Diagnostic Utility of Red Flags for Detecting Spinal Malignancies in Patients with Low Back Pain: A Scoping Review
Gianluca Notarangelo, Michele Margelli, Giuseppe Giovannico, Francesco Bruno, Claudia Milella, Daniel Feller, James Dunning, Lorenzo Storari, Firas Mourad, Filippo Maselli

TL;DR
This review examines how red flags can help identify spinal cancer in patients with low back pain, finding that a history of cancer is the most reliable indicator.
Contribution
The study systematically evaluates the diagnostic utility of red flags for spinal malignancies in low back pain patients.
Findings
Cancer prevalence among low back pain patients ranges from 0.1% to 1.6%, with metastatic disease being most common.
A prior history of cancer is the most reliable red flag with high specificity.
Combining red flags improves diagnostic accuracy, but most have poor standalone performance.
Abstract
Introduction: While low back pain (LBP) is most often associated with musculoskeletal issues, in a minority of cases, it can be caused by serious underlying conditions such as cancer. Recognizing malignancy early remains a major clinical challenge, as the warning signs, known as red flags (RFs), are often vague and inconsistent. Methods: A comprehensive search of six databases (PubMed, Scopus, Google Scholar, Web of Science, Cochrane Library, and SciELO) and grey literature was conducted for studies published from January 1999 to March 2025. Eligible sources included studies describing adult patients with cancer presenting with LBP. Study selection and data extraction were independently performed by two reviewers. Results: We included 70 studies, most of which were case-based, along with reviews and observational research. In these studies, cancer prevalence among patients with LBP…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
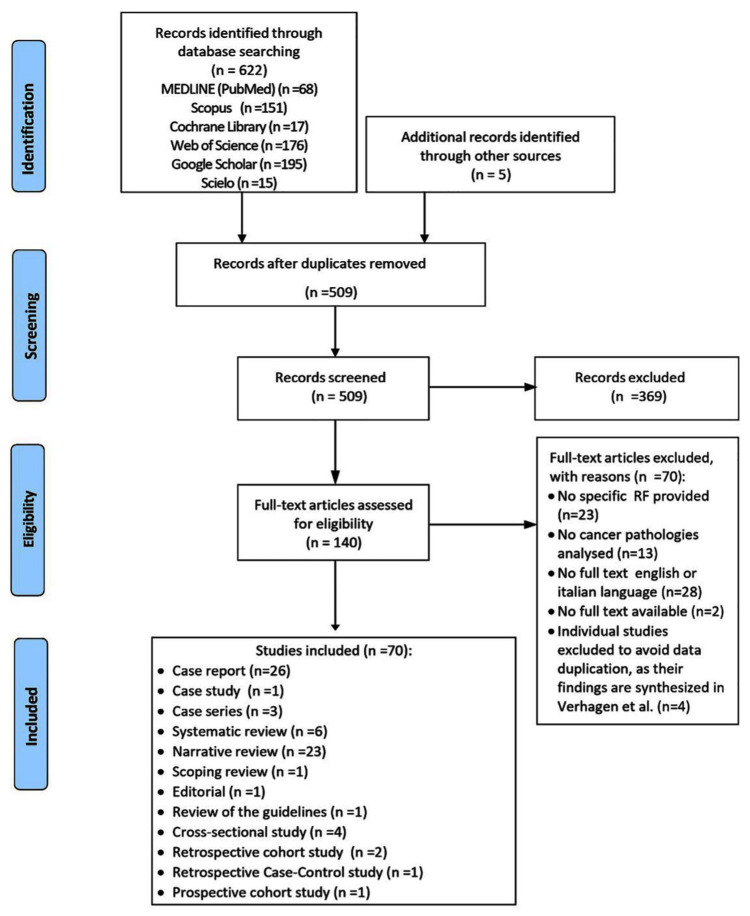 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Spine and Intervertebral Disc Pathology · Anesthesia and Pain Management
1. Background
Low back pain (LBP) refers to pain or discomfort occurring between the lower ribs and the gluteal folds with or without leg pain [1,2,3,4,5]. When no specific cause, such as infection, tumor, fracture, peripheral arterial disease, or nerve involvement, is identified, it is classified as non-specific LBP [1,2,3,4,5]. In recent years, LBP has been recognized as the most common musculoskeletal disorder and the leading cause of disability worldwide [6,7]. In the primary care setting, between 1% and 5% of all patients who present with LBP have a serious spinal pathology [8]. Among these serious conditions, cancer is the second most frequently reported cause mimicking LBP, with prevalence reported up to 2.1% of cases, while spinal fractures are the most frequent, with prevalence up to 7.2% [9,10]. According to the World Health Organization (WHO), cancer remains the second leading cause of death globally [11]. These serious conditions are often associated with pathognomonic signs/symptoms or red flags (RFs), as they serve as clinical alerts to prompt referral to a medical physician for further investigation [12]. Physiotherapists must be able to recognize sinister presentations that may require further investigation or urgent referral [13].
Delayed recognition of spinal malignancies may result in misdiagnosis and rapid disease progression without the appropriate intervention; therefore, for the primary purpose of identifying relevant RFs, a thorough history and physical examination is essential when encountering patients with LBP [14]. Notably, when only low- or intermediate-risk RFs are present, a watchful waiting approach may be appropriate to monitor progress to avoid a delayed or missed diagnosis of a serious disease [15]. When RFs with high diagnostic value are identified, a timely investigation and referral to a medical physician or spinal specialist is warranted. Screening for these indicators must be a priority and core responsibility for physiotherapists who are managing patients with spinal pain [16]. However, screening tools have limitations and may not be sufficient to definitively rule out serious underlying conditions [17].
This scoping review aimed to map and synthesize the literature; furthermore, it aimed to describe the relevant RFs associated with cancer-related cases of LBP.
2. Materials and Methods
This scoping review has been conducted in accordance with the methodology from the Joanna Briggs Institute (JBI) [18]. In addition, the “Preferred Reporting Items for Systematic Reviews and Meta Analyses extension for Scoping Reviews (PRISMA ScR)” checklist [19] has been used for reporting the findings.
2.1. Research Question
The following research question was formulated:
“What is known from the current literature on RFs for cancer in patients presenting with LBP?”
2.2. Protocol and Registration
The scoping review protocol was published on 1 September 2024 and is available online at: medRxiv 2024.09.01.24311072 [20].
2.3. Inclusion Criteria
Studies were included if they fulfilled the following criteria regarding population, concept, and study context (PCC criteria):
Population: patients of any age and gender.
Concept: studies that have explored and reported RFs associated with LBP caused by any cancer pathology. We defined RFs as clinical findings—i.e., signs and/or symptoms from the history and/or physical examination—that may indicate serious conditions (e.g., cancer) and are used to support early detection and appropriate referral [12].
Context: studies conducted in any setting and geographic context, published in English or Italian, from January 1999 to March 2025.
2.4. Exclusion Criteria
Studies that did not meet the above PCC criteria were excluded.
2.5. Search Strategy
The literature search was conducted on the following databases until 15 March 2025: MEDLINE (via PubMed), Scopus, Google Scholar, Web of Science, Cochrane Library and SciELO.
The complete search strategy for all databases can be found in the Appendix A.
2.6. Selection of Studies
Search results were imported into EndNote V.X9 (Clarivate Analytics, PA, USA), and duplicates were removed. Two independent authors (GN, FB) screened records at two levels (title/abstract and full-text) using Rayyan [21]; disagreements were resolved by a third author (FM). Study design classification followed authors’ descriptions and methodology. Systematic reviews were identified by structured search strategies, eligibility criteria, and formal quality or bias assessment, in line with PRISMA [22]. Scoping reviews were classified according to exploratory aims and broad inclusion criteria (PRISMA-ScR [19]), while narrative reviews were defined as overviews without reproducible methodology [23]. Additional articles were categorized as guideline review or editorial.
2.7. Data Extraction
Data extraction followed the PCC model using a standardized Excel sheet. Recorded information included study details (author, year, country, design), population characteristics, and clinical data (case description, diagnosis, out-comes). Diagnostic accuracy measures were noted only when explicitly reported in the original studies. Two independent authors (CM, GG) extracted data, with disagreements resolved by a third author (FM). Full data are available in Appendix B.
2.8. Data Synthesis
Data were summarized and collected as a descriptive analysis. A mapping of the data was carried out that showed the distribution of the studies by publication period, study design and topics. A thematic synthesis of cancer-specific RFs was performed in patients presenting with LBP. Additional descriptive analyses of subgroups (e.g., gender, pathology, etc.) were reported. In line with the Joanna Briggs Institute (JBI) methodology for scoping reviews [18], no formal assessment of methodological quality or risk of bias was performed, as the aim was to map and synthesize the available evidence rather than appraise the study validity.
3. Results
3.1. Characteristics of the Included Studies
The PRISMA-ScR flowchart (Figure 1) illustrates the study selection process. From 627 records initially identified (including grey literature), 118 duplicates were removed. Following title/abstract and full-text screening, 70 studies fulfilled the eligibility criteria and were included in this scoping review. Four studies (three case reports [24,25,26] and one case study [27]) were excluded at this stage as their data were already synthesized in Verhagen et al.’s systematic review [28]. Detailed reasons for exclusion are provided in Appendix C. The selected studies include 27 case reports [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55], 3 case series [56,57,58], 6 systematic reviews [10,17,28,59,60,61], 1 scoping review [62], 23 narrative reviews [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83] 1 review of the guidelines [84], 1 editorial [85], 4 cross-sectional studies [86,87,88,89], 2 retrospective cohort studies [90,91], 1 prospective cohort study [92], and 1 case–control study [93].
The studies were conducted primarily in the United States (39%), Italy (10%), and Brazil (8%). Thirty of the included studies were conducted from 1999 to 2014, while the remainder were conducted in the last decade (Table 1).
3.2. Patient Assessment and Clinical Findings
3.2.1. Case Reports, Case Series, Case Studies
Several comorbidities were reported, including cardiac or vascular diseases (i.e., hypertension and cerebrovascular disorders [31,36,37,56]), type 2 diabetes [31,37,45] and gastrointestinal diseases [31,39,56]. In addition, hip dysplasia [55], osteoporosis [49,55], obesity [34,37], and gynecological diseases [32,42] were reported. Neurological disorders (cerebrovascular disease) [31], kidney disease (presence of stones) [36], hypothyroidism [36], and a rheumatic disease (scleroderma with Raynaud’s phenomenon) [55] were also reported. Notably, 16 patients reported no comorbidities.
Considering laboratory tests, blood work was requested in 17 patients and biopsies were requested for 20 patients. The most requested imaging examinations were magnetic resonance imaging (MRI) and X-rays in 23 cases, and computed tomography (CT) in 18 cases. There were 23 cases of direct access to hospitals, 3 cases of direct access to a physiotherapist, and 6 cases of direct access to a chiropractor. Two patients reported a history of smoking or alcohol use [34,52].
In patients with LBP associated with underlying serious pathologies, Table 1 demonstrates that the presence of sinister signs and symptoms has a heterogeneous distribution. Lumbar tenderness was reported in 7 cases [29,31,34,35,43,55,56] and the presence of radiating pain was reported in 14 cases [31,32,33,35,36,38,41,43,46,47,50,53,56] (2 cases in the same study [56]). Neurological signs (such as reduced sensitivity, loss of sphincter control, gait impairment, and changes in osteotendinous reflexes) were reported in 22 cases [29,30,31,32,33,35,36,38,39,40,41,46,47,49,50,51,52,53,54,55,56]; muscle weakness was reported in 9 cases [31,33,38,46,53,54,55,56]. Both findings included two patients described in the same case study [56].
Patient characteristics (e.g., gender, age, setting, comorbidities, clinical signs, imaging findings, and outcomes) from the studies included in this review have been summarized in Table 1. Additionally, Table 1 summarizes the 30 case-based studies (26 case reports, 1 case study, and 3 case series) included in the analysis; notably, there are 32 patients in total as two studies described more than one case [56,57] and in one case series [58] only one patient presented with LBP.
3.2.2. Observational Studies
In addition to case-based studies, eight observational studies offered further insight into patient assessment and clinical presentation in broader populations.
Chu et al. conducted a retrospective analysis of 20 patients with cancer-specific LBP in chiropractic clinics [88]. All patients underwent MRI, and 18 reported symptoms radiating to the lower limbs; further, the pain onset was classified as acute (less than 6 weeks) in 10 cases and chronic (more than 12 weeks) in 18 cases. Reported comorbidities included a history of cancer and hypertension (three cases each), hyperlipidaemia, cardiovascular disease, and diabetes. No comorbidities were reported in 12 of the patients. Heterogeneous RFs were found, including progressive symptoms in three patients, while night pain, pain at rest, bilateral radiculopathy, and increased urinary frequency were each reported in one patient [88].
Reito et al. evaluated 900 emergency department visits with acute or subacute atraumatic low back pain with or without radicular symptoms and found only 3.7% of cases were due to a specific spinal pathology. Nevertheless, the low incidence of spinal pathologies reflects the limited predictive accuracy of RF findings in this setting [86].
In patients undergoing surgery for spinal metastases, Van Tol et al. reported that back pain was the most common presenting symptom and was often accompanied by neurological deficits; however, the referral documentation frequently failed to record these specific clinical findings, even when they were present at the time of patient assessment [89]. Likewise, Henschke’s prospective cohort of 1172 primary care patients with acute LBP reported serious spinal pathology, such as cancer, in patients over the age of 50, with a history of malignancy, or with unexplained weight loss [92].
Premkumar et al. observed that malignancy-related LBP is often clinically indistinguishable from benign presentations, with RFs like prior cancer history or advanced age not always accompanied by specific alarming signs [90]. Collectively, these studies confirm that cancer-related LBP frequently mimics non-specific presentations, with RFs and comorbidities emerging only after more in-depth assessment [90,92].
3.3. Cancer-Specific RFs
3.3.1. Case Reports, Case Series, Case Studies
The most frequently reported RF was “neurological signs” cited in 22 cases. Other relevant RFs were: “history of cancer”, “family history of cancer”, “failure of conservative treatment”, “age over 50”, “progressive worsening pain”, “night pain”, pain duration over 3 months, and “severe and continuous pain”.
Table 2 below summarizes the RFs identified in the included case reports, case studies, and case series. For each case, RFs were either explicitly reported in the article or inferred from the information provided in the onset, clinical presentation, and physical examination. All terms were standardized to predefined terminology. In addition to the column indicating whether each RF was reported by the authors because of clinical findings during the history and physical examination, a further column specifies the number of studies in which the RF was not reported.
3.3.2. Observational Studies
Several primary studies investigated the diagnostic performance of RFs in patients with LBP, with considerable variability in sensitivity (Se), specificity (Sp), and likelihood ratios (LR) depending on the individual feature and the study setting.
Demographic-related RFs such as “age > 50” were among the most frequently examined. Notably, in the prospective cohort by Henschke et al. [92], this RF (i.e., “age > 50”) showed a specificity of 0.660 (95% CI 0.630–0.690), whereas, in Premkumar et al. [90], it dropped to 0.326 with an LR+ of only 1.060, suggesting poor diagnostic accuracy when considered alone.
Raising the threshold to “age > 70” increased the specificity to 0.795 (0.950 in Henschke’s study [92]); however, the sensitivity dropped to 0.220 in comparison to the previous “age > 50” in the same study. Demographic-related RFs can be viewed in Table 3.
Medical history-related RFs, particularly a “history of cancer,” consistently demonstrated the strongest diagnostic accuracy across studies. In Premkumar et al. [90], a specificity of 0.956 and an LR+ of 7.250 were reported, with Tsiang et al. [93] reporting similar values for diagnostic accuracy (Sp 0.778; Se 0.917). Although Henschke et al. [92] found zero sensitivity for this indicator, the specificity remained high at 0.960, supporting its strong role of ruling in a diagnosis when a history of cancer is confirmed. Likewise, “unexplained weight loss” showed poor sensitivity across all studies (0.082 in Premkumar [90], 0.000 in Henschke [92]), but excellent specificity (0.956 in Premkumar [90] and 1.000 in Henschke [92]), reinforcing its limited value in ruling out malignancy, but strong utility in reinforcing diagnostic suspicion when present. Clinical symptoms such as night pain and pain at rest were also explored, though with less favorable results. Tsiang et al. [93] found that night pain had a sensitivity of 0.542 and specificity of 0.496 indicating lower diagnostic utility. Notably, pain at rest fared even worse with a sensitivity of 0.250. Among neurological or systemic signs, urinary retention possessed high specificity (0.958) but low sensitivity (0.042).
Overall, and in patients with LBP associated with underlying malignancy, RFs seem to be more useful for ruling in rather than ruling out (i.e., screening) serious pathologies. Medical history-related RFs are reported in Table 4.
The physical examination-related RFs were generally consistent with this trend. In the cohort by Henschke et al. [92], altered sensation had a high specificity (0.980), but close to zero sensitivity. More specifically, this impairment does not effectively exclude malignancy; however, the presence of such should heighten concern. No additional relevant data on physical examination-related RFs were reported in the other included primary studies. Physical examination-related RFs can be consulted in Table 5.
Importantly, combining multiple RFs considerably improved diagnostic performance. Premkumar et al. [90] demonstrated that the combination of “history of cancer” with “unexplained weight loss” gave an LR+ of 10.250, significantly increasing the post-test probability of spinal malignancy. The diagnostic accuracy of combined RFs is reported in Table 6.
3.3.3. Review Studies
Additional combinations of RFs have been described in secondary literature, although these findings were not extracted from primary studies. Importantly, the primary studies referenced within these secondary sources are not included among the studies selected for the present scoping review; therefore, their reported diagnostic values should be interpreted with caution and considered as indirect evidence rather than as part of the primary data synthesis.
These proposed clusters may serve as reference points for clinical reasoning, but their diagnostic value should be interpreted with caution, given the absence of original patient-level data. For instance, Delladio et al. [82] reported a combination including age > 50 years, history of cancer, unexplained weight loss, and failure to improve after one month, yielding a sensitivity of 1.000, specificity of 0.600, LR+ of 2.400, and LR− of 0.060. Similarly, the systematic review by Henschke et al. [60] described the same cluster with a sensitivity of 1.000, though without a corresponding specificity estimate. In line with these observations, Finucane et al. [63] similarly noted that most RFs beyond ‘history of cancer’ remain poorly validated and often present too late to aid early detection. The diagnostic accuracy of combined RFs is reported in Table 7.
3.4. Differential Diagnosis
3.4.1. Case-Based Studies
The most frequently reported diagnosis was “secondary metastatic lesions” (17 cases), as described in 16 different sources [29,30,31,34,35,36,39,40,41,44,45,47,48,52,55,56]; notably, one of these studies reported two distinct metastatic cases [56], accounting for the total of 17. Primary cancers were the second most cited diagnosis, with 15 cases identified across the literature. The different cancer-related diagnoses included Ewing’s sarcoma [32,41,51], osteoid osteoma [57], lumbar schwannoma [33,43], and primary bone liposarcoma [38]. Other rare conditions reported in single cases were cavernous angioma [46], giant cell cancer [54], spinal neurofibroma [53], mastocytosis [49], renal angiomyolipoma [50], and leukemia [44]. The metastatic lesions were highly heterogeneous and originated from various primary sites, including the stomach, lung, colon, prostate, breast, pancreas, urothelium, appendix, pelvis, penis, and spine.
3.4.2. Observational Studies
Among the observational studies included, several provided data relevant to the differential diagnosis of malignancy-related LBP. In the study by Premkumar et al. [90], conducted on a cohort of 2505 patients, 35 were diagnosed with serious pathology. More specifically, metastatic disease was found in 18 cases (51%), while primary cancers such as lymphoma (2 cases), multiple myeloma (2 cases), and Ewing sarcoma (1 case) were much less common. The remaining 12 cases included infections, fractures, and inflammatory pathologies.
Henschke et al. [92], in a prospective cohort of 1172 patients in a primary care setting, reported 11 cases of serious spinal pathology. Notably, only two cases were cancers: one individual with prostate cancer and one individual with multiple myeloma. The study confirmed that cancer is rare in this context (around 0.17%), which highlights how difficult it can be to spot serious conditions during the initial evaluation.
Tsiang et al. [93], in a retrospective analysis of 7221 self-reported LBP cases, identified 20 patients with confirmed cancer-related diagnoses. Of these, 18 were secondary metastatic lesions (90%), while only two (10%) were due to primary cancers. Although the exact distribution was not detailed, the most frequently involved cancers were prostate, breast, lung, and gastrointestinal.
Reito et al. [86] investigated 790 patients attending the emergency department and identified 79 cases (10%) of specific spinal pathologies. Among these, 13 patients (1.6%) were diagnosed with cancer, including six with metastatic disease, four with multiple myeloma, and two with lymphoma. Other serious conditions included vertebral fractures (n = 19) and spinal infections (n = 6), illustrating the broad spectrum of differential diagnoses in acute atraumatic low back pain.
Chu et al. [88] conducted a retrospective study within chiropractic clinics, analyzing 20 patients with LBP ultimately diagnosed with malignancy. Notably, 18 of these patients (90%) had metastatic lesions, while only 2 (10%) had primary cancers. Furthermore, most lesions originated from prostate, breast, lung, and urogenital cancers. This study also revealed that many patients first sought help from chiropractors, suggesting that non-medical settings can play an important role in raising early suspicion and prompting referral for serious conditions.
Van Tol et al. [89] retrospectively analyzed 389 patients treated surgically for symptomatic spinal metastases. The distribution of primary cancer sources was as follows: urogenital cancers (21.9%), hematological malignancies (19.8%), breast cancer (18.8%), lung cancer (14.9%), gastrointestinal cancer (6.4%), gynecological cancer (1.5%), and other or unspecified causes (16.7%). This study emphasized the diagnostic complexity and delayed diagnoses frequently observed in cancer-related LBP.
Finally, Erausquin et al. [91] presented a case series of Naka grade III lumbar epidural lipomatosis, of which only one case reported LBP as a primary symptom. The diagnosis was a benign epidural lesion, suggesting how important it may be to also consider rare, non-cancer causes when evaluating patients with LBP.
4. Discussion
This scoping review aimed to map the existing literature about RFs described in patients with cancer-related LBP. Although the studies varied considerably in their methodological design and level of detail in reporting, formal quality appraisal was not undertaken, in line with current JBI guidance for scoping reviews [18]. Most of the available evidence comes from case-based studies; nevertheless, while these studies are useful for illustrating rare or atypical cases, they are observational in nature and do not provide experimental data to support broad conclusions. Among the 32 patients described in the case-based literature, secondary spinal malignancies represented the most frequent diagnosis, often presenting with nonspecific symptoms such as persistent pain, neurological deficits, or insidious onset. The variety of comorbidities and patient ages highlights how complex these cases can be and how much their presentation can differ from one another. The frequent use of advanced imaging techniques and biopsies indicates that initial presentations were often nonspecific, making early clinical suspicion of malignancy unlikely and sometimes leading to diagnostic delay. The observational studies included in this review collectively offer insight into how cancer is diagnosed in patients with LBP and the types of cancers most frequently identified. Across these studies, metastatic disease emerged as the predominant finding, while primary cancers such as prostate, breast, lung, gastrointestinal, hematologic, and urogenital malignancies were less common [86,87,88,89,90,91,92,93]. The study by Chu [88], which examined both individual case presentations and a broader retrospective sample (n = 7221), confirmed the low overall prevalence of cancer in LBP (0.1–1.6%), but also emphasized that metastatic disease was by far the most common serious diagnosis when cancer was present. In van Tol’s retrospective analysis of surgically treated patients with spinal metastases [89], breast, lung, urogenital, and hematologic cancers emerged as the most frequent primary sites. These findings align with what was observed in the case-based literature and further support the idea that spinal metastases often develop from common types of systemic cancer [29,30,31,35,36]. Similarly, Reito et al. [86] reported hematologic and lung cancers among patients with acute LBP in the emergency setting, reinforcing the importance of considering these etiologies in differential diagnosis.
Most of the systematic, scoping, and narrative reviews identified were relevant to our research question and offered useful context, but they were excluded from the quantitative analysis. Their quality was not formally assessed, as this lies outside the domain of a scoping review. For example, Maselli et al. [17], Henschke et al. [60], and Verhagen et al. [28] discussed approaches to evaluating RFs in suspected serious pathology, including cancer; however, for methodological reasons, their findings were cited only as background rather than included in the statistical synthesis. The limited strength of evidence, as well as conflicting diagnostic accuracy values, were repeatedly highlighted by the authors themselves, justifying a cautious interpretation of the diagnostic utility of RFs.
A main outcome of this scoping review is that most of the evidence derives from case reports or small observational studies. Even reviews in this field rely on very few primary sources, underscoring the scarcity of robust data and thus limiting the strength of epidemiological or clinical inferences. Within this context, some authors proposed specific combinations of RFs, referred to as clusters, as more diagnostically valuable than isolated signs. These clusters, discussed by Henschke [60], Verhagen [28], and Delladio [82], were associated with higher sensitivity and/or specificity values and appear particularly relevant in guiding early referral or diagnostic imaging. In line with these observations, “history of cancer” consistently emerged as the most reliable individual RF [90,92,93], while most others showed limited accuracy when assessed in isolation. Similar conclusions were drawn by Finucane et al. [63], who emphasized that aside from a previous history of cancer, most RFs lack sufficient validation and may present too late to be useful for early detection. This supports the importance of combining RFs with clinical judgment to strengthen diagnostic reasoning. Although the quality of the supporting evidence is only moderate to low, the fact that these combinations are repeatedly mentioned across different sources suggests they may be worth exploring further in clinical research.
Considering these findings, the existing literature on cancer presenting with LBP appears fragmented and often limited to anecdotal or retrospective data. The lack of prospective studies and the predominance of case-based literature limit the development of strong epidemiological conclusions, highlighting the need for better-designed research with larger samples to improve understanding of the diagnostic process. Similar observations have also been made in studies on neck pain, where single RFs showed limited reliability and most serious cases were due to metastatic disease. This suggests that the difficulties in recognizing cancer are not confined to the lumbar spine but can be seen across different spinal regions [94]. A final summary table (Table 8) presents the diagnostic performance of selected individual RFs together with clinical clusters identified across Premkumar’s primary study [90]. For comparative purposes, two additional clusters derived from two reviews are included, although these are secondary data and were not used in the main analysis [60,82].
4.1. Implications for Clinical Practice
This scoping review offers valuable insights into the nature and limitations of the current evidence surrounding the diagnostic process for identifying cancer in patients presenting with low back pain. The predominance of case-based studies highlights the lack of high-level research and reinforces the need for clinical caution when interpreting RFs. Although several systematic reviews have attempted to define the diagnostic utility of the RFs, they often rely on limited primary data, and the findings appear inconsistent. Clinicians should avoid over-reliance on individual RFs; more specifically, clinicians should adopt a reasoned clinical approach that considers combinations of risk factors and the broader clinical context. Overall, and in patients with LBP associated with underlying malignancy, RFs seem to be more useful for ruling in rather than ruling out (i.e., screening) serious pathologies. Nevertheless, the poor specificity of many RFs underscores the risk of both under- and over-diagnosis. These findings support the development of more refined clinical tools and structured decision-making frameworks to enhance cancer screening in patients with LBP, particularly in direct access contexts.
4.2. Research Implications
More robust evidence is needed to understand how individual RFs, and especially their combinations, can help in the early detection of cancer in patients presenting with LBP. At present, much of the literature is not homogeneous due to differences in diagnostic criteria, clinical settings, and patient populations. Most of the available studies are case reports or small observational series; thus, while these are useful to describe unusual presentations, they do not allow firm or generalizable conclusions. Future research should make use of multicenter registries or large retrospective cohorts, especially in primary care settings, to build and test predictive models that support clinical decisions and help identify patients who may need earlier referral for suspected serious disease. Although based mainly on case reports, some RF clusters described in the literature [60,82,90] may provide preliminary guidance, but their value needs to be confirmed in studies with experimental designs.
4.3. Strengths and Limitations
This review has several strengths. First, the analysis was conducted using a systematic and transparent method, based on the JBI approach [18] and PRISMA-ScR criteria [19].
In addition, the inclusion of heterogeneous sources such as case-based studies and narrative reviews made it possible to identify less frequent clinical presentations and to map a broader overview of the literature. However, some limitations should be acknowledged. The quality of the included studies was not formally assessed. Most consisted of case-based studies or narrative reviews, which provide valuable descriptive information but are methodologically limited and prone to bias. Furthermore, the inclusion of only English or Italian language studies, together with the restriction to publications from 1999 to 2025, may have led to the exclusion of relevant evidence. The variability among the studies and the lack of precision in the description of RFs also made it difficult to group findings and interpret the data consistently. Finally, results from systematic reviews were not directly used to avoid methodological errors related to data duplication, although these reviews were consulted to identify relevant primary studies.
5. Conclusions
This scoping review aimed to map the current evidence on the presence and diagnostic utility of RFs for detecting spinal malignancies in patients presenting with low back pain. Although a substantial number of studies were identified, the majority consisted of case-based literature, reflecting a limited availability of high-quality primary research. While certain RFs, such as a history of cancer, showed greater consistency across studies, most others demonstrated poor standalone diagnostic performance. Furthermore, considerable variability was observed in how RFs were defined, applied, and reported. Overall, and in patients with LBP associated with underlying malignancy, RFs seem to be more useful for ruling in rather than ruling out (i.e., screening) serious pathologies. Nevertheless, the findings point to the need for clearer research methods and better-designed studies to help clinicians recognize serious conditions earlier in patients with low back pain. Although current evidence remains limited, assessing RFs in combination rather than in isolation may lead to better diagnostic accuracy. Greater clarity on how RFs are defined, along with the development of reliable clinical tools, could improve clinical decision-making and help detect cancer earlier in patients with low back pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burton A.K. COST B 13 Working Group European Guidelines for Prevention in Low Back Pain University of Huddersfield Huddersfield, UK 2004153
- 2Feller D. Giudice A. Maritati G. Maselli F. Rossettini G. Meroni R. Lullo G. Hutting N. Mourad F. Physiotherapy Screening for Referral of a Patient with Peripheral Arterial Disease Masquerading as Sciatica: A Case Report Healthcare 202311152710.3390/healthcare 1111152737297667 PMC 10252713 · doi ↗ · pubmed ↗
- 3Maselli F. Storari L. Barbari V. Colombi A. Turolla A. Gianola S. Rossettini G. Testa M. Prevalence and incidence of low back pain among runners: A systematic review BMC Musculoskelet. Disord.20202134310.1186/s 12891-020-03357-432493481 PMC 7271446 · doi ↗ · pubmed ↗
- 4Maselli F. Esculier J.F. Storari L. Mourad F. Rossettini G. Barbari V. Pennella D. Cataldi F. Viceconti A. Geri T. Low back pain among Italian runners: A cross-sectional survey Phys. Ther. Sport 20214813614510.1016/j.ptsp.2020.12.02333434869 · doi ↗ · pubmed ↗
- 5Maselli F. Testa M. Superficial peroneal nerve schwannoma presenting as lumbar radicular syndrome in a non-competitive runner J. Back Musculoskelet. Rehabil.20193236136510.3233/BMR-18116430664501 · doi ↗ · pubmed ↗
- 6Blyth F.M. Briggs A.M. Schneider C.H. Hoy D.G. March L.M. The Global Burden of Musculoskeletal Pain—Where to From Here?Am. J. Public Health 201910935403049599710.2105/AJPH.2018.304747 PMC 6301413 · doi ↗ · pubmed ↗
- 7GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017 Lancet 20173921789185810.1016/S 0140-6736(18)32279-7PMC 622775430496104 · doi ↗ · pubmed ↗
- 8Han C.S. Hancock M.J. Downie A. Jarvik J.G. Koes B.W. Machado G.C. Verhagen A.P. Williams C.M. Maher C.G. Red flags to screen for vertebral fracture in patients presenting with low back pain Cochrane Database Syst. Rev.20222022 CD 01446110.1002/14651858.cd 014461 PMC 1044886437615643 · doi ↗ · pubmed ↗