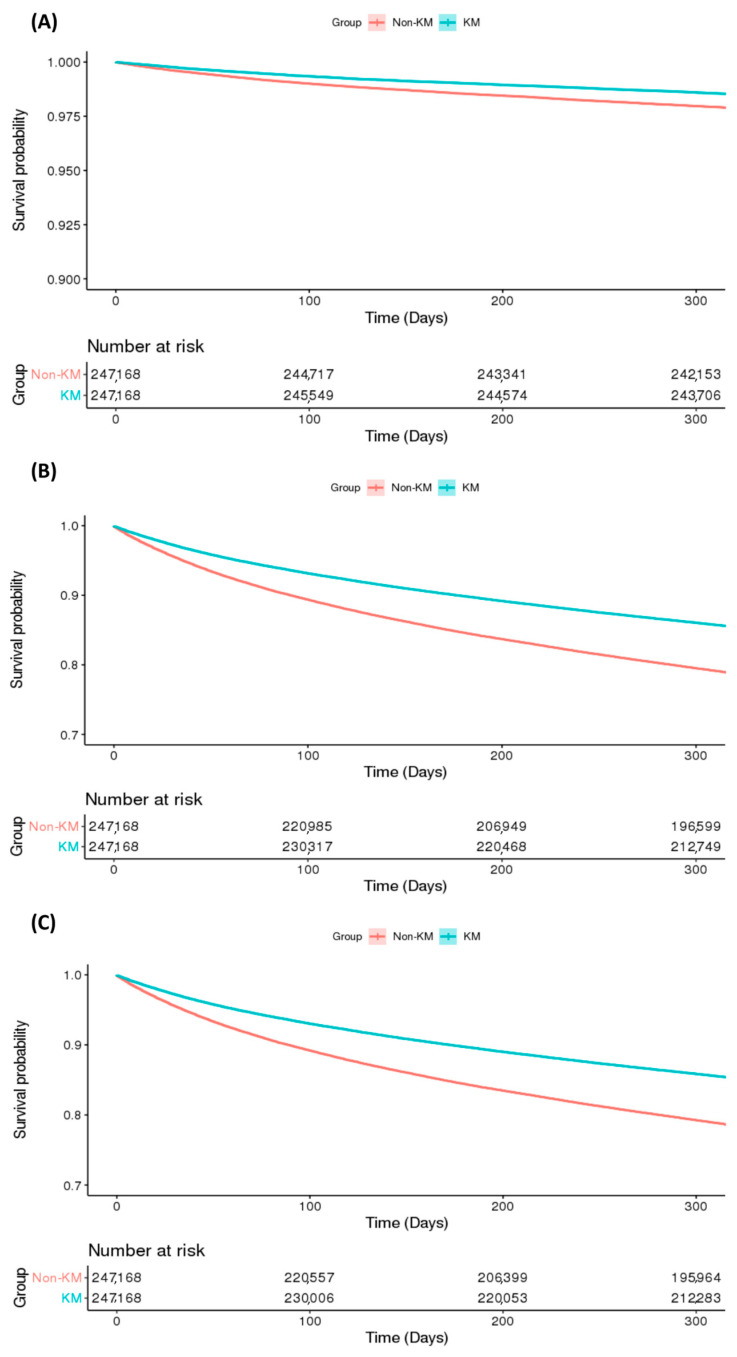 Figure 3
Figure 3- —the Traditional Korean Medicine R&D Program through the Korea Health Industry Development Institute funded by the Ministry of Health and Welfare, Republic of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare and Venom Research
1. Introduction
Knee osteoarthritis (KOA) is a common condition that affects approximately 30% of individuals aged ≥45, characterized by cartilage degradation, bone remodeling, osteophyte formation, joint inflammation, and impaired joint function due to abnormal joint metabolism [1]. KOA represents approximately 80% of global osteoarthritis cases, with its incidence rising alongside obesity and age [2]. In South Korea, KOA is the leading disease among adults ≥65 years, and associated surgeries rank first in terms of costs [3,4], highlighting its significant socioeconomic impact.
The primary goal of treating osteoarthritis is to alleviate symptoms and slow disease progression. Current recommendations for KOA include physical therapy, orthopedic aids, and pharmacotherapy. Surgery is considered when all conservative measures fail [4]. Among nonsurgical treatments, nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and glucocorticoids are most commonly used. From 2000 to 2015 in the UK, 84% of patients with KOA were prescribed opioids [5]. However, the 2021 American Academy of Orthopedic Surgeons (AAOS) Clinical Practice Guidelines on the Management of KOA notes that oral opioids offer limited pain relief or function improvement and carry significant risk of side effects [6]. Typical adverse effects related to opioid therapy comprise sedation, dizziness, nausea, vomiting, constipation, physical dependence, tolerance, and respiratory depression [7]. Therefore, cautious use of opioids is warranted.
Knee arthroplasty is considered the standard surgical intervention for KOA. Although it remains an effective option, it is associated with high costs [8], an increased risk of postoperative infection, and a likelihood that younger patients may require subsequent revision surgeries [9]. Additionally, certain patients may have contraindications due to individual characteristics, warranting careful consideration when designing treatment regimens [10].
Recent analyses of global research trends in nonsurgical treatments for KOA indicate a declining proportion of studies focusing on pharmacotherapy, alongside growing interest in physical therapy and complementary or alternative therapies, such as acupuncture [11]. South Korea operates a dual healthcare system consisting of Western medicine service and traditional Korean medicine service (TKMS), where patients may choose between the two according to their symptoms and preferences [12]. In this context, “TKMS” refers to services provided by licensed Korean medicine (KM) physicians in KM clinics or hospitals, which typically include modalities such as acupuncture, electroacupuncture, pharmacopuncture, Chuna manual therapy, moxibustion, and cupping [12].
Particularly, KOA is one of the conditions for which patients frequently seek TKMS. In 2023, approximately 480,000 patients with KOA utilized TKMS in South Korea [3]. In the global context, other complementary and integrative medicine (CIM) approaches are also used for KOA management, such as Ayurvedic therapies [13] in South Asia, and osteopathic [14] or chiropractic manual therapies [15] in western countries. Within this landscape, KM represents a nationally institutionalized CIM system, integrated into the dual healthcare structure of South Korea and characterized by the delivery of multimodal interventions by licensed physicians.
Evidence supporting the efficacy of TKMS for KOA has been steadily accumulating. A randomized controlled trial (RCT) involving patients with chronic KOA of Kellgren–Lawrence grade 2 or lower demonstrated that acupuncture significantly improved the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores compared with a waiting-list control [16]. In addition, moxibustion was reported to provide greater improvements in pain and function than usual treatments [17], and electroacupuncture showed superior benefits compared with pharmacotherapy [18]. An observational study of 180 inpatients who received TKMS—including acupuncture, herbal medicine, and pharmacopuncture—reported significant improvements in pain, functional indices, and quality of life, with 96% of patients indicating clinical improvement and no adverse events observed [19]. Collectively, these findings suggest that TKMS may serve as an effective and safe treatment option for patients with KOA.
However, while research on acupuncture has been relatively active, fewer studies have investigated other KM modalities such as herbal medicine, pharmacopuncture, or electroacupuncture. In clinical practice in South Korea, patients generally receive not a single modality but a combination of KM interventions; to our knowledge, only one small-scale observational study has reported the effects of such integrative KM interventions [19]. This discrepancy underscores the need for studies assessing the overall impact of TKMS as delivered in real-world multimodal practice. Furthermore, despite the well-known limitations of opioid and surgical treatments including tolerance, side effects, and high costs [7,10], no prior study has examined whether TKMS may mitigate these risks or explored the associations between TKMS with opioid use or surgical interventions. Considering the safety and cost concerns of opioids and surgery, clarifying whether TKMS can reduce reliance on these treatments is of particular clinical and policy relevance.
Therefore, in this study, we utilized customized data from the Health Insurance Review and Assessment Service (HIRA) to investigate the association between TKMS and the risks of knee surgery and opioid use in patients with KOA. We hypothesized that the utilization of TKMS would be associated with a reduced risk of undergoing surgery and using opioids compared with those who did not utilize TKMS.
2. Materials and Methods
2.1. Data Source
This study used a customized dataset from the Health Insurance Review and Assessment Service (HIRA) database (2015–2017). HIRA collects basic demographic details, medical service records, and expense information for each patient in South Korea, based on claims submitted by healthcare providers to the National Health Insurance Service. Researchers can request customized datasets tailored to their studies, which include data from all medical service bills for the entire Korean population. Data requests are handled via the HIRA Open Data Portal [20].
Diagnoses were coded using the Korean Standard Classification of Diseases, Version 7 (KCD-7), based on the International Classification of Diseases, 10th Revision Clinical Modification (ICD-10-CM) [19,21]. Researchers received data with encrypted personal identification numbers to protect privacy. Analyses can be performed remotely at a designated center, with only result tables exportable.
This study was approved by the Institutional Review Board (IRB) of the Jaseng Hospital of Korean Medicine (IRB Approval No.: JASENG 2024-11-011, Date of Approval: 29 November 2024). Patient consent was waived because the analysis was conducted using de-identified and encrypted data, making it impossible to obtain consent from individual patients, and the study posed no risk of harm to patients.
2.2. Study Population
The study population comprised patients who used medical services with KOA as the primary diagnosis in 2016. KOA was defined using the KCD-7 code M17. The entry date was set to be the date of the first visit to a medical institution with osteoarthritis of knee as the primary diagnosis in 2016. To ensure baseline homogeneity of the study population, a 6-month washout period was applied; patients who underwent knee surgery or were diagnosed with malignancies during this period were excluded. Additional exclusion criteria were as follows: patients who had knee surgery, hospital admission, or opioid prescriptions with an M17 diagnosis as the primary or secondary diagnosis within 6 weeks from the entry date; and patients who used medical services for parasitic or infectious diseases, neoplasms, fractures, or infectious arthropathies during the study period from the entry date (Figure 1).
2.3. Intervention
The study population was divided into TKMS and Non-TKMS groups. The TKMS group included patients who used TKM two or more times within 6 weeks of the entry date, with KOA as the primary or secondary diagnosis. TKMS was defined as having claims records of visits to KM clinics or hospitals, regardless of the specific modalities received. Detailed treatment information, such as acupuncture or cupping, was not considered in this classification. The Non-TKMS group consisted of patients who did not visit KM institutions within 6 weeks of the entry date but had the same diagnosis criteria.
2.4. Outcome Measures
Three outcomes were measured: knee surgery, opioid use, and either knee surgery or opioid use. Knee surgery included total knee replacement, partial knee replacement, revision knee replacement, knee osteotomy, knee arthroplasty, arthrodesis, meniscectomy, meniscal suture, meniscal transplantation, and cruciate ligament reconstruction and repair. Opioid use was defined as having at least one prescription for medications classified under anatomical therapeutic chemical (ATC) code N02A. The ATC system, overseen by the WHO, is an international standard that categorizes active substances according to the organ or body system on which they act and their therapeutic, pharmacological, and chemical properties [22]. In this system, cod N02A specifically refers to opioids [23]. The procedure codes for knee surgeries are summarized in Supplementary Table S1. The follow-up window covered knee surgery and opioid use.
The composite outcome of “either knee surgery or opioid use” was included to capture overall treatment escalation, as both events represent high-risk or invasive management strategies in KOA. This composite endpoint allowed for a more comprehensive assessment of the potential association between TKMS utilization and the reduced need for such treatments.
2.5. Statistical Analysis
Propensity score matching (1:1) was performed based on age, sex, Charlson comorbidity index (CCI), and the number of outpatient visits over a 6-week period. The CCI was calculated based on medical records from the 6 months preceding the entry date. Outpatient visits for relevant diagnoses (Korean and Western medicine) were summed and grouped into three categories: 2–5, 6–11, and ≥12 visits. Baseline characteristics after propensity score matching were compared using McNemar’s test and standardized mean differences (SMDs) [24].
Survival analysis was performed, with time to knee surgery, opioid use, and compound events of knee surgery or opioid use plotted using Kaplan–Meier curves [25]. The log-rank test was used to assess differences between groups. Cox proportional hazards regression was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for knee surgery and opioid use. When calculating HRs, sex, age, CCI, and number of outpatient visits served as covariates for adjustment in sensitivity analyses. Before performing Cox proportional, the proportional hazards (PHs) assumption was evaluated along log–log plots.
Sensitivity analyses classified groups based on whether patients accessed TKMS (visiting KM institutions) within 4-, 8-, and 10-week TKMS treatment windows, instead of the standard 6 weeks. These time frames were determined through internal discussion among the research team. For each window, event incidence (knee surgery, opioid use, or knee surgery or opioid use) and HRs were calculated. All statistical analyses were performed using the SAS statistical software suite (SAS 9.4; SAS Institute, Inc., Cary, NC, USA).
3. Results
3.1. Baseline Statistics
In 2016, 2,925,551 patients received medical care for KOA as their primary diagnosis. After applying the exclusion criteria, 1,304,715 remained: 247,174 in the TKMS group and 1,109,870 in the Non-TKMS group. After 1:1 propensity score matching by age, sex, CCI, and the number of outpatient visits over a 6-week period, 494,336 patients (247,168 per group) were included in the final dataset (Figure 2).
After propensity score matching, the SMDs for sex, age, insurance payment type, CCI score, and number of outpatient visits were below 0.1 (Table 1, Table S1), indicating no statistically significant differences between groups.
3.2. Comparison of Knee Surgery and Opioid Use by TKMS Use
Kaplan–Meier survival analysis revealed that the TKMS group had a lower cumulative incidence of knee surgery, opioid use, and compound events compared to the Non-TKMS group (log-rank test, p < 0.001; Figure 3). Cox proportional hazards modeling confirmed statistically lower HRs in the TKMS group for knee surgery (HR = 0.69; 95% CI: 0.66–0.72), opioid use (HR = 0.65; 95% CI: 0.65–0.66), and compound events (HR = 0.66; 95% CI: 0.65–0.67) compared to the Non-TKMS group (Table 2). The PH assumption was verified using a log–log plot (Figure S1).
3.3. Sensitivity Analysis
A sensitivity analysis was conducted by changing the TKMS group’s index date to 4, 8, or 10 weeks after the entry date. In all scenarios, TKMS use lowered the HRs for knee surgery, opioid use, and compound events (Table 3). Survival analyses confirmed significantly lower HRs in the TKMS group compared to the Non-TKMS group for knee surgery, opioid use, and compound events (p < 0.001; Tables S3–S5).
4. Discussion
This study assessed the impact of TKMS on the incidence of subsequent knee surgery and opioid use in patients with KOA. The TKMS group had a significantly lower risk of knee surgery and opioid use compared to the Non-TKMS group.
This study demonstrated that the utilization of TKMS was associated with a reduced risk of surgery in patients with KOA. Although surgical treatment may be considered when nonsurgical management fails, surgery does not necessarily guarantee improved outcomes. Previous studies have reported variable efficacy between arthroscopic surgery and conservative treatment [26]. Moreover, surgery can increase the risk of falls in patients with KOA [26]. Arthroscopy has been shown to triple the risk of progression to total knee arthroplasty (TKA), and TKA itself is associated with a four-fold increase in complications during the follow-up period [27].
Surgery is also linked to considerable socioeconomic costs. A previous study reported that patients who underwent TKA have comparable medical expenses and income to the control group up to 3 years before surgery but consistently experience higher medical costs and reduced income after surgery. This was attributed to factors like lost earnings from work, requirements for home care, and increased medication use [28]. These reports suggest an increase in direct surgical expenditures and ongoing socioeconomic costs after surgery.
Utilization of TKMS was also associated with a reduced risk of opioid use in patients with KOA. Long-term opioid use has been reported in more than 800,000 patients with KOA in the United States [29]. However, opioids have a higher incidence of side effects than non-opioids, without offering superior efficacy in terms of pain relief or functional improvement [30]. Additionally, in patients with osteoarthritis, opioids can cause gastrointestinal disorders, nausea, vomiting, loss of appetite, dermatologic adverse events, and central nervous system disorders [31]. Considering these safety concerns, a growing emphasis has been placed on effective management of opioid use and exploring alternative treatment options [32]. The current study indicates that TKMS may be an effective alternative treatment strategy for reducing opioid use.
On the other hand, among older adults, who have a high prevalence of KOA, polypharmacy—the use of multiple drugs or those exceeding medical necessity—is common due to multiple underlying conditions [33]. Polypharmacy may lead to issues such as drug–drug interactions, toxicity, falls, injuries, cognitive impairment (such as delirium), and poor adherence to medication regimens [34]. Excessive polypharmacy has been associated with reduced nutritional status, decreased functional ability, and impaired cognitive capacity compared to those not experiencing polypharmacy [35]. Therefore, lowering the risk of opioid use has meaningful implications for addressing polypharmacy-related issues. Moreover, one study reported that acupuncture provided greater pain reduction than NSAIDs in patients with KOA [36], raising the possibility that TKMS use may also be associated with reduced use of non-opioid analgesics such as NSAIDs. Considering that a substantial proportion of patients with chronic pain are exposed to polypharmacy [37], our findings suggest that TKMS use could contribute to mitigating polypharmacy. Further related research is needed.
Acupuncture, a major KM treatment modality, helps manage osteoarthritis pain and prevent functional issues by improving joint blood flow, regulating inflammatory cytokine levels, and activating pain-modulating pathways to reduce the nociceptive response in the central nervous system [38,39]. Recent research also supports the effectiveness of other KM modalities, such as herbal medicine, pharmacopuncture, and Chuna manual therapy, for KOA. Herbal medicines exert chondroprotective effects on the cartilage through their anti-inflammatory and antioxidant actions [40]. Pharmacopuncture combines mechanical stimulation with pharmacological action to relieve pain and restore joint function [41]. Chuna manual therapy can correct misaligned joints and reduce mechanical stress by relieving muscle imbalances [42,43]. The analgesic, anti-inflammatory, and joint function-enhancing effects of these KM modalities provide a plausible explanation for the observed associations between TKMS utilization and the reduced need for surgery and opioid use among patients with KOA.
Randomized controlled trials have reported that acupuncture can alleviate pain and enhance physical function in patients with KOA. An individual patient data meta-analysis examining acupuncture’s efficacy for four chronic pain conditions reported that the effects of acupuncture were sustained over time [44]. Indeed, electroacupuncture and manual acupuncture are reportedly more effective than sham acupuncture in reducing pain and improving function [45]. However, most previous research has focused on short-term and subjective outcomes or measures, with relatively little known about objective and long-term outcomes such as surgery or medication use. Therefore, the value of the present study lies in the use of large-scale NHI claims data to evaluate clinically relevant objective outcomes (effect of TKMS on surgery and opioid use).
This study has several limitations. First, as a retrospective cohort study, the results should be interpreted with caution. In particular, the NHI claims data lack details related to non-reimbursed treatments and specific KM treatment modalities, making it difficult to analyze the efficacy of individual intervention. Treatment frequently used in TKMS such as pharmacopuncture and herbal medicine, are non-reimbursed and thus not captured in claims data. Accordingly, we defined TKMS solely based on visits to KM clinics or hospitals rather than the receipt of specific modalities. Nevertheless, considering that patients in South Korea typically receive integrated TKMS, including acupuncture, pharmacopuncture, and Chuna manual therapy, the study design was deemed suitable for real-world clinical practice.
Second, due to the inherent limitations of claims data, patient-reported outcomes such as pain intensity, functional scores, or quality of life could not be assessed. It is therefore unclear whether the lower incidence of surgery in the TKMS group reflects true symptom improvement or a preference among TKMS users to avoid surgery. Future studies using hospital-based electronic medical records that include non-reimbursed treatment details and patient-reported outcomes are warranted.
Third, we attempted to minimize selection bias between patients who preferred TKMS and those who did not through propensity score matching. However, while this method adjusts for measured confounders, it cannot eliminate the possibility of residual confounding by unmeasured factors [46]. Patient preferences for non-invasive treatments, health literacy, socioeconomic status, and the severity of KOA are potential unmeasured variables that may have influenced the observed association.
Finally, regarding opioid outcomes, our analysis defined opioid use as having received at least one prescription for an opioid medication. Information on treatment duration or cumulative dose was not available. Considering that short-term and long-term opioid use carries very different clinical implications, including the risk of substance abuse [46], a more granular analysis would have provided greater clarity on the role of TKMS in reducing opioid use.
Nevertheless, this is the first study to show that TKMS are associated with lower rates of knee surgery and opioid use among patients with KOA, based on large-scale NHI claims data from HIRA. The main strengths of this study are the use of objective outcomes—surgery and opioid use—evaluated at the national population level, and the consistent hazard ratios across sensitivity analyses with varying treatment windows, which reinforce the robustness of the findings. Further research should include prospective cohort studies and Randomized controlled trials with comprehensive treatment records, patient characteristics, symptom severity, and radiographic evidence.
5. Conclusions
The analyses in this study demonstrate that TKMS use in patients with KOA may be associated with reduced subsequent knee surgeries and opioid use. These findings offer insights for clinicians, patients, and policymakers for consideration when evaluating treatment options and developing healthcare policies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Katz J.N. Arant K.R. Loeser R.F. Diagnosis and treatment of hip and knee osteoarthritis: A review JAMA 202132556857810.1001/jama.2020.2217133560326 PMC 8225295 · doi ↗ · pubmed ↗
- 2Cui A. Li H. Wang D. Zhong J. Chen Y. Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studiese Clinical Medicine 20202910058710.1016/j.eclinm.2020.10058734505846 PMC 7704420 · doi ↗ · pubmed ↗
- 3Korean Statistical Information Service Available online: https://kosis.kr/stat Html/stat Html.do?org Id=350&tbl Id=TX_35001_A 061&conn_path=I 2(accessed on 28 August 2025)
- 4Michael J.W. Schlüter-Brust K.U. Eysel P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee Dtsch. Aerzteblatt Online 201010715216210.3238/arztebl.2010.0152 PMC 284186020305774 · doi ↗ · pubmed ↗
- 5Taqi A.O.H. Knaggs R. Trends in opioid prescribing in primary care patients with knee osteoarthritis: A population based observational study Value Health 201720 A 540A 54110.1016/j.jval.2017.08.804 · doi ↗
- 6Brophy R.H. Fillingham Y.A. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition J. Am. Acad. Orthop. Surg.202230 e 721e 72910.5435/JAAOS-D-21-0123335383651 · doi ↗ · pubmed ↗
- 7Benyamin R. Trescot A.M. Datta S. Buenaventura R.M. Adlaka R. Sehgal N. Glaser S.E. Vallejo R. Opioid complications and side effects Pain Physician 200811 S 10510.36076/ppj.2008/11/S 10518443635 · doi ↗ · pubmed ↗
- 8Kan H. Chan P. Chiu K. Yan C. Yeung S. Ng Y. Shiu K. Ho T. Non-surgical treatment of knee osteoarthritis Hong Kong Med. J.20192512713310.12809/hkmj 18760030919810 · doi ↗ · pubmed ↗